

Abstract
Total Knee replacement (TKR) is one of the commonest arthroplasty surgeries performed. Various techniques of closures in TKR are described. This technical note describes an useful technique of achieving water tight closure in TKR. An optimal tension watertight closure also reduces the chances of dead space hematomas and infection. The author has described his technique where the soft tissues are never unduly compromised. In his experience the patient can be mobilized freely in bed and even allowed to sleep prone after first wound check.
Keywords: Total knee replacement, Closure
Introduction
The seventies marked the beginning of the era of Total Knee Replacement (TKR). Over the years the operation has now evolved both in terms of component design and surgical technique. TKR is meant to relieve pain from arthritis and is generally recommended for older people as it has a finite life. However newer designs and materials are available for younger patients with arthritis. The success of a TKR depends on various factors which include appropriate choice of implant and meticulous surgical technique. It is often said that a knee replacement is a soft tissue operation and balancing the soft tissues gives good outcomes. Mention must also be made of the concept of minimal soft tissue trauma surgery where gentle handling of the tissues during surgery helps in reduced wound complications. However many standard textbooks of knee arthroplasty do not dwell on the detail of closure.
Meticulous wound closure has a bearing on wound healing and also on infection rate. Moreover TKR requires a mobile recovery and thus an optimal tension wound environment which will allow early rehabilitation. Recently there have been some articles on wound closure where the focus was on the suture material and time required to closure using a special barbed suture which gives a watertight closure of the arthrotomy. Closure of the knee in flexion or extension has also been studied. One study showed that the position of the knee during closure does not have any bearing on early rehabilitation[1]. A systematic review of knee position during closure has showed that closure of the knee in flexion allows more flexion range and less domiciliary physiotherapy [2]
This note explains in detail about the authors technique of soft tissue closure in TKR Surgery.
Technical Note
The author usually deflates the tourniquet after cementation when the cement becomes hard. After copious saline lavage the closure is started by keeping the limb in extension. The planning of the closure is done at the beginning of the surgery. The medial arthrotomy is performed in a specific way which allows a landmark in the quadriceps to approximate correctly during closure. The vertical limb of the rectus tendon incision is taken down to the patella and sharply angulated medially causing an L shaped cut (Fig. 1a-b) which then skirts the medial patella leaving a cuff of tissue around the patella, before taking the incision down to the tibia adjacent to the patella tendon. The closure begins at the angle of the angle of ‘L’ incision (Fig. 1c). This will allow perfect approximation of the tendon and prevent a large degree of vertical translation error in soft tissues.
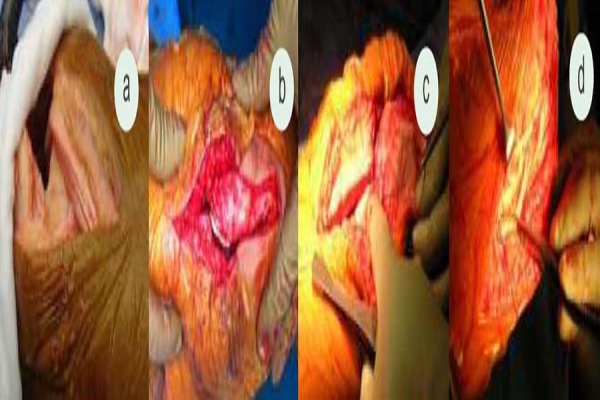
Fig 1a.L arthrotomy Fig 1b. Medial parapatellar arthrotomy Fig 1c. first step- Approximate sharp ends of L cut in extension Fig 1d. 2 layers of Quadriceps tendon suturing technique
Once this step is done the knee is placed in 90° of flexion and the inner layer of the rectus muscle is sutured upwards starting from the ‘L’ knot and running proximally in a continuous locking manner (Fig. 1d). Once the proximal limit of the arthrotomy is reached where the tendon ends and muscle begins the suture is locked and the running locking suture technique is used to oppose the superficial tendon layer till it reaches the ‘L’ angle where the suture is finally tied and cut.
This technique invariably creates a water tight suture. Once this is done the drain is now placed in the suprapatellar pouch and into the knee taking it out proximally. Putting the drain in at this stage also ensures that the drain will not be inadvertently sutured!
Attention is now directed to the patellar tendon part of the arthrotomy. The knee is kept in ninety degrees and interrupted figure of eight and or mattress type sutures are taken till the distal limit of the arthrotomy. It must be mentioned that the primary exposure of the proximal tibia should always be done in an unhurried manner carefully stripping of the medial cuff of tissue during the release. This cuff elevated off the tibia helps strong closure. The remaining parapatellar arthrotomy is now closed with the knee in extension using interrupted mattress type sutures or locked figure of eight sutures. Thus the entire medial parapatellar arthrotomy is closed with optimal tension and minimal soft tissue trauma (Fig 2b). The subcutaneous tissue is closed with 2-0 Vicrly and the skin is closed with staples without traumatizing it by using tooth forceps subcutaneously (Fig 2c). Many times the skin may not need handling as the edges come together after the subcutaneous closure.
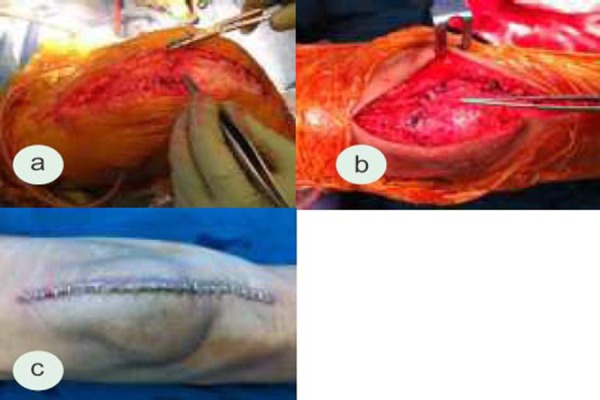
Fig 2a. closure in 90 degree flexion
Fig 2b. High tension closure of medial parapatellar arthrotomy
Fig2c. final skin closure
Conclusion
Meticulous closure of the soft tissues after a knee replacement has an impact on early recovery and mobilization. An optimal tension watertight closure also reduces the chances of dead space hematomas and infection. The author has described his technique where the soft tissues are never unduly compromised. In his experience the patient can be mobilized freely in bed and even allowed to sleep prone after first wound check.
Video of the technique is available at www.jocr.co.in
Footnotes
Conflict of Interest: Nil
Source of Support: None
References
- 1.Masri B A, Laskin R S, Windsor R E, Haas S B. Knee closure in total knee replacement: a randomized prospective trial. Acta Orthop Belg. 2010 Jun;76(3):298–306. doi: 10.1097/00003086-199610000-00011. [DOI] [PubMed] [Google Scholar]
- 2.Smith TO, Davies L, Hing CB. Wound closure in flexion versus extension following total knee arthroplasty: a systematic review. Int Orthop. 2009 Aug;33(4):887–93. [PubMed] [Google Scholar]