

Abstract
To compare the consistency of contrast-enhanced ultrasound (CEUS) and contrast-enhance CT (CECT) in diagnosis of 1~2 cm and 2.1~3 cm small hepatocellular carcinoma (HCC) and evaluate the value of CEUS in diagnosis of HCC. Methods: A total of 74 patients (89 lesions) with small HCC and cirrhosis background were retrospectively analyzed. All of the eighty-nine lesions were confirmed by histopathological examination of surgical samples or needle biopsy. All the cases were divided into 1~2 cm group and 2.1~3 cm group. The CEUS and CECT enhanced pattern and diagnosis results of the two groups were compared and the consistency between the two imaging methods were statistically analyzed. Results: In the diagnosis of 1.0-2.0 cm HCC, CEUS and CECT had a moderate consistency in arterial phase, CEUS showed a tolerable consistency with CECT in portal venous and delayphase. The two imaging methods have a better consistency for the diagnosis in 2.1-3.0 cm HCC. Conclusion: CEUS can be used as a supplement to provide important diagnostic information in clinical practice when positive results or definite diagnoses cannot obtain.
Keywords: Contrast-enhanced ultrasound, enhanced CT, small hepatocellular carcinoma
Introduction
China is a high prevalence area of hepatocellular carcinoma (HCC), where the morbidity and mortality has an increasing trend. Because the clinical symptoms of HCC were not obvious, most HCC patients have already lost the optimal treatment when they were definitely diagnosed. Thus, most cases show poor prognosis.
At present, contrast-enhanced computed tomography (CECT) is commonly used as an important imaging method in the diagnosis of HCC [1]. In the previous studies, contrast-enhanced ultrasound (CEUS) was compared with CECT, and it was considered not inferior to CECT according to most results [1,2]. To date, as far as we know, the reports involving the consistency of CEUS and CECT in the diagnosis of small HCC are quite limited.
With the cirrhosis background, the possibility of a malignant nodule to have diameter less than 1 cm is low. Therefore, 1 cm has become a cutoff in the differential diagnosis of benign and malignant nodules. In those lesions with diameter between 1~2 cm, the possibility of malignant nodule is 66%. In those lesions with diameter of 2~3 cm, the possibility of malignant nodule is 80% [3]. Therefore, in this study, we divided all cases into 1~2 cm group and 2.1~3 cm group, and compared the CEUS and CECT enhanced pattern and diagnosis results of the two groups. And we analyzed the consistency of the two imaging methods to assess the application value of CEUS in the diagnosis of HCC.
Patients and methods
Patients
A total of 74 patients (89 lesions) in Tumor Hospital of Guangxi Medical University with small HCC and cirrhosis background were retrospectively analyzed. There were 63 male and 11 female, aged 29-81 years; average age was 48 years. The minimum and maximum diameters of the lesions were 1.1 cm and 3.0 cm. Among them, 53 lesions were confirmed by histopathological examination of surgical samples and 36 lesions were confirmed by needle biopsy.
Instruments and methods
Ultrasound
Instruments and methods
GE Logiq9 color Doppler ultrasonography was used in this study, 2.5 or 3.5 MHz transducer ultrasound probe and a low acoustic power setting were applied. SonoVue® Contrast agent (Bracco company, Italy) was applied, and 5 ml of 0.9% NaCl was used to dilute SonoVue into 5 mg/ml of sulfur hexafluoride microbubbles suspensions. We injected microbubbles suspensions via ulnar vein (2.4 ml per injection), and then we used 5 ml of 0.9% NaCl to flush the tube. Two-dimensional ultrasound, including location, boundary and echo of tumor (Figure 1A), and color Doppler examination results, including blood flow velocity and resistance index of the tumor were recorded before underwent contrast, the probe was fixed then the contrast mode was started. The timer was started and the recording began when the contrast media was injected. Each lesion was observed for at least 5 min; the interval between each examination was at least 15 min.
Figure 1.
