

Abstract
Introduction:
Fractures have been described mainly following falling accidents in horse-related injuries. Horse bites are uncommon accidents. We present a case of open fracture of the forearm due to horse bite.
Case Report:
A 35-year-old male farm-worker presented to the emergency room with alleged history of horse bite to the right forearm about 2 hours prior to presentation while feeding the horse. There was deformity of the forearm with multiple puncture wounds, deep abrasions and small lacerations on the distal-third of the forearm. Copious irrigation with normal saline was done and he was administered anti-tetanus and postexposure rabies prophylaxis. Prophylactic antibiotic therapy was commenced. Radiographs revealed fracture of radius and ulna in the mid-shaft region. He underwent emergency wound debridement, and the ulna was stabilised with an intra-medullary square nail. Seventy-two hours later, he underwent re-debridement and conversion osteosynthesis. He had an uneventful recovery and at three-month follow-up, the fractures had healed radiographically in anatomic alignment. At two-year follow-up, he is doing well, is pain free and has a normal range of motion compared to the contralateral side.
Conclusion:
Horse bites behave as compound fractures however rabies prophylaxis will be needed and careful observation is needed. Early radical debridement, preliminary skeletal stabilisation, re-debridement and conversion osteosynthesis to plate, and antibiotic prophylaxis were the key to the successful management of our patient.
Keywords: Horse, animal bite, forearm, open fracture
Introduction
Falls and kicks are common mechanism of injuries in people handling horses [1-3]. Bite injuries are quite uncommon and fractures due to horse bite are even rarer. Animal bites also have the fear of wound infection by zoonotic organisms. We present a case of forearm open fracture due to horse bite and its management. Previous reports of mammalian bite injuries and their complications are discussed.
Case Report
A 35-year-old male farm-worker presented to the emergency room with alleged history of horse bite to the right forearm about 2 hours prior to presenting to us. He was bitten by his horse when he was feeding it. He had recently bought the horse for renting it for marriages and other social and religious functions. On examination, there was deformity of the forearm with multiple puncture wounds, deep abrasions and small lacerations on the distal-third of the forearm. (Fig. 1(a) and (b))
Figure 1 (a) and 1(b).

Front and dorsal view of the forearm on presentation showing the bite wounds.
Sensations and motor functions in the hand were grossly normal. Copious irrigation with normal saline was done for the wounds. He was given 0.5 ml tetanus toxoid and 500 IU Tetglob® (human Tetanus Immunoglobulin BP), and received post-exposure rabies prophylaxis with Vaxirab™ (Purified Duck Embryo Vaccine for Rabies IP). Prophylactic antibiotic therapy with intravenous penicillin, gentamicin, cloxacillin and metronidazole was commenced. Radiographs revealed fracture of radius and ulna in the mid-shaft region (Fig. 2).
Figure 2.
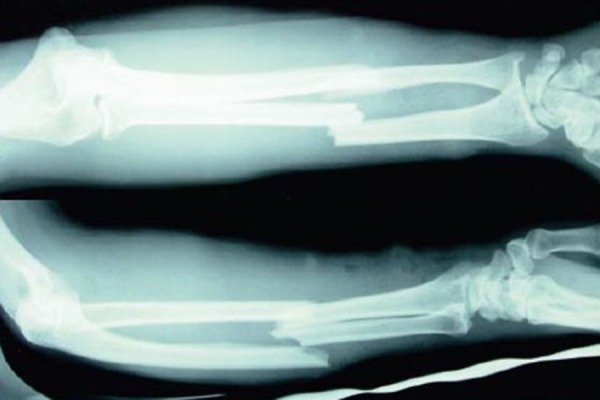
Pre-operative radiographs showing fracture of shafts of Radius and Ulna.
