

Abstract
Hepatitis C virus (HCV) is endemic in Pakistan and its burden is expected to increase in coming decades owing mainly to widespread use of unsafe medical procedures. The prevalence of HCV in Pakistan has previously been reviewed. However, the literature search conducted here revealed that at least 86 relevant studies have been produced since the publication of these systematic reviews. A revised updated analysis was therefore needed in order to integrate the fresh data. A systematic review of data published between 2010 and 2015 showed that HCV seroprevalence among the general adult Pakistani population is 6.8%, while active HCV infection was found in approximately 6% of the population. Studies included in this review have also shown extremely high HCV prevalence in rural and underdeveloped peri-urban areas (up to 25%), highlighting the need for an increased focus on this previously neglected socioeconomic stratum of the population. While a 2.45% seroprevalence among blood donors demands immediate measures to curtail the risk of transfusion transmitted HCV, a very high prevalence in patients attending hospitals with various non-liver disease related complaints (up to 30%) suggests a rise in the incidence of nosocomial HCV spread. HCV genotype 3a continues to be the most prevalent subtype infecting people in Pakistan (61.3%). However, recent years have witnessed an increase in the frequency of subtype 2a in certain geographical sub-regions within Pakistan. In Khyber Pakhtunkhwa and Sindh provinces, 2a was the second most prevalent genotype (17.3% and 11.3% respectively). While the changing frequency distribution of various genotypes demands an increased emphasis on research for novel therapeutic regimens, evidence of high nosocomial transmission calls for immediate measures aimed at ensuring safe medical practices.
Keywords: Hepatitis C, Pakistan, Hepatitis C virus, Liver cancer, Hepatitis C virus genotypes, Epidemiology
Core tip: Hepatitis C virus (HCV) in Pakistan is highly endemic, with around 6.8% of general population infected with this virus. Approximately 6% of the population of Pakistan is actively infected with HCV. However, only very few relevant reports are available and more studies are needed. Research articles reviewed suggest a link between underdevelopment and HCV prevalence, as well as the predominant involvement of unsafe medical procedures in the spread of the virus in Pakistan. Although genotype 3a is most prevalent HCV subtype in Pakistan, recent years have witnessed an increase in the incidence of genotype 2a in Sindh and Khyber Pakhtunkhwa provinces.
INTRODUCTION
Infection with hepatitis C virus (HCV) is a major global health concern. With an estimated 170 million people infected with HCV worldwide, this disease is proving to be an escalating economic, social and health burden[1,2]. Although the prevalence of HCV infection seems to have declined in the past two decades in the United States[3,4], Western and Northern Europe[5,6], Japan[7] and Australia[8], the burden of this disease in many of the lesser developed and developing countries is continuously on the rise[2]. Awareness, improved safety of blood products, the availability of affordable and effective HCV therapies have contributed significantly to the decline in HCV in developed countries. However, lack of awareness, inadequate blood screening facilities, nosocomial transmission and a lack of effective treatments (due to various reasons) have so far been the major factors responsible for seemingly inexorable rise in HCV infection in many developing countries[2,9].
HCV is a member of the family Flaviviridae with an approximately 9.6 kb single-stranded, positive sense RNA genome[10]. Owing to the poor fidelity of HCV RNA-dependent-RNA-polymerase (NS5B protein), the virus exhibits a high level of sequence heterogeneity[10]. Based on sequence homology six major HCV genotypes (1-6) and numerous distinct subtypes (denoted by a small English alphabet suffixed after genotype, e.g., 1b, 3a etc.) have so far been identified[11]. The distribution of HCV genotypes is highly variable. Genotypes 1-3 are distributed globally, whereas genotypes 4 and 5 are restricted to the Middle East and Africa, and genotype 6 occurs predominantly in south-east Asian countries[2,12-14]. HCV genotype 3 is endemic on the Indian subcontinent[1]. Multiple studies have identified subtype 3a as the most prevalent HCV variant in Pakistan[15,16]. However, recent data suggest that, although genotype 3a might still be the predominant HCV subtype in Pakistan, the epidemiological pattern and relative frequency distribution of various genotypes have undergone appreciable change[17,18]. These studies have indicated a rise in the incidence of genotype 2a, particularly in the north-western province Khyber Pakhtunkhwa (KPK)[17,18].
The prevalence of HCV varies by region. Western Europe, the Americas and Australia are considered regions of low HCV prevalence (< 2%). African and the eastern Mediterranean are areas with the highest HCV prevalence[9]. In Egypt, the prevalence of HCV is greater than 14%, the highest of any country in world[19,20]. Even though the prevalence in Asia has been estimated to be a little above 2%, it varies greatly between individual countries[1]. Mongolia has the highest HCV prevalence (above 10%), followed by Uzbekistan and Pakistan where, according to some reports, around 6% of the total population is infected with HCV[1].
Our understanding of HCV epidemiology in Pakistan has been greatly improved by the numerous studies conducted over the span of the past two decades. Additionally, a comprehensive nation-wide survey of HBV/HCV prevalence, probably the first of its kind, was carried out in the years 2007-2008[21] and a national hepatitis sentinel site surveillance system has been fully operational since June 2010[22]. Five single facility-based sentinel sites (located in four provincial capitals and Islamabad) have so far been established. Nonetheless, due to limited catchment areas of these facilities, data related to the incidence of new cases and ongoing transmission patterns and trends in the majority of the population remains inadequate. Also, the scope of the national survey was limited only to screening for HBV/HCV seropositivity among healthy individuals. Thus the survey did not encompass HCV prevalence in high risk groups and the frequency distribution of HCV genotypes was also not studied. Even a cumbersome endeavor like national survey therefore did not provide data of such high translational importance.
Data on the prevalence of HCV in Pakistan has previously been comprehensively reviewed[16,23,24]. Recent years have seen an increased focus among Pakistani researchers on the study of HCV prevalence patterns and frequency distribution of its genotypes. At least eighty six relevant studies have been published in national and international journals since the publication of aforementioned reviews (2009, 2010). These newer studies have not only explored HCV prevalence in previously uncovered areas (such as Azad Kashmir[25] and Balochistan[26,27]) but have also shed light on the possible connection between underdevelopment and high HCV prevalence (for example, 23.83% prevalence in peri-urban areas of country’s largest city Karachi[28] and 25.1% in rural Sindh[29]). This highlights the importance and need for integration of newer reports in a comprehensive updated analysis. Above all, given the fact that some 15%-45% HCV infected patients may spontaneously clear the virus but still remain seropositive for HCV[30,31], results from seroprevalence studies may end up exaggerating the actual burden of disease. Recent World Health Organization (WHO) guidelines also recommend that polymerase chain reaction (PCR) based HCV diagnosis should be carried out not only to confirm HCV seropositivity but also to distinguish persons with active HCV infection from those with resolved past infection[32]. Not much attention has been paid to the categorical estimation of active HCV infection as determined by HCV nucleic acid testing (NAT) in previous systematic reviews[16,23,24].
The primary objective of this review is to summarize recent evidence and attempt to address the deficiencies in our knowledge of the epidemiology of HCV in Pakistan. Moreover, a thorough literature search, spanning the last two decades (1994-2015), was carried out to identify studies that investigated HCV prevalence in the general adult population of Pakistan. Results from these studies were pooled to produce a comprehensive map of HCV prevalence in Pakistan at the district level (Figure 1).
Figure 1.
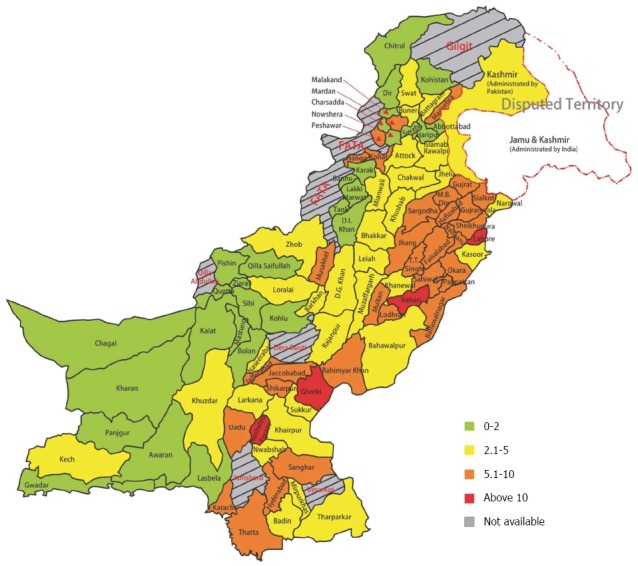
Hepatitis C virus seroprevalence in Pakistan at the district level.
METHODOLOGY
Literature search
A systematic literature search was carried out for publications dealing with the prevalence of HCV infection in the general population, blood donors, various population sub-groups considered to be at increased risk of contracting HCV infection and patients suffering from liver disease etc. Moreover scientific reports of the frequency distribution of HCV genotypes in Pakistan were also considered. Articles and abstracts published between 2010 and April 2015, in both indexed and non-indexed journals, were included. The literature search used the electronic databases PubMed, Google Scholar as well as PakMediNet (for non-indexed Pakistani journals). Relevant literature and unpublished data was also obtained from the Pakistan Medical Research Council website (http://www.pmrc.org.pk). All the relevant research articles that appeared after the publication of earlier compilations of HCV related Pakistani data (December 2009[16], Summer 2010[23] and December 2010[24]) were included. Any relevant papers published prior this, which were not covered in any of the previous reviews, were also included. Furthermore, references cited within articles were also carefully screened to look for more relevant publications. In total, eighty seven relevant publications were identified. Out of these, one study was excluded due to possible data duplication and eighty-six (86) studies were finally included in the review.
A few studies used two step confirmatory testing for estimating the seroprevalence of HCV; verification of the initial immunochromatographic screening (ICT) by more sensitive methods such as enzyme linked immunosorbent assay (ELISA). In such cases, only those samples were included in calculations which tested positive for both of the assays. In addition to the estimation of HCV seroprevalence, as defined by detection of antibodies against HCV in an individual’s blood, studies which investigated active HCV infection in various population groups were included. Active HCV infection was defined as the presence of HCV RNA in a patient’s serum, as assessed by established PCR based methods[33]. For studies that reported both seroprevalence and active HCV infection, respective results were included in both estimates. Similarly, data from studies reporting HCV prevalence (sero- or active) in more than one population group was included in both calculations.
Analysis
Results from all the studies pertaining to a specific population subset were pooled and the results are presented as the weighted average. The weighted mean was calculated using the formula previously described[16].
Where ω represents the number of subjects included in an individual study and x stands for percent prevalence found in that particular study.
HCV PREVALENCE IN VARIOUS POPULATION GROUPS
Seroprevalence of HCV in the general population
Data obtained from sixteen studies[26,28,29,34-46] and the national survey on the prevalence of HCV infection in Pakistan (described as the “national survey” from here on)[21] is presented in this section (Table 1). A total of 165846 persons were screened in these studies. The prevalence of HCV infection in general adult population (15 years of age and above) ranged from 2.3% in Gujranwala[43] to 28.6% in rural areas of Nausheroferoz district, Sindh[29]. Mean serofrequency of HCV infection among healthy adults in Pakistan was found to be 6.8%, significantly higher than previous estimates; 4.7%[23] and 4.95%[16] as well as 4.87% for the national survey[21]. Unfortunately no reports were available from Federally Administered Tribal Areas, Gilgit Baltistan and some districts in Balochistan and KPK. Nonetheless, studies cited in this article mainly pertained to three of the bigger provinces, Punjab, Sindh and KPK (most districts), as well as one study from Balochistan[26], which together make up for more than 80% of the population of Pakistan.
Table 1.