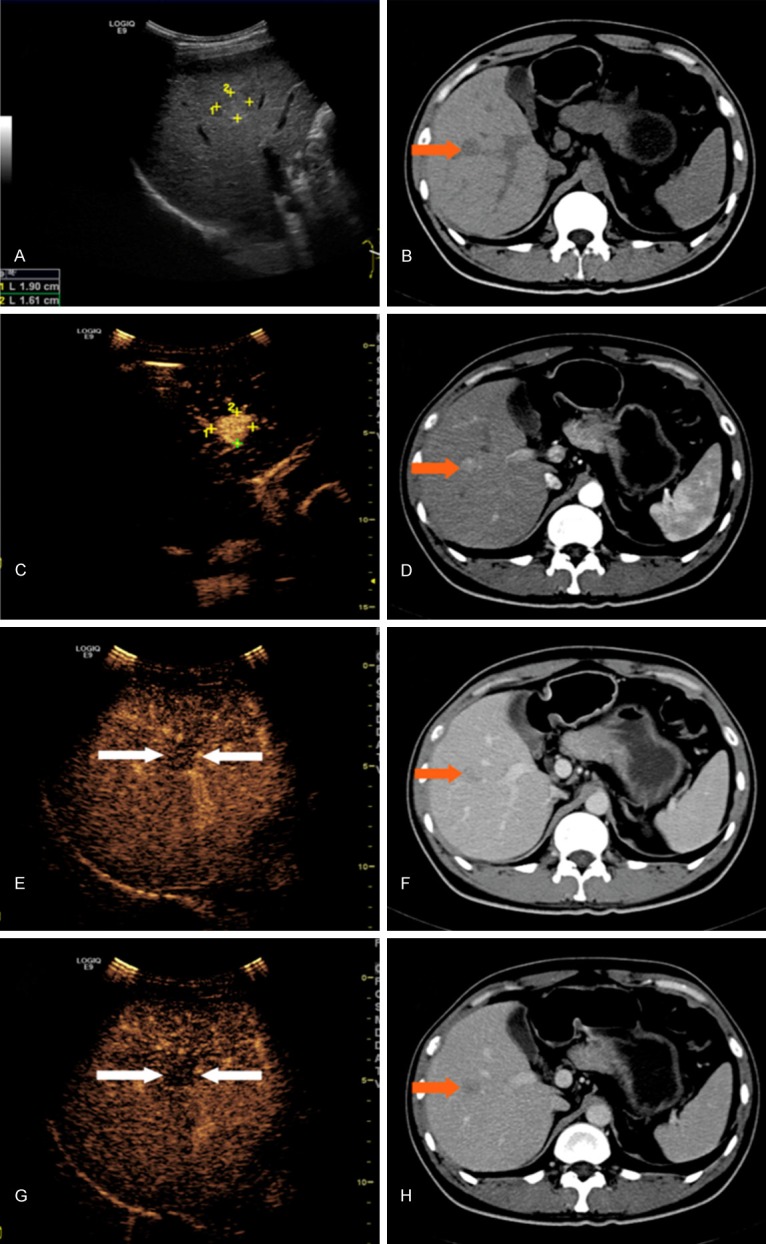
Typical features of HCC in CEUS and CECT for a male patient aged 58 years old. A: Two-dimensional ultrasound showed a hyper-echo lesion with uneven internal echo in right anterior inferior segment, measured the size of 1.9×1.6 cm. B: CT Plain scan showed a lesion with low density in the junction of upper and lower section of right anterior segment, measured the size of 1.8×1.7 cm. C: The whole lesion was enhanced rapidly in arterial phase (about 17 s) and the range of enhancement was about 1.9×1.8 cm in CEUS. D: Heterogeneous enhancement was observed in the lesion in arterial phase in CECT. E: The enhancement of this lesion started to fade in early portal phase (about 32 s). The density of the echo was lower than that of hepatic parenchyma in CEUS. F: The enhancement of this lesion faded in portal venous phase in CECT. G: The enhancement of this lesion kept fading in delay phase (about 128 s). The density of the echo was significantly lower than that of hepatic parenchyma and the lesion displayed well in CEUS. H: The enhancement of this lesion faded further in delay phase and showed low density in CECT.
