

Abstract
A 45‐year‐old Japanese woman complained of uncontrolled hypertension and face swelling. She was diagnosed with Cushing's syndrome with secretion of adrenocorticotropic hormone. Fluorodeoxyglucose positron emission tomography‐computed tomography revealed a 2 × 2 cm mass in her left lung, with high standardized maximum uptake value. She underwent bronchoscopy with endobronchial ultrasound via a guide‐sheath. Surgical resection of her left upper lung was performed, and pathological examination showed a typical carcinoid tumor. After lung resection, she recovered from her subjective symptoms. Diagnosis of peripheral carcinoid tumor of the lung is generally difficult. Here, we introduce a case of peripheral pulmonary carcinoid tumor diagnosed by endobronchial‐ultrasound‐guided bronchoscopy.
Keywords: Carcinoid, endobronchial‐ultrasound‐guided bronchoscopy (EBUS‐GS), peripheral lung lesion
Abbreviations
- ACTH
adrenocorticotropic hormone
- EBUS‐GS
endobronchial ultrasound‐guided bronchoscopy
- FDG‐PET/CT
fluorodeoxyglucose position emission tomography/computed tomography
- SUV
standardized uptake value
Introduction
Pulmonary carcinoid tumor is a rare disease, accounting for approximately 2% of all primary lung tumors. The gastrointestinal tract is the most frequently involved site, while the lung is the second most common [1]. About 85% of carcinoid tumors are located in the central airway; 75% arise from the lobar bronchi, and 10% arise from the mainstem bronchi [2]. In cases of carcinoids in the central airway, the majority of patients are symptomatic at presentation. Common symptoms include cough, hemoptysis, wheezing, and pneumonia. In contrast, patients with peripheral carcinoids are usually asymptomatic and the condition is difficult to diagnose.
In recent years, it has been reported that bronchoscopy with endobronchial ultrasound (EBUS) demonstrates a high diagnostic yield with low complication rate in the evaluation of small peripheral nodules [3]. Here, we report a case of peripheral pulmonary carcinoid tumor diagnosed by EBUS‐guided bronchoscopy.
Case Report
A 45‐year‐old Japanese woman complained of uncontrolled hypertension and facial swelling. She visited the community hospital, and was diagnosed with adrenocorticotropic hormone (ACTH)‐dependent Cushing's syndrome. She was referred to our hospital for further investigation. Computed tomography (CT) of her chest revealed a 2 × 2 cm mass in her left upper lung (S1 + 2) with homogeneous enhancement. The maximum standardized uptake value (SUV) of this lesion was 4.09 on fluorodeoxyglucose positron emission tomography (FDG‐PET)/CT (Fig. 1A). Bronchoscopic findings showed a yellow submucosal lesion in the left upper bronchus (Fig. 1B), and EBUS demonstrated a solid lesion in the same location. We performed transbronchial lung biopsy using a guide‐sheath within the tumor (Fig. 1C). The pathological specimen showed a rosette‐like formation (Fig. 2A), and alveolar hyperplastica with hematoxylin and eosin staining. There were < 2 mitoses per 2 mm2 (with high‐power field), without necrosis. Immunohistochemical staining showed strong positivity for chromogranin A, synaptophysin, CD56, and ACTH (Fig. 2B, C). Based on these results, we diagnosed the patients as having an ACTH‐secreting, peripheral pulmonary carcinoid tumor.
Figure 1.
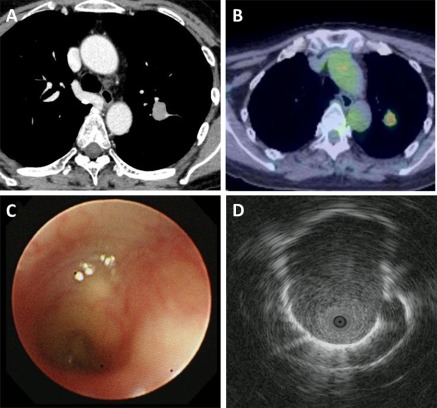
Fluorodeoxyglucose position emission tomography/computed tomography reveals a mass in the left upper lung (S1 + 2) field. The maximum standardized uptake value of the mass was 4.09 (A). The mass is enhanced on contrast‐enhanced CT (B). Bronchoscopy shows a yellow submucosal lesion on macroscopic examination in the left upper 1 + 2 bronchus (C). EBUS demonstrates a solid lesion in the same location (D). CT: computed tomography, EBUS: endobronchial ultrasound.
Figure 2.