Hepatitis C virus seroprevalence among healthy adult population
| S. # | Year | Place | Method |
Sample size |
Seroprevalence (%) |
Ref. | ||||
| Male | Female | Total | Male | Female | Total | |||||
| 1 | 2009 | Lahore | ELISA9 | - | - | 2000 | - | - | 6.5 | [38] |
| 2 | 2009 | Larkana | ICT1 | 353 | 97 | 450 | 7.37 | 4.12 | 6.66 | [46] |
| 3 | 2010 | Swat | ICT2 | 290 | 300 | 590 | 6.2 | 11.3 | 8.81 | [45] |
| 4 | 2010 | Mansehra | ICT2 | - | - | 400 | - | - | 7.0 | [36] |
| 5 | 2010 | Thatta/Nausheroferoz | ICT3 | - | - | 303 | - | - | 25.1 | [29] |
| 6 | 2010 | Karachi(peri-Urban) | EIA4 | 649 | 1348 | 1997 | 19 | 26 | 23.83 | [28] |
| 7 | 2010 | Karachi | ICT9 | 351 | 153 | 504 | 2.8 | 5.23 | 3.17 | [34] |
| 8 | 2010 | ELISA9 | [41] | |||||||
| Multan | 625 | - | 625 | 9.6 | - | 9.6 | ||||
| Lahore | 1892 | - | 1892 | 9.4 | - | 9.4 | ||||
| Faisalabad | 2736 | - | 2736 | 8.8 | - | 8.8 | ||||
| Gujranwala | 16522 | - | 16522 | 7.3 | - | 7.3 | ||||
| Gujrat | 9770 | - | 9770 | 6.8 | - | 6.8 | ||||
| Sargodha | 1620 | - | 1620 | 6.7 | - | 6.7 | ||||
| Rawalpindi | 445 | - | 445 | 6.7 | - | 6.7 | ||||
| Sialkot | 24707 | - | 24707 | 6.2 | - | 6.2 | ||||
| Bahawalpur | 363 | - | 363 | 5.0 | - | 5.0 | ||||
| 9 | 2010 | Islamabad | ICT9 | - | 252 | 252 | - | 24.6 | 24.6 | [40] |
| 10 | 2010 | Mansehra | ICT9 | 394 | 254 | 648 | 11.8 | 9.4 | 10.34 | [44] |
| 11 | 2010 | National Survey | ICT3 | 24444 | 22599 | 47043 | 4.9 | 4.8 | 4.87 | [21] |
| 12 | 2011 | Gujranwala | EIA5 | 1770 | 732 | 2502 | 2.6 | 1.68 | 2.32 | [43] |
| 13 | 2011 | Karachi | CLIA6 | - | - | 32049 | - | - | 9.75 | [35] |
| 14 | 2012 | Kech | EIA7 | 709 | 1291 | 2000 | 7.62 | 4.34 | 5.5 | [26] |
| 15 | 2012 | Punjab | EIA7 | 14027 | 14027 | - | 3.13 | - | 3.13 | [39] |
| 16 | 2014 | Mardan | ICT8 | 757 | 662 | 1419 | 13.6 | 9.52 | 11.7 | [37] |
| 17 | 2014 | Peshawar | CMIA4 | 543 | 439 | 982 | 15.4 | 9.7 | 12.93 | [42] |
Nobis Labordiagnostica, Cluj-Napoca, Romania;
Acon Laboratories, CA, United States;
Bionike Inc. CA, United States;
Abbott Diagnostics, IL, United States;
DSI, srl. Saronno VA, Italy;
Roche Diagnostics, CA, United States;
DiaSorin International Inc., Saluggia, Italy;
Accurate Diagnostic Labs, NJ, United States;
Manufacturer not mentioned in cited reference. ELISA: Enzyme linked immunosorbent assay; CLIA: Chemiluminescence immunoassay; ICT: Immunochromatographic test; EIA: Enzyme immunoassay; CMIA: Chemiluminescent microparticle immunoassay.
An almost 40% increase in HCV seroprevalence shown in our analysis, in comparison to earlier reports, is alarming. However, it is not clear whether this upward trend is due to the coverage of more high risk groups, better sampling strategies and improved diagnostic facilities or actually indicates an increase in the incidence of new HCV cases. It must be noted here that in the last seven years, Pakistan has suffered at least one major natural disaster (2010 flood) as well as fallout from the ongoing war on terror in the form of mass population displacements. Effects of such human tragedies on the spread of HCV infection in an already high prevalence country cannot be overlooked and needs to be monitored carefully. At least one report can be cited in this context. A study conducted in 2010 revealed that HCV serofrequency in internally displaced persons from Swat district was indeed much higher than reported previously for the healthy adult population of the same district (8.8% vs 2.2%)[45,47].
It is worthwhile mentioning that subjects of most of the studies cited in the current review were either in urban areas or in some cases not clearly defined (Table 1). Nonetheless, at least two of the studies that categorically targeted rural[29] or peri-urban populations[28] reported an extremely high frequency of anti-HCV prevalence in these areas, 28.6% and 23.8% respectively (entries 5 and 6 in Table 1). In addition to this, an older study found a remarkably high HCV prevalence in the rural population of Punjab province in comparison to urbanized areas (15.73% vs 9.95%, respectively)[48]. Earlier reports published by Abbas et al[25,34] also substantiate the suspicion that the burden of HCV disease among rural areas is manifold higher than in urban areas. Unfortunately, due to scarcity of studies specifically targeting the rural population, neither the true extent of HCV spread in rural areas is known, nor does it reflect in national prevalence estimates. As more than 60% of people in Pakistan reside in these high prevalence rural areas[49], the actual burden of HCV disease in Pakistan may be much higher than current and previous estimates. More studies are needed to fill this fundamental gap in our knowledge regarding the true burden of HCV disease in Pakistan.
Previous studies as well as the national survey have indicated a highly heterogeneous pattern of HCV prevalence in various cities and regions of Pakistan. In order to obtain a more comprehensive picture of HCV prevalence in various districts and regions of Pakistan, we carried out a thorough literature search spanning the last two decades, from 1994 to 2015 (Figure 1). All studies that investigated HCV prevalence in the general adult population were included. We found fifty relevant studies[21,26,28,29,34-48,50-80] published in international and local journals. In total 366066 individuals were screened in these studies. Reports from almost all provinces/administrative units of Pakistan were included. Moreover, a detailed district-wise prevalence estimate was available through the results of the national survey. Where more than one report was available from same district, a weighted mean was calculated using the data (including the national survey). For districts for which no reports, other than the national survey were available, the data was used to construct the district wise prevalence map which is presented in Figure 1.
HCV seroprevalence in blood donors
Regular screening of blood donors is essential for controlling the spread of transfusion transmitted infections (TTIs). Screening of blood for TTIs, including HCV, prior to transfusion is now a common practice among healthcare providers in Pakistan, especially after the introduction of a comprehensive National Blood Policy in 2003 and development and implementation of blood transfusion laws in all the provinces and units of federation[81]. However, the risk of non-implementation and non-adherence to these regulations is still quite high, particularly in remote and underdeveloped areas[16]. Thirteen studies[25,27,82-92] published between 2009 and 2014 reported HCV prevalence in blood donors (Table 2). Mean HCV prevalence among healthy blood donors was estimated at 2.45%. A majority of blood donors hailed from the country’s largest city Karachi alone (159942 out of total of 400716)[83,86,87,90], where mean prevalence of HCV infection among blood donors was 2.31%. Pakistan’s largest province Punjab remained underrepresented in this group, as only three reports comprising of 10345 patients were available[82,85,88]. A study conducted by Akhtar et al[82] reported a very high prevalence (15.1%) of HCV infection among blood donors from Lahore, the second largest metropolitan city in Pakistan. Khan et al[27] reported a 20.8% seroprevalence of HCV infection in a group of 356 blood donors hailing from Quetta, capital of Balochistan, the province which is otherwise considered a low endemicity area (1.5% prevalence in national survey)[21].
Table 2.
Seroprevalence of hepatitis C virus infection in blood donors
| S. # | Year | Place | Method | Sample size | Seroprevalence (%) | Ref. |
| 1 | 2009 | Mirpurkhas | ELISA7 | 804 | 15.05 | [25] |
| 2 | 2010 | Multan | ELISA1 | 10000 | 4.90 | [88] |
| 3 | 2010 | Peshawar | ELISA7 | 32042 | 1.57 | [92] |
| 4 | 2011 | KPK/FATA | ELISA2 | 7148 | 1.89 | [89] |
| 5 | 2011 | KPK/FATA | ELISA2 | 62251 | 2.60 | [91] |
| 6 | 2011 | Karachi | -8 | 5717 | 1.90 | [86] |
| 7 | 2012 | Karachi | ELISA3 | 5517 | 2.00 | [83] |
| 8 | 2012 | Peshawar | ELISA2 | 127828 | 2.46 | [84] |
| 9 | 2012 | Sargodha | ELISA3 | 100 | 12.00 | [85] |
| 10 | 2013 | Karachi | MEIA/CLIA4 | 108598 | 2.61 | [87] |
| 11 | 2013 | Quetta | ELISA2 | 356 | 20.8 | [27] |
| 12 | 2013 | Lahore | ELISA5 | 245 | 15.00 | [82] |
| 13 | 2014 | Karachi | CLIA6 | 42830 | 1.65 | [90] |
Labkit Chemelex, Barcelona, Spain;
Biokit;
General Biologicals Corporation, Taiwan;
Abbott Diagnostics,
DiaSorin;
Ortho Clinical Diagnostics, NJ, United States;
Manufacturer not mentioned in cited reference;
Method not mentioned in cited reference. KPK: Khyber Pakhtunkhwa; FATA: Federally Administered Tribal Areas; ELISA: Enzyme linked immunosorbent assay; MEIA: Microparticle immunoassay; CLIA: Chemiluminescence immunoassay.
HCV infection in patients with liver disease
Hepatitis C virus infection is an important underlying cause of liver disease and accounts for about 25% of hepatocellular carcinoma (HCC) cases worldwide[93]. However, epidemiological data suggests that in contrast to the worldwide trend, where HBV is considered the major etiology underlying HCC, in countries of high HCV prevalence such as Egypt and Pakistan, HCV is the most common cause of chronic liver diseases including HCC[93]. A previous comprehensive review of all the studies published before 2010 (ten studies) estimated 50.6% mean frequency of HCV seropositivity among HCC patients in Pakistan[23]. Three studies published between 2010 and 2014[94-96], and also two studies published in 2009[97,98] but not included in previous reviews[16,23,24], dealing with the frequency of HCV infection HCC patients were identified. These studies screened 1100 HCC patients from different areas of Pakistan. Serofrequency of HCV infection among HCC patients ranged from 48.5%[95] to 79.2%[98] (Table 3, entries 1-5). Mean HCV prevalence in this patient group was 57.5%.
Table 3.
Hepatitis C virus in patients with liver disease
| S. # | Year | Place | Method | Sample size | Seroprevalence (%) | Ref. | ||||
| Hepatocellular carcinoma | ||||||||||
| 1 | 2009 | Punjab/KPK | ELISA1 | 145 | 76.5 | [97] | ||||
| 2 | 2009 | Pakistan | EIA2 | 82 | 79.2 | [98] | ||||
| 3 | 2010 | Karachi | -5 | 40 | 50 | [94] | ||||
| 4 | 2013 | Pakistan | ELISA4 | 645 | 48.5 | [95] | ||||
| 5 | 2014 | Hyderabad | ELISA4 | 188 | 66 | [96] | ||||
| Liver disease | AH | CH/CLD | Carrier | Cirrhosis | ||||||
| 6 | 2009 | Swat | ELISA4 | 110 | - | - | - | 63.6 | [99] | |
| 7 | 2009 | Pakistan | EIA2 | 107 | - | 62.6 | - | 24.3 | [98] | |
| 8 | 2010 | Karachi | -5 | 5153 | 7 | 72.9 | 51.7 | 59.4 | [94] | |
| Hepatic encephalopathy | ||||||||||
| 9 | 2009 | Hyderabad | -5 | 87 | 66.67 | [100] | ||||
| Suspected for viral hepatitis | ||||||||||
| 10 | 2014 | Islamabad | ELISA3 | 845 | 24.8 | [101] | ||||
DRG Instruments, Germany;
Abbott Diagnostics;
Biokit;
Manufacturer not mentioned in cited reference;
Method not mentioned in cited reference. AH: Acute hepatitis; CH: Chronic hepatitis; CLD: Chronic liver disease; ELISA: Enzyme linked immunosorbent assay; EIA: Enzyme immunoassay; KPK: Khyber Pakhtunkhwa.
Three studies reported HCV prevalence among cirrhosis patients[94,98,99] (Table 3, entries 6-8). Khan and colleagues found 24.3% cirrhotic patients positive for anti-HCV[98], another report from a different group showed that 63.6% cirrhotic patients in the district Swat were infected with HCV[99]. Ahmed and coworkers found 59.4% HCV seroprevalence among cirrhotic patients in Karachi city[94]. Similarly Khan et al[98] and Ahmed et al[94] found 62.6% and 72.9%, respectively, HCV seroprevalence among patients suffering from chronic hepatitis or chronic liver disease. A hospital based study conducted by Devrajani et al[100] in 2009 found that more than two thirds of patients reporting with complaint of hepatic encephalopathy tested positive for the presence of anti-HCV in their blood. A recent single center study showed that among all the patients referred to the said hospital with a suspected hepatitis virus infection, approximately one quarter were found to be positive for HCV[101] (for details see Table 3).