Image analysis
Two ultrasonic physicians with 10 years working experience confirmed the results respectively. The enhanced phases were classified as arterial phase (0-30 s), portal venous phase (31-120 s) and delay phase (>120 s).
In arterial phase, the typical pattern of HCC was fast hyper-enhancement within the whole lesion (Figure 1C). The enhancements are classified as atypical in arterial phase when the lesions do not show “fast-in” hyper-enhancement, or the lesions have same enhancement as the surrounding hepatic parenchyma, or the enhancement patterns was not typical (e.g. rim enhancement around the lesions). For portal venous and delay phase, the typical pattern of HCC is the enhancement gradually faded and the lesion shows hypo-enhancement eventually (Figure 1E, 1G). The enhancements are classified as atypical in portal venous and delayphase when the lesions do not show “fast-out”, or the lesions faded with the surrounding hepatic parenchyma, or shows hyper-enhancement than the surrounding hepatic parenchyma.
CECT
Instruments and methods
SIEMENS sensation 64-slice CT was used for plain and enhanced scans, slice thickness was set as 7 mm. Iohexolwas injected with a rate of 4.5 ml/s via ulnar vein by high-pressure injector. Scans were carried out at 20-25 s for arterial phase and at 60-90 s for portal venous phase.
Image analysis
Two radiologists with 10 years working experience confirmed the results respectively. The performance of HCC show low-density lesion inn enhanced CT scan, it is similar to the two-dimensional ultrasound (Figure 1B). The typical pattern of HCC in arterial phase is hyper-enhancement (Figure 1D). The enhancements are classified as atypical in arterial phase when the lesions do not show “fast-in” high density, or the lesions show no obvious enhancement. For portal venous and delayphase (Figure 1F, 1H), the typical pattern of HCC is low density. The enhancements are classified as atypical in portal venous and delay phase when the lesions do not show “fast-out”, or the lesions have same density or higher density than the surrounding hepatic parenchyma, or the lesions shows blurred pattern or abnormal faded pattern.
Statistical analyses
All statistical analyses were performed with SPSS19.0 software. Kappa test was used to evaluate the consistency between the enhanced pattern and diagnosis results of CEUS and CECT. The criterion of k value was set as following: (1) Poor: k value in the range of 0-0.2. (2) Tolerable: k value in the range of 0.21-0.4 (3) Moderate: k value in the range of 0.41-0.6. (4) Well: k value in the range of 0.61-0.8. (5) Excellent: k value in the range of 0.81-1.0.
Results
The consistency of CEUS and CECT in the diagnosis of 1.0-2.0 cm HCC lesions
A total of 41 lesions were with the diameters of 1.0-2.0 cm. Among those lesions, 32 showed hypoechoic, 1 showed equal-echoic and 8 showed hyperechoic. No obvious color Doppler flow signal was found in 39 lesions. The enhanced pattern and diagnosis results of CEUS and CECT are shown in Table 1.
Table 1.
The consistency of CEUS and CECT in the diagnosis of 1.0-2.0 cm HCC lesions
| Methods | Arterial Phase | Portal venous and delay phase | Diagnoses |
|---|---|---|---|
|
| |||
| Enhanced (+)/Atypical enhanced (-) | Clearance (+)/Atypical clearance (-) | HCC (+)/Other lesions (-) | |
| CEUS (+) CECT (+) | 31 | 30 | 32 |
| CEUS (+) CECT (-) | 4 | 6 | 3 |
| CEUS (-) CECT (+) | 1 | 2 | 2 |
| CEUS (-) CECT (-) | 5 | 3 | 4 |
| k value | 0.596 | 0.346 | 0.543 |
| P | >0.05 | 0.017 | >0.05 |
The consistency of CEUS and CECTin the diagnosis of 2~3 cm HCC lesions
A total of 48 lesions were with the diameters of 2-3 cm. Among those lesions, 41 of them showed hypoechoic and 7 showed hyperechoic. A total of 3 lesions showed surrounding flow signals and 1 lesion showed internal flow signals in Color Doppler ultrasound. The enhanced pattern and diagnosis results of CEUS and CECT are shown in Table 2.