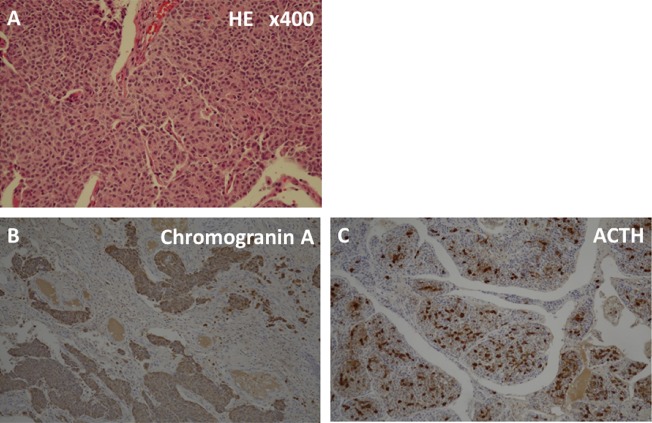
Pathological findings. Hematoxylin and eosin staining shows rosette‐like formation without necrosis (A; 400× magnification). Immunohistochemistry staining indicates strong positivity for chromogranin A (B) and ACTH (C). ACTH: adrenocorticotropic hormone.
Surgical resection of her left upper lung was performed, and her subjective symptoms resolved.
Discussion
Pulmonary carcinoids are known to arise from the central airway. As a result, common presenting symptoms include cough, hemoptysis, wheezing, and pneumonia. In cases of peripheral pulmonary carcinoids, they are usually asymptomatic.
A common radiological finding of peripheral pulmonary carcinoid tumor is lobulated solitary pulmonary nodules with homogeneous enhancement, and the mean tumor diameter is less than 20 mm2. With regard to FDG‐PET, Chong et al. reported that its sensitivity is only 75% [4], and the mean maximum SUVs of carcinoids is 3.4 [5]. This low sensitivity value is due to their size and hypometabolic state. Our case findings correspond with these findings.
In recent years, it has been reported that EBUS has a higher diagnostic yield with lower complication rate in the evaluation of small solitary pulmonary nodules. Steinfort et al. reported that the diagnostic yield of conventional bronchoscopy in the investigation of lesions <20 mm is 14%, while the diagnostic yield with EBUS is higher than 70% [3]. Based on this result, EBUS is commonly adopted as the first choice to diagnose small‐sized peripheral lung cancers in Japanese clinical practice. In this case, we were able to obtain enough biopsy samples to diagnose our case using EBUS. It was reported that over one‐third of carcinoid tumors are diagnosed only at thoracotomy. CT‐guided needle biopsy is the second most common diagnostic procedure, but pneumothoraces frequently occur [3]. To the best of our knowledge, this is the first report of a peripheral pulmonary carcinoid tumor diagnosed with EBUS.
In conclusion, we report a case of an ACTH‐secreting carcinoid tumor of the peripheral lung diagnosed by transbronchial biopsy using EBUS. Through this case, we learned the importance of an appropriate localizing diagnosis, and found that EBUS is useful to diagnose these small peripheral lesions even in rare thoracic malignancies.
Disclosure Statements
No conflict of interest declared.
Appropriate written informed consent was obtained for publication of this case report and accompanying images.
References
- 1. De Vita VT, Lawrence TS, and Rosenberg SA. 2008. De Vita, Hellman, and Rosenberg's Cancer: Principles and Practice of Oncology, 8th edn Wolters Kluwer/ Lippincott Williams & Wilkins, Philadelphia, USA. [Google Scholar]
- 2. Meisinger QC, Klein JS, Butnor KJ, et al. 2011. CT Features of Peripheral pulmonary carcinoid tumors. AJR Am. J. Roentgenol. 197:1073–1080. [DOI] [PubMed] [Google Scholar]
- 3. Steinfort DP, Finlay M, and Irving LB. 2008. Diagnosis of peripheral pulmonary carcinoid tumor using endobronchial ultrasound. Ann. Thorac. Med. 3:146–148. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4. Daniels CE, Lowe VJ, Aubry MC, et al. 2007. The utility of fluorodeoxyglucose positron emission tomography in the evaluation of carcinoid tumors presenting as pulmonary nodules. Chest 131:255–260. [DOI] [PubMed] [Google Scholar]
- 5. Chong S, Lee KS, Kim BT, et al. 2007. Integrated PET/CT of pulmonary neuroendocrine tumors: Diagnostic and prognostic implications. AJR Am. J. Roentgenol. 188:1223–1231. [DOI] [PubMed] [Google Scholar]