

Abstract
In most cases of aspiration pneumonia in children, the disease is specific to this age group. Clinical and radiological correlation is essential for the diagnosis. The present pictorial essay is aimed at showing typical images of the most common etiologies.
Keywords: Pneumonia, Aspiration, Childhood
Abstract
A maioria das pneumonias por aspiração na infância é específica deste grupo etário. Para diagnosticá-las é essencial a correlação clinicorradiológica. O objetivo deste ensaio é mostrar imagens típicas das causas mais frequentes.
INTRODUCTION
Recently, the Brazilian radiological literature has been worried a lot about the relevance of imaging methods in the improvement of the diagnosis in pediatrics(1-11). Aspiration pneumonias result from passage of the oropharyngeal, esophageal or stomach contents into the lower respiratory tract(12). The resulting compromise of the lungs depends on the nature and amount of aspirated material(12). In the pediatric group, aspiration occurs most frequently because of deglutition abnormality, congenital malformations and gastroesophageal reflux. Lipoid pneumonia is more rarely observed and is always iatrogenic(13-17). Chest radiography, sometimes supplemented by computed tomography and esophagealgastroduodenal seriography (EGDS) are almost always enough to make the diagnosis(13,18).
DISCUSSION
The function of conducting food from the mouth to the stomach involves a joint action of the muscles innervated by the IX, X, XI and XII cranial pairs(12,19). Due to immaturity, central nerve system injuries or drugs effects, this mechanism may be disturbed, and part of the food is diverted into the airways (Figures 1, 2 and 3). In such situations, radiological findings are similar to those observed in adult individuals(13).
Figure 1.

A neonate with encephalopathy caused by perinatal anoxia, presenting with respiratory symptoms. A: Anteroposterior chest radiography showing opacity in the upper third of the right lung, limited by the horizontal scissure, characterizing involvement of the right upper lobe. B: Deglutition study demonstrating the contrast agent transit into the nasopharynx (arrows), characterizing lack of motor coordination.
Figure 2.

A three-month-old male child with neurological sequelae of congenital toxoplasmosis. Inadvertent contrast aspiration into the bronchial three during EGDS, resulting from non-coordinated deglutition. Chest radiography demonstrating paracardiac opacities corresponding to aspiration bronchopneumonia.
Figure 3.
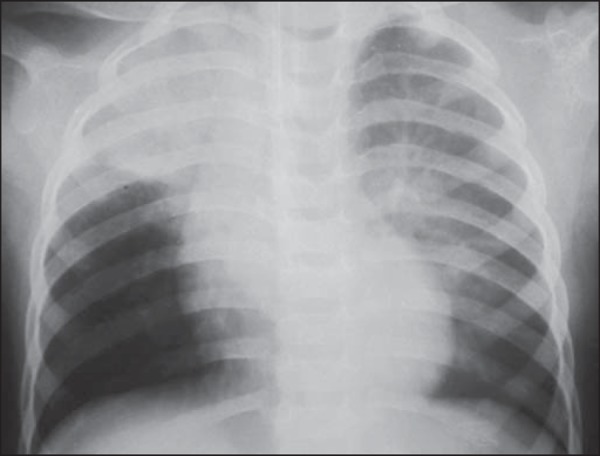
A previously healthy 18-month-old, afebrile male child, presented vomiting during recovering from anesthesia for palpebral injury suture, progressing to respiratory failure requiring ventilatory assistance. Anteroposterior view of the chest demonstrating opacities in the right upper lobe and in the upper segment of the left lower lobe, which represent usual sites in cases of aspiration occurring with the child in dorsal decubitus.
Any stasis resulting from narrowing of the esophageal lumen may lead to aspiration(18-20). Usually, this does not occur in cases of acquired achalasia and stenosis, because children frequently adapt themselves to such conditions. Esophageal atresia usually is detected and surgically corrected before causing significant aspiration(18,19). Amongst those cases of compression by anomalous vessels, compression by double aortic arch is the one that most frequently causes symptoms(13,21) (Figure 4). The diagnosis of H-type tracheoesophageal fistula may be late, as contrast-enhanced images not always can easily demonstrate it(13,18) (Figure 5).
Figure 4.