Table 2.
The consistency of CEUS and CECT in the diagnosis of 2~3 cm HCC lesions
| Methods | Arterial Phase | Portal venous and delay phase | Diagnoses |
|---|---|---|---|
|
| |||
| Enhanced (+)/Atypical enhanced (-) | Clearance (+)/Atypical clearance (-) | HCC (+)/Other lesions (-) | |
| CEUS (+) CECT (+) | 46 | 44 | 45 |
| CEUS (+) CECT (-) | 0 | 1 | 0 |
| CEUS (-) CECT (+) | 1 | 1 | 1 |
| CEUS (-) CECT (-) | 1 | 1 | 2 |
| k value | 0.657 | 0.644 | 0.749 |
| P | >0.05 | >0.05 | >0.05 |
Discussion
The early detection of HCC depends on clinical examination because of its insidious onset [1]. CECT provides clear imaging data for HCC diagnosis, and its accuracy has already been approved. CEUS could reflect the blood infusion of tissues, which could increase the accuracy of ultrasound diagnosis. However, on the diagnosis of HCC, the value of CEUS remains further investigation.
In recent years, many studies demonstrated that HCC could be diagnosed by CEUS as well as CECT [3-5]. However, there are few studies indicated the consistency of CEUS and CECT in the diagnosis of small HCC (1.0-2.0 cm and 2.1-3.0 cm). In this study, for the diagnosis of 1.0-2.0 cm HCC, CEUS showed a moderate consistency with CECT in arterial phase and tolerable consistency in portal venous and delay phase. For the diagnosis of 2.1-3.0 cm HCC, the consistency of CEUS and CECT was well.
The possible causes of inconsistency between CEUS and CECT in diagnosis of small HCC are as follows: (1) the process that the contrast media flows in and out of the lesion could be observed by CEUS real-timely and dynamically. CECT scans the lesion on each time point in each phase. Individual circulation difference has little effect on CEUS, which could perform the enhancement in each patient more neatly than CECT. (2) CECT makes slice scan in each phase, each slice has a certain thickness, and the volume effect of CT would lead to a missed diagnosis for a relatively small lesion. (3) In CEUS, SonoVue is a pure vascular contrast agent, which could reflect the arterial supply and venous outflow more clearly. However, iodine contrast agent in CECT may flow into intercellular space. This two imaging methods are different in the specific methods and contrast media. (4) Under cirrhosis background, the pathological process of 90% HCC are as follows: hyperplastic nodules→heterotypic hyperplastic nodules→ well differentiated HCC→ poorly differentiated HCC [1]. In this process, tumor blood supply gradually becomes arterialized. Arterial nourishment system has not completely built for relatively small lesions and may have a possibility of dual blood supply. Therefore, the enhancement pattern may not be typical [6,7].
In this study, in diagnosis of 1.0-2.0 cm HCC, CEUS showed a tolerable consistency with CECT in portal venous and delay phase. The possible causes may as follows: after arterial phase, SonoVue flows out of the lesion with the blood flow, and would not flow into the intercellular space. SonoVue and iodine contrast agent are different in biological behavior. In addition, the arterial nourishment system of 1.0-2.0 cm lesions has not built completely. Therefore, in diagnosis of 1.0-2.0 cm HCC, all of these causes may lead to a tolerable consistency between CEUS and CECT in portal venous and delay phase.
