

Abstract
Background:
High-dose chemotherapy followed by autologous stem cell transplantation (ASCT) is a promising approach for lymphomas. This study aimed to evaluate the effect of ifosfamide, cisplatin or carboplatin, and etoposide (ICE)-based regimen as a mobilization regimen on relapsed, refractory, or high-risk aggressive lymphoma.
Methods:
From June 2001 to May 2013, patients with lymphomas who mobilized by ICE-based regimen for ASCT were analyzed in this retrospective study. The results of the autologous peripheral blood stem cells collection, toxicity, engraftment after ICE-based mobilization regimen were analyzed in this study. Furthermore, risk factors for overall survival (OS) and progression free survival (PFS) were evaluated by univariate analysis.
Results:
The stem cells were mobilized using ICE-based regimen plus rituximab or ICE-based regimen alone in 12 patients and 54 patients, respectively. The results of stem cell mobilization were excellent. Ninety-seven percentages of the patients had the stem cell collection of at least 2.0 × 106 CD34+ cells/kg and 68% had at least 5 × 106 CD34+ cells/kg. Fifty-eight percentage of the patients experienced Grade 4 neutropenia, 20% developed febrile neutropenia, and only 12% had Grade 4 thrombocytopenia. At a median follow-up of 63.8 months, the 5-year PFS and OS were 64.4% and 75.3%, respectively.
Conclusion:
ICE is a powerful regimen for stem cell mobilization in patients with lymphomas.
Keywords: ICE, Mobilization, Rituximab, Stem Cell Transplantation
INTRODUCTION
High-dose chemotherapy (HDC) followed by autologous stem cell transplantation (ASCT) is considered standard treatment for chemosensitive patients with relapsed or refractory aggressive lymphoma, particularly the disease responding to the salvage second-line chemotherapy.[1] Stem cells for ASCT are almost invariably collected from peripheral blood after mobilization therapy.[2] A variety of salvage regimens have been investigated, which have a miscellaneous efficacy, toxicity, and mobilization potential for the collection of autologous peripheral blood stem cells (APBSCs),[3,4,5] but there is no consensus as to the optimal regimen for the relapsed lymphoma. As reported, combination chemotherapy with ifosfamide, cisplatin or carboplatin, and etoposide (ICE) has the capacity to mobilize and collect a sufficient number of APBSC with limited nonhematological toxicity, which may complicate consolidative HDCT.[4,6] However, there are rare data about ICE chemotherapy in the mobilization of APBSC in a Chinese population. Therefore, efforts to identify the optimal mobilization regimen represent are challenging and urgent issues for Chinese patients.
Herein, we have retrospectively analyzed the ICE-based chemotherapy in 66 Chinese patients with relapsed, refractory or high-risk lymphomas with regard to the ability to mobilize and collect APBSC, toxicity, response, and long-term progression free survival (PFS) and overall survival (OS).
METHODS
Patient selection
Between June 2001 and May 2013, a total of 66 patients with relapsed, refractory or high-risk non-Hodgkin's lymphoma (NHL) or Hodgkin's lymphoma (HL) were included in this study. Patients were identified from a database of prospective observational research on HDC/ASCT in malignant lymphoma. The analysis was approved by the Institutional Review Board of the Cancer Hospital, Chinese Academy of Medical Science & Peking Union Medical College (CAMS & PUMC). All of the patients were histologically confirmed at the Department of Pathology, Cancer Hospital, CAMS & PUMC using the 2008 World Health Organization (WHO) classification of lymphoma.[7] According to the requirements, all patients were younger than 65 years old and had adequate organ function including a bone marrow reserve. Patients were excluded if they had a human immunodeficiency virus or central nervous system disease, active hepatitis B or C, or Grade ≥2 peripheral neuropathy. Patients were staged according to Ann Arbor System before mobilization. Staging procedures included physical examination, reporting of B-symptoms, computed tomography (CT) scans, or positron emission tomography (PET)-CT and bone marrow biopsy. Because this was a retrospective review of patients treated in clinical practice, over time there was variability in the use of PET-CT to aid in the assessment of response. The median age of patients was 28.5 years (range, 11–47 years). Summary of patient characteristics is provided in Table 1.
Table 1.