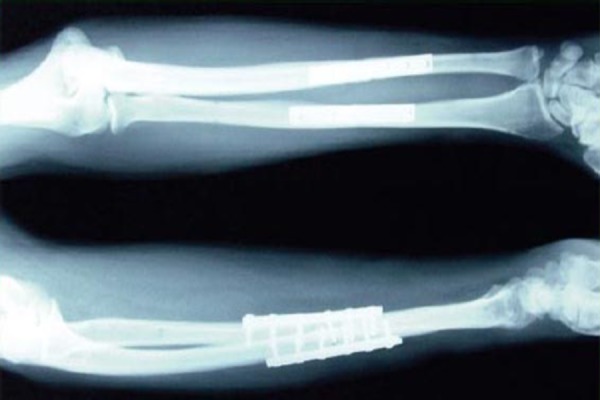
He was taken to the operating room (OR) where careful debridement of the wounds was done under loupe-magnification. The crushed wound margins were excised. The forearm muscles on both flexor and extensor aspects appeared churned and partly crushed. The devitalised portions of these muscles were excised. The fractured bone ends were curetted. The ulna was stabilised with an intra-medullary Talwalkar square nail (INOR, Mumbai, India). Skin edges were approximated with loose sutures. The same antibiotics were continued in the post-operative period. He had no episode of fever and there were no features of wound infection. Seventy-two hours later, he was taken to the OR for re-debridement. There were no features of infection. The nail in ulna was removed and conversion osteosynthesis using dynamic compression plate and screws for radius and ulna was done (Fig. 3).
Figure 3.
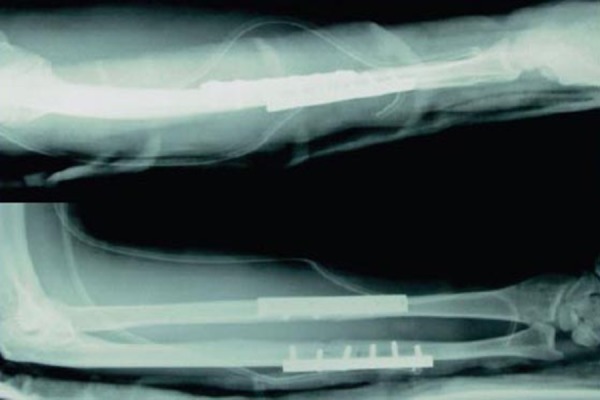
Post-operative radiograph following conversion osteosynthesis with dynamic compression plates and screws.
He was changed to oral cephalexin and ciprofloxacin on day 6 which were given till suture removal. He had an uneventful recovery and was discharged from the hospital on the 10th day from injury. He returned for suture removal at 2 weeks’ time. The plaster splint was removed at one-month follow-up (Fig. 4(a) and (b)).
Figure 4(a) and 4(b).

Clinical photographs one-month follow-up.
The horse had no features of rabies. The patient, however, sold the horse as he was too scared to keep it. At three-months, the fractures had healed radiographically in anatomic alignment (Fig. 5).
Figure 5.
Three-month follow-up radiographs showing fracture healing in anatomic alignment.
At two-year follow-up, he is doing well, is pain free and has a normal range of motion compared to the contralateral side. He is able to use his hand for all routine work and has returned to his work in the farm. The patient gave the informed consent for publication of this study.
Discussion
In horse-related accidents, the majority of injuries occur when the person falls from a horse [1-3]. Blow by a horse, getting struck by an object while riding a horse, being kicked by a horse, the horse falling on the patient, being entangled by reins, and being bitten by a horse are other less common horse-related accidents.
Horse bites are uncommon injuries. Of all reported injuries involving horses, approximately 3% to 4.5% are related to bites [4]. Most people bitten by horses do not seek medical advice as most bite injuries are minor and self-treated or do not require admission to hospital [1,5].
Thomas et al [2] in their study estimated that 102,900 people are treated yearly in emergency rooms in the US due to nonfatal horse related injuries, and about 1800 patients are treated each year after horse bites. Mammalian bite injuries are known to have distressing physical and psychological consequences. Our patient was too frightened to keep the horse and risk another bite, and hence, sold it not caring for the implications of financial loss.
Domestic animals at home differ between societies, and therefore, local traditions affect the epidemiology of animal-related injuries [5]. Comparing animal bite wounds, cat bites result in punctured deep wounds, dog bites cause rather superficial abrasion and laceration type wounds [6]; because of the great deal of force exerted by an equine in closing its jaws, in horse and donkey bites, the severity of injuries may range from mild superficial pressure trauma, cutaneous breaks of the skin, deep lacerations with loss of tissue, to amputations of digits and even the nose [4,7]. Fractures have been reported mainly following falling accidents in horse-related injuries [1]. Peel et al [8] reported a case of fracture of the forearm bones following horse bite that was treated with open reduction and internal fixation primarily. He sustained repeated infections with purulent wound discharge from which mixed cultures of bacteria, including Staphylococcus aureus, Prevotella melaninogenica, Escherichia coli, and Pasteurella multocida were isolated. More than 3 months after the initial attack by the horse Actinobacillus suis was isolated by bone biopsy specimen.