PREVALENCE OF HCV IN HIGH RISK POPULATION GROUPS
Pregnant women
It has previously been suggested that the predominant mode of HCV transmission in Pakistan is nosocomial or iatrogenic[16]. Therefore pregnant women who require more hospital visits and have to undergo more medical and surgical procedures are considered to be at an increased risk of contracting HCV infection. Based on data from six relevant studies[102-107], mean HCV prevalence in pregnant women was estimated around 4.51%. The prevalence of HCV infection in pregnant women ranged from 1.83% in Karachi[106] to 8.6% in Hazara division[104] (Table 4, entries 1-6).
Table 4.
Hepatitis C virus serofrequency in high risk population groups
| S. # | Year | Place | Method | Sample size | Seroprevalence (%) | Ref. |
| Pregnant women | ||||||
| 1 | 2009 | Hazara | ELISA1 | 500 | 8.6 | [104] |
| 2 | 2009 | Swat | ICT6 | 5607 | 2.6 | [105] |
| 3 | 2009 | Karachi | EIA2 | 5902 | 1.8 | [106] |
| 4 | 2010 | Multan | ICT6 | 500 | 7.0 | [107] |
| 5 | 2011 | Karachi | ELISA3 | 18000 | 5.79 | [102] |
| 6 | 2013 | Hyderabad | ELISA2 | 3078 | 4.7 | [103] |
| Multi-transfused population (including pediatric population) | ||||||
| 7 | 2009 | Islamabad | ELISA6 | 103 | 36.0 | [108] |
| 8 | 2010 | Lahore | Questionnaire | 408 | 1.5 | [110] |
| 9 | 2011 | KPK | ICT4 | 40 | 15.0 | [111] |
| 10 | 2011 | Karachi | ELISA3 | 173 | 51.4 | [86] |
| 11 | 2012 | Karachi | ELISA5 | 160 | 13.0 | [83] |
| 12 | 2014 | Rawalpindi | ELISA6 | 95 | 49.5 | [109] |
| Intravenous drug users | ||||||
| 13 | 2011 | KPK | ICT4 | 42 | 14.28 | [111] |
| 14 | 2011 | KPK | ICT4 | [113] | ||
| Peshawar | 100 | 35.0 | ||||
| Kohat | 60 | 25.0 | ||||
| Mardan | 40 | 32.5 | ||||
Ortho Clinical Diagnostics;
Abbott Diagnostics;
DiaSorin;
Acon Laboratories, CA, United States;
General Biologicals Corporation;
Manufacturer not mentioned in cited reference. KPK: Khyber Pakhtunkhwa; ELISA: Enzyme linked immunosorbent assay; EIA: Enzyme immunoassay; ICT: Immunochromatographic test.
Multi-transfused individuals
Patients suffering from congenital coagulation disorders, or other diseases that require multiple transfusions of blood at regular intervals throughout their life, are also considered at an increased risk of catching transfusion transmitted infections including HCV. Six relevant studies, covering 979 patients that were regular recipients of blood or blood products transfusions, were identified (Table 4, entries 7-12)[83,86,108-111]. The results obtained were surprisingly variable. HCV prevalence rates in this group ranged from as low as 1.47% in Lahore[110] to around 50% at centers located in Rawalpindi and Karachi[86,109]. Mean HCV prevalence in multi-transfused patients was calculated as 21.04%.
Intravenous drug users
Intravenous drug use is one of the most important risk factors in HCV transmission worldwide[1]. However, its relative contribution to the HCV endemic in Pakistan, is not clear. According to a recent United Nations Office on Drugs and Crime report, some 6-7 million Pakistanis admitted using drugs in the past one year, around half million of which were regular intravenous drug users (IDUs)[112]. Unfortunately, not many studies are available which have focused on serofrequency of HCV infection in this high risk group. Only two recent studies reported HCV prevalence in various districts of KPK province[111,113]. These reports show a prevalence of HCV infection among IDUs to range from 14.3% to 35%. The results of these studies are summarized in Table 4 (entries 13 and 14).
Health care workers
Risk of HCV transmission in health care workers (HCWs) is particularly high[114], and regular screening of this population subgroup is important in order to curtail further spread of HCV infection to patients. Unfortunately not many relevant studies could be found. Only two studies published in the recent past determined anti-HCV frequency in HCWs and both originated from KPK province (Table 5, entries 1 and 2)[115,116]. Khan et al[115] screened HCWs from three major hospitals in Peshawar and reported 4.1% prevalence of HCV, while Sarwar et al[116] reported 5.6% HCV prevalence among HCWs at various hospitals of Abbottabad. An earlier review of published data suggested similar levels of HCV prevalence in HCWs, except for those who reported a history of needle stick injury, in which the prevalence was as high as 10%[24]. Based on available data it is likely that HCV prevalence in HCWs in Pakistan is equal to that of general population.
Table 5.
Hepatitis C virus serofrequency in miscellaneous high risk population groups
| S. # | Year | Place | Method | Sample Size | Seroprevalence (%) | Ref. |
| Health care workers | ||||||
| 1 | 2008 | Abbottabad | ELISA7 | 125 | 5.6 | [116] |
| 2 | 2011 | Peshawar | ICT1 | 824 | 4.1 | [115] |
| Prisoners | ||||||
| 3 | 2010 | Sindh | ELISA2 | 7539 | 12.8 | [117] |
| 4 | 2010 | Karachi | ELISA3 | 357 | 15.2 | [118] |
| Dialysis patients | ||||||
| 5 | 2011 | KPK | ICT4 | 25 | 28.0 | [111] |
| 6 | 2011 | Peshawar | ELISA1 | 384 | 29.2 | [119] |
| Homosexual community | ||||||
| 7 | 2010 | Sindh | ELISA5 | 396 | 23.5 | [120] |
| Vertical transmission | ||||||
| 8 | 2011 | Karachi | ELISA6 | 129 | 3.9 | [102] |
Acurate Diagnostics;
Medical Biological Services, Italy;
Abbott Diagnostics;
Acon Laboratories;
Biokit;
DiaSorin;
Manufacturer not mentioned in cited reference. KPK: Khyber Pakhtunkhwa; ELISA: Enzyme linked immunosorbent assay; ICT: Immunochromatographic test.
Other high risk groups
Other population subsets are also considered at increased risk of HCV infection (Table 5). These include prison inmates, patients on regular dialysis, as well as the homosexual community. Two reports published in 2010 found the serofrequency of HCV infection among inmates of various prisons in Sindh province to be 12.8% and 18.2% (entries 3 and 4 in Table 5)[117,118]. Among dialysis patients, 28%-29% tested positive for presence of HCV antibodies in their blood (entries 5 and 6 in Table 5)[111,119]. Khanani and colleagues reported that 23.5% of 396 homosexuals/MSMs (males who have sex with males) tested positive for anti-HCV (entry 7, Table 5)[120]. In addition, Aziz et al[102] reported a 4% rate of vertical HCV transmission from infected mothers to newborn children of ages up to 18 mo (entry 8, Table 5).
Patients seeking hospital care
Screening of patients suffering from diseases, which are not considered a direct consequence of HCV infection or do not directly pose an increased risk of contracting HCV infection, except for the risk of nosocomial and iatrogenic transmission, is also an important surveillance strategy. Firstly, it can provide a window into the prevalence in general population and secondly, for an infection like HCV, it can also provide useful insights into the possible risk factors involved in the transmission of this virus. At least thirteen studies reported the prevalence of HCV in patients (Table 6)[88,106,111,121-130]. These patients visited/attended hospitals with various complaints ranging from general mild sickness requiring outpatient care, to major and gynecological surgeries as well as dermatological and urological disorders.
Table 6.
Hepatitis C virus seropositivity among patients other than those with liver disease
| S. # | Year | Place | Method | Sample size | Seroprevalence (%) | Ref. |
| Urological patients | ||||||
| 1 | 2010 | Lahore | ELISA4 | 558 | 13.4 | [130] |
| Major gynecological surgery | ||||||
| 2 | 2009 | Karachi | EIA1 | 548 | 16.2 | [106] |
| Surgery (eye/elective/major) | ||||||
| 3 | 2010 | Sukkur | ICT5 | 913 | 13.8 | [126] |
| 4 | 2011 | KPK | ICT2 | 25 | 8.0 | [111] |
| 5 | 2013 | Kharian | ELISA5 | 554 | 6.4 | [122] |
| Dental surgery | ||||||
| 6 | 2011 | KPK | ICT2 | 35 | 14.28 | [111] |
| Type II diabetes | ||||||
| 7 | 2010 | Multan | ELISA3 | 3000 | 30.2 | [88] |
| Cataract patients | ||||||
| 8 | 2012 | Karachi | ELISA5 | 377 | 11.4 | [127] |
| Dermatological disorders | ||||||
| 9 | 2012 | Karachi/Rawalpindi | ELISA5 | 355 | 9.01 | [128] |
| Tuberculosis patients | ||||||
| 10 | 2013 | Rahim Yar Khan | ELISA4 | 110 | 9.1 | [121] |
| Sexually transmitted infection patients | ||||||
| 11 | 2014 | Faisalabad | ELISA1 | 39780 | 21.99 | [124] |
| Seeking hospital care (Misc diseases/disease not defined) | ||||||
| 12 | 2010 | Bannu | ELISA5 | 25944 | 3.3 | [125] |
| 13 | 2011 | Karachi | ELISA1 | 2965 | 12.8 | [123] |
| 14 | 2011 | Kotli (AJK) | ELISA5 | 9564 | 6.38 | [129] |
Abbott Diagnostics;
Acon Laboratories;
Labkit;
Bio-tech Company Limited, United States;
Manufacturer not mentioned in cited reference. KPK: Khyber Pakhtunkhwa; ELISA: Enzyme linked immunosorbent assay; EIA: Enzyme immunoassay; ICT: Immunochromatographic test.
The results show an alarmingly high rate of HCV prevalence. 14.2% and 16.2% prevalence in patients undergoing dental[111] and gynecological surgeries[106] respectively, clearly points towards a possible high rate of hospital acquired infection. With the exception of the study by Majid et al[125], which showed a 3.3% prevalence in patients at a single hospital in district Bannu, most studies reported prevalence rates much higher than the national prevalence estimated here (6.8%) as well as earlier systematic reviews[16,23,24] and the national survey[21]. A recent report from Faisalabad indicated alarmingly high HCV seropositivity (21.99%) among patients visiting a sexually transmitted infections clinic[124].
COMPARISON OF METHODS USED IN SEROPREVALENCE STUDIES
A variety of methods have been used for the diagnosis of HCV infection. Studies cited in this review used methods ranging from rapid, point of care tests, such as the ICT, to more expensive laboratory conducted assays such as ELISA, EIA, CMIA and CLIA. A recent meta-analysis of at least 30 different studies that compared point of care testing results with those of more advanced laboratory based assays used for HCV diagnosis showed a high pooled accuracy for all studies[131]. However, the same study showed a high degree of heterogeneity in performance of various commercially available point of care tests. Caution therefore must be observed while selecting appropriate rapid HCV diagnosis testing platforms. While it is beyond the scope of this article to recommend certain manufacturer(s) over others, readers are referred to the WHO list of prequalified diagnostics[132] or other studies reporting a direct comparison of different commercially available HCV diagnostic tests (e.g.[133]). Furthermore, although rapid tests like ICT are quite efficient in diagnosing HCV infection with less than 1% false negative rates, such screening tests should not be considered as sole diagnostic criteria, as studies have reported high rate of false positive results[38]. Finally considering the fact that some 15%-45% HCV infected patients may spontaneously clear the virus but still remain seropositive for HCV[30,31], as discussed in preceding paragraphs, a positive anti-HCV test should be followed by nucleic acid testing as per WHO and CDC guidelines[32].
PREVALENCE OF ACTIVE HCV INFECTION
Recent WHO and CDC guidelines recommend NAT directly following a positive anti-HCV test[32], so that an active HCV infection can be differentiated from a false positive or resolved past infection. However, not much attention has been paid to distinguishing active HCV infection from seroprevalence of anti-HCV. Only five studies (Table 7) reported active HCV infection[36,37,45,134,135]. These studies encompassed a combined samples size of 7158 persons. Based on these studies, active HCV infection was found to be approximately 6% in the general population of Pakistan. Active HCV infection ranged from 3.5% in Mansehra[36] to 17.2% in Rawalpindi[135] (Table 7, entries 2 and 3, respectively).