Patient characteristics (n = 66)
| Characteristics | Number | Percentage (%) |
|---|---|---|
| Sex | ||
| Male | 35 | 53.0 |
| Female | 31 | 47.0 |
| Histology* | ||
| HL | 10 | 15.2 |
| B cell origin | ||
| DLBCL | 20 | 30.3 |
| Non-DLBCL | 7 | 10.6 |
| T cell origin | ||
| PTCL-NOS | 7 | 10.6 |
| ALCL | 9 | 13.6 |
| Others | 8 | 12.1 |
| Ann Arbor Stage | ||
| I/II | 17 | 25.8 |
| III/IV | 49 | 74.2 |
| ECOG | ||
| <2 | 62 | 93.9 |
| ≥2 | 4 | 6.1 |
| Elevated LDH | 28 | 42.4 |
| B-symptom | 26 | 39.4 |
| Bulky disease(≥10 cm) | 25 | 37.9 |
| Extranodal site >1 | 35 | 53.0 |
| aaIPI (NHL) | ||
| 0–1 | 33 | 58.9 |
| 2–3 | 23 | 41.1 |
| Disease status | ||
| CR or PR to first-line therapy | 28 | 42.4 |
| CR or PR to second-line therapy | 27 | 40.9 |
| Primary refractory | 11 | 16.7 |
| Prior radiation therapy | 18 | 27.3 |
*The cell origin of five NHL patients was unknown. HL: Hodgkin’s lymphoma; NHL: Non-Hodgkin’s lymphoma; aaIPI: Age-adjusted international prognostic index; ECOG: Eastern cooperative oncology group; LDH: Lactate dehydrogenase; CR: Complete response; PR: Partial response.
Treatment before autologous peripheral blood stem cell mobilization
For patients with NHL, induction chemotherapy included cyclophosphamide, doxorubicin, vincristine and prednisone (CHOP); cyclophosphamide, doxorubicin, vincristine, prednisone, and etoposide (CHOEP); bleomycin, epirubicin, cyclophosphamide, vincristine, and prednisone (BACOP); and prednisone, doxorubicin, cyclophosphamide, and etoposide, followed by cytarabine, bleomycin, vincristine, and methotrexate with leucovorin, rescue (proMACE-CytaBOM). For patients with HL, epirubicin, bleomycin, vinblastine, and dacarbazine (ABVD) was the induction regimen. Patients with relapsed or refractory disease were rescued with the ICE-based regimen as the second-line chemotherapy, and 2–4 cycles of ICE-based regimens were conducted for the salvage therapy and APBSC mobilization.
Mobilization and collection of autologous peripheral blood stem cell
Of all patients in our study, APBSC were mobilized with the chemotherapy of ICE-based regimen, combined with recombinant human granulocyte colony-stimulating factor (rhG-CSF). Fifty-three patients were mobilized with DICE ± rituximab and the others were mobilized with ICE ± rituximab. DICE was administrated as follows: Oral dexamethasone, 10 mg/m2, from day 1 to day 4; ifosfamide, 1000 mg/m2, from day 1 to day 4; cisplatin, 25 mg/m2, from day 1 to day 4; etoposide, 60 mg/m2, from day 1 to day 4. ICE consisted of etoposide 100 mg/m2, from days 1 to 3, ifosfamide 5000 mg/m2, day 2 and carboplatin at an area under the curve (AUC) of 5 (maximum dose, 800 mg) based on 12-hour measured creatinine clearance on day 2. Twelve patients received rituximab, 375 mg·m−2·d−1, for 4 days, in details, the day before mobilization, day 7 after mobilization, the day before APBSC reinfusion and day 8 after reinfusion.