Though the acute trauma is readily apparent from a biting event, there is also the risk of exposure to various microbes in the oral secretions of equines. Transmission of such agents with zoonotic potential can also occur from the non-bite exposures to the oral and respiratory secretions [4]. Because of the large number of bacteria in the mouth, animal bite wounds are generally contaminated and their treatment is difficult, particularly in extensive lesions. The occurrence of bacterial infection after animal bites depends on several factors, such as species of animal aggressors (humans would be associated with a higher infection risk), type and site of the injuries (wounds located in hands have a higher infection risk), care given to the wound, inherent factors in the individual (greater risk in elderly, those with diabetes mellitus, vascular disease, etc). In relation to wound type, puncture wounds have been reported to have a higher infection rate after animal bites, possibly due to the deposition of bacteria deep in the skin. There is evidence that the use of antibiotic prophylactic after bites of the hand reduces infection [9]. Horse bites most commonly lead to infections with Burkholderia, Streptococcus, Staphylococcus, Rhodococcus, Actinobacillus, Yersinia, and Pasteurella, Escherichia, Neisseria, Prevotella, Pseudomonas, Listeria, Hendra virus, Vesicular stomatitis virus species [4].
Lucas et al [10] reported on significant injuries in veterinarians. Bites, kicks or strikes, animal contact and cutting or scratching were the most frequent mechanisms of injury reported. Nearly 20% of reported horse-related injuries, 14% of cattle and cats and 11% of dog-related injuries resulted in admission. Brouwer et al [11] reported a case of Streptococcus equi meningitis complicated by brain abscesses, as a result of a horse bite.
Köse et al [6] performed a retrospective evaluation of 24 patients presenting with animal bites (19 horse and 5 donkey bites). The head and neck were the most frequent bite sites (14 cases), followed by the extremities (eight cases) and the trunk (two cases). Acceptable aesthetic outcomes were achieved with early primary repair and reconstructive procedures.
Our management was staged with damage control and infection control taking precedence. Our primary aim was damage-control – to aggressively debride and at the same time give stability to the limb for wound dressings. Preliminary stabilisation of the forearm by an intramedullary Talwalkar square nail (INOR, Mumbai, India) in the ulna was done following debridement of the wounds and excision of devitalised tissues. Fixing the ulna with a nail also helped in maintaining forearm length. Re-debridement at 72 hours, showed no features of infection and decision of internal fixation with plate and screws was taken. This, we believe, was possible because of aggressive primary debridement. We also wish to highlight to the journal reader community that putting in implants when there is any doubt of contamination is risking long term bone infection and other associated complications of delay-in-union and non-union with compromised hand function. This was the reason for not fixing both the bones at the primary sitting.
Intra-medullary nail was preferred over external fixator in this case, though in fractures with severe soft tissue damage the use of external fixator is indicated. The problems of using external fixation in the forearm include: pin-track-infection, nerve damage due to insufficient anatomical exposure and a relatively high rate of non-union [12]. Conversion osteosynthesis to internal fixation after primary external fixation is associated with high rates of osteomyelitis [12]. Plating is established as the standard method in the operative treatment of forearm fractures in adults [13]. Plating provides a stable osteosynthesis and allows shorter immobilisation periods. We successfully converted the fixation from intra-medullary nail to plating with no incidence of infection or delay-in-union.
The goal of any debridement is to prevent bacterial adherence and thus infection. Bacteria are more likely to adhere to non-vascular tissue or foreign bodies. Bacterial adherence is known to be time dependent. Therefore, it makes sense to debride wounds which have necrotic tissue early rather than later. Early bone stabilisation helps prevent further tissue damage and decreases the likelihood of infection [14].
Conclusion
Considering the most common complication of zoonotic infection related to animal bite injuries, our successful surgical treatment without complication appears to have definite clinical relevance. The systematic treatment protocol of early radical debridement, preliminary skeletal stabilisation, re-debridement and conversion osteosynthesis to plate, and antibiotic prophylaxis were the key to the successful management of our patient.