Table 7.
Prevalence of active hepatitis C virus infection in Pakistan
| S. # | Year | Place |
Sample size |
Active HCV infection (%) |
Ref. | ||||
| Male | Female | Total | Male | Female | Total | ||||
| General population | |||||||||
| 1 | 2010 | Swat | 290 | 300 | 590 | 2.8 | 5.7 | 4.2 | [45] |
| 2 | 2010 | Mansehra | 300 | 100 | 400 | 4.0 | 2.0 | 3.5 | [36] |
| 3 | 2012 | Rawalpindi | 147 | 156 | 303 | 17.7 | 16.7 | 17.2 | [135] |
| Islamabad | 75 | 125 | 200 | 5.3 | 3.2 | 4.0 | |||
| 4 | 2013 | Lahore | 1914 | 2332 | 4246 | 5.3 | 4.7 | 4.9 | [134] |
| 5 | 2014 | Mardan | 757 | 662 | 1419 | 11.5 | 5.1 | 8.5 | [37] |
| Intravenous drug users | |||||||||
| 6 | 2011 | KPK | 42 | 14.3 | [111] | ||||
| 7 | 2011 | KPK | 200 | 24.0 | [113] | ||||
| Dialysis patients | |||||||||
| 8 | 2011 | KPK | 25 | 28.0 | [111] | ||||
| 9 | 2011 | KPK | 384 | 27.6 | [119] | ||||
| Blood donors | |||||||||
| 10 | 2011 | KPK/FATA | - | - | 7148 | - | - | 1.6 | [89] |
| Health care workers | |||||||||
| 11 | 2011 | KPK | 824 | 2.8 | [115] | ||||
| Multi transfused population | |||||||||
| 12 | 2011 | KPK | 40 | 15.0 | [111] | ||||
| Patients undergoing major surgery | |||||||||
| 13 | 2011 | KPK | 25 | 8.0 | [111] | ||||
| Dental surgery patients | |||||||||
| 14 | 2011 | KPK | 35 | 14.3 | [111] | ||||
| Pregnant women | |||||||||
| 15 | 2011 | Karachi | 18000 | -1 | [102] | ||||
Out of 18000 subjects studied, 1043 women tested positive for anti- hepatitis C virus (HCV) during screening; only 640 out of these 1043 agreed to undergo nucleic acid testing of which 510 tested positive for HCV-RNA. KPK: Khyber Pakhtunkhwa; FATA: Federally Administered Tribal Areas.
Similarly, only two reports have been published on active HCV infection among IDUs in Pakistan since 2010[111,113]. While Ali and colleagues found 14.3% active HCV infection among a small group of 42 IDUs[111], a study by Rehman et al[113] reported a very high (24%) HCV prevalence among 200 IDUs. Active HCV infection has not been adequately investigated in other population subsets, particularly the high risk groups. Except for dialysis patients, for which two reports are available[111,119], only one report each was published for blood donors[89], health care workers[115], pregnant women[102], multi-transfused patients[111] and patients undergoing major surgery[111]. The results of each of these studies are detailed in Table 7 and show an alarmingly high rate of active HCV infection.
FREQUENCY DISTRIBUTION OF HCV GENOTYPES IN PAKISTAN
Methodologies used for genotyping of HCV isolates
HCV genotype is an important determinant of disease severity and pathogenesis as well as patient response to antiviral therapy. Therefore accurate genotyping of HCV isolates is of fundamental significance. Several HCV genotyping approaches have been reported in the literature and have been reviewed comprehensively elsewhere[136]. Readers are referred to aforementioned review as well as other recent studies (e.g.[137,138]) in order to develop a better understanding of advantages and shortcomings related to each methodology. Studies included in this review mostly relied on PCR based amplification of HCV Core and/or 5’ non-coding region sequences using subtype specific primers. The amplicons thus generated differ in their sizes and genotype/subtype of an isolate can be determined by gel electrophoresis[13,139]. The method originally developed by Ohno and coworkers[13] has been extensively used and most of the studies included in this review[17,18,37,45,115,119,140-149] used this methodology. This methodology was further refined by Idrees in 2008[139] by designing primers based on updated HCV genome sequence data with particular emphasis on isolates from Pakistan. A few of the studies relied on the method developed by Idrees[113,150-154]. Very few studies reported using commercially available genotyping assays. For example Ahmad et al[155] and Ijaz et al[156] used the Invader HCV Genotyping Assay (Third Wave Technologies, Inc., WI, United States) while Akhund and coworkers used a commercially available, type specific PCR amplification kit (AnaGen Technologies Inc., GA, United States)[157].
Frequency distribution of HCV genotypes
Genotyping of HCV isolates from Pakistan has been carried out extensively in the recent past. Twenty-five reports were published between 2010 and 2014 that pertained to the distribution of various HCV genotypes in Pakistan[17,18,37,45,113,115,119,141-158]. However, none of the studies reported the genotype distribution in Balochistan province. Therefore, so as to present a more comprehensive picture of HCV genotype frequency distribution in Pakistan, a 2009 study pertaining to Balochistan province was included[140] (Table 8). A total of 37025 subjects were genotyped in these studies and show a heterogeneous pattern of genotype distribution in various regions of Pakistan. Genotype 3a was found in approximately 61.4% patients as mono-infection, as well as in most of the patients with mixed genotype infection.
Table 8.
Frequency distribution of hepatitis C virus genotypes in Pakistan
| Frequency (%) of hepatitis C virus genotypes | ||||||||||||||||||
|
1 |
2 |
3 |
4 |
5 |
6 |
Mixed | Untypable | Ref. | ||||||||||
| 1a | 1b | U | 2a | 2b | U | 3a | 3b | U | 4a | 4b | U | 5a | U | 6a | U | |||
| 3.5 | 0.8 | - | 1 | - | - | 88.1 | 3 | - | - | - | - | - | - | - | - | 3.6 | - | [142] |
| 6.1 | 6 | - | 15.1 | 6.1 | - | 42.3 | 12.1 | - | - | - | - | - | - | - | - | - | 12.1 | [45] |
| 0.72 | 0.72 | 80.26 | 6 | 6.73 | 27.88 | [151] | ||||||||||||
| 5.4 | 8.1 | 34.1 | 7 | 7.6 | 37.8 | [154] | ||||||||||||
| 1.5 | 2.5 | 39 | 1 | 31 | 8 | 17 | [17] | |||||||||||
| 7.14 | 35.71 | 28.6 | 14.29 | 14.29 | [113] | |||||||||||||
| 12.1 | 1.2 | - | 1.2 | 0.4 | 0.31 | 64.5 | 6.4 | 0.0011 | 6.7 | 0.6 | - | 0.5 | - | 0.4 | - | 3.2 | 2.4 | [156] |
| 14.3 | 3.6 | - | 8.9 | 1.8 | - | 32.1 | 17.8 | 1.8 | 10.7 | 8.9 | [119] | |||||||
| 6.8 | 4.6 | 1.3 | 54.4 | 8.2 | 8.2 | 16.4 | [152] | |||||||||||
| 5.6 | - | - | - | - | - | 90.3 | 0.6 | - | - | - | 0.6 | - | - | - | - | 2.8 | - | [141] |
| 2.6 | 0.8 | - | 0.3 | 0.2 | - | 82.6 | 0.2 | - | - | - | - | 0.1 | - | - | - | 2.4 | 10.8 | [150] |
| 12.5 | 8.9 | 9.8 | 1.8 | 42.9 | 22.3 | 1.8 | [149] | |||||||||||
| 7.4 | 5.8 | - | 13.2 | 6.6 | - | 26.4 | 16.5 | - | - | - | 2.5 | - | - | - | - | 4.1 | 17.4 | [37] |
| 10 | 3.6 | - | - | - | - | 56.4 | 15 | - | - | - | 1.4 | - | - | - | - | 7.1 | 6.4 | [143] |
| 1.3 | 0.7 | - | - | - | - | 82.1 | 13.9 | - | - | - | - | - | - | - | - | 2 | - | [146] |
| 1 | - | - | 12 | - | - | 38.2 | 21 | - | - | - | - | - | - | - | - | 7.3 | 21 | [148] |
| 8.8 | 3 | - | 6.5 | 1 | - | 45.5 | 16 | - | 0.8 | - | - | - | - | - | - | 16 | 2.2 | [145] |
| 5.3 | 5.1 | 11 | 24.9 | 6.1 | - | 39.4 | 6.3 | - | 2.4 | 2.4 | 2 | - | 5.7 | [18] | ||||
| 2.9 | 1.5 | - | - | - | 1.2 | 70.3 | 5.5 | - | - | - | - | - | 0.9 | - | - | 2.6 | 15.1 | [157] |
| 3.3 | 0.8 | 0.21 | 2.1 | 0.2 | 0.021 | 61 | 8.9 | 0.241 | - | - | 0.5 | 0.1 | 0.1 | 4.7 | 17.8 | [153] | ||
| 23.6 | - | - | - | - | - | 55.9 | 3.2 | - | 12.5 | 1.2 | - | - | - | - | - | 1.2 | 2.5 | [155] |
| 4.3 | - | - | - | - | - | 73.9 | 13 | - | - | - | - | - | - | - | - | 4.3 | 4.3 | [115] |
| 0.9 | 0.9 | - | 7.4 | 0.9 | - | 66.1 | 2.6 | - | - | - | - | - | - | - | - | 2.2 | 18.8 | [144] |
| - | - | - | 1.1 | 2.2 | - | 86.8 | 2.2 | - | - | - | - | - | - | - | - | - | 7.7 | [149] |
| 7.1 | - | - | - | - | - | 50 | 10.7 | - | - | - | - | - | - | - | - | - | 32.1 | [140] |
| 0.5 | 1.5 | - | 10.3 | 1.2 | - | 68.3 | 2.6 | - | - | - | - | - | - | - | - | - | 15.6 | [158] |
Subtype C. U: Undefined subtype.
Overall, approximately 12.5% samples could not be assigned a specific genotype or subtype by the methods used, making the proportion of untypable samples higher than all the subtypes except 3a. A province wise break-up of untypable samples revealed the highest levels in samples originating from Balochistan (32.1%) and KPK province (12.6%). Only 2.7% of samples from Punjab could not be typed. It is worthwhile discussing here the diagnostic and therapeutic relevance of a high ratio of untypable samples. Due to the high rate of mutations in the HCV genome, as well as other factors mentioned by Afzal et al[158], the emergence of new subtypes or genetic variants that are untypable by current methods is unavoidable. There is an urgent need not only to upgrade genotyping methodologies by using updated HCV sequence information, but also to develop a consensus reference genotyping method in order to avoid cross-methodology ambiguities. Sequencing of untypable samples can be of great importance in this regard, as it will not only help researchers to upgrade methodologies but might also help in identifying new genotypes/subtypes.
A closer look at the frequency distribution of genotypes other than 3a also indicated a change in the distribution pattern of HCV genotypes in Pakistan. Overall, genotype 3 (69.1%) was the most prevalent genotype in Pakistan, followed by genotypes 1 (7.1%), 2 (4.2%) and 4 (2.2%). Genotypes 5 and 6 both accounted for approximately 0.2% each of the total sample pool and thus are rare in Pakistan. Samples with mixed genotype accounted for 4.2% of total samples. Among subtypes, overall genotype 3a was found in 61.4% of the samples, followed by genotype 3b (7.6%), 1a (5.7%), 2a (3.7%) and 1b (1.4%). The frequency of all the other subtypes (1c, 2b, 2c, 3c, 4b, 5a and 6a) was found to be less than 1% each.
The genotype distribution in each province showed important differences (Figure 2). A higher frequency of genotype 2 was observed in Sindh and KPK province (11.3% and 17.3% respectively), making it the second most prevalent typable genotype in these provinces. The relative frequency distribution of various subtypes differed considerably across Pakistan. Although genotype 3a was found to be the most prevalent subtype in all three provinces for which reports were available (67.7%, 53.9% and 46.9% in Punjab, Sindh and KPK, respectively), genotype 2a emerged as the second most prevalent subtype in typable samples originating from Sindh and KPK provinces (6.06% and 15.1% respectively). In contrast, only 1.9% of samples from Punjab province tested positive for genotype 2a and the second most prevalent subtype after 3a was found to be 1a (10.8%) in this province. Overall the frequency distribution of all subtypes found is shown in Figure 3 while Figure 2 shows a province wise break-down of major HCV genotype distributions. Results from individual studies are summarized in Table 8.