A daily blood routine test was conducted during the mobilization period. rhG-CSF was subcutaneously administrated from the day when the white blood cell (WBC) counts first rose from the nadir after chemotherapy to the day prior to the last apheresis, which was firstly administrated at a fixed dose of 300 μg/d (150 μg/d for patients whose weight was <45 kg). APBSC were collected as previously described when WBC counts, mononuclear cells (MNCs) counts, and the percentage of CD34+ cells in peripheral blood exceeded 10 × 109/L, 2 × 109/L, and 1%, respectively. Continuous APBSC collection was conducted daily (with a CS-3000 Plus Blood Cell Separator, Baxter Healthcare Corp., Deerfield, IL, USA) until a target collection of at least 2 × 106 CD34+ cells/kg or 4 × 108 MNCs/kg was achieved. The blood volume processed by each single apheresis was 110–150 ml/kg at a speed of 40–70 ml/min. Venous access was obtained by a double lumen catheter (Arrow International Inc., PA, USA) placed in a femoral vein.[8,9,10] Successful mobilization was defined as a collection of at least of 2 × 106 CD34+ cells/kg body weight in a single mobilization. Optimal mobilization was defined as a collection of 5 × 106 CD34+ cells/kg body weight collection in a single mobilization.[11] Failed mobilization was defined as failure to collect a minimum of 2 × 106 CD34+ cells/kg body weight in the initial aphaeresis. Conditioning regimens of transplantation ASCT was not proceeded in 6 (9%) patients, since APBSC mobilization (CD34+ cell count: 0.3 × 106/kg) failed in one patient, relapse affected two soon after mobilization but before ASCT, and three refused transplantation due to personal reasons. Conditioning regimens for the remaining 60 patients included carmustine, etoposide, cytarabine, and melphalan (BEAM); carmustine, etoposide, cytarabine, and cyclophosphamide (BEAC); and cyclophosphamide, carmustine and etoposide (CBV).
Evaluation of toxicity and engraftment
Toxicity was evaluated according to the National Cancer Institute Common Terminology Criteria for Adverse Events. Engraftment after transplantation was defined, if absolute neutrophil counts (ANC) and platelets (PLT) counts recovered to more than 0.5 × 109/L and more than 50 × 109/L for 2 consecutive days without transfusion support, respectively.[9,10] rhG-CSF (300 μg/d) was administrated on day 6 after APBSC infusion, and the administration continued until the neutrophil counts recovered.
Response and survival
Response to mobilization regimen was evaluated according to WHO criteria.[12] Response to therapy was initially assessed at month 3 after transplantation. Thereafter, routine follow-up by imaging analysis was performed every 3 months for the first 2 years, every 6 months for the next 3 years, and then annually or whenever clinically indicated.[13] OS was measured from the first date of mobilization to the date of a patient's death for any reasons or the last follow-up. PFS was measured from the first date of mobilization to progress or death, whereas patients with stable disease or remission were censored.
Statistical methods
All calculations and statistical analyses were conducted using SPSS software (version 19.0, SPSS Inc., Chicago, IL, USA). Quantitative variables were described in medians, ranges, and proportions by descriptive statistics and frequency analysis. Categorical variables between groups were compared by the Chi-square test or Fisher's exact tests and continuous variables between two groups were compared by Mann–Whitney U-test. Survival data were analyzed using the Kaplan-Meier method, and survival curves were compared using the log-rank test. Two-sided values of P < 0.05 were considered statistically significant.
RESULTS
Patients
A total of 66 consecutive transplant-eligible patients with relapsed, refractory, or high-risk lymphoma who received ICE-based mobilization regimen were analyzed. The median age of the patients was 28.5 years, ranging from 11 to 47 years. Among them, 36.3% were histologically confirmed as T cell lymphoma, 40.9% were B cell lymphoma, and 15.2% were HL, with cell origin of the others unclear. A median number of prior chemotherapy cycles was 6 ranging from 2 to 22. The baseline characteristics of the patients are listed in Table 1.
Mobilization efficacies
Sixty-four patients (97%) received a successful mobilization defined as total CD34+ cells > 2 × 106/kg and 45 patients (68%) achieved an optimal mobilization defined as a total CD34+ cells >5 × 106/kg. The median collection for the first apheresis was 4.99 × 106/kg (range, 0.30–21.35). The median total CD34+ yield was 6.31 × 106/kg (range, 0.30–32.7). The median days from the initial mobilization to first apheresis were 17 days (range, 13–23 days). There was no significant difference observed in patients mobilized with rituximab or not. Among the 54 patients mobilized without rituximab which had a median CD34+ cells count of 6.30 × 106/kg (range, 0.30–27.94), 52 patients of them received a successful mobilization and 37 patients received an optimal mobilization. For all the patients, 35 patients reached a complete response (CR) after mobilized by ICE-based regimen and overall response rate was 86.3%. Among the 11 primary refractory patients, 6 patients reached a CR, 2 patients reached a partial response (PR) after mobilized by ICE-based mobilization regimen. The detailed data are shown in Table 2.
Table 2.