Clinical Message.
Horse or other animal bites are uncommon injuries. The management of these cases should be staged with the principles of damage control and infection control taking precedence. Through this publication we wish to highlight these rare injuries in the orthopaedic community and the journal readers.
Biography


Footnotes
Conflict of Interest: Nil
Source of Support: None
References
- 1.Abu-Zidan FM, Rao S. Factors affecting the severity of horse-related injuries. Injury. 2003;34:897–900. doi: 10.1016/s0020-1383(03)00054-8. [DOI] [PubMed] [Google Scholar]
- 2.Thomas KE, Annest JL, Gilchrist J, Bixby-Hammett DM. Non-fatal horse related injuries treated in emergency departments in the United States 2001-2003. Br J Sports Med. 2006;40:619–26. doi: 10.1136/bjsm.2006.025858. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Court-Brown CM, Wood AM, Aitken S. The epidemiology of acute sports-related fractures in adults. Injury. 2008;39:1365–72. doi: 10.1016/j.injury.2008.02.004. [DOI] [PubMed] [Google Scholar]
- 4.Langley R, Morris T. That Horse Bit Me: Zoonotic Infections of Equines to Consider after Exposure through the Bite or the Oral/Nasal Secretions. J Agromedicine. 2009;14:370–81. doi: 10.1080/10599240903058087. [DOI] [PubMed] [Google Scholar]
- 5.Emet M, Beyhun NE, Kosan Z, Aslan S, Uzkeser M, Gokcen Cakir ZG. Animal-Related Injuries: Epidemiological and Meteorological Features. Ann Agric Environ Med. 2009;16:87–92. [PubMed] [Google Scholar]
- 6.Köse R, Söğüt Ö, Mordeniz C. Management of Horse and Donkey Bite Wounds: A Series of 24 Cases. Plast Reconstr Surg. 2010;125:251e–2e. doi: 10.1097/PRS.0b013e3181d515dd. [DOI] [PubMed] [Google Scholar]
- 7.Danielsson LG, Westlin NE. Riding Accidents. Acta Orthop Scand. 1973;44:597–603. doi: 10.3109/17453677308989097. [DOI] [PubMed] [Google Scholar]
- 8.Peel MM, Hornidge KA, Luppino M, Stacpoole AM, Weaver RE. Actinobacillus spp. and Related Bacteria in Infected Wounds of Humans Bitten by Horses and Sheep. J Clin Microbiol. 1991;29:2535–38. doi: 10.1128/jcm.29.11.2535-2538.1991. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Medeiros IM, Saconato H. Antibiotic prophylaxis for mammalian bites. Cochrane Database of Systematic Reviews. 2001;2:CD001738. doi: 10.1002/14651858.CD001738. [DOI] [PubMed] [Google Scholar]
- 10.Lucas M, Day L, Shirangi A, Fritschi L. Significant injuries in Australian veterinarians and use of safety precautions. Occup Med. 2009;59:327–33. doi: 10.1093/occmed/kqp070. [DOI] [PubMed] [Google Scholar]
- 11.Brouwer MC, Kasanmoentalib ES, Opstelten FW, van der Ende A, van de Beek D. A horse bite to remember. Lancet. 2010;376(9747):1194. doi: 10.1016/S0140-6736(10)60965-8. [DOI] [PubMed] [Google Scholar]
- 12.Helber MU, Ulrich C. External fixation in forearm shaft fractures. Injury. 2000;31:45–7. doi: 10.1016/s0020-1383(99)00262-4. [DOI] [PubMed] [Google Scholar]
- 13.Fernandez FF, Egenolf M, Carsten C, Holz F, Schneider S, Wentzensen A. Unstable diaphyseal fractures of both bones of the forearm in children: Plate fixation versus intramedullary nailing. Injury. 2005;36:1210–6. doi: 10.1016/j.injury.2005.03.004. [DOI] [PubMed] [Google Scholar]
- 14.Rick Buckley. Open long-bone fractures: Early versus delayed debridement as a prognostic factor for infection. Orthop trauma dir. 2008;06:11–8. [Google Scholar]