

Abstract
Gastrocnemius aponeurotic recession is the surgical treatment for symptomatic gastrocnemius contracture. Endoscopic gastrocnemius recession procedures has been developed recently and reported to have fewer complications and better cosmetic outcomes. Classically, this is performed at the aponeurosis distal to the gastrocnemius muscle attachment. We describe an alternative endoscopic approach in which the intramuscular portion of the aponeurosis is released.
Gastrocnemius contracture can lead to various problems, including Achilles tendinosis, flatfoot, lower-back pain or strain, knee hyperextension (genu recurvatum), plantar fasciitis, midfoot pain or arthritis, metatarsalgia, posterior tibial tendon insufficiency, osteoarthritis, and foot ulcers.1, 2, 3, 4 Gastrocnemius recession surgery is performed if the symptomatic contracture cannot be eliminated with stretching exercises. The aim of surgery is to weaken or eliminate the gastrocnemius muscle's plantar-flexor action on the foot.5 Classically, this is performed as an open procedure. The level of recession can be either at the gastrocnemius aponeurosis distal to the gastrocnemius muscle attachment6, 7, 8 or at the anterior surface of the muscle-bound portion of the gastrocnemius aponeurosis.5, 9, 10, 11, 12 Endoscopic gastrocnemius recession procedures have been developed recently and reported to have fewer complications and better cosmetic outcomes.1, 2, 13, 14, 15, 16, 17, 18, 19, 20, 21, 22, 23 The endoscopic techniques have mostly used an endoscopic approach of the Strayer type of gastrocnemius aponeurosis recession. We describe an alternative endoscopic approach in which the recession is at the intramuscular portion of the gastrocnemius aponeurosis.
Technique
The patient is supine with the legs spread. A thigh tourniquet is applied to provide a bloodless surgical field. A towel roll is put under the ankle to free the calf from the table. The distal border of the gastrocnemius muscle is palpated and marked. The medial portal is located on the medial side of the calf and 3 cm proximal to the distal border of the gastrocnemius muscle. It is ideal if the portal incision is made over the interval between the gastrocnemius and soleus muscles (Table 1). This can be identified by flexion and extension of the knee, keeping the ankle in dorsiflexion. The gliding of the gastrocnemius muscle over the soleus muscle can be palpated. A 1.5-cm medial portal incision is made (Fig 1). Blunt dissection of the subcutaneous tissue is performed with a hemostat, and the deep fascia is incised open. The plane between the aponeuroses of the gastrocnemius and soleus muscles is identified. If the plantaris tendon can be identified, it is cut at this point. A 4.0-mm 30° arthroscope (Dyonics; Smith & Nephew, Andover, MA) is inserted through the medial portal, and the correct plane is confirmed if both the gastrocnemius and soleus intramuscular aponeuroses can be assessed by rotating the arthroscope anteriorly and posteriorly, respectively. The arthroscope is advanced laterally through this plane until the lateral borders of the gastrocnemius and soleus intramuscular aponeuroses are reached. The arthroscope is removed, and the arthroscopic cannula (Dyonics; Smith & Nephew) is left in situ. A Wissinger rod is inserted through the arthroscopic cannula and penetrates the deep fascia of the lateral calf. The lateral portal incision is made at the exit point of the rod. The cannula is then advanced along the rod and exits through the lateral portal incision. The rod is removed, and the arthroscope is inserted into the cannula. The arthroscope is then withdrawn, and a retrograde knife (Smith & Nephew) is inserted through the lateral portal under arthroscopic guidance until the midpoint of the gastrocnemius intramuscular aponeurosis is reached. The aponeurosis is penetrated by the knife, and the lateral half of the aponeurosis is released by the retrograde knife. After completion of the lateral half of the aponeurosis, the arthroscope is advanced again to the lateral portal. Penetration into the gastrocnemius or soleus muscle can be avoided by arthroscopic guidance. After the arthroscope passes through the lateral portal incision, the arthroscope is removed, and the Wissinger rod is inserted into the cannula again (Fig 2). The cannula is removed, and the rod is left in situ. The cannula is inserted along the rod through the lateral portal. The rod is then removed, and the arthroscope is inserted into the cannula. The retrograde knife is inserted and advanced through the medial portal under arthroscopic guidance until the medial end of the lateral cut of the gastrocnemius intramuscular aponeurosis is reached (Fig 3). The medial half of the aponeurosis is released by the retrograde knife. The ankle is in dorsiflexion with the knee extended. The even separation of the cut edges of the aponeurosis confirms completeness of the gastrocnemius intramuscular aponeurotic recession (Video 1).