Figure 2.
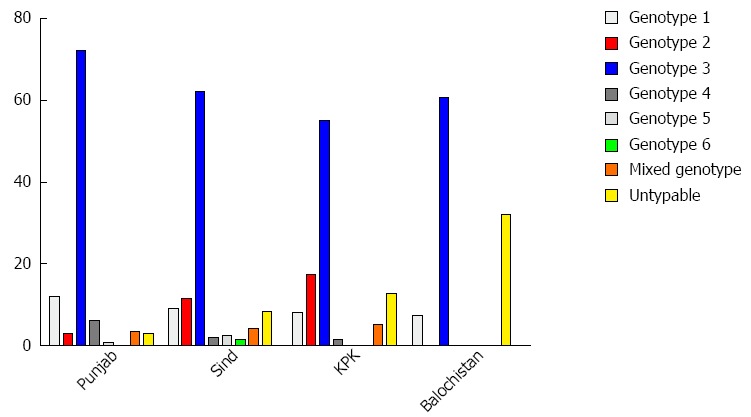
Distribution pattern of major hepatitis C virus genotypes at the province level. KPK: Khyber Pakhtunkhwa.
Figure 3.
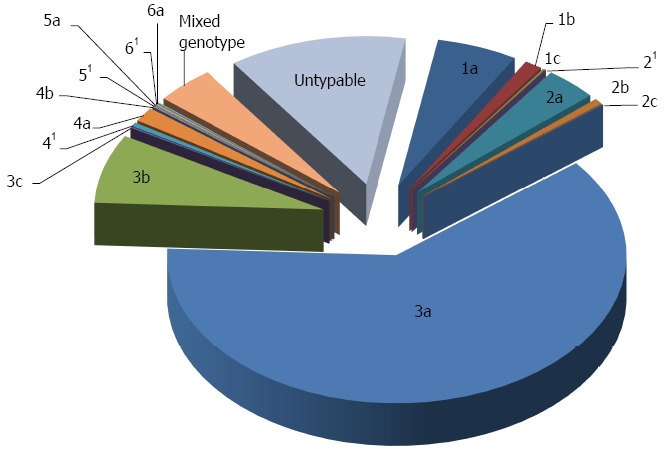
Relative frequency distribution of hepatitis C virus subtypes in Pakistan. 1Undefined subtype.
CONCLUSION
HCV prevalence data published recently (2009/10 to 2015) suggests that HCV infection is on the rise in Pakistan. While the almost 40% increase in HCV seroprevalence among the general population suggested by the analysis here, compared to previous estimates (6.8% rather than 4.7%-5%) is alarming, high prevalence rates among persons who have had surgical and medical interventions suggest a predominant involvement of nosocomial transmission in the spread of HCV in Pakistan. Given the evidence of high nosocomial transmission as well as increased burden of this disease in lesser developed areas (discussed below) where health service related malpractices are more common, there is an urgent need to implement strict measures in order to ensure safe medical practices. Reducing unnecessary injections, ensuring that surgical and dental instruments are sterilized or disposable instruments are used, avoiding shared razors at barber shops as well as unhygienic piercing and tattooing instruments are among the most important preventive measures. Although the response rate to conventional IFN-ribavirin therapy regimen among genotype 3a patients (the most prevalent genotype in Pakistan) is already quite good and with the availability of direct acting antivirals such as Sofosbuvir at reduced prices for patents in Pakistan, it is hoped that HCV can be controlled more effectively.
Reports reviewed in the current study also suggest that there is extremely high HCV prevalence in underdeveloped rural and peri-urban areas. However, much less attention has been paid to this socioeconomic dimension of the HCV epidemic in Pakistan. Considering the fact that a majority of the population of Pakistan resides in these rural areas with high HCV prevalence, it is likely that the actual burden of hepatitis C in Pakistan may be much higher. Undoubtedly, an increased focus is needed to gauge HCV prevalence in rural areas for better evaluation and implementation of preventative strategies. Moreover, in light of recent WHO and CDC guidelines, it is imperative that more effort is invested in determining the prevalence of active HCV infection in Pakistan.
The analysis also showed a shift in relative frequency distribution of HCV subtypes in various regions of Pakistan. Although 3a continues to be the most prevalent genotype, recent years have witnessed an increase in incidence of genotype 2a infection in KPK and Sindh provinces. This temporal change in relative distribution of various genotypes has fundamental implications with regard to translational efforts aimed at limiting and eradicating HCV in Pakistan. The high proportion of samples that could not be assigned to a specific genotype demands improvements in methodologies currently used in order to develop a better understanding of HCV genotype distribution and evolutionary trends in Pakistan.
ACKNOWLEDGMENTS
The authors are grateful to Professor Rob W Briddon for critically reviewing this manuscript. We are also thankful to Mr. Tahir Mehdi and Mr Shoaib Tariq for their help in producing the map of HCV prevalence.
Footnotes
Supported by Higher Education Commission of Pakistan, through Grant No. 20-2056 to Iqbal M.
Conflict-of-interest statement: Authors declare no conflict of interest.
Open-Access: This article is an open-access article which was selected by an in-house editor and fully peer-reviewed by external reviewers. It is distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Peer-review started: May 7, 2015
First decision: September 9, 2015
Article in press: December 14, 2015
P- Reviewer: Afzal MS, Rodriguez-Frias F, Santos-Lopez G, Yoshioka K S- Editor: Gong ZM L- Editor: A E- Editor: Zhang DN
References
- 1.Lavanchy D. Evolving epidemiology of hepatitis C virus. Clin Microbiol Infect. 2011;17:107–115. doi: 10.1111/j.1469-0691.2010.03432.x. [DOI] [PubMed] [Google Scholar]
- 2.Hajarizadeh B, Grebely J, Dore GJ. Epidemiology and natural history of HCV infection. Nat Rev Gastroenterol Hepatol. 2013;10:553–562. doi: 10.1038/nrgastro.2013.107. [DOI] [PubMed] [Google Scholar]
- 3.Armstrong GL, Wasley A, Simard EP, McQuillan GM, Kuhnert WL, Alter MJ. The prevalence of hepatitis C virus infection in the United States, 1999 through 2002. Ann Intern Med. 2006;144:705–714. doi: 10.7326/0003-4819-144-10-200605160-00004. [DOI] [PubMed] [Google Scholar]
- 4.Williams IT, Bell BP, Kuhnert W, Alter MJ. Incidence and transmission patterns of acute hepatitis C in the United States, 1982-2006. Arch Intern Med. 2011;171:242–248. doi: 10.1001/archinternmed.2010.511. [DOI] [PubMed] [Google Scholar]
- 5.Duberg A, Janzon R, Bäck E, Ekdahl K, Blaxhult A. The epidemiology of hepatitis C virus infection in Sweden. Euro Surveill. 2008;13:18882. doi: 10.2807/ese.13.21.18882-en. [DOI] [PubMed] [Google Scholar]
- 6.Delarocque-Astagneau E, Meffre C, Dubois F, Pioche C, Le Strat Y, Roudot-Thoraval F, Hillon P, Silvain C, Dhumeaux D, Desenclos JC. The impact of the prevention programme of hepatitis C over more than a decade: the French experience. J Viral Hepat. 2010;17:435–443. doi: 10.1111/j.1365-2893.2009.01196.x. [DOI] [PubMed] [Google Scholar]
- 7.Chung H, Ueda T, Kudo M. Changing trends in hepatitis C infection over the past 50 years in Japan. Intervirology. 2010;53:39–43. doi: 10.1159/000252782. [DOI] [PubMed] [Google Scholar]
- 8.Razali K, Thein HH, Bell J, Cooper-Stanbury M, Dolan K, Dore G, George J, Kaldor J, Karvelas M, Li J, et al. Modelling the hepatitis C virus epidemic in Australia. Drug Alcohol Depend. 2007;91:228–235. doi: 10.1016/j.drugalcdep.2007.05.026. [DOI] [PubMed] [Google Scholar]
- 9.Lavanchy D. The global burden of hepatitis C. Liver Int. 2009;29 Suppl 1:74–81. doi: 10.1111/j.1478-3231.2008.01934.x. [DOI] [PubMed] [Google Scholar]
- 10.Moradpour D, Penin F, Rice CM. Replication of hepatitis C virus. Nat Rev Microbiol. 2007;5:453–463. doi: 10.1038/nrmicro1645. [DOI] [PubMed] [Google Scholar]
- 11.WHO. Epidemic and pandemic alert and response, Hepatitis C virus. 2003, cited 2014-11. Available from: http://www.who.int/csr/disease/hepatitis/whocdscsrlyo2003/en/index2.html.
- 12.McOmish F, Yap PL, Dow BC, Follett EA, Seed C, Keller AJ, Cobain TJ, Krusius T, Kolho E, Naukkarinen R. Geographical distribution of hepatitis C virus genotypes in blood donors: an international collaborative survey. J Clin Microbiol. 1994;32:884–892. doi: 10.1128/jcm.32.4.884-892.1994. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Ohno O, Mizokami M, Wu RR, Saleh MG, Ohba K, Orito E, Mukaide M, Williams R, Lau JY. New hepatitis C virus (HCV) genotyping system that allows for identification of HCV genotypes 1a, 1b, 2a, 2b, 3a, 3b, 4, 5a, and 6a. J Clin Microbiol. 1997;35:201–207. doi: 10.1128/jcm.35.1.201-207.1997. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Li CS, Chan PK, Tang JW. Molecular epidemiology of hepatitis C genotype 6a from patients with chronic hepatitis C from Hong Kong. J Med Virol. 2009;81:628–633. doi: 10.1002/jmv.21430. [DOI] [PubMed] [Google Scholar]
- 15.Hamid S, Umar M, Alam A, Siddiqui A, Qureshi H, Butt J. PSG consensus statement on management of hepatitis C virus infection--2003. J Pak Med Assoc. 2004;54:146–150. [PubMed] [Google Scholar]
- 16.Waheed Y, Shafi T, Safi SZ, Qadri I. Hepatitis C virus in Pakistan: a systematic review of prevalence, genotypes and risk factors. World J Gastroenterol. 2009;15:5647–5653. doi: 10.3748/wjg.15.5647. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Ali S, Ali I, Azam S, Ahmad B. Frequency distribution of HCV genotypes among chronic hepatitis C patients of Khyber Pakhtunkhwa. Virol J. 2011;8:193. doi: 10.1186/1743-422X-8-193. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Khan N, Akmal M, Hayat M, Umar M, Ullah A, Ahmed I, Rahim K, Ali S, Bahadar S, Saleha S. Geographic distribution of hepatitis C virus genotypes in pakistan. Hepat Mon. 2014;14:e20299. doi: 10.5812/hepatmon.20299. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Guerra J, Garenne M, Mohamed MK, Fontanet A. HCV burden of infection in Egypt: results from a nationwide survey. J Viral Hepat. 2012;19:560–567. doi: 10.1111/j.1365-2893.2011.01576.x. [DOI] [PubMed] [Google Scholar]
- 20.Mohamoud YA, Mumtaz GR, Riome S, Miller D, Abu-Raddad LJ. The epidemiology of hepatitis C virus in Egypt: a systematic review and data synthesis. BMC Infect Dis. 2013;13:288. doi: 10.1186/1471-2334-13-288. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Qureshi H, Bile KM, Jooma R, Alam SE, Afridi HU. Prevalence of hepatitis B and C viral infections in Pakistan: findings of a national survey appealing for effective prevention and control measures. East Mediterr Health J. 2010;16 Suppl:S15–S23. [PubMed] [Google Scholar]
- 22.Centers for Disease Control and Prevention (CDC) Establishment of a viral hepatitis surveillance system--Pakistan, 2009-2011. MMWR Morb Mortal Wkly Rep. 2011;60:1385–1390. [PubMed] [Google Scholar]
- 23.Umar M, Bushra HT, Ahmad M, Data A, Ahmad M, Khurram M, Usman S, Arif M, Adam T, Minhas Z, et al. Hepatitis C in Pakistan: a review of available data. Hepat Mon. 2010;10:205–214. [PMC free article] [PubMed] [Google Scholar]
- 24.Bosan A, Qureshi H, Bile KM, Ahmad I, Hafiz R. A review of hepatitis viral infections in Pakistan. J Pak Med Assoc. 2010;60:1045–1058. [PubMed] [Google Scholar]
- 25.Abbas S, Ali M, Muhammad A, Shaw S, Abbas S. Frequency of HCV infection and its genotypes among patients attending a liver clinic and voluntary blood donors in a rural area of pakistan. Pak J Med Sci. 2009;25:579–582. [Google Scholar]
- 26.Ahmed F, Irving WL, Anwar M, Myles P, Neal KR. Prevalence and risk factors for hepatitis C virus infection in Kech District, Balochistan, Pakistan: most infections remain unexplained. A cross-sectional study. Epidemiol Infect. 2012;140:716–723. doi: 10.1017/S0950268811001087. [DOI] [PubMed] [Google Scholar]
