

Abstract
Treatment engagement is a primary pathway to change. Because motivation consistently predicts engagement and sustained recovery following treatment, targeted efforts at improving problem recognition (i.e., a significant ingredient in motivation) during early weeks of treatment are critical. The purpose of this study is to compare the effectiveness of Standard Operating Practice (SOP) versus SOP plus an 8-session Treatment Readiness and Induction Program (TRIP; delivered in the first weeks of treatment) on cognitive indicators and treatment engagement among youth in 5 residential substance use treatment settings. Structural Equation Modeling (SEM) documented higher problem recognition, decision making, and treatment engagement (participation, satisfaction, counselor rapport) among youth receiving TRIP (compared to SOP only), even when controlling for background characteristics such as age, race-ethnicity, gender, baseline drug use severity, etc. Findings suggest that TRIP is an effective induction tool that directly impacts targeted constructs (i.e., problem recognition, decision making), and also directly affects indicators of engagement.
Keywords: Treatment motivation, adolescents, treatment readiness intervention, treatment engagement
1. Introduction
Treatment engagement is a primary means through which therapeutic change occurs. The concept can refer to an “intermediate step between initially accessing care (in a first visit) and completing a full course of treatment” (Garnick, Lee, Acevedo, Horgan, & the Washington Circle Public Sector Workgroup, 2007) or to level of participation during sessions (for example, actively contributing to discussion, developing relationships with counselors and peers). Measures of therapeutic involvement – participation in sessions, satisfaction with treatment, relationships with counselors, and perceived support from peers in treatment – are useful indicators of whether individuals are embracing or resisting the process of personal change (Cunningham, Duffee, Huang, Steinke, & Naccarato, 2009; Hawke, Hennen, & Gallione, 2005; Hiller, Knight, Leukefeld, & Simpson, 2002; Simpson, 2004; Simpson & Knight, 2001; Staton-Tindall et al., 2007). The more engaged an individual is in treatment, the stronger the commitment to change, the greater the personal transformation, and the greater the likelihood of sustained change after treatment discharge (Crits-Christoph et al., 2011; Diamond et al., 2006; Garnick et al., 2012; Simpson, Joe, Rowan-Szal, & Greener, 1995). Indeed, the influence of engagement in improving outcomes remains important, even when accounting for other factors such as legal pressures, DSM diagnoses, and demographics (Joe, Knight, Becan, & Flynn, 2014).
Barriers to successful engagement are numerous and include low motivation for change, cognitive challenges, poor relationships, and comorbidity, among others (Broome, Joe, & Simpson, 2001; Dakof, Tejeda, & Liddle, 2001; Hiller et al., 2002; Kaminer & Frances, 1991; Simpson & Joe, 2004). Motivation is pivotal in the engagement process for adults (Simpson, 2004), adolescents in general (Brown & Ramo, 2006), and adolescents referred to treatment by juvenile justice systems (Orlando, Chan, & Morral, 2003). Compared to adults, teens usually are less motivated to change (Melnick, De Leon, Hawke, Jainchill, & Kressel, 1997) and only 20% of those with symptoms indicative of substance abuse problems view their use as a “problem” (Titus & Dennis, 2006). While juvenile justice involvement may provide external motivation or pressure to remain in treatment for a determined length of time, youth under legal pressure exhibit lower motivation for treatment, which can negatively impact therapeutic engagement (Joe et al., 2014) – in other words, these youth are often “going through the motions” without actively engaging. Youth also face cognitive challenges that can interfere in decision making. Compared to adults, youth typically exhibit less preparedness for coping with difficult situations (Myers & Brown, 1990) and tend to place greater importance on social perceptions than on factual information about future consequences (Steinberg, 2007). As they mature, the ability to suppress or inhibit inappropriate thoughts and actions increases (see Casey, Jones, & Hare, 2008 for a review).
Because motivation or “readiness” (including problem recognition) consistently predicts retention, engagement, and the likelihood of sustained recovery following treatment (e.g., Broome et al., 2001; Callaghan et al., 2005; Joe et al., 2014, Melnick et al., 1997), targeted efforts at improving motivation are critical in the early weeks of treatment. Educational literature on academic motivation suggests that experiential activities and peer-to-peer interaction can facilitate motivation for learning (Master & Walton, 2013; Plass et al., 2013), increasing content knowledge, stimulating self-awareness, and fostering self-efficacy (O'Donnell et al., 1990; Young, 2005). Given that recovery from substance abuse involves learning to acknowledge personal problems and develop new strategies for coping with challenges (e.g., risk avoidance techniques, cognitive restructuring, and strengthening productive relationships), it is likely that the experiential and interactive principles that influence academic motivation are also applicable in therapeutic settings. Indeed, effective methods for engaging youth include high arousal activities that capture attention, followed by a transition to lower-arousal activities that promote self-reflection and personal insight (Perry et al., 2011). Interventions designed to boost problem recognition and decision making competencies through structured, interactive activities have the potential to impact treatment engagement as well.
Considering the aforementioned learning principles and approaches to facilitating motivation and engagement, evidence-based induction and readiness tools were adapted for adolescents in substance abuse treatment and bundled as the Treatment Readiness and Induction Program (TRIP). The goal of TRIP (Knight, Dansereau, Becan, Rowan, & Flynn, 2015) is to enhance therapeutic engagement (facilitate participation, strengthen therapeutic relationships) by improving readiness (problem recognition) and capacity (decision making) for personal change. Increasing readiness and capacity for change is accomplished through interactive modules and activities that promote problem recognition and more thoughtful, reasoned decision making. The TRIP intervention was designed as an enhancement to standard substance abuse treatment for adolescents and is based on a compilation of effective strategies and materials for engaging adults in treatment (e.g., Blankenship, Dansereau, & Simpson, 1999; Czuchry & Dansereau, 2000; Dees, Dansereau, & Simpson, 2002; Sia, Dansereau, & Czuchry, 2000). TCU Mapping Enhanced Counseling forms the core and serves to focus attention, facilitate communication, and visually illustrate concepts and ideas for better decision making (Dansereau & Simpson, 2009). Mapping is particularly effective for clients with attentional problems or lower cognitive functioning (Czuchry & Dansereau, 2004; Newbern, Dansereau, Czuchry, & Simpson, 2005) and leads to a more engaging counseling approach, especially when included with interactive games and peer mentoring (Czuchry, Sia, & Dansereau, 2006; Czuchry, Sia, Dansereau, & Dees, 1997). The intervention incorporates the use of guide maps or analytically created schemas that provide a structure for thinking through complex problems. Through practice, these schemas can be internalized and used to address everyday problems as they arise. “Helping individuals form more robust and effective schemas can serve to enhance judgment, decision-making, and self-regulation” (Dansereau, Knight, & Flynn, 2013, p. 278).
TRIP was designed to facilitate awareness of personal problems and to help youth make better choices (targeting decision making skills). Indeed, TRIP is effective for promoting decision making among youth in early phases of treatment. Compared to youth in residential settings who received standard operating practice, youth in TRIP reported greater gains in decision making competence (Knight et al., 2015). In addition, TRIP has been found to promote treatment motivation among adolescents, especially for those who have a low tendency to behave rashly when experiencing positive emotions (Becan, Knight, Crawley, Joe, & Flynn, 2015). While TRIP appears to be successful in promoting targeted skills, the degree to which it also promotes active participation and development of productive therapeutic relationships is unknown.