Table 1.
Pearls for Endoscopic Gastrocnemius Intramuscular Aponeurotic Recession
| 1. The portal incisions should be placed over the interval between the soleus and gastrocnemius muscles. |
| 2. To avoid penetration of the instruments into the muscle bellies, the arthroscopic cannula should pass through the portals in the intermuscular plane under arthroscopic guidance. |
| 3. To minimize postoperative bleeding and pain, it is important to avoid excessive cutting of the muscle fibers. |
| 4. It is important to ensure release of the medial and lateral edges of the aponeurosis to achieve complete aponeurotic recession. |
Fig 1.

Endoscopic gastrocnemius intramuscular aponeurotic recession in a right leg. The medial portal (a) is made about 3 cm proximal to the distal border of the gastrocnemius muscle (b).
Fig 2.

Endoscopic gastrocnemius intramuscular aponeurotic recession in a right leg. The visualization portal is switched from medial to lateral. (A) The arthroscope is advanced to the lateral portal. (B) The arthroscope is removed, and a Wissinger rod is inserted into the cannula.
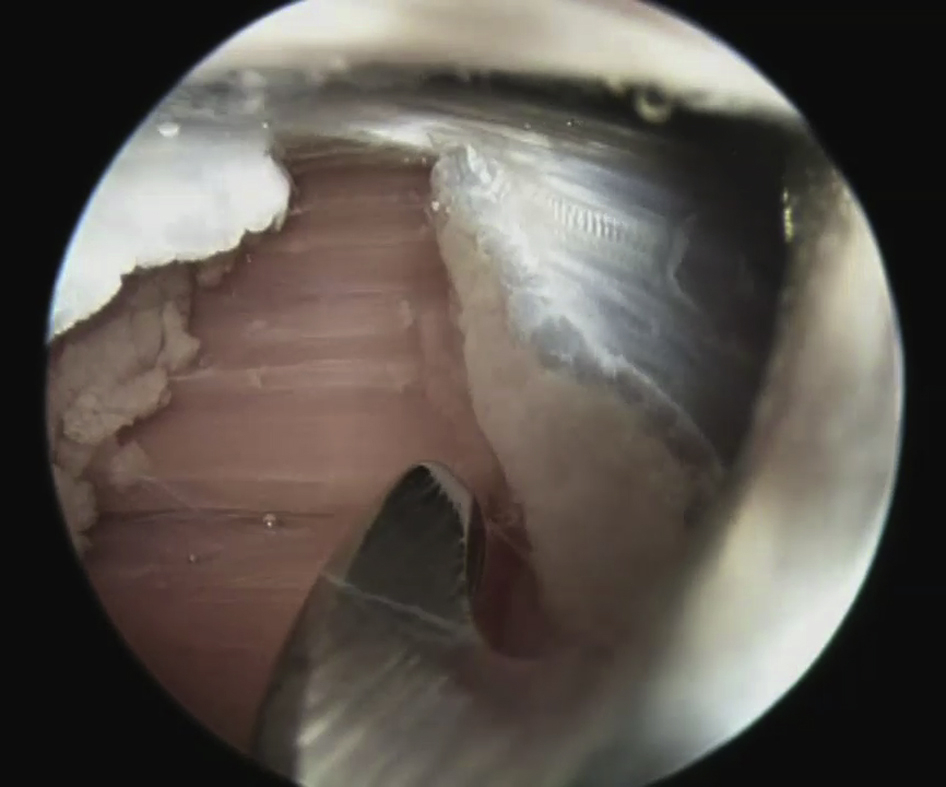
Fig 3.

Endoscopic gastrocnemius intramuscular aponeurotic recession in a right leg. (A) Release of the medial half of the aponeurosis. (B) Arthroscopic view of the reach of the medial end of the lateral gastrocnemius aponeurotic recession (ga).
If combined soleus-gastrocnemius intramuscular aponeurotic recession is planned, the arthroscope can be turned 180° to visualize the soleus aponeurosis. The procedure can be repeated to release the soleus intramuscular aponeurosis (Fig 4). Postoperatively, the patient is instructed on full–weight bearing walking and gastrocnemius stretching exercises.
Fig 4.