- 27.Khan A, Tareen AM, Ikram A, Rahman H, Wadood A, Qasim M, Khan K. Prevalence of HCV among the young male blood donors of Quetta region of Balochistan, Pakistan. Virol J. 2013;10:83. doi: 10.1186/1743-422X-10-83. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Janjua NZ, Hamza HB, Islam M, Tirmizi SF, Siddiqui A, Jafri W, Hamid S. Health care risk factors among women and personal behaviours among men explain the high prevalence of hepatitis C virus infection in Karachi, Pakistan. J Viral Hepat. 2010;17:317–326. doi: 10.1111/j.1365-2893.2009.01230.x. [DOI] [PubMed] [Google Scholar]
- 29.Aziz S, Khanani R, Noorulain W, Rajper J. Frequency of hepatitis B and C in rural and periurban Sindh. J Pak Med Assoc. 2010;60:853–857. [PubMed] [Google Scholar]
- 30.Gerlach JT, Diepolder HM, Zachoval R, Gruener NH, Jung MC, Ulsenheimer A, Schraut WW, Schirren CA, Waechtler M, Backmund M, et al. Acute hepatitis C: high rate of both spontaneous and treatment-induced viral clearance. Gastroenterology. 2003;125:80–88. doi: 10.1016/s0016-5085(03)00668-1. [DOI] [PubMed] [Google Scholar]
- 31.Thomson EC, Fleming VM, Main J, Klenerman P, Weber J, Eliahoo J, Smith J, McClure MO, Karayiannis P. Predicting spontaneous clearance of acute hepatitis C virus in a large cohort of HIV-1-infected men. Gut. 2011;60:837–845. doi: 10.1136/gut.2010.217166. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.WHO Guidelines Approved by the Guidelines Review Committee. Guidelines for the Screening, Care and Treatment of Persons with Hepatitis C Infection. Geneva: World Health Organization; 2014. [PubMed] [Google Scholar]
- 33.Petrelli E, Manzin A, Paolucci S, Cioppi A, Brugia M, Muretto P, Clementi M. Chronic liver disease and active hepatitis C virus infection in patients with antibodies to this virus. J Clin Pathol. 1994;47:148–151. doi: 10.1136/jcp.47.2.148. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Abbas M, Hussain MF, Raza S, Shazi L. Frequency and awareness of hepatitis B and C in visitors of Hepatitis Awareness Mela. J Pak Med Assoc. 2010;60:1069–1071. [PubMed] [Google Scholar]
- 35.Abdullah F, Pasha H, Memon A, Shah U. Increasing frequency of anti-hcv seropositivity in a cross-section of people in Karachi, Pakistan. Pak J Med Sci. 2011;27:767–770. [Google Scholar]
- 36.Ali A, Ahmad H, Ali I, Khan S, Zaidi G, Idrees M. Prevalence of active hepatitis c virus infection in district Mansehra Pakistan. Virol J. 2010;7:334. doi: 10.1186/1743-422X-7-334. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Ali S, Ahmad A, Khan RS, Khan S, Hamayun M, Khan SA, Iqbal A, Khan AA, Wadood A, Ur Rahman T, et al. Genotyping of HCV RNA reveals that 3a is the most prevalent genotype in mardan, pakistan. Adv Virol. 2014;2014:606201. doi: 10.1155/2014/606201. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Batool A, Khan MI, Bano KA. Efficacy of immunoassay chromatography test for hepatitis-C antibodies detection. J Ayub Med Coll Abbottabad. 2009;21:38–39. [PubMed] [Google Scholar]
- 39.Hafeez-ud-din TS, Lahrasab W, Sharif MA. Prevalence of hepatitis B and C in healthy adult males of paramilitary personnel in Punjab. J Ayub Med Coll Abbottabad. 2012;24:138–140. [PubMed] [Google Scholar]
- 40.Hashmi A, Saleem K, Soomro JA. Prevalence and factors associated with hepatitis C virus seropositivity in female individuals in islamabad, pakistan. Int J Prev Med. 2010;1:252–256. [PMC free article] [PubMed] [Google Scholar]
- 41.Hyder O, Ijaz M, Arshad MA, Zahira T. Age-specific frequency of screen-detected hepatitis C virus seropositivity in men from the Punjab province of Pakistan. J Med Screen. 2010;17:214–216. doi: 10.1258/jms.2010.010101. [DOI] [PubMed] [Google Scholar]
- 42.Ilyas M, Ahmad I. Chemiluminescent microparticle immunoassay based detection and prevalence of HCV infection in district Peshawar Pakistan. Virol J. 2014;11:127. doi: 10.1186/1743-422X-11-127. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Ilyas M, Iftikhar M, Rasheed U. Prevalence of hepatitis B and hepatitis C in populations of college students in Gujranwala. Biologia (Pakistan) 2011;57:89–95. [Google Scholar]
- 44.Jamil MS, Ali H, Shaheen R, Basit A. Prevalence, knowledge and awareness of hepatitis C among residents of three Union Councils in Mansehra. J Ayub Med Coll Abbottabad. 2010;22:192–196. [PubMed] [Google Scholar]
- 45.Rauf A, Nadeem MS, Ali A, Iqbal M, Mustafa M, Latif MM, Latif MZ, Ahmed N, Shakoori AR. Prevalence of hepatitis B and C in internally displaced persons of war against terrorism in Swat, Pakistan. Eur J Public Health. 2011;21:638–642. doi: 10.1093/eurpub/ckq084. [DOI] [PubMed] [Google Scholar]
- 46.Shaikh FH, Ali Abro H, Ali Chhutto M, Abbasi PA, Shaikh AW, Ali Buriro S. Hepatitis C: frequency and risk factors associated with sero-positivity among adults in Larkana City. J Ayub Med Coll Abbottabad. 2009;21:107–109. [PubMed] [Google Scholar]
- 47.Ahmad A. Frequency of HBV surface antigen and anti-HCV in healthy voluntary blood donors in Swat district. J Postgrad Med Inst. 2006;20:187–190. [Google Scholar]
- 48.Idrees M, Lal A, Naseem M, Khalid M. High prevalence of hepatitis C virus infection in the largest province of Pakistan. J Dig Dis. 2008;9:95–103. doi: 10.1111/j.1751-2980.2008.00329.x. [DOI] [PubMed] [Google Scholar]
- 49.Idrees M, Riazuddin S. Frequency distribution of hepatitis C virus genotypes in different geographical regions of Pakistan and their possible routes of transmission. BMC Infect Dis. 2008;8:69. doi: 10.1186/1471-2334-8-69. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50.Abbas Z, Jeswani NL, Kakepoto GN, Islam M, Mehdi K, Jafri W. Prevalence and mode of spread of hepatitis B and C in rural Sindh, Pakistan. Trop Gastroenterol. 2008;29:210–216. [PubMed] [Google Scholar]
- 51.Agboatwalla M, Isomura S, Miyake K, Yamashita T, Morishita T, Akram DS. Hepatitis A, B and C seroprevalence in Pakistan. Indian J Pediatr. 1994;61:545–549. doi: 10.1007/BF02751716. [DOI] [PubMed] [Google Scholar]
- 52.Ahmad N, Asgher M, Shafique M, Qureshi JA. An evidence of high prevalence of Hepatitis C virus in Faisalabad, Pakistan. Saudi Med J. 2007;28:390–395. [PubMed] [Google Scholar]
- 53.Alam M, Tariq W, Akram S, Qureshi T. Frequency of Hepatitis B and C in central Punjab. Pak J Pathol. 2006;17:140–141. [Google Scholar]
- 54.Alam M, Tariq W, Saleem J, Akram S. Ethnic and geographical distribution of HBsAg and anti-HCV in recruits belonging to Mianwali district. P. ak J Pathol. 2008;19:3–5. [Google Scholar]
- 55.Ali N, Khattak J, Anwar M, Tariq WZ, Nadeem M, Irfan M. Prevalence of hepatitis B surface antigen and hepatitis C antibodies in young healthy adults. Pak J Pathol. 2002;13:3–6. [Google Scholar]
- 56.Altaf C, Akhtar S, Qadir A, Malik K, Ahmed P, Tariq W. Frequency of Hepatitis B and C among healthy adult males from Central Sindh. Pak J Pathol. 2007;18:113–115. [Google Scholar]
- 57.Amin J, Yousuf H, Mumtaz A, Iqbal M, Ahmed R, Adhami S, Malik K. Prevalence of Hepatitis B Surface Antigen and anti Hepatitis C virus. Professional Med J. 2004;11:334–337. [Google Scholar]
- 58.Anwar M, Bokhari S. Prevalence of Anti-HCV Antibodies in Patients with Suspected Liver Disease. Biomedica. 1999;15:80–84. [Google Scholar]
- 59.Aslam M, Aslam J. Seroprevalence of the antibody to hepatitis C in select groups in the Punjab region of Pakistan. J Clin Gastroenterol. 2001;33:407–411. doi: 10.1097/00004836-200111000-00013. [DOI] [PubMed] [Google Scholar]
- 60.Bhatti S, Quraishi M, Mahmood CZ, Javaid K. Seroprevalence of HBsAg and HCV antibodies in healthy individuals of high socioeconomic status. Biomedica. 2007;23:131–133. [Google Scholar]
- 61.Butt T, Amin MS. Seroprevalence of hepatitis B and C infections among young adult males in Pakistan. East Mediterr Health J. 2008;14:791–797. [PubMed] [Google Scholar]
- 62.Farooq M, Iqbal M, Tariq W, Hussain A, Ghani I. Prevalence of Hepatitis B and C in a healthy cohort. Pak J Pathol. 2005;16:42–46. [Google Scholar]
- 63.Farooqi JI, Farooqi RJ, Khan NM. Frequency of hepatitis B and C in selected groups of population in NWFP. J Postgrad Med Inst. 2007;21:165–168. [Google Scholar]
- 64.Fayyaz M, Qazi MA, Ishaq M, Chaudhary GM, Bukhari MH. Frequency of hepatitis B and C seropositivity in prisoners. Biomedica. 2006;22:55–58. [Google Scholar]
- 65.Hakim S, Kazmi S, Bagasra O. Seroprevalence of hepatitis B and C genotypes among young apparently healthy females of karachi-pakistan. Libyan J Med. 2008;3:66–70. doi: 10.4176/071123. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 66.Hashim R, Hussain A, Rehman K. Seroprevalence of Hepatitis-C virus antibodies among healthy young men in Pakistan. Pak J Med Res. 2005;44:140–142. [Google Scholar]
- 67.Jafri W, Jafri N, Yakoob J, Islam M, Tirmizi SF, Jafar T, Akhtar S, Hamid S, Shah HA, Nizami SQ. Hepatitis B and C: prevalence and risk factors associated with seropositivity among children in Karachi, Pakistan. BMC Infect Dis. 2006;6:101. doi: 10.1186/1471-2334-6-101. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 68.Khan MSA, Khalid M, Ayub N, Javed M. Seroprevalence and risk factors of hepatitis C virus (HCV) in Mardan, NWFP: a hospital based study. Rawal Med J. 2004;29:57–60. [Google Scholar]
- 69.Khan S, Rai MA, Khan A, Farooqui A, Kazmi SU, Ali SH. Prevalence of HCV and HIV infections in 2005-Earthquake-affected areas of Pakistan. BMC Infect Dis. 2008;8:147. doi: 10.1186/1471-2334-8-147. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 70.Khokhar N, Gill ML, Malik GJ. General seroprevalence of hepatitis C and hepatitis B virus infections in population. J Coll Physicians Surg Pak. 2004;14:534–536. [PubMed] [Google Scholar]