A seven-month-old male child with repetition pneumonia. Anteroposterior view of the chest with esophageal contrast-enhancement. Opacity is observed in the right upper lobe, compatible with pneumonia. Concentric narrowing of the lumen of the proximal esophageal third, with upstream dilatation. Such findings are strongly suggestive of extrinsic compression by double aortic arch. After surgical correction, the respiratory symptoms and the esophageal compression disappeared.
Figure 5.

A six-year-old boy with repetition pneumonia. A: Chest radiography, anteroposterior view showing subtle diffuse opacities in both lungs, confluent in the middle lobe. The caudal sift of the horizontal scissure (arrows) characterizes the presence of atelectatic component. B: Esophagography demonstrating H-type fistula to the trachea (arrow). C: High resolution computed tomography, axial section at the level of the fistula characterized by the dark dot (arrow) between the esophagus (with air) and the trachea. Centrilobular opacities, some of them branching, demonstrating involvement of small airways.
Respiratory manifestations stand out in the wide spectrum of gastroesophageal reflux disease(18-21). More than highlighting the presence of reflux - whose diagnosis is essentially clinical -, EGDS plays a relevant role in the demonstration of either normal or pathological anatomy(19-21). In the absence of anatomical alterations, reflux is considered to be primary, resulting from generally transient immaturity of the distal esophageal high pressure zone(19,20) (Figure 6). Surgical intervention is indicated in cases of reflux secondary to partial or total obstruction - usually hypertrophic pyloric stenosis or malformations of the second portion of the duodenal arch (Figure 7)(13,19,20).
Figure 6.

A twenty-month-old female child presenting with fever and cough. A: Anteroposterior chest radiography revealing the presence of bilateral, diffuse, ill defined, coalescent opacities in the middle lobe, conditioning the partial fading of the cardiac silhouette. B: Computed tomography, axial section identifying bilateral, predominantly central consolidations with air bronchograms. C: EGDS demonstrating reflux. As no clinical and radiological improvement was observed after antibiotic therapy, lung biopsy was indicated and showed foreign body granulomas and vegetal fibers presumably coming from gastroesophageal reflux. After appropriate treatment, clinical and radiological healing was observed.
Figure 7.