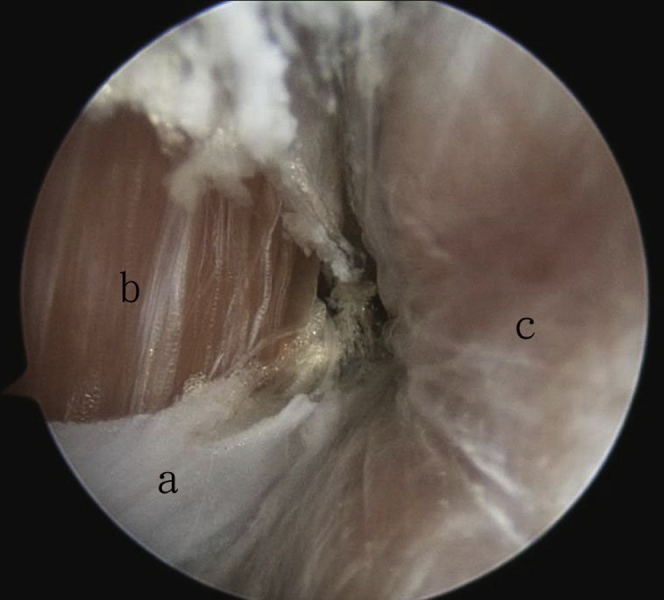
Endoscopic gastrocnemius intramuscular aponeurotic recession in a right leg, showing arthroscopic view with visualization through medial portal. Release of the soleus aponeurosis (a) with the soleus muscle (b) exposed. The gastrocnemius aponeurosis is already released with the gastrocnemius muscle (c) exposed.
Discussion
Endoscopic gastrocnemius aponeurosis recession procedures allow release of the gastrocnemius aponeurosis under arthroscopic visualization through small portal wounds. The reported techniques target the exposed inferior portion of the aponeurosis that is not directly covered by muscle.1, 2, 13, 14, 15, 16, 17, 18, 19, 20, 21, 22, 23 The portal incisions should be placed accurately at the level of the muscle-void portion of the gastrocnemius aponeurosis. Otherwise, the wounds would need to be extended, and the goal of “minimal incision surgery” is defeated. Different surface landmarks have been used to locate the muscle-void portion of the gastrocnemius aponeurosis, including the distal border of the gastrocnemius muscle,19, 20 the fibula length,24 and the medial malleolus.19 However, the location where the gastrocnemius aponeurosis joins the soleus aponeurosis and the length of the muscle-void portion of the gastrocnemius aponeurosis can be variable, and the gastrocnemius muscle can even insert directly onto the tendinous superficial surface of the soleus.9 Therefore intraoperative identification of this portion of the aponeurosis by surface landmarks is not reliable.
On the other hand, endoscopic recession of the intramuscular gastrocnemius aponeurosis has more constant surface landmarks.25 The level of recession is 3 cm proximal to the distal border of the gastrocnemius muscle, ensuring that the intramuscular portion of the aponeurosis is reached even if the gastrocnemius muscle inserts directly onto the tendinous superficial surface of the soleus. This approach preserves the insertion of the gastrocnemius, allowing for both an intramuscular and aponeurotic lengthening.5, 10 It can lessen the force applied by the gastrocnemius muscle on the foot without entirely decommissioning the muscle's biomechanical influence.5 In contrast to the Strayer-type endoscopic gastrocnemius aponeurosis recession, preservation of the gastrocnemius insertion allows the gastrocnemius to maintain a “weakened” effect on the foot and the amount of calf atrophy will be diminished.10 Moreover, the sural nerve will be protected by the gastrocnemius muscle during endoscopic recession of the muscle-bound portion of the gastrocnemius aponeurosis, and the risk of iatrogenic sural nerve injury will be lessened.10, 21 Furthermore, the palpable (if not visible) gap at the site of recession that is frequently noted after Strayer-type endoscopic gastrocnemius aponeurotic recession will be covered by the gastrocnemius muscle in this endoscopic gastrocnemius intramuscular aponeurotic recession.25 However, it can be difficult to identify the interval between the soleus and gastrocnemius muscles, especially in obese patients. The placement of the medial portal incision may not be at this interval, and the portal incision may need to be extended to identify the plane between the muscles. Moreover, some of the muscle fibers are cut during aponeurotic release, and more postoperative pain and bleeding may occur as compared with Strayer-type endoscopic gastrocnemius aponeurotic recession. Supervised postoperative gastrocnemius stretching exercises are advisable. Finally, gastrocnemius-soleus intramuscular aponeurotic recession may be indicated in patients with spastic diplegic cerebral palsy.11 This can be performed through the same portal incisions.