Results of APBSC collection
| Parameters | All | R+(D)ICE (n = 12) | (D)ICE (n = 54) | P |
|---|---|---|---|---|
| Days of rhG-CSF treatment (range) | 6 (3–12) | 6 (3–8) | 6 (4–12) | 0.765 |
| Days to first apheresis (range) | 17 (13–23) | 17.5 (14–23) | 16 (13–21) | 0.091 |
| Number of apheresis procedures (range) | 1 (1–3) | 2 (1–3) | 1 (1–3) | 0.129 |
| CD34+ cell percentage in PB for the first apheresis (%) (range) | 2.87 (0.17–17.27) | 3.67 (0.66–17.27) | 2.3 (0.17–12.2) | 0.306 |
| CD34+ CD38− cell percentage in PB for the first apheresis (%) (range) | 0.30 (0–4.43) | 0.25 (0.07–4.43) | 0.32 (0–2.64) | 0.721 |
| CD34+ cells collected for the first apheresis, ×106/kg (range) | 4.99 (0.30–21.35) | 4.88 (0.91–15.19) | 4.99 (0.3–21.35) | 0.803 |
| CD34+ cells collected in total, ×106/kg (range) | 6.31 (0.3–32.70) | 6.45 (2.36–32.7) | 6.30 (0.3–27.94) | 0.678 |
| Optimal mobilization rate of CD34+ cells collection in total (%) | 45 (68.2) | 8 (66.7) | 37 (68.5) | 0.901 |
| Successful mobilization rate of CD34+ cells collection in total (%) | 64 (97.0) | 12 (100) | 52 (96.3) | 0.498 |
| CR rate after ICE-based regimen (%)* | 35 (53.0) | 10 (83.3) | 25 (46.3) | 0.026 |
*The status after ICE-based regimen was evaluated in 62 patients (93.9%). PB: Peripheral blood; rhG-CSF: Recombinant human granulocyte colony-stimulating factor; CR: Complete response; APBSC: Autologous peripheral blood stem cells.
Toxicity
Mobilization-induced neutrophil nadir developed on a median of 10 days after ICE-based chemotherapy was provided, which was significantly delayed in the R-(D) ICE group (12.5 days, P = 0.021), the same as the day of WBC and PLT nadir (P = 0.008, P = 0.001, respectively). However, the counts of WBC, neutrophil and PLT at nadir were similar. During the collection phase, there was a relatively low incidence of treatment-related adverse events [Table 3]. The most common toxicity was hematologic toxicity. Fifty-eight percentage of the patients experienced Grade 4 neutropenia, 20% developed febrile neutropenia, and only 12% had Grade 4 thrombocytopenia. There were no significant differences between two groups about the adverse events [Table 3]. One patient in the (D)ICE group died of multiorgan failure during the transplant and was not considered to be related to mobilization chemotherapy.
Table 3.
Toxicities of two groups
| Parameters | All | R+(D)ICE (n = 12) | (D)ICE (n = 54) | P |
|---|---|---|---|---|
| Days of WBC nadir (range) | 11 (8–17) | 12.5 (9–16) | 11 (8–17) | 0.008 |
| WBC count at nadir (range) | 1 (0.27–3.63) | 0.95 (0.50–3.63) | 1 (0.27–2.30) | 0.511 |
| Days of neutrophil nadir (range) | 11 (8–24) | 12.5 (9–17) | 11 (8–24) | 0.021 |
| ANC at nadir (range) | 0.22 (0–1.79) | 0 (0–1.79) | 0.28 (0–1.60) | 0.720 |
| Days of PLT nadir (range) | 15 (9–22) | 16.5 (13–22) | 14 (9–20) | 0.001 |
| PLT count at nadir (range) | 55.5 (12–173) | 58.5 (32–160) | 54.5 (12–173) | 0.690 |
| Number of patients with PLT transfusions (%) | 30 (45.5) | 6 (50) | 24 (44.4) | 0.758 |
| Number of patients with RBC transfusions (%) | 4 (6.1) | 1 (8.3) | 3 (5.6) | 0.561 |
| Neutropenic fever (%) | 13 (19.7) | 4 (33.3) | 9 (16.7) | 0.194 |
WBC: White blood cell; ANC: Absolute neutrophil count; PLT: Platelet; RBC: Red blood cell.
Conditioning regimens and engraftment
In terms of conditioning regimens for the 60 patients proceeding to ASCT, 22 (37%) patients received BEAM, 30 (50%) patients received BEAC, and 8 (13%) patients received CBV. The median number of CD34+ cells and MNCs reinfused was 4.76 × 106/kg (1.24–16.87) and 3.04 × 106/kg (1.03–6.90), respectively. Furthermore, the recovery of WBC, PLT, neutrophil was not affected by rituximab addition [Table 4].