Based on the process of HCC under cirrhosis background, 2.1-3.0 cm lesions have a relatively more arterialized nourishment system. Thus the enhancements may be more typical than 1.0-2.0 cm lesions. Because the sizes of 1.0-2.0 cm lesions are smaller than that of 2.1-3.0 cm lesions, the slice scans and volume effect of CECT may have influence on imaging observation. This may be a relatively good explanation for the result that the two imaging methods have a better consistency for the diagnosis in 2.1-3.0 cm HCC.
Conclusion
CEUS and CECT have a relatively good consistency in the diagnosis of 2.1-3.0 cm lesions. However, with the diagnosis of 1.0-2.0 cm lesions, CEUS and CECT show a relatively poor consistency. CEUS may be considered as first-line imaging examination method in some special cases, such asrenal dysfunction, Iodine allergy or unsuitable for ray, et al.
Acknowledgements
This study was supported by Guangxi Natural Science Foundation (no. 2011GXNSFD018032), HCC Bridge Study (no. CA182023) and Guangxi scientific research and technological development projects (no. 14124003-4).
Disclosure of conflict of interest
None.
References
- 1.Egger C, Goertz RS, Strobel D, Lell M, Neurath MF, Knieling F, Scharf M. Dynamic contrast-enhanced ultrasound (DCE-US) for easy and rapid evaluation of hepatocellular carcinoma compared to dynamic contrast-enhanced computed tomography (DCE-CT)--a pilot study. Ultraschall Med. 2012;33:587–592. doi: 10.1055/s-0032-1325545. [DOI] [PubMed] [Google Scholar]
- 2.Khalili K, Kim TK, Jang HJ, Haider MA, Khan L, Guindi M, Sherman M. Optimization of imaging diagnosis of 1-2 cm hepatocellular carcinoma: an analysis of diagnostic performance and resource utilization. J Hepatol. 2011;54:723–728. doi: 10.1016/j.jhep.2010.07.025. [DOI] [PubMed] [Google Scholar]
- 3.Zheng SG, Xu HX, Liu LN. Management of hepatocellular carcinoma: The role of contrastenhanced ultrasound. World J Radiol. 2014;6:7–14. doi: 10.4329/wjr.v6.i1.7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Claudon M, Dietrich CF, Choi BI, Cosgrove DO, Kudo M, Nolsoe CP, Piscaglia F, Wilson SR, Barr RG, Chammas MC, Chaubal NG, Chen MH, Clevert DA, Correas JM, Ding H, Forsberg F, Fowlkes JB, Gibson RN, Goldberg BB, Lassau N, Leen EL, Mattrey RF, Moriyasu F, Solbiati L, Weskott HP, Xu HX. Guidelines and good clinical practice recommendations for contrast enhanced ultrasound (CEUS) in the liver--update 2012: a WFUMB-EFSUMB initiative in cooperation with representatives of AFSUMB, AIUM, ASUM, FLAUS and ICUS. Ultraschall Med. 2013;34:11–29. doi: 10.1055/s-0032-1325499. [DOI] [PubMed] [Google Scholar]
- 5.Maruyama H, Takahashi M, Ishibashi H, Yoshikawa M, Yokosuka O. Contrast-enhanced ultrasound for characterisation of hepatic lesions appearing non-hypervascular on CT in chronic liver diseases. Br J Radiol. 2012;85:351–357. doi: 10.1259/bjr/20440141. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Liu GJ, Xu HX, Lu MD, Xie XY, Xu ZF, Zheng YL, Liang JY. Correlation between enhancement pattern of hepatocellular carcinoma on real-time contrast-enhanced ultrasound and tumour cellular differentiation on histopathology. Br J Radiol. 2007;80:321–330. doi: 10.1259/bjr/54805002. [DOI] [PubMed] [Google Scholar]
- 7.Park YN. Update on precursor and early lesions of hepatocellular carcinomas. Arch Pathol Lab Med. 2011;135:704–715. doi: 10.5858/2010-0524-RA.1. [DOI] [PubMed] [Google Scholar]