Footnotes
The author reports that he has no conflicts of interest in the authorship and publication of this article.
Supplementary Data
Endoscopic gastrocnemius intramuscular aponeurotic recession in a right leg. The medial and lateral portals are 3 cm proximal to the distal border of the gastrocnemius muscle. In step 1, release of the lateral half of the gastrocnemius intramuscular aponeurosis is performed with a retrograde knife through the lateral portal. In step 2, release of the medial half of the aponeurosis is performed with a retrograde knife through the medial portal. In step 3, the completeness of the release is confirmed by even separation of the cut edges of the aponeurosis by ankle dorsiflexion with the knee extended.
{kind=link}
References
- 1.Barske H.L., DiGiovanni B.F., Douglass M., Nawoczenski D.A. Current concepts review: Isolated gastrocnemius contracture and gastrocnemius recession. Foot Ankle Int. 2012;33:915–921. doi: 10.3113/FAI.2012.0915. [DOI] [PubMed] [Google Scholar]
- 2.Grady J.F., Kelly C. Endoscopic gastrocnemius recession for treating equinus in pediatric patients. Clin Orthop Relat Res. 2010;468:1033–1038. doi: 10.1007/s11999-009-1084-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Maskill J.D., Bohay D.R., Anderson J.G. Gastrocnemius recession to treat isolated foot pain. Foot Ankle Int. 2010;31:19–23. doi: 10.3113/FAI.2010.0019. [DOI] [PubMed] [Google Scholar]
- 4.Pinney S.J., Hansen S.T., Jr., Sangeorzan B.J. The effect on ankle dorsiflexion of gastrocnemius recession. Foot Ankle Int. 2002;23:26–29. doi: 10.1177/107110070202300105. [DOI] [PubMed] [Google Scholar]
- 5.Blitz N.M., Eliot D.J. Anatomical aspects of the gastrocnemius aponeurosis and its muscular bound portion: A cadaveric study—Part II. J Foot Ankle Surg. 2008;47:533–540. doi: 10.1053/j.jfas.2008.08.006. [DOI] [PubMed] [Google Scholar]
- 6.Pinney S.J., Sangeorzan B.J., Hansen S.T., Jr. Surgical anatomy of the gastrocnemius recession (Strayer procedure) Foot Ankle Int. 2004;25:247–250. doi: 10.1177/107110070402500409. [DOI] [PubMed] [Google Scholar]
- 7.Strayer L.M., Jr. Recession of the gastrocnemius: An operation to relieve spastic contracture of the calf muscles. J Bone Joint Surg Am. 1950;32:671–676. [PubMed] [Google Scholar]
- 8.Strayer L.M., Jr. Gastrocnemius recession: Five-year report of cases. J Bone Joint Surg Am. 1958;40:1019–1030. [PubMed] [Google Scholar]
- 9.Blitz N.M., Eliot D.J. Anatomical aspects of the gastrocnemius aponeurosis and its insertion: A cadaveric study. J Foot Ankle Surg. 2007;46:101–108. doi: 10.1053/j.jfas.2006.11.003. [DOI] [PubMed] [Google Scholar]
- 10.Blitz N.M., Rush S.M. The gastrocnemius intramuscular aponeurotic recession: A simplified method of gastrocnemius recession. J Foot Ankle Surg. 2007;46:133–138. doi: 10.1053/j.jfas.2007.01.004. [DOI] [PubMed] [Google Scholar]
- 11.Dreher T., Buccoliero T., Wolf S.I. Long-term results after gastrocnemius-soleus intramuscular aponeurotic recession as a part of multilevel surgery in spastic diplegic cerebral palsy. J Bone Joint Surg Am. 2012;94:627–636. doi: 10.2106/JBJS.K.00096. [DOI] [PubMed] [Google Scholar]
- 12.Baumann J.U., Koch H.G. Lengthening of the anterior aponeurosis of musculus gastrocnemius through multiple incisions. Orthopedics and Traumatology. 1992;1:278–282. [Google Scholar]
- 13.Adelman V.R., Szczepanski J.A., Adelman R.P. Radiographic evaluation of endoscopic gastrocnemius recession, subtalar joint arthroereisis, and flexor tendon transfer for surgical correction of stage II posterior tibial tendon dysfunction: A pilot study. J Foot Ankle Surg. 2008;47:400–408. doi: 10.1053/j.jfas.2008.06.005. [DOI] [PubMed] [Google Scholar]