Table 4.
Engraftment of two groups
| Parameters | ALL | R+(D)ICE (n = 12) | (D) ICE(n = 54) | P |
|---|---|---|---|---|
| Number of patients without ASCT (%) | 6 (9.1) | 0 | 6 | 0.582 |
| Median number of CD34+ cells infused, ×106/kg* (range) | 4.76 (1.24–16.87) | 4.18 (1.73–12.27) | 4.83 (1.24–16.87) | 0.966 |
| Median number of MNC cells infused, ×109/kg* (range) | 3.04 (1.03–6.90) | 2.49 (1.70–5.05) | 3.3 (1.03–6.90) | 0.492 |
| Median days to WBC recovery (range) | 11 (8–17) | 11 (1–14) | 11 (8–17) | 0.754 |
| Median days to PLT recovery (range) | 12 (7–26) | 11 (9–26) | 12 (7–20) | 0.844 |
| Median days to neutrophil recovery (range) | 10 (8–17) | 10.5 (10–13) | 10 (8–17) | 0.902 |
*The data of CD34+ and MNC cells infused was missed in 24 patients (36.4%). ASCT: Autologous stem cell transplantation; MNC: Mononuclear cells; WBC: White blood cell; PLT: Platelet; CR: Complete response; PFS: Progression free survival; OS: Overall survival.
Survival data
At a median follow-up of 63.8 months, the 5-year PFS rate and OS rate among the patients, after mobilized by ICE-based regimen in our study, were 64.4% and 75.3%, respectively [Figure 1]. Of the 35 patients who achieved a CR to the ICE-based regimen, 12 (34.3%) experienced a relapse during the follow-up time, and median survival duration was 25.6 months.
Figure 1.

Overall survival (OS) and progression-free survival (PFS) of all the patients (n = 66).
Univariate analysis was employed to evaluate the possible factors related to successful outcomes following ASCT. There was no significant difference in PFS rate or OS rate depending upon patient age, tumor origin, stage, disease status or a number of prior chemotherapy regimens. Of the 54 patients without rituximab, 5-year OS rate and 5-year PFS rate were 72.7% and 64.2%, respectively. Of the 12 patients received rituximab 5-year OS rate and 5-year PFS rate were 75.4% and 64.0%, respectively. However, the differences were not statistically significant [Table 5]. In the analysis of survival, the few patients who progressed after mobilization had a significantly poor prognosis (P < 0.001, Figure 2), with a median survival of 5.1 months. There were 28 patients who did not have chemotherapy failure before mobilization, and the 5-year OS rate was 83.9%, without significant difference compared with other patients (P = 0.362, Figure 3). When time to first relapse was compared, 5-year OS rate and 5-year PFS rate for patients who relapsed <12 months before mobilization were 62.7% and 56.7% respectively, while 5-year survival for patients who relapsed ≥12 months before mobilization was not reached. As shown in Figure 4, there was a slight trend toward improved 5-year OS rate and 5-year PFS rate in patients who relapsed >12 months, but it was not statistically significant possibly due to the smaller number (P = 0.098, P = 0.184).
Table 5.
Univariate analysis for PFS and OS for all 66 patients
| Characteristics | n | 5-year PFS (%) | P | 5-year OS (%) | P |
|---|---|---|---|---|---|
| Disease status at transplantation* | |||||
| CR | 35 | 64.1 | 0.002 | 73.8 | <0.001 |
| PR | 22 | 70.2 | 83.3 | ||
| PD/SD | 5 | 20.0 | 20.0 | ||
| Number of prior regimens | |||||
| 1 or 2 | 49 | 66.4 | 0.284 | 74.7 | 0.853 |
| 3 or more | 17 | 58.8 | 76.0 | ||
| Receipt of rituximab | |||||
| Yes | 54 | 64.0 | 0.628 | 75.4 | 0.662 |
| No | 12 | 64.2 | 72.7 | ||
| Chemotherapy failure before mobilization | |||||
| Yes | 38 | 61.7 | 0.379 | 68.8 | 0.362 |
| No | 28 | 67.9 | 83.9 | ||
| Time to relapse | |||||
| <12 months | 31 | 56.7 | 0.184 | 62.7 | 0.098 |
| ≥12 months | 7 | 85.7 | – |
*The data of disease status at transplantation was missed in 4 patients (6.1%). CR: Complete response; PR: Partial response; SD: Stable disease; PD: Progressive disease; PFS: Progression free survival; OS: Overall survival.