A neonate with Down syndrome and respiratory symptoms. A: Anteroposterior chest radiography showing left lung with decreased volume and transparency. Fading of the left cardiac silhouette indicates upper lobe atelectasis. B: EGDS. Small bowel transit shows partial obstruction at the level of the second duodenal portion, with appearance suggestive of duodenal diaphragm (windsock sign). C: Secondary gastroesophageal reflux.
Lipoid pneumonia is not related to anatomical or functional anomalies(13,15). Aspiration occurs because of the use of mineral oil in the treatment of intestinal constipation (Figure 8) or as an adjuvant in cases of intestinal subocclusion caused by Ascaris lumbricoides(4). The oil inhibits the cough reflex and ciliary motion, and silently reaches the alveoli. Because of the difficulty in removing the oil from the lungs, such pneumonias present a slow evolution pattern(14,15).
Figure 8.
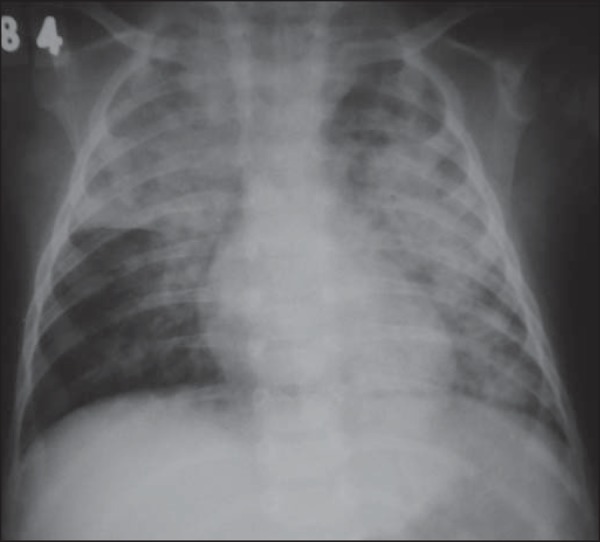
Anteroposterior view of chest in a three-year-old boy undergoing treatment for constipation with mineral oil e diagnosis of bronchopneumonia refractory to antibiotics. Coalescent opacities in both lungs, with "butterfly wing" distribution. In the clinical context, such a finding allows for the diagnosis of lipoid pneumonia, with no need for biopsy.
IMAGING FINDINGS
Aspiration pneumonias involve the alveoli(12,20,21). The literature reports a most frequent involvement of the posterior segments of the upper lobes and the upper segments of the lower lobes(12,13,18). This happens as aspiration occurs with the child in dorsal decubitus, like in most gastroesophageal reflux and vomiting episodes(12,13). In other situations, such as tracheoesophageal fistula and lack of motor coordination, other pulmonary segments may be affected(19-21) (Figures 2 and 5). In most of cases, chest radiography and EGDS are sufficient to confirm the clinical suspicion; eventually, high resolution computed tomography is useful(13). Aspiration may result in atelectasis or pneumonia, the latter with or without atelectatic component(13). The absence of fever suggests pure atelectasis(22) (Figures 3 and 9).
Figure 9.