- 14.Angthong C., Kanitnate S. Dual-portal endoscopic gastrocnemius recession for the treatment of severe posttraumatic equinus deformity: A case series and a review of technical modifications. J Nippon Med Sch. 2012;79:198–203. doi: 10.1272/jnms.79.198. [DOI] [PubMed] [Google Scholar]
- 15.Barrett S.L., Jarvis J. Equinus deformity as a factor in forefoot nerve entrapment: Treatment with endoscopic gastrocnemius recession. J Am Podiatr Med Assoc. 2005;95:464–468. doi: 10.7547/0950464. [DOI] [PubMed] [Google Scholar]
- 16.DiDomenico L.A., Adams H.B., Garchar D. Endoscopic gastrocnemius recession for the treatment of gastrocnemius equinus. J Am Podiatr Med Assoc. 2005;95:410–413. doi: 10.7547/0950410. [DOI] [PubMed] [Google Scholar]
- 17.Poul J., Tuma J., Bajerova J. Video-assisted gastrocnemius-soleus and hamstring lengthening in cerebral palsy patients. J Pediatr Orthop B. 2008;17:81–84. doi: 10.1097/01.bpb.0000302748.66435.e9. [DOI] [PubMed] [Google Scholar]
- 18.Roukis T.S., Schweinberger M.H. Complications associated with uni-portal endoscopic gastrocnemius recession in a diabetic patient population: An observational case series. J Foot Ankle Surg. 2010;49:68–70. doi: 10.1053/j.jfas.2009.07.018. [DOI] [PubMed] [Google Scholar]
- 19.Saxena A., Widtfeldt A. Endoscopic gastrocnemius recession: Preliminary report on 18 cases. J Foot Ankle Surg. 2004;43:302–306. doi: 10.1053/j.jfas.2004.07.001. [DOI] [PubMed] [Google Scholar]
- 20.Schroeder S.M. Uniportal endoscopic gastrocnemius recession for treatment of gastrocnemius equinus with a dedicated EGR system with retractable blade. J Foot Ankle Surg. 2012;51:714–719. doi: 10.1053/j.jfas.2012.08.002. [DOI] [PubMed] [Google Scholar]
- 21.Tashjian R.Z., Appel A.J., Banerjee R., DiGiovanni C.W. Endoscopic gastrocnemius recession: Evaluation in a cadaver model. Foot Ankle Int. 2003;24:607–613. doi: 10.1177/107110070302400807. [DOI] [PubMed] [Google Scholar]
- 22.Trevino S., Gibbs M., Panchbhavi V. Evaluation of results of endoscopic gastrocnemius recession. Foot Ankle Int. 2005;26:359–364. doi: 10.1177/107110070502600503. [DOI] [PubMed] [Google Scholar]
- 23.Yeap E.J., Shamsul S.A., Chong K.W., Sands A.K. Simple two-portal technique for endoscopic gastrocnemius recession: Clinical tip. Foot Ankle Int. 2011;32:830–833. doi: 10.3113/FAI.2011.0830. [DOI] [PubMed] [Google Scholar]
- 24.Tashjian R.Z., Appel A.J., Banerjee R., DiGiovanni C.W. Anatomic study of the gastrocnemius-soleus junction and its relationship to the sural nerve. Foot Ankle Int. 2003;24:473–476. doi: 10.1177/107110070302400604. [DOI] [PubMed] [Google Scholar]
- 25.Lui T.H. Modified endoscopic release of gastrocnemius aponeurosis. J Foot Ankle Surg. 2015;54:140–142. doi: 10.1053/j.jfas.2014.07.014. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Endoscopic gastrocnemius intramuscular aponeurotic recession in a right leg. The medial and lateral portals are 3 cm proximal to the distal border of the gastrocnemius muscle. In step 1, release of the lateral half of the gastrocnemius intramuscular aponeurosis is performed with a retrograde knife through the lateral portal. In step 2, release of the medial half of the aponeurosis is performed with a retrograde knife through the medial portal. In step 3, the completeness of the release is confirmed by even separation of the cut edges of the aponeurosis by ankle dorsiflexion with the knee extended.