The purpose of this study is to expand on the impact that TRIP has on cognitive outcomes during treatment and examine the intervention's effectiveness in promoting engagement in residential substance use treatment. Because personal change occurs through active participation and development of productive relationships during treatment sessions, and because TRIP uses interactive activities to promote interpersonal communication and improve introspection, the primary hypothesis states that youth receiving TRIP sessions in addition to SOP during the first weeks of treatment will report better during-treatment outcomes than youth receiving SOP only. Two groups of youth entering 5 residential substance use treatment agencies were compared on during-treatment measures of problem recognition, decision making, and therapeutic engagement. The study design uses sequential comparison, whereby each treatment agency served as its own control (i.e., a separate sample pretest –posttest design; Campbell & Stanley, 1963) and controls for historical differences in client population characteristics.
2. Method
2.1. Procedures
Data were collected as part of an ongoing research project funded by the National Institute on Drug Abuse (NIDA; Grant R01DA013093). A sequential comparison design was used to gather data from 2 groups of adolescents enrolled in 5 community-based residential substance abuse treatment agencies from 2011 through 2013. This design was chosen because a randomized control trial could not be satisfactorily maintained in the residential programs (no assurance that control group members would not be exposed to the TRIP intervention material). To avoid contamination across groups, all agencies agreed to provide assessment data for a 6-month period before implementing TRIP with clients. Therefore, in this design, agency participation occurred in two phases (1) assessment only and (2) assessment and curriculum. Youth participated in only 1 phase (SOP or SOP+TRIP) and group assignment was made based their date of admission to the agency. This enabled a comparison between two groups: standard operating practice (SOP) versus SOP plus the TRIP curriculum (TRIP). For both groups, background, motivation, psychosocial functioning, and engagement data were collected at intake and during treatment. After an initial period (range: 5 to 8 months; average: 6 months), agency staff were trained to facilitate the TRIP intervention. Each agency incorporated the 8-session intervention into existing practice and implemented it with newly-admitted youth during their first month of treatment. Youth who enrolled in treatment during the initial 6-month period of data collection received standard operating practice (SOP) and comprised the SOP group. Youth who enrolled following the agency's adoption of the TRIP curriculum comprised the TRIP group. TRIP group data reported here reflect TRIP implementation over a 5-month period (an average of 6 intervention cycles). The TRIP group was an intent-to-treat sample; however, 80% of youth received 4 or more of the 8 TRIP sessions. To further reduce potential for cross-group influence (i.e., youth in the SOP group being exposed to TRIP concepts after staff were trained on TRIP but before TRIP groups began), all youth admitted to treatment within the 30 days prior to the agency's first TRIP group were excluded from the sample. Institutional Review Boards affiliated with the research institution and participating treatment agencies approved all research protocols.
Throughout the project, participating agencies were granted access to the Texas Christian University (TCU) Adolescent Screening and Assessment Package (TCU-ASAP) via an online assessment system developed and managed by the research team. Clinical staff within the participating agencies administered the TCU Adolescent Screening and Assessment Package (TCU-ASAP; Knight, Becan, Landrum, Joe, & Flynn, 2014) to newly-enrolled youth at intake (Time 1) and at 30-45 days into treatment (Time 2; during treatment). While the ideal target date for Time 2 data collection was Day 45 (to allow time for initial assessments plus completion of 8 TRIP sessions), youth admitted to the two shorter-term programs were encouraged to complete Time 2 at discharge, which often occurred at Day 30. The average time from treatment admission to when the time 2 instruments were given were 40.1 days (SD = 8.6; agency averages ranged from 32.1 to 49.4 days). Agency staff assigned identification numbers to newly enrolled clients which were then were used by staff to create online client accounts, schedule and administer assessments, and link assessment responses across time. Clients responded to assessment items independently with a staff coordinator available to assist when questions or problems arose. Assessment coordinators received in-depth training on how to log-in, setup client accounts, monitor and facilitate an assessment session, stop and start a session, track progress over time, print reports, and troubleshoot when problems arose. In addition to providing a mechanism for data collection, the online system produced automated real-time client-level assessment reports for staff to use in client documentation and treatment planning (Knight et al., 2014).
After approximately 6 months of assessment administration, agency staff were trained on the Treatment Readiness and Induction Program (TRIP; Bartholomew, Dansereau, Knight, Becan, & Flynn, 2012). Training covered the use of Mapping-Enhanced Counseling, an overview of session content, how to facilitate session activities, how to train and utilize peer mentors, and strategies for implementing the intervention at their particular site. Participating agencies received all materials needed to implement TRIP (manual, Downward Spiral game, and a flash drive with all curriculum and training materials). Attendees were responsible for conducting TRIP groups at their agencies and for training additional staff to ensure that the TRIP curriculum would continue in the event of staff turnover. Continuing education credits were awarded to trainees, and additional training support was provided upon request.
The TRIP manual includes detailed descriptions and materials list for each activity as well as clinical scripts for session facilitation (including prompts and processing questions). Each 90-minute module is structured to shift the interaction platform between lecture, didactic, individual, and group every 25 minutes. For example, in first “Work-it” session, youth watch a video where a magician uses a magic trick to demonstrate the importance of paying attention and following a set of steps when making a decision. Facilitators then walk the group through a decision making tool for decision making (W-O-R-K-I-T; “What's the problem?” “Think about Options,” “Rate it,” “Know what to do,” “Imagine the plan,” and “Test the results”). Youth then work in pairs to complete Work-it on a problem of their choosing.
TRIP implementation began at each agency approximately one month after TRIP training. Youth were placed in TRIP groups upon completion of intake assessments using an open-enrollment process. Agencies were asked to implement the 8-session curriculum within a 4-week period. Three agencies implemented TRIP during two 90-minute sessions per week (4-week cycles); 2 agencies implemented TRIP during four 90-minute sessions per week (2-week cycles).
TRIP facilitators were generally female (65%), white (76%) and had a Master's degree or were certified/licensed counselors (71%). Checklists on group attendance and fidelity to curriculum content were completed by group facilitators after each TRIP session (see Knight et al., 2014). Facilitators reported covering all prescribed content in 90% of sessions and used board/flip charts to map out group ideas in 96% of sessions.
2.2. Treatment agencies
The sample of youth was drawn from 5 community-based substance abuse treatment agencies located in urban, suburban, and rural communities within 3 states. The selection of residential TC programs for participation in the current study afforded researchers the opportunity to examine the effectiveness of TRIP when interfaced into a peer-emphasis standard operating practice. Two of the agencies were short-term residential (planned length of stay was less than 60 days), 2 were long-term residential (planned length of stay 60 days or more), and 1 had both short- and long-term “tracks” (the long-term track was comprised primarily of youth referred through juvenile justice agencies). All agencies used a modified therapeutic community (TC) approach as standard operating practice (SOP), which included a highly structured residential environment with on-campus schooling (provided through the local school district), individual and group counseling for substance use and related issues, vocational and skills training, case management linkage to social services, and the use of a phase system (youth earn privileges as they move from orientation to higher levels within the system).