A six-year-old male child said to be asthmatic, presented with dyspnea and sudden chest pain. A: Anteroposterior view showing left hemithorax with decreased volume and transparency, right lung herniation and mediastinal displacement to the left, characterizing left lung atelectasis. B: EGDS demonstrating reflux. After four-day anti-reflux treatment, the symptoms disappeared and chest radiography was normal. C: Normal anteroposterior chest radiography after treatment for gastroesophageal reflux disease.
Footnotes
Study developed in the Unit of Radiology and Imaging Diagnosis at Universidade Federal do Espírito Santo (UFES), Vitória, ES, Brazil.
Oliveira GA, Pessanha LB, Guerra LFA, Martins DLN, Rondina RG, Silva JRP. Aspiration pneumonia in children: an iconographic essay. Radiol Bras. 2015 Nov/Dez;48(6):391–395.
REFERENCES
- 1.Araújo BCL, Motta MEA, Castro AG, et al. Clinical and video-fluoroscopic diagnosis of dysphagia in chronic encephalopathy of childhood. Radiol Bras. 2014;47:84–88. doi: 10.1590/S0100-39842014000200009. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Sakuno T, Tomita LM, Tomita CM, et al. Sonographic evaluation of visceral and subcutaneous fat in obese children. Radiol Bras. 2014;47:149–153. doi: 10.1590/0100-3984.2013.1828. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Lederman HM. Visceral and subcutaneous fat. Radiol Bras. 2014;47(3):ix. doi: 10.1590/0100-3984.2014.47.3e3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Fonseca JM, Borém LMA. Cloverleaf skull syndrome: case report. Radiol Bras. 2014;47:189–190. doi: 10.1590/0100-3984.2013.1681. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Berdichevski EH, Mattos SG, Bezerra S, et al. Prevalence of acute pyelonephritis and incidence of renal scarring in children under the age of two with urinary tract infection evaluated by 99mTc-DMSA renal scintigraphythe experience of a university scintigraphy: the experience of a university hospital. Radiol Bras. 2013;46:30–34. [Google Scholar]
- 6.Daud DF, Campos MMF, Fleury LAP., Neto Cardiac tamponade in an infant during contrast infusion through central venous catheter for chest computed tomography. Radiol Bras. 2013;46:385–386. [Google Scholar]
- 7.Gun S, Ciantelli GL, Takahashi MAU, et al. Complete renal fusion in a child with recurrent urinary tract infection. Radiol Bras. 2012;45:233–234. [Google Scholar]
- 8.Monteiro AMV, Lima CMAO, Medina P. Is there any influence of breastfeeding on the cerebral blood flow? A review of 256 healthy newborns. Radiol Bras. 2012;45:263–266. [Google Scholar]
- 9.Bitencourt AGV, Pinto PNV, Almeida MFA, et al. Incidence and imaging findings of lymphoma after liver transplantation in children. Radiol Bras. 2012;45:7–11. [Google Scholar]
- 10.Valente M, Oliveira LAN, Carneiro-Sampaio M. Pediatric radiology: the necessity of a child-friendly diagnosis. Radiol Bras. 2012;45(5):v. [Google Scholar]
- 11.Araújo JAB, Filho, Martines JAS, Martines BMR, et al. Inflammatory myofibroblastic tumor of the bladder in a child: a case report. Radiol Bras. 2012;45:230–232. [Google Scholar]
- 12.Marik PE. Aspiration pneumonitis and aspiration pneumonia. N Engl J Med. 2001;344:665–671. doi: 10.1056/NEJM200103013440908. [DOI] [PubMed] [Google Scholar]
- 13.Franquet T, Giménez A, Rosón N, et al. Aspiration diseases: findings, pitfalls, and differential diagnosis. Radiographics. 2000;20:673–685. doi: 10.1148/radiographics.20.3.g00ma01673. [DOI] [PubMed] [Google Scholar]
- 14.Oliveira GA, Lamego CM, Vargas PR. Pneumonias lipóides exógenas na infância. Rev Assoc Med Bras. 1984;30:34–36. [PubMed] [Google Scholar]
- 15.Oliveira GA, Del Caro SR, Bender Lamego CM, et al. Radiographic plain film and CT findings in lipoid pneumonia in infants following aspiration of mineral oil used in treatment of bowel obstruction by Ascaris lumbricoides. Pediatr Radiol. 1985;15:157–160. doi: 10.1007/BF02388601. [DOI] [PubMed] [Google Scholar]
- 16.Sias SMA, Quirico-Santos TQ. Pneumonia lipóide na infância - revisão de literatura. Pulmão RJ. 2009;(Supl 1):S9–S16. [Google Scholar]
- 17.Wolfson BJ, Allen JL, Panitch HB, et al. Lipid aspiration pneumonia due to gastroesophageal reflux. A complication of nasogastric lipid feedings. Pediatr Radiol. 1989;19:545–547. doi: 10.1007/BF02389570. [DOI] [PubMed] [Google Scholar]
- 18.Vaughan D, Katkin JP, et al. Chronic and recurrent pneumonias in children. Semin Respir Infect. 2002;17:72–84. doi: 10.1053/srin.2002.31693. [DOI] [PubMed] [Google Scholar]
- 19.Weir K, McMahon S, Barry L, et al. Oropharyngeal aspiration and pneumonia in children. Pediatr Pulmonol. 2007;42:1024–1031. doi: 10.1002/ppul.20687. [DOI] [PubMed] [Google Scholar]
- 20.Loughlin GM. Respiratory consequences of dysfunctional swallowing and aspiration. Dysphagia. 1989;3:126–130. doi: 10.1007/BF02407130. [DOI] [PubMed] [Google Scholar]
- 21.Toufen C, Junior, Camargo FP, Carvalho CRR. Pneumonia aspirativa associada a alterações da deglutição: Relato de caso. Rev Bras Ter Intensiva. 2007;19:118–122. [PubMed] [Google Scholar]
- 22.Tutor JD, Schoumacher RA. Is aspiration causing your pediatric patient's symptoms? J Respir Dis. 2003;24:30–40. [Google Scholar]