- 71.Luby SP, Qamruddin K, Shah AA, Omair A, Pahsa O, Khan AJ, McCormick JB, Hoodbhouy F, Fisher-Hoch S. The relationship between therapeutic injections and high prevalence of hepatitis C infection in Hafizabad, Pakistan. Epidemiol Infect. 1997;119:349–356. doi: 10.1017/s0950268897007899. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 72.Malik N, Butt T, Mansoor N, Khan T, Akbar M, Aslam M. Percentage of hepatitis B and C among young adult males from interior Sindh. Pak Armed Forces Med J. 2008;58:260–266. [Google Scholar]
- 73.Mirza I, Mirza S, Irfan S, Siddiqi R, Tariq W, Janjua A. Seroprevalence of Hepatitis B and C in young adults seeking recruitment in armed forces. Pak Armed Forces Med J. 2006;56:192–197. [Google Scholar]
- 74.Mirza IA, Kazmi SM, Janjua AN. Frequency of hepatitis B surface antigen and anti- HCV in young adults--experience in Southern Punjab. J Coll Physicians Surg Pak. 2007;17:114–115. [PubMed] [Google Scholar]
- 75.Muhammad N, Jan MA. Frequency of hepatitis “C” in Buner, NWFP. J Coll Physicians Surg Pak. 2005;15:11–14. [PubMed] [Google Scholar]
- 76.Parker SP, Khan HI, Cubitt WD. Detection of antibodies to hepatitis C virus in dried blood spot samples from mothers and their offspring in Lahore, Pakistan. J Clin Microbiol. 1999;37:2061–2063. doi: 10.1128/jcm.37.6.2061-2063.1999. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 77.Sherif T, Tariq W. Seroprevalence of Hepatitis B and C in healthy adult male recruits. Pak J Pathol. 2006;17:147–150. [Google Scholar]
- 78.Sultana N, Bari A, Qazalbash AA. Prevalence of anti-HCV antibodies in patients with liver disease and normal population. Pak J Med Res. 1999;38:106–111. [Google Scholar]
- 79.Tanveer A, Batool K, Qureshi AW. Prevalence of hepatitis B and c in university of the Punjab, Quaid-e-azam campus, Lahore. ARPN J Agri and Bio Sci. 2008;3:30–32. [Google Scholar]
- 80.Zaman R. Prevalence of Hepatitis B and Hepatitis C Viruses in Human Urban Population of Bahawalpur District, Pakistan. J Med Sci. 2006;6:367–373. [Google Scholar]
- 81.SBTP. Safe Blood Transfusion Programme. 2015. Available from: http://www.sbtp.gov.pk/
- 82.Akhtar AM, Khan MA, Ijaz T, Iqbal Z, Rana MY, Maqbool A, Rehman A. Seroprevalence and determinants of hepatitis-C Virus infection in blood donors of Lahore, Pakistan. Pak J Zool. 2013;45:1–7. [Google Scholar]
- 83.Ansari SH, Shamsi TS, Khan MT, Perveen K, Farzana T, Erum S, Ansari I. Seropositivity of hepatitis C, hepatitis B and HIV in chronically transfused β-thalassaemia major patients. J Coll Physicians Surg Pak. 2012;22:610–611. [PubMed] [Google Scholar]
- 84.Attaullah S, Khan S, Khan J. Trend of transfusion transmitted infections frequency in blood donors: provide a road map for its prevention and control. J Transl Med. 2012;10:20. doi: 10.1186/1479-5876-10-20. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 85.Bhutta A, Tahir Z, Ayub S, Mushtaq S. Seroprevalence of anti-hcv in non-professional blood donors. Pak J Med Health Sci. 2012;6:175–178. [Google Scholar]
- 86.Borhany M, Shamsi T, Boota S, Ali H, Tahir N, Naz A, Naseer I, Farzana T, Ansari S, Nadeem M, et al. Transfusion transmitted infections in patients with hemophilia of Karachi, Pakistan. Clin Appl Thromb Hemost. 2011;17:651–655. doi: 10.1177/1076029611398122. [DOI] [PubMed] [Google Scholar]
- 87.Irfan SM, Uddin J, Zaheer HA, Sultan S, Baig A. Trends in transfusion transmitted infections among replacement blood donors in karachi, pakistan. Turk J Haematol. 2013;30:163–167. doi: 10.4274/Tjh.2012.0132. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 88.Jadoon NA, Shahzad MA, Yaqoob R, Hussain M, Ali N. Seroprevalence of hepatitis C in type 2 diabetes: evidence for a positive association. Virol J. 2010;7:304. doi: 10.1186/1743-422X-7-304. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 89.Khan NU, Ali I, Ahmad NU, Iqbal A, Rehman LU, Munir I, Rehman MU, Khan S, Ali S, Siddique L, et al. Prevalence of active HCV infection among the blood donors of Khyber Pakhtunkwa and FATA region of Pakistan and evaluation of the screening tests for anti-HCV. Virol J. 2011;8:154. doi: 10.1186/1743-422X-8-154. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 90.Moiz B, Moatter T, Shaikh U, Adil S, Ali N, Mahar F, Shamsuddin N, Khurshid M. Estimating window period blood donations for human immunodeficiency virus Type 1, hepatitis C virus, and hepatitis B virus by nucleic acid amplification testing in Southern Pakistan. Transfusion. 2014;54:1652–1659. doi: 10.1111/trf.12521. [DOI] [PubMed] [Google Scholar]
- 91.Safi SZ, Afzal MS, Waheed Y, Butt UJ, Fatima K, Parvez Y, Qadri I. Seroprevalence of hepatitis C and human immunodeficiency viruses in blood donors of northwestern Pakistan. Asian Biomed. 2011;5:389–392. [Google Scholar]
- 92.Shah SM, Khattak IU, Ali A, Tariq M. Seropositivity for hepatitis B and C in voluntary blood donors. J Ayub Med Coll Abbottabad. 2010;22:149–151. [PubMed] [Google Scholar]
- 93.Ferlay J, Shin HR, Bray F, Forman D, Mathers C, Parkin DM. Estimates of worldwide burden of cancer in 2008: GLOBOCAN 2008. Int J Cancer. 2010;127:2893–2917. doi: 10.1002/ijc.25516. [DOI] [PubMed] [Google Scholar]
- 94.Ahmed W, Qureshi H, Arif A, Alam SE. Changing trend of viral hepatitis--”A twenty one year report from Pakistan Medical Research Council Research Centre, Jinnah Postgraduate Medical Centre, Karachi”. J Pak Med Assoc. 2010;60:86–89. [PubMed] [Google Scholar]
- 95.Butt AS, Hamid S, Wadalawala AA, Ghufran M, Javed AA, Farooq O, Ahmed B, Ul Haq T, Jafri W. Hepatocellular carcinoma in Native South Asian Pakistani population; trends, clinico-pathological characteristics & differences in viral marker negative & viral-hepatocellular carcinoma. BMC Res Notes. 2013;6:137. doi: 10.1186/1756-0500-6-137. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 96.Munaf A, Memon MS, Kumar P, Ahmed S, Kumar MB. Comparison of viral hepatitis-associated hepatocellular carcinoma due to HBV and HCV - cohort from liver clinics in Pakistan. Asian Pac J Cancer Prev. 2014;15:7563–7567. doi: 10.7314/apjcp.2014.15.18.7563. [DOI] [PubMed] [Google Scholar]
- 97.Idrees M, Rafique S, Rehman I, Akbar H, Yousaf MZ, Butt S, Awan Z, Manzoor S, Akram M, Aftab M, et al. Hepatitis C virus genotype 3a infection and hepatocellular carcinoma: Pakistan experience. World J Gastroenterol. 2009;15:5080–5085. doi: 10.3748/wjg.15.5080. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 98.Khan A, Tanaka Y, Azam Z, Abbas Z, Kurbanov F, Saleem U, Hamid S, Jafri W, Mizokami M. Epidemic spread of hepatitis C virus genotype 3a and relation to high incidence of hepatocellular carcinoma in Pakistan. J Med Virol. 2009;81:1189–1197. doi: 10.1002/jmv.21466. [DOI] [PubMed] [Google Scholar]
- 99.Khan P, Ahmad A, Muhammad N, Khan TM, Ahmad B. Screening of 110 cirrhotic patients for hepatitis B and C at Saidu Teaching Hospital Saidu Sharif Swat. J Ayub Med Coll Abbottabad. 2009;21:119–121. [PubMed] [Google Scholar]
- 100.Devrajani BR, Shah SZ, Devrajani T, Kumar D. Precipitating factors of hepatic encephalopathy at a tertiary care hospital Jamshoro, Hyderabad. J Pak Med Assoc. 2009;59:683–686. [PubMed] [Google Scholar]
- 101.Khan J, Shafiq M, Mushtaq S, Ayaz S, Ullah R, AbdEI-Salam NM, Fouad H, Wasim MA. Seropositivity and coinfection of hepatitis B and C among patients seeking hospital care in Islamabad, Pakistan. Biomed Res Int. 2014;2014:516859. doi: 10.1155/2014/516859. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 102.Aziz S, Hossain N, Karim SA, Rajper J, Soomro N, Noorulain W, Qamar R, Khanani R. Vertical transmission of hepatitis C virus in low to middle socio-economic pregnant population of Karachi. Hepatol Int. 2011;5:677–680. doi: 10.1007/s12072-010-9229-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 103.Bibi S, Dars S, Ashfaq S, Ara Qazi R, Akhund S. Seroprevalence and risk factors for hepatitis C virus (HCV) infection in pregnant women attending public sector tertiary care hospital in Hyderabad Sindh. Pak J Med Sci. 2013;29:505–508. doi: 10.12669/pjms.292.3211. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 104.Gul N, Sarwar J, Idris M, Farid J, Rizvi F, Suleman M, Shah SH. Seroprevalence of hepatitis C in pregnant females of Hazara division. J Ayub Med Coll Abbottabad. 2009;21:83–86. [PubMed] [Google Scholar]
- 105.Khattak ST, Ali Marwat M, Khattak Iu, Khan TM, Naheed T. Comparison of frequency of hepatitis B and hepatitis C in pregnant women in urban and rural area of district Swat. J Ayub Med Coll Abbottabad. 2009;21:12–15. [PubMed] [Google Scholar]
- 106.Sami S, Korejo R, Bhutta SZ. Prevalence of hepatitis B and C: a Jinnah Postgraduate Medical Centre experience. J Obstet Gynaecol Res. 2009;35:533–538. doi: 10.1111/j.1447-0756.2008.00991.x. [DOI] [PubMed] [Google Scholar]
- 107.Taseer IU, Ishaq F, Hussain L, Safdar S, Mirbahar AM, Faiz SA. Frequency of anti-HCV, HBsAg and related risk factors in pregnant women at Nishtar Hospital, Multan. J Ayub Med Coll Abbottabad. 2010;22:13–16. [PubMed] [Google Scholar]
- 108.Asif N, Zafar T, Hassan K, Naseem L. Seroprevalence Anti HCV Antibodies, HCV-RNA and its Genotypes among Patients of Hemophilia, at Hemophilia Treatment Centre Pakistan Institute of Medical Sciences, Islamabad. Int J Pathol. 2009;7:84–87. [Google Scholar]
- 109.Din G, Malik S, Ali I, Ahmed S, Dasti JI. Prevalence of hepatitis C virus infection among thalassemia patients: a perspective from a multi-ethnic population of Pakistan. Asian Pac J Trop Med. 2014;7S1:S127–S133. doi: 10.1016/S1995-7645(14)60218-2. [DOI] [PubMed] [Google Scholar]
- 110.Sajid R, Khalid S, Mazari N, Azhar WB, Khurshid M. Clinical audit of inherited bleeding disorders in a developing country. Indian J Pathol Microbiol. 2010;53:50–53. doi: 10.4103/0377-4929.59183. [DOI] [PubMed] [Google Scholar]
- 111.Ali I, Siddique L, Rehman LU, Khan NU, Iqbal A, Munir I, Rashid F, Khan SU, Attache S, Swati ZA, et al. Prevalence of HCV among the high risk groups in Khyber Pakhtunkhwa. Virol J. 2011;8:296. doi: 10.1186/1743-422X-8-296. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 112.UNODC. Drug Use in Pakistan. 2013. Available from: http://www.unodc.org/documents/pakistan//Survey_Report_Final_2013.pdf.