Figure 2.

Overall survival (OS) according to disease status at ICE-based regimen for assessable patients (n = 62).
Figure 3.
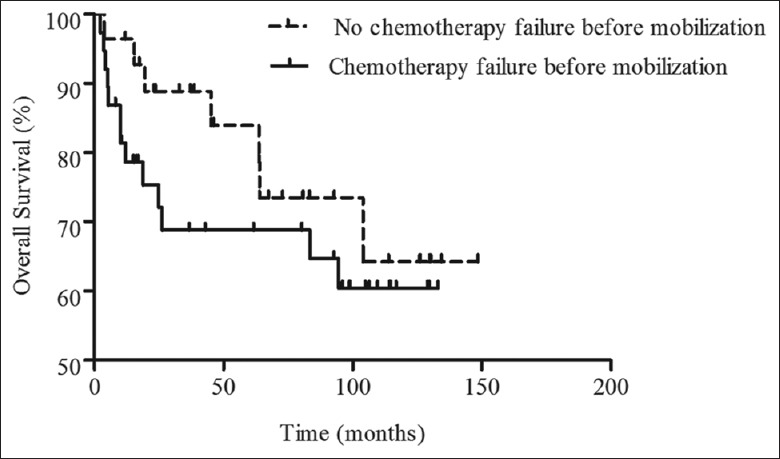
Overall survival (OS) according to chemotherapy failure before mobilization (n = 66).
Figure 4.

(a) Overall survival according to the time to first relapse before mobilization (n = 38); (b) Progression-free survival according to the time to first relapse before mobilization (n = 38).
DISCUSSION
The ideal mobilization regimen for patients who are eligible for ASCT is respected to have a high APBSC mobilization capacity, high response rate, and limited toxicity.[14] The benefit of ASCT in relapsed or refractory aggressive lymphoma is largely restricted to patients with chemosensitive disease, and patients who undergo transplantation in CR have better outcomes than those patients who undergo transplantation in PR as previously reported.[15,16] Therefore, the way of improving outcome is to potentiate the effects of chemotherapy regimen and increase the CR rate.
This study analyzed the efficacy of ICE-based salvage regimen in mobilizing patients with high-risk or relapsed/refractory NHL or HL, who were treated within a single center. The ICE-based regimen was proved to be highly effective on mobilizing a sufficient number of CD34+ cells. The median number of CD34+ cells collected after mobilization was 6.31 × 106/kg, and 45 patients (68.2%) achieved an optimal mobilization. The mobilization yield seemed similar to the yield from etoposide in the WA Wood study (6.23 × 106/kg)[17] but better than that from the rhG-CSF alone (1.98 × 106/kg).[18] Likewise, it was superior to that associated with the ICE regimens, in which CD34+ cell yield was 3.6–6.3 × 106/kg.[4,6,19] Possibly because of the excellent mobilization, 90.9% of the patients mobilized by ICE-based regimen in our series proceeded to transplantation, as was favorable when compared to the other regimens reported previously.[20,21] However, the cross-trial comparison is of limited value.
Though direct comparison are unwarranted, as ours was not a randomized study and baseline characteristics among the patient populations may have varied, Table 6 suggests that our results are at least comparable, from an efficacy standpoint to other mobilization strategies. The CD34+ stem cell yield with ICE-based chemomobilization (6.31 × 106/kg) appears similar to the yield from the plerixafor arm in the Dipersio study (5.69 × 106/kg) and better than the rhG-CSF alone arm (1.98 × 106/kg).[18]
Table 6.
Comparison of efficacy of mobilization with published data
| Parameters | (D)ICE±R (current sample) (n = 66) | G-CSF alone (published) (n = 148) | G-CSF+P (published) (n = 150) |
|---|---|---|---|
| CD34+ cells collected in total, ×106/kg (range) | 6.31 (0.30–32.70) | 1.98 (0.06–15.00) | 5.69 (0.03–29.22) |
| Number of patients proceeding to ASCT (%) | 60 (90.9) | 66 (45.0) | 135 (90.0) |
| Median number of days to PLT recovery (range) | 12 (7–26) | 20 | 20 |
| Median number of days to neutrophil recovery (range) | 10 (8–17) | 10 | 10 |
ASCT: Autologous stem cell transplantation; G-