2.3. Sample
There were 1228 adolescents admitted to treatment during the time period of the current study (2011-2013; SOP = 749, TRIP = 479). Of these, 1106 (90%; SOP = 656, TRIP = 450) completed the Time 1 assessments and reported demographic information, and 729 (59%) completed engagement assessments at Time 2 [SOP = 455 (61% of SOP admissions), TRIP = 274 (57% of TRIP admissions); 43% of these were no longer in treatment at Time 2]. A comparison of those who completed engagement assessments at Time 2 (N = 729) with the remaining individuals (N = 497) found that 60% of the former group had stayed in treatment at least 50 days compared to 39% of the latter group. It would appear dropout would be one reason for those not having engagement data, but it is not the primary reason. The lower completion rate for Time 2 assessments was also due to a combination of treatment-specific factors (e.g., early discharge due to physical altercations, leaving against medical advice) and non-treatment factors (e.g., staff forgetting to schedule Time 2, shifting of responsibility for Time 2 assessments from one staff member to another
An examination of variables on which the sample with during-treatment engagement data and the excluded sample that had no during treatment engagement data found that they differed significantly on demographics (gender, race), time in treatment, expectancy of being drug free, and legal pressure to be in treatment. Those in the no during-treatment engagement sample tended to have a higher percentage of males (71% vs. 61%), to have more African-Americans (8% vs. 5%) and more other race (9% vs. 6%). The no during-treatment engagement sample also was more likely to be in treatment for 30 days or less (34% vs. 2%). Their scores on expectancy of being drug free was also lower (36.6 vs. 38.0). A smaller percentage of them also had legal pressure (31% vs. 40%). In contrast, the two samples did not differ significantly on age, being in school, having dropped out of school, in juvenile detention, living on the street, in drug treatment, ever having been treated for mental problems, premeditation, optimism and hope, assertiveness, drug control, self esteem, self efficacy in problem solving, and self efficacy in resisting drugs.
Subsequent structural models that included all additional covariates (e.g., hostility) to account for differences between the SOP and TRIP groups were based on a sample of 603 (SOP = 361, TRIP = 242).
2.4. Measures
2.4.1. Group
Youth admitted to treatment at least 30 days prior to the agency's initiation of TRIP groups comprised the SOP group, while youth admitted to treatment after the agency began conducting TRIP sessions comprised the TRIP group (SOP = -1 vs TRIP = 1).
2.4.2. During-treatment outcomes
Dependent measures were assessed at Time 2 and include scales that have been used in previous studies (e.g., Becan et al., 2015; Knight et al., 2015). Engagement scales from the adolescent version of the Client Evaluation of Self and Treatment (CEST; Knight et al., 2014) measured youth's perceptions of their treatment participation (11 items, coefficient alpha = .92), treatment satisfaction (6 items, coefficient alpha = .82), rapport with counselors (counselor rapport; 12 items, coefficient alpha = .94), and support received from peers in treatment (peer support; 5 items, coefficient alpha = .82). Cognitive measures, also from the CEST, included assessments of drug-related problem recognition (10 items, coefficient alpha = .89) and decision making (8 items, coefficient alpha = .78). The items from the CEST were measured using a Likert scale (1 = disagree strongly, 2 = disagree, 3 = uncertain, 4 = agree, 5 = agree strongly).
2.4.3. Covariates
Because participants were not randomly assigned to the SOP or TRIP groups, it is important to control for potential baseline differences between the participant groups on factors that might possibly affect the study's outcomes. Demographic and baseline covariates— including gender, age, race-ethnicity, drug use severity, legal pressure, and mental health treatment—were selected based on indications that these factors have the potential to influence the treatment process (e.g., Austin, Hospital, Wagner, & Morris, 2010; Barnett et al., 2002; Catalano, Hawkins, Wells, Miller, & Brewer, 1990; Crowley, Mikulich, MacDonald, Young, & Zerbe, 1998; Fickenscher et al., 2006; Melnick, De Leon, Hawke, Jainchill, & Kressel, 1997; Rivers, Greenbaum, & Goldberg, 2001; Wise, Cuffe, & Fischer, 2001). Without controlling for these influences, it may be more difficult to associate outcomes to TRIP.
Background characteristics, such as gender, age, and ethnicity/race were collected from the TCU RSK forms (Simpson, Joe, Knight, Rowan-Szal, & Gray, 2012) at Time 1. Drug use data (drug use severity, 9 items, coefficient alpha = .82) was gathered using the TCU Drug Screen II (TCUDS II; Knight, Simpson, & Hiller, 2002). The Legal Pressure measure was a single item from the TCU MOT form (Motivation; “You have legal problems that require you to be in treatment”). Youth responded using a Likert scale (1 = disagree strongly, 2 = disagree, 3 = uncertain, 4 = agree, 5 = agree strongly). Hostility was measured from the TCU SOC form and consists of 8 items, each scored on a 5-point Likert scale (Knight et al, 2014) coefficient alpha reliability of .84). School enrollment was defined as having been enrolled in school in the 30 days prior to intake. Mental health treatment was defined as having ever been treated for mental health problems during the youth's lifetime. Both items were from the TCU RSK form and coded as 1 = no or 2 = yes.
Other variables used only in predicting participants with complete data versus no engagement data included risk taking (TCU SOC form, 7 items, coefficient alpha = .76), self-esteem (TCU PSY form, 6 items, coefficient alpha = .81), expectancy for drug use (TCU PSY form, 4 items, coefficient alpha = .83), and four scales from the TCU ADOL THK Form, including premeditation (6 items, coefficient alpha = .85), assertiveness (5 items, coefficient alpha = .79), optimism/hope (5 items, coefficient alpha = .56), and drug culture (6 items, coefficient alpha = .86).
2.5. Analysis plan
The present study compared during-treatment outcomes (month 2 treatment participation, treatment satisfaction, counselor rapport, peer support, problem recognition, decision making) for the SOP and TRIP groups. Analyses proceeded in two steps: examination of differences in background characteristics among the samples and examination of the hypothesis using Structural Equation Modeling (SEM).
In the first step, analysis of variance was used to identify potential differences between the samples (complete data versus Time 2 missing) and groups within each sample (SOP versus TRIP) on demographic and other background variables of interest. The t-tests from each of the analyses of variance are reported in Table 1 for identifying significant differences. In the second step, SAS PROC CALIS (SAS Institute Inc., 2009) was used to test the significance of TRIP vs. SOP, estimating the six dependent variables simultaneously. The initial structural equation model (SEM) tested was a simultaneous test that TRIP had significantly higher means than SOP for each of the six dependent variables. A significant positive path coefficient from the TRIP vs. SOP measure (where SOP = -1 and TRIP = 1) to each dependent variable would be an indicator in support of the hypothesis. This initial structural model was based on the maximum number of youth available (N = 729; SOP = 455, TRIP = 274). The second model included covariates as predictors of each dependent variable in order to adjust for possible baseline differences between the SOP and TRIP samples (N= 603; SOP = 361, TRIP = 242). There was a reduction in the sample available due to missing data on the covariates that were used. Drug use severity was the covariate with the most missing data; 74 individuals in the SOP group and 17 individuals in the TRIP group did not have information of this covariate. The third model included an engagement latent variable as a dependent variable (including Participation, Satisfaction, and Rapport) and the covariates.