- 113.ur Rehman L, Ullah I, Ali I, Khan IA, Iqbal A, Khan S, Khan SH, Zaman KU, ullah Khan N, Swati ZA, et al. Active hepatitis C infection and HCV genotypes prevalent among the IDUs of Khyber Pakhtunkhwa. Virol J. 2011;8:327. doi: 10.1186/1743-422X-8-327. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 114.Hamid SS, Farooqui B, Rizvi Q, Sultana T, Siddiqui AA. Risk of transmission and features of hepatitis C after needlestick injuries. Infect Control Hosp Epidemiol. 1999;20:63–64. doi: 10.1086/501547. [DOI] [PubMed] [Google Scholar]
- 115.Khan S, Attaullah S, Ayaz S, Niaz Khan S, Shams S, Ali I, Bilal M, Siraj S. Molecular epidemiology of hcv among health care workers of khyber pakhtunkhwa. Virol J. 2011;8:105. doi: 10.1186/1743-422X-8-105. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 116.Sarwar J, Gul N, Idris M, Anis-ur-Rehman J, Adeel MY. Seroprevalence of hepatitis B and hepatitis C in health care workers in Abbottabad. J Ayub Med Coll Abbottabad. 2008;20:27–29. [PubMed] [Google Scholar]
- 117.Gorar ZA, Zulfikar I. Seropositivity of hepatitis C in prison inmates of Pakistan--a cross sectional study in prisons of Sindh. J Pak Med Assoc. 2010;60:476–479. [PubMed] [Google Scholar]
- 118.Kazi AM, Shah SA, Jenkins CA, Shepherd BE, Vermund SH. Risk factors and prevalence of tuberculosis, human immunodeficiency virus, syphilis, hepatitis B virus, and hepatitis C virus among prisoners in Pakistan. Int J Infect Dis. 2010;14 Suppl 3:e60–e66. doi: 10.1016/j.ijid.2009.11.012. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 119.Khan S, Attaullah S, Ali I, Ayaz S, Naseemullah SN, Siraj S, Khan J. Rising burden of Hepatitis C Virus in hemodialysis patients. Virol J. 2011;8:438. doi: 10.1186/1743-422X-8-438. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 120.Khanani MR, Somani M, Khan S, Naseeb S, Ali SH. Prevalence of single, double, and triple infections of HIV, HCV and HBV among the MSM community in Pakistan. J Infect. 2010;61:507–509. doi: 10.1016/j.jinf.2010.09.035. [DOI] [PubMed] [Google Scholar]
- 121.Akhtar J, Qamar MU, Hakeem A, Waheed A, Sarwar F, Anwar J. Sero-prevalence of HBV and HCV in Tuberculous Patients at Sheikh Zayed Hospital Rahim Yar Khan, Pakistan. Biomedica. 2013;29:70. [Google Scholar]
- 122.Hameed A. Frequency of hepatitis B & C in elective eye surgery. RMJ. 2013;38:15–17. [Google Scholar]
- 123.Khan RAW, Ahmed W, Alam SE, Arif A. Screening of HBsAg and anti HCV from tertiary care, private and public sector hospitals. Pak J Med Res. 2011:50. [Google Scholar]
- 124.Maan MA, Hussain F, Jamil M. Epidemiology of hepatitis C viral infection in Faisalabad, Pakistan: a retrospective study (2010-2012) Afr Health Sci. 2014;14:810–815. doi: 10.4314/ahs.v14i4.6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 125.Majid A, Khan MS, Ullah S. Rising prevalence of Hepatitis B and C and risk factors at District Headquarter Teaching Hospital Bannu, Khyber-Pakhtunkhwa. J Coll Physicians Surg Pak. 2010;20:492–493. [PubMed] [Google Scholar]
- 126.Memon MR, Shaikh AA, Soomro AA, Arshad S, Shah QA. Frequency of hepatitis B and C in patients undergoing elective surgery. J Ayub Med Coll Abbottabad. 2010;22:167–170. [PubMed] [Google Scholar]
- 127.Naeem SS, Siddiqui EU, Kazi AN, Khan S, Abdullah FE, Adhi I. Prevalence of hepatitis ‘B’ and hepatitis ‘C’ among preoperative cataract patients in Karachi. BMC Res Notes. 2012;5:492. doi: 10.1186/1756-0500-5-492. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 128.Rahman A, Rizvi SD, Sheikh ZI. Frequency of HCV infection in different dermatological disorders. J Ayub Med Coll Abbottabad. 2012;24:58–61. [PubMed] [Google Scholar]
- 129.Saleem M, Ahmad W, Sarwar J, Jamshed F, Gul N, Idrees M. Frequency of hepatitis C in asymptomatic patients in District Headquarters Hospital Kotli, Azad Kashmir. J Ayub Med Coll Abbottabad. 2011;23:59–62. [PubMed] [Google Scholar]
- 130.Waheed A, Zafar-ul-Ahsan FA, Shariff MM, Qayyum A. Operating in a yellow nation; the frequency of hepatitis B and hepatitis C positive at a tertiary care teaching hospital. J Pak Med Assoc. 2010;60:1058–1060. [PubMed] [Google Scholar]
- 131.Khuroo MS, Khuroo NS, Khuroo MS. Diagnostic accuracy of point-of-care tests for hepatitis C virus infection: a systematic review and meta-analysis. PLoS One. 2015;10:e0121450. doi: 10.1371/journal.pone.0121450. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 132.WHO. Hepatitis C test kit evaluations. 2001, cited 2015-8-31. Available from: http://www.who.int/diagnostics_laboratory/evaluations/hepc/en/
- 133.Hayder I, Ahmed W, Alam SE. Comparison of Different ICT Kits for HBsAg and Anti HCV Using Gold Standard ELISA. Pak J Med Res. 2012;51:72–76. [Google Scholar]
- 134.Anwar MI, Rahman M, Hassan MU, Iqbal M. Prevalence of active hepatitis C virus infections among general public of Lahore, Pakistan. Virol J. 2013;10:351. doi: 10.1186/1743-422X-10-351. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 135.Satti R, Mustafa F, Khan MI, Haq TS, Khan ZU, Zubair M, ur Rasool ST, Azam M, Ajmal M, Qamar R. Prevalence of Hepatitis C Virus in Urban Ghettos of Twin Cities. Pakistan J Zool. 2012;44:937–943. [Google Scholar]
- 136.Weck K. Molecular methods of hepatitis C genotyping. Expert Rev Mol Diagn. 2005;5:507–520. doi: 10.1586/14737159.5.4.507. [DOI] [PubMed] [Google Scholar]
- 137.Cai Q, Zhao Z, Liu Y, Shao X, Gao Z. Comparison of three different HCV genotyping methods: core, NS5B sequence analysis and line probe assay. Int J Mol Med. 2013;31:347–352. doi: 10.3892/ijmm.2012.1209. [DOI] [PubMed] [Google Scholar]
- 138.Qiu P, Stevens R, Wei B, Lahser F, Howe AY, Klappenbach JA, Marton MJ. HCV genotyping from NGS short reads and its application in genotype detection from HCV mixed infected plasma. PLoS One. 2015;10:e0122082. doi: 10.1371/journal.pone.0122082. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 139.Idrees M. Development of an improved genotyping assay for the detection of hepatitis C virus genotypes and subtypes in Pakistan. J Virol Methods. 2008;150:50–56. doi: 10.1016/j.jviromet.2008.03.001. [DOI] [PubMed] [Google Scholar]
- 140.Afridi S, Naeem M, Hussain A, Kakar N, Babar ME, Ahmad J. Prevalence of hepatitis C virus (HCV) genotypes in Balochistan. Mol Biol Rep. 2009;36:1511–1514. doi: 10.1007/s11033-008-9342-0. [DOI] [PubMed] [Google Scholar]
- 141.Afridi SQ, Zahid MN, Shabbir MZ, Hussain Z, Mukhtar N, Tipu MY, Akhtar F, Yaqub T. Prevalence of HCV genotypes in district Mardan. Virol J. 2013;10:90. doi: 10.1186/1743-422X-10-90. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 142.Aziz H, Raza A, Murtaza S, Waheed Y, Khalid A, Irfan J, Samra Z, Athar MA. Molecular epidemiology of hepatitis C virus genotypes in different geographical regions of Punjab Province in Pakistan and a phylogenetic analysis. Int J Infect Dis. 2013;17:e247–e253. doi: 10.1016/j.ijid.2012.09.017. [DOI] [PubMed] [Google Scholar]
- 143.Imran M, Manzoor S, Khattak NM, Tariq M, Khalid M, Javed F, Bhatti S. Correlation of OAS1 gene polymorphism at exon 7 splice accepter site with interferon-based therapy of HCV infection in Pakistan. Viral Immunol. 2014;27:105–111. doi: 10.1089/vim.2013.0107. [DOI] [PubMed] [Google Scholar]
- 144.Khan TM, Mehr MT, Ullah H, Khan H, Iman NU. Frequency of hepatitis C virus genotypes in the north of Pakistan. Gomal J Med Sci. 2014:12. [Google Scholar]
- 145.Mahmood K, Mohammad N. Genotype variation of hepatitis C virus in District Buner Swat. J Ayub Med Coll Abbottabad. 2011;23:18–21. [PubMed] [Google Scholar]
- 146.Nabi SG, Zaffar G, Sheikh NI, Hassan K, Hassan U. Hepatitis C virus genotypes: a plausible association with viral loads. Indian J Pathol Microbiol. 2013;56:384–387. doi: 10.4103/0377-4929.125319. [DOI] [PubMed] [Google Scholar]
- 147.Safi SZ, Waheed Y, Sadat J, Solat-Ul-Islam S, Saeed U, Ashraf M. Molecular study of HCV detection, genotypes and their routes of transmission in North West Frontier Province, Pakistan. Asian Pac J Trop Biomed. 2012;2:532–536. doi: 10.1016/S2221-1691(12)60091-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 148.Saleha S, Kamal A, Ullah F, Khan N, Mahmood A, Khan S. Prevalence of hepatitis C virus genotypes in district bannu, khyber pakhtunkhwa, pakistan. Hepat Res Treat. 2014;2014:165826. doi: 10.1155/2014/165826. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 149.Yahya KM, Khan RR, Aziz U, Hussain SA. Frequency of various hepatitis C virus (HCV) genotypes in Faisalabad and surrounding districts. JUMDC. 2013;4:57–62. [Google Scholar]
- 150.Afridi SQ, Ali MM, Awan F, Zahid MN, Afridi IQ, Afridi SQ, Yaqub T. Molecular epidemiology and viral load of HCV in different regions of Punjab, Pakistan. Virol J. 2014;11:24. doi: 10.1186/1743-422X-11-24. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 151.Ali A, Ahmed H, Idrees M. Molecular epidemiology of Hepatitis C virus genotypes in Khyber Pakhtoonkhaw of Pakistan. Virol J. 2010;7:203. doi: 10.1186/1743-422X-7-203. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 152.Ali A, Nisar M, Ahmad H, Saif N, Idrees M, Bajwa MA. Determination of HCV genotypes and viral loads in chronic HCV infected patients of Hazara Pakistan. Virol J. 2011;8:466. doi: 10.1186/1743-422X-8-466. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 153.Butt S, Idrees M, Akbar H, ur Rehman I, Awan Z, Afzal S, Hussain A, Shahid M, Manzoor S, Rafique S. The changing epidemiology pattern and frequency distribution of hepatitis C virus in Pakistan. Infect Genet Evol. 2010;10:595–600. doi: 10.1016/j.meegid.2010.04.012. [DOI] [PubMed] [Google Scholar]
- 154.Inamullah M, Ahmed H, Sajid-ul-ghafoor M, Ali L, Ahmed A. Hepatitis C virus genotypes circulating in district Swat of Khyber Pakhtoonkhaw, Pakistan. Virol J. 2011;8:16. doi: 10.1186/1743-422X-8-16. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 155.Ahmad W, Ijaz B, Javed FT, Jahan S, Shahid I, Khan FM, Hassan S. HCV genotype distribution and possible transmission risks in Lahore, Pakistan. World J Gastroenterol. 2010;16:4321–4328. doi: 10.3748/wjg.v16.i34.4321. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 156.Ijaz B, Ahmad W, Javed FT, Gull S, Sarwar MT, Kausar H, Asad S, Jahan S, Khaliq S, Shahid I, et al. Association of laboratory parameters with viral factors in patients with hepatitis C. Virol J. 2011;8:361. doi: 10.1186/1743-422X-8-361. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 157.Akhund AA, Akhtar R, Naqvi SQH, Kamal M. Chronic hepatitis; HCV Genotypes in correlation with alanine aminotransferase level in patients in interior of Sindh. Professional Med J. 2014;21:450–454. [Google Scholar]
- 158.Afzal MS, Khan MY, Ammar M, Anjum S, Zaidi NU. Diagnostically untypable hepatitis C virus variants: it is time to resolve the problem. World J Gastroenterol. 2014;20:17690–17692. doi: 10.3748/wjg.v20.i46.17690. [DOI] [PMC free article] [PubMed] [Google Scholar]