Table 1. Background for Standard Operating Practice (SOP) and Treatment Retention and Induction Program (TRIP) Groups by Engagement Measure Availability.
| Engagement Form Availability | Comparison within SOP and TRI | ||||||||
|---|---|---|---|---|---|---|---|---|---|
|
| |||||||||
| Variables | Total | No Engagement Measures (NE) | Engagement (E) (Study Sample) | SOP NE vs. E | TRIP NE vs. E | ||||
|
| |||||||||
| SOP | TRIP | t-test | SOP (E) | TRIP (E) | t-test | t-test | t-test | ||
| N | 1228 | 294 | 205 | 455 | 274 | ||||
| Male | 65% | 69% | 74% | -1.1 | 62% | 58% | 1.0 | -2.0* | -3.5*** |
| Race-ethnicityb | |||||||||
| White | 21% | 24% | 15% | 2.4* | 18% | 26% | -2.3* | -1.7† | 2.9** |
| Black | 5% | 8% | 6% | 1.1 | 5% | 3% | 1.0 | -1.8† | -1.35 |
| Hispanic | 67% | 58% | 73% | -3.6*** | 71% | 67% | 1.0 | 3.5*** | -1.5 |
| Other race | 7% | 10% | 6% | 1.9+ | 6% | 4% | .9 | -2.2+ | -.7 |
| School Enrollment a | 75% | 70% | 76% | -1.6 | 71% | 83% | -3.5*** | .3 | 1.6 |
| Mental Health Txe | 30% | 38% | 18% | 4.6*** | 31% | 28% | .8 | -2.0† | 2.4* |
| Agea | 15.8 (1.1) | 15.8 (1.1) | 15.9 (1.0) | -1.1 | 15.7 (1.1) | 15.7 (1.1) | .0 | -.9 | -1.8† |
| TCU drug severityc | 2.6 (2.7) | 5.5 (2.7) | 5.5 (2.7) | .1 | 5.5 (2.6) | 5.9 (2.8) | -1.9† | .2 | 1.9† |
| Legal Pressure d | 2.9 (1.3) | 2.6 (1.3) | 3.0 (1.3) | -2.7** | 2.9 (1.3) | 2.9 (1.4) | -.3 | 2.4* | -.5 |
| Hostility (month 1)e | 27.9 (8.3) | 28.0 (8.5) | 28.4 (7.8) | -.5 | 27.9 (8.3) | 27.4 (8.4) | .7 | -.1 | -1.2 |
p < .10,
p < .05,
p < .01,
p < .001,
p < .0001
Total n = 1106;
Total n = 1161;
Total n = 1051,
Total n = 1096,
Total n = 1101.
In interpreting the fit of the model to the data, the goodness-of-fit chi-square, the root mean square residual (RMSEA), the standardized root mean square residual (SRMSR) the comparative fit index (CFI), and the Bentler-Bonett normed fit index (NFI) are reported. Because the chi-square test of model fit may be sensitive to sample sizes larger than 200, a significant chi-square may not be a satisfactory indicator of the model fit. As noted in Schumacker and Lomax (2004), if the normed chi-square (computed as chi-square divided by its degrees of freedom) is less than 3.84, then this may be a better indicator of the data fitting the model. RMSEA values of .01, .05, and .08 indicate excellent, good, and mediocre fit respectively (MacCallum, Browne, & Sugawara, 1996). For SRMSR, a value less than .08 is considered a good fit (Hu & Bentler, 1998). The CFI ranges from 0 to 1, with values above 0.9 indicating reasonable fit. For NFI, values of .90 to .95 reflect a good model fit.
3. Results
3.1. Sample differences in background characteristics
Background information for the two primary samples (study sample with complete data versus sample with no engagement measures) is presented in Table 1. Adolescents in the original sample (n = 1228) were nearly 16 years old on average, mostly male (65%), and Hispanic (67%) or White (21%). As reported in Table 1, differences existed between samples. Males were more likely to have missing engagement data compared to females (in both SOP and TRIP groups), TRIP youth with engagement data were more likely to be white, SOP youth without engagement data were more likely to be under legal pressure, and TRIP youth without engagement data were less likely to have been treated for mental health problems in the past. Bivariate correlations also indicated group differences on the dependent variables (see Table 2). Youth in TRIP reported higher problem recognition, decision making, counselor rapport, treatment satisfaction, and peer support at time 2.
Table 2. Means and Correlation Coefficients for Dependent Variables Comparing SOP and TRIP Groups.
| Dependent Variables | Total (N = 729) Mean (SD) | SOP (n = 455) Mean (SD) | TRIP (n = 274) Mean (SD) | Between Group R |
|---|---|---|---|---|
| Problem Recognition | 34.9 (8.8) | 33.9 (8.7) | 36.6 (8.8) | .14**** |
| Decision Making | 35.2 (6.4) | 34.6 (6.3) | 36.2 (6.5) | .12** |
| Treatment Participation | 40.0 (5.9) | 39.8 (5.4) | 40.3 (6.6) | .05 |
| Counselor Rapport | 39.7 (6.6) | 39.3 (6.3) | 40.5 (7.0) | .09* |
| Treatment Satisfaction | 38.6 (6.7) | 38.1 (6.3) | 39.4 (7.4) | .10** |
| Peer Support | 35.7 (6.5) | 35.2 (6.4) | 36.4 (6.7) | .09* |
3.2. Examination of group differences using SEM
The initial model indicated that five of the six paths from the intervention variable (TRIP vs. SOP) were significant (the exception being treatment participation), and the direction of the signs of the standardized weights were all positive {[Participation: b = .05 (se =.04), t = 1.32]; [Satisfaction: b = .10 (se = .04), t = 2.68**]; [Rapport: b = .09 (se = .04), t = 2.55**]; [Peer Support: b = .09 (se = .04), t = 2.45**]; [Problem Recognition: b = .14 (se = .04), t = 3.96***]; [Decision Making: b = .12 (se = .04), t = 3.24***]. Thus, TRIP participants had higher mean scores on treatment satisfaction, counselor rapport, peer support, problem recognition, and decision making at Time 2 compared to SOP participants. However, evaluation of the fit statistics for this model indicated a poor fit (χ2(1) = 44.3088, p < .000, CFI = .98, – NFI = .98, GFI = .98; RMSEA = .244 (.187, .309), SRMSR = .069).
To determine whether significant path results from the first model were due to sample differences, a second model was tested with covariates added as predictors of each of the dependent variables. Although nearly every dependent variable was significantly predicted by at least one of the covariates, the pattern of significant results for group (TRIP versus SOP) was similar to that found in model 1 {[Participation: b = .05 (se = .04), t = 1.15]; [Satisfaction: b = .12 (se = .04), t = 3.04**]; [Rapport: b = .09 (se = .04), t = 2.26*]; [Peer Support: b = .12 (se = .04), t = 2.89**]; [Problem Recognition: b = .19 (se = .04), t = 5.38***]; [Decision Making: b = .11 (se = .04), t = 2.76**] }. The covariates differed as significant predictors for the dependent variables. For each dependent variable these covariates were as follows: Participation (race-ethnicity), Satisfaction (school), Rapport (none), Peer Support (gender, hostility), Problem Recognition (gender, legal pressure, hostility, ever treated for mental problem, drug use severity), Decision Making (gender, age). While this estimated model yielded interesting results, it was not a good fit for the data (χ2(4) = 144.0842, p < .0001, CFI = .95, NFI = .95, GFI = .97; RMSEA = .242 (.209, .277), SRMSR = .072).
Modification indices suggested that some of the engagement variables were highly correlated, and a latent variable comprised of these might be useful in the model. Therefore, a re-conceptualization of model 2 was tested with treatment participation, treatment satisfaction, and counselor rapport used as indicators of a latent variable representing treatment engagement. This estimated model had a better fit (χ2(22) = 49.7995, p < .0006, CFI = .99, NFI = .98, GFI = .99; RMSEA = .046 (.029, .063), SRMSR = .012). All fit indices improved (especially the SRMSR, which changed from .072 to .012). In this model (see Figure 1), the intervention variable is significantly related to the latent engagement variable and to the other outcomes (peer support, problem recognition, and decision making) {[Engagement latent variable: b = .09 (se = .04), t = 2.16*]; [Peer Support: b = .12 (se = .04), t = 2.89**]; [Problem Recognition: b = .19 (se = .04), t = 5.38****]; [Decision Making: b = .14 (se = .04), t = 3.50***]}. For the corresponding paths from the covariates, it was seen that each dependent variable was significantly related to at least two covariates as follows (see Table 3): Problem Recognition (male, legal pressure, higher hostility, mental health treatment, lower drug use severity), Decision Making (male, older), Peer Support (male, lower hostility), and Engagement latent variable (male, not enrolled in school). TRIP participants had significantly better during-treatment outcomes than SOP, and these differences were not due to the sample characteristics addressed. The fact that some covariates were also significantly related to engagement suggests that further studies will need to investigate the extent to which interactions occur. The present analyses were limited to each predictor controlling for the effects of the other predictors.
Figure 1.
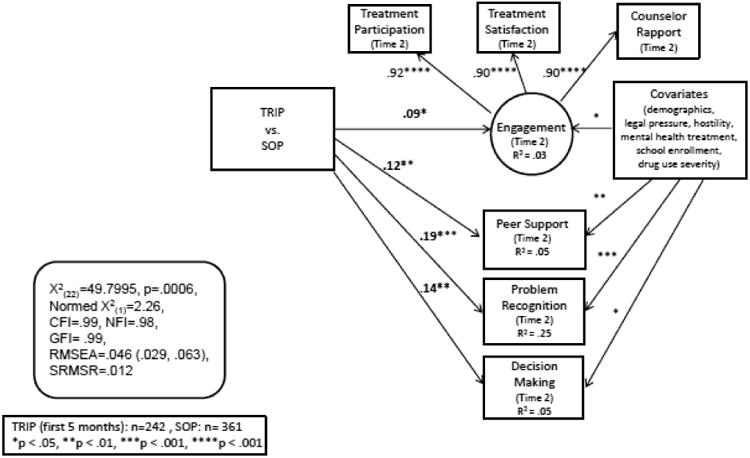
Engagement and cognitive outcomes at Month 2: TRIP vs. SOP.
Table 3. Standardized B-Weights for Covariates Predicting Dependent Variables.
| Dependent Variables in Structural Equation Model (N = 603) | ||||
|---|---|---|---|---|
| Covariates | Problem Recognition | Decision Making | Peer Support | Engagement |
| Male | .16**** | .12** | .12** | .09* |
| Age | .02 | .09* | -.04 | .05 |
| White | .04 | .05 | -.04 | .04 |
| Legal Pressure | .13** | .04 | .04 | .05 |
| Hostility | .11* | -.04 | -.13** | -.08+ |
| Mental Health Treatment | .09* | .01 | .01 | .03 |
| School Enrollment | -.05 | -.01 | -.07+ | -.08* |
| Drug Severity | -.34**** | .05 | .01 | -.03 |
p< .10,
p< .05,
p < .01,
p < .001,
p < .0001
4. Discussion
This study documents the effectiveness of TRIP for promoting during-treatment outcomes. After approximately one month in treatment, youth receiving standard practice plus TRIP groups had higher problem recognition, higher decision making, and were more engaged in treatment compared to youth receiving standard practice alone. The present research suggests that the effects of the TRIP curriculum can occur within the first month of residential treatment, indicating that the curriculum can serve as an early induction tool. These effects exist even when controlling for possible background differences between the TRIP and SOP samples (i.e., age, race-ethnicity, gender, baseline drug use severity, external pressures such as legal problems, enrolled in school at intake, and prior mental treatment). Findings affirm prior studies demonstrating the effectiveness of TRIP in improving motivation for treatment and promoting the use of more thoughtful, objective decision making strategies (Becan et al., 2015; Knight et al., 2015). The TRIP curriculum was specifically designed to target these areas. It uses graphical approaches (including analytically-created schemas; Dansereau et al., 2013) to assist youth in exploring underlying causes and consequences of personal choices, identifying social networks and internal competencies available to help when making daily decisions, and practicing strategies for making more methodical and less impulsive choices. These activities facilitate realistic self-assessment regarding the severity of drug problems and improve decision making confidence.
While the literature suggests that improvements in motivation result in stronger treatment engagement (Broome et al., 2001; Callaghan et al., 2005; Joe et al., 2014, Melnick et al., 1997), this study documents that participating in TRIP activities also directly promotes higher treatment satisfaction and better relationships with counselors. Through these structured activities, TRIP appears to facilitate an appropriate balance between experiential and analytic decision making systems (Dansereau et al., 2013). By design, TRIP uses social interaction and experiential activities to maintain attention, encourage appropriate self-disclosure, and facilitate peer interaction throughout each session, thereby increasing the likelihood of individual participation (Dansereau et al., 2013). Mapping-Enhanced Counseling (Czuchry & Dansereau, 2003; Dansereau & Dees, 2002) forms the structural basis of TRIP and promotes communication between counselor and client and among youth in the group. Analytically-created schemas (i.e., structured maps) direct thinking in logical sequences, and fictitious scenarios make sharing answers less risky. Experiential games are used to demonstrate thinking strategies and consequences of risky behavior, and peer-to-peer mentoring and collaborative learning strategies are embedded throughout all activities. Findings from this study indicate that this approach appears to be effective for facilitating higher engagement in the general treatment process among adolescents.
The finding that youth in TRIP report greater support for recovery among peers could also be attributed to TRIP's deliberate involvement of peers who are more experienced in treatment and recovery as mentors during group sessions. Because youth often place greater value on what they believe their peers think than on potential consequences of their actions (Steinberg, 2007), interventions aimed at strengthening prosocial peer support may be instrumental in promoting change both directly through positive peer influences on thinking and decision making and indirectly through more active engagement in the treatment process.
Although the primary function of including covariates in analyses was to control for potential group differences, it is worth noting that some covariates were significantly related to specific outcomes. In the final structural model, gender was related to all outcomes, with males reporting higher scores than females. Higher problem recognition was related to lower drug severity, higher hostility, legal pressure, and mental health treatment. Decision making was higher among older youth. Higher peer support was associated with lower hostility and higher engagement was associated with not having been in school during the 30 day period prior to treatment admission. To fully understand how these factors contribute to differential outcomes among youth in TRIP, future studies should explore their interactions with other factors. For example, youth who have greater affinity toward school may respond more favorably to analytical activities within the TRIP curriculum. Likewise, older youth may enter treatment with better decision making skills and competence than their younger counterparts. These factors could differentially affect the effectiveness of TRIP, leading to insights on how the curriculum could be tailored for specific age or competency groups.
The current study documents the utility of TRIP in promoting during-treatment outcomes, however, several limitations should be noted. First, data are restricted to youth admitted to residential treatment settings. Although agency characteristics, locations, and length varied across the 5 settings, findings may not generalize to all residential programs or to other modalities such as outpatient, day treatment, or aftercare. In outpatient settings, the average number of contact hours (e.g., sessions per week) is typically fewer; therefore, an 8-session group format may have to be adapted (e.g., shortening session length, omitting content, spanning 8 weeks instead of 4). Furthermore, group composition is more variable from week to week in outpatient settings, which could potentially impact the effectiveness of peer-to-peer interaction (e.g., potentially less disclosure when group membership changes each time) or interrupt the continuity of discussion from one session to the next. Future studies should examine what types of adaptations are needed for TRIP to fit into non-residential modalities and determine whether adapted versions of TRIP remain effective in promoting desired outcomes. Additionally, while the Treatment Episode Data Set (2010) indicate that 8.5% and 10.1% of youth in short term and long term residential (respectively) reported Hispanic ethnicity, the agencies involved in this study serve a high proportion of Hispanic youth. Therefore, although TRIP appears to be effective with Hispanic youth (suggesting that culture or language may not serve as a barrier), the oversampling could serve as a limitation of this study.
Because the aim of the study was to examine during-treatment outcomes, one sample inclusion criterion was that youth remained in treatment long enough to complete Time 2 assessments (approximately 1 month). A sizeable proportion of youth were missing time 2 data, and these youth were more likely to be male, African-American, and in treatment for less than 30 days. Some who left early may have done so for legitimate reasons (i.e., limited funding) and therefore were not missing at random. Thus, findings cannot be generalized to youth who dropped out of treatment before this criterion was met, nor can inferences be made about the potential relationship between participation in TRIP and length of stay. In an attempt to address how the omission of these individuals might have affected study findings, engagement measures were imputed for youth with missing data (using stepwise multiple regression weights), with predicted scores used as dependent variables in ANOVAs comparing TRIP versus SOP. Results were significant only for decision making (TRIP higher than SOP; t = 1.99; p < .05). Findings are inconclusive, however, because only small percentages of variance can be accounted for: decision making (22%), problem recognition (14.7%), and treatment participation (12.8%).
Additional research is needed to determine if gains in problem recognition result in longer treatment stays (even if only by a few days) or if gains in decision making early in treatment promote longer retention and more successful completion rates. The models tested in the current study focused on the direct impact of TRIP on during-treatment outcomes. However, prior research suggests that problem recognition and decision making improve over time, and that gains are greater among youth participating in TRIP, compared to SOP (Becan et al., 2015; Knight et al., 2015). Prior studies also suggest that motivation for change plays a role in promoting engagement (Brown & Ramo, 2006; Orlando, Chan, & Morral, 2003). It is possible that the effect that TRIP has on engagement can be fully or partially explained by gains in motivation during treatment (i.e., where improved problem recognition functions as a mediator) or different levels of decision making competence at treatment entry (baseline functioning level may moderate TRIP's effectiveness). However, these questions were beyond the focus of the present study.
In addition to these above areas of inquiry, analyses from the current study documenting relationships between covariates and study outcomes suggest that future studies should explore which subgroups of youth benefit most from TRIP. It may be that for some, experiential, peer-interaction-based activities serve to promote genuine self-expression and treatment buy-in; for others, such activities may be uncomfortable or threatening and may promote withdrawal or hostility. It is possible that for this latter group, certain activities within TRIP sessions may be counter-productive. Future models should also examine the sequential nature of the treatment process, including measures of engagement later in treatment in order to more fully explore change over time. Exploring differential patterns among key variables for TRIP versus SOP clients may illuminate whether TRIP creates a synergy among factors affecting engagement. For instance, relationships among motivation, decision making, and engagement would potentially be more strongly correlated among TRIP clients.
To help youth make significant progress during their limited time in treatment, it is important to utilize practices that facilitate active participation and commitment to change. Indeed, interventions should build upon youths' interests, capitalize on their creativity (by promoting self-expression through non-threatening activities), and utilize their desire for peer connections. Findings from this study suggest that interventions like TRIP that incorporate a blend of activities and strategies for promoting and sustaining attention and active participation can be beneficial not only for improving the targeted content areas (in this case problem recognition and decision making), but also in promoting treatment engagement during the first month of treatment. The earlier and more fully youth engage in the treatment process, the greater the impact interventions can have.
Highlights.
The study compares the effectiveness of Standard Operating Practice (SOP) versus SOP plus an 8-session Treatment Readiness and Induction Program (TRIP; delivered in the first weeks of treatment) on cognitive indicators and treatment engagement among youth in residential substance abuse treatment
Youth in TRIP had higher problem recognition, decision making, and treatment engagement (participation, satisfaction, counselor rapport)
Youth in TRIP reported greater support for recovery among peers in treatment
Group differences remained after controlling for background characteristics such as age, race-ethnicity, gender, baseline drug use severity
TRIP is effective for promoting early treatment induction among youth entering substance use treatment
Acknowledgments
This work was funded by the National Institute on Drug Abuse (NIDA; Grant R01DA013093). The interpretations and conclusions, however, do not necessarily represent the position of the NIDA, National Institutes of Health, or Department of Health and Human Services. The authors would like to acknowledge the contributions of administrators and clinical staff at participating agencies who worked diligently to insure that assessment and curriculum protocols were implemented with fidelity.
Footnotes
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final citable form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
References
- Austin A, Hospital M, Wagner EF, FMorris SL. Motivation for reducing substance use among minority adolescents: Targets for intervention. Journal of Substance Abuse Treatment. 2010;39(4):399–407. doi: 10.1016/j.jsat.2010.07.008. [DOI] [PubMed] [Google Scholar]
- Barnett NP, Lebeau-Craven R, Wollard R, Rohsenow DJ, Spiriro A, Monti PM. Predictors of motivation to change after medical treatment for drinking-related events in adolescents. Psychology of Addictive Behaviors. 2002;16:106–112. [PubMed] [Google Scholar]
- Bartholomew NG, Dansereau DF, Knight DK, Becan JE, Flynn PM. Fort Worth: Texas Christian University, Institute of Behavioral Research; 2013. Treatment Readiness and Induction Program (TRIP) Available at www.tcu.edu. [Google Scholar]
- Becan JE, Knight DK, Crawley RD, Joe GW, Flynn PM. Effectiveness of the Treatment Readiness and Induction Program for increasing adolescent motivation for change. Journal of Substance Abuse Treatment. 2015;50:38–49. doi: 10.1016/j.jsat.2014.10.002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Blankenship J, Dansereau DF, Simpson DD. Cognitive enhancements of readiness for corrections-based treatment for drug abuse. The Prison Journal. 1999;79(4):431–445. [Google Scholar]
- Broome KM, Joe GW, Simpson DD. Engagement models for adolescents in DATOS-A. Journal of Adolescent Research. 2001;16(6):608–623. [Google Scholar]
- Brown SA, Ramo DE. Clinical course of youth following treatment for alcohol and drug problems. In: Liddle HA, Rowe CL, editors. Adolescent substance abuse: Research and clinical advances. Cambridge, NY: Cambridge University Press; 2006. [Google Scholar]
- Callaghan RC, Hathaway A, Cunningham JA, Vettese LC, Wyatt S, Taylor L. Does stage-of-change predict dropout in a culturally diverse sample of adolescents admitted to inpatient substance-abuse treatment? A test of the Transtheoretical Model. Addictive Behaviors. 2005;30:1834–1847. doi: 10.1016/j.addbeh.2005.07.015. [DOI] [PubMed] [Google Scholar]
- Campbell DT, Stanley JC. Experimental and quasi-experimental designs for research. Chicago, IL: Rand McNally College Publishing Company: 1963. [Google Scholar]
- Casey BJ, Jones RM, Hare TA. Annals of the New York Academy of Sciences. 2008. The adolescent brain; pp. 111–126. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Catalano RF, Hawkins J, Wells EA, Miller JL, Brewer DD. Evaluation of the effectiveness of adolescent drug abuse treatment, assessment of risks for relapse, and promising approaches for relapse prevention. International Journal of the Addictions. 1990;25(9A-10A):1085–1140. doi: 10.3109/10826089109081039. [DOI] [PubMed] [Google Scholar]
- Crits-Christoph P, Hamilton JL, Ring-Kurtz S, Gallop R, McClure B, Kulaga A, Rotrosen J. Program, counselor, and patient variability in the alliance: A multilevel study of the alliance in relation to substance use outcomes. Journal of Substance Abuse Treatment. 2011;40(4):405–413. doi: 10.1016/j.jsat.2011.01.003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Crowley TJ, Mikulich SK, MacDonald M, Young SE, Zerbe GO. Substance-dependent, conduct-disordered adolescent males: Severity of diagnosis predicts 2-year outcome. Drug and Alcohol Dependence. 1998;49(3):225–237. doi: 10.1016/s0376-8716(98)00016-7. [DOI] [PubMed] [Google Scholar]
- Cunningham WS, Duffee DE, Huang Y, Steinke CM, Naccarato T. On the meaning and measurement of engagement in youth residential treatment centers. Research on Social Work Practice. 2009;19(1):63–76. doi: 10.1177/1049731508314505. [DOI] [Google Scholar]
- Czuchry M, Dansereau DF. Drug abuse treatment in criminal justice settings: Enhancing community engagement and helpfulness. American Journal of Drug and Alcohol Abuse. 2000;26(4):537–552. doi: 10.1081/ada-100101894. [DOI] [PubMed] [Google Scholar]
- Czuchry M, Dansereau DF. A model of the effects of node-link mapping on drug abuse counseling. Addictive Behaviors. 2003;28(3):537–549. doi: 10.1016/s0306-4603(01)00252-0. [DOI] [PubMed] [Google Scholar]
- Czuchry M, Dansereau DF. The importance of need for cognition and educational experience in enhanced and standard substance abuse treatment. Journal of Psychoactive Drugs. 2004;36(2):243–251. doi: 10.1080/02791072.2004.10399735. [DOI] [PubMed] [Google Scholar]
- Czuchry M, Sia TL, Dansereau DF. Improving early engagement and treatment readiness of probationers: Gender differences. The Prison Journal. 2006;86(1):56–74. [Google Scholar]
- Czuchry M, Sia TL, Dansereau DF, Dees SM. Downward Spiral: A pedagogical game depicting the dangers of substance abuse. Journal of Drug Education. 1997;27(4):373–387. doi: 10.2190/3VEK-GQE2-4VFT-L2XH. [DOI] [PubMed] [Google Scholar]
- Dakof GA, Tejeda M, Liddle HA. Predictors of engagement in adolescent drug abuse treatment. Journal of the American Academy of Child and Adolescent Psychiatry. 2001;40(3):274–281. doi: 10.1097/00004583-200103000-00006. [DOI] [PubMed] [Google Scholar]
- Dansereau DF, Dees SM. Mapping training: The transfer of a cognitive technology for improving counseling. Journal of Substance Abuse Treatment. 2002;22(4):219–230. doi: 10.1016/s0740-5472(02)00235-0. [DOI] [PubMed] [Google Scholar]
- Dansereau DF, Knight DK, Flynn PM. Improving adolescent judgment and decision making. Professional Psychology Research and Practice. 2013;44(4):274–282. doi: 10.1037/a0032495. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Dansereau DF, Simpson DD. A picture is worth a thousand words: The case for graphic representations. Professional Psychology: Research & Practice. 2009;40(1):104–110. [Google Scholar]
- Dees SM, Dansereau DF, Simpson DD. Implementing a readiness program for mandated substance abuse treatment. Offender Substance Abuse Report. 2002;11(2):17–32. [Google Scholar]
- Diamond GS, Liddle HA, Wintersteen MB, Dennis ML, Godley SH, Tims F. Early therapeutic alliance as a predictor of treatment outcome for adolescent cannabis users in outpatient treatment. American Journal on Addictions. 2006;15(Suppl 1):26–33. doi: 10.1080/10550490601003664. [DOI] [PubMed] [Google Scholar]
- Fickenscher A, Novins D, Beals J. A pilot study of motivation and treatment completion among American Indian adolescents in substance abuse treatment. Addictive Behaviors. 2006;31:1402–1414. doi: 10.1016/j.addbeh.2005.11.001. [DOI] [PubMed] [Google Scholar]
- Garnick D, Lee M, Acevedo A, Horgan C the Washington Circle Public Sector Workgroup. Specifications for Washington Circle Public Sector Performance Measures: Initiation, engagement, and continuity of care measures for state substance abuse agencies. 2007 Jun; Retrieved May 28, 2015 from http://www.washingtoncircle.org/pdfs/9a1.pdf.
- Garnick DW, Lee MT, O'Brien PL, Panas L, Ritter GA, Acevedo A, et al. Godley MD. The Washington circle engagement performance measures' association with adolescent treatment outcomes. Drug and Alcohol Dependence. 2012;124(3):250–258. doi: 10.1016/j.drugalcdep.2012.01.011. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hawke JM, Hennen J, Gallione P. Correlates of therapeutic involvement among adolescents in residential drug treatment. The American Journal of Drug and Alcohol Abuse. 2005;1:163–177. doi: 10.1081/ADA-200047913. [DOI] [PubMed] [Google Scholar]
- Hiller ML, Knight K, Leukefeld C, Simpson DD. Motivation as a predictor of therapeutic engagement in mandated residential substance abuse treatment. Criminal Justice and Behavior. 2002;29:56–75. [Google Scholar]
- Hu L, Bentler PM. Fit indices in covariance structure modeling: Sensitivity to underparameterized model misspecification. Psychological Methods. 1998;3:424–453. [Google Scholar]
- Joe GW, Knight DK, Becan JE, Flynn PM. Recovery among adolescents: Models for post-treatment gains in drug abuse treatments. Journal of Substance Abuse Treatment. 2014;46:362–373. doi: 10.1016/j.jsat.2013.10.007. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kaminer Y, Frances RJ. In-patient treatment of adolescents with psychiatric and substance abuse disorder. Hospital and Community Psychiatry. 1991;42:894–896. doi: 10.1176/ps.42.9.894. [DOI] [PubMed] [Google Scholar]
- Knight DK, Becan JE, Landrum B, Joe GW, Flynn PM. Screening and assessment tools for measuring adolescent client needs and functioning in substance abuse treatment. Substance Use & Misuse. 2014;49(7):902–918. doi: 10.3109/10826084.2014.891617. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Knight DK, Dansereau DF, Becan JE, Rowan GA, Flynn PM. Effectiveness of a theoretically-based judgment and decision making intervention for adolescents. Journal of Youth and Adolescence. 2015;44:1024–1038. doi: 10.1007/s10964-014-0127-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Knight K, Simpson DD, Hiller ML. Screening and referral for substance-abuse treatment in the criminal justice system. In: Leukefeld CG, Tims F, Farabee D, editors. Treatment of drug offenders: Policies and issues. New York: Springer; 2002. pp. 259–272. [Google Scholar]
- MacCallum RC, Browne MW, Sugawara HM. Power analysis and determination of sample size for covariance structure modeling. Psychological Methods. 1996;1:130–149. [Google Scholar]
- Master A, Walton GM. Minimal groups increase young children's motivation and learning on group-relevant tasks. Child Development. 2013;84(2):737–751. doi: 10.1111/j.1467-8624.2012.01867.x. [DOI] [PubMed] [Google Scholar]
- Melnick G, De Leon G, Hawke J, Jainchill N, Kressel D. Motivation and readiness for therapeutic community treatment among adolescent and adult substance abusers. American Journal of Drug and Alcohol Abuse. 1997;23(4):485–506. doi: 10.3109/00952999709016891. [DOI] [PubMed] [Google Scholar]
- Myers MG, Brown SA. Coping and appraisal in potential relapse situations among adolescent substance abusers following treatment. Journal of Adolescent Chemical Dependency. 1990;1(2):95–115. [Google Scholar]
- Newbern D, Dansereau DF, Czuchry M, Simpson DD. Node-link mapping in individual counseling: Treatment impact on clients with ADHD-related behaviors. Journal of Psychoactive Drugs. 2005;37(1):93–103. doi: 10.1080/02791072.2005.10399752. [DOI] [PubMed] [Google Scholar]
- O'Donnell AM, Dansereau DF, Hall RH, Skaggs LP, Hythecker VI, Peel JL, Rewey KL. Learning concrete procedures: Effects of processing strategies and cooperative learning. Journal of Educational Psychology. 1990;82(1):171–177. [Google Scholar]
- Orlando M, Chan KS, Morral AR. Retention of court-referred youths in residential treatment programs: Client characteristics and treatment process effects. American Journal of Drug and Alcohol Abuse. 2003;29(2):337–357. doi: 10.1081/ada-120020518. [DOI] [PubMed] [Google Scholar]
- Perry JL, Joseph JE, Jiang Y, Zimmerman RS, Kelly TH, Darna M, et al. Bardo MT. Prefrontal cortex and drug abuse vulnerability: Translation to prevention and treatment interventions. Brain Research Reviews. 2011;65:124–149. doi: 10.1016/j.brainresrev.2010.09.001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Plass JL, O'Keefe PA, Homer BD, Case J, Hayward EO, Stein M, Perlin K. The impact of individual, competitive, and collaborative mathematics game play on learning, performance, and motivation. Journal of Educational Psychology. 2013;105(4):1050–1066. doi: 10.1037/a0032688. [DOI] [Google Scholar]
- Rivers SM, Greenbaum RL, Goldberg E. Hospital-based adolescent substance abuse treatment: Comorbidity, outcomes and gender. Journal of Nervous and Mental Disease. 2001;189(4):229–237. doi: 10.1097/00005053-200104000-00004. [DOI] [PubMed] [Google Scholar]
- SAS Institute Inc. SAS/STAT 9.2 user's guide. Cary, NC: Author; 2009. [Google Scholar]
- Schumacker RE, Lomax RG. A beginner's guide to structural equation modeling. 3rd. New York: Routledge; 2004. [Google Scholar]
- Sia TL, Dansereau DF, Czuchry ML. Treatment readiness training and probationers' evaluation of substance abuse treatment in a criminal justice setting. Journal of Substance Abuse Treatment. 2000;19:459–467. doi: 10.1016/s0740-5472(00)00139-2. [DOI] [PubMed] [Google Scholar]
- Simpson DD. A conceptual framework for drug treatment process and outcomes. Journal of Substance Abuse Treatment. 2004;27:99–121. doi: 10.1016/j.jsat.2004.06.001. [DOI] [PubMed] [Google Scholar]
- Simpson DD, Joe GW. A longitudinal evaluation of treatment engagement and recovery stages. Journal of Substance Abuse Treatment. 2004;27(2):89–97. doi: 10.1016/j.jsat.2004.03.001. [DOI] [PubMed] [Google Scholar]
- Simpson DD, Joe GW, Knight K, Rowan-Szal GA, Gray JS. Texas Christian University (TCU) short forms for assessing client needs and functioning in addiction treatment. Journal of Offender Rehabilitation. 2012;51(1-2):34–56. doi: 10.1080/10509674.2012.633024. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Simpson DD, Joe GW, Rowan-Szal GA, Greener JM. Client engagement and change during drug abuse treatment. Journal of Substance Abuse. 1995;7(1):117–134. doi: 10.1016/0899-3289(95)90309-7. [DOI] [PubMed] [Google Scholar]
- Simpson DD, Knight K. The TCU model of treatment process and outcomes in correctional settings. Offender Substance Abuse Report. 2001;1(4):51–58. [Google Scholar]
- Staton-Tindall M, Garner BR, Morey JT, Leukefeld C, Krietemeyer J, Saum CA, Oser CB. Gender differences in treatment engagement among a sample of incarcerated substance abusers. Criminal Justice and Behavior. 2007;34(9):1143–1156. [Google Scholar]
- Steinberg RJ. Wisdom, intelligence, and creativity synthesized. Cambridge, NY: Cambridge University Press; 2007. [Google Scholar]
- Titus JC, Dennis ML. Cannabis youth treatment intervention: Preliminary findings and implications. In: Liddle HA, Rowe CL, editors. Adolescent substance abuse: Research and clinical advances. Cambridge, NY: Cambridge University Press; 2006. pp. 104–126. [Google Scholar]
- Treatment Episode Data Set – Discharges (TEDS-D) Analysis ran on 2015-10-15 (02:28 PM EDT) using SDA 3.5: Tables 2010 [Google Scholar]
- Wise BK, Cuffe SP, Fischer T. Dual diagnosis and successful participation of adolescents in substance abuse treatment. Journal of Substance Abuse Treatment. 2001;21(3):161–165. doi: 10.1016/s0740-5472(01)00193-3. [DOI] [PubMed] [Google Scholar]
- Young MR. The motivational effects of the classroom environment in facilitating self-regulated learning. Journal of Marketing Education. 2005;27(1):25–40. doi: 10.1177/0273475304273346. [DOI] [Google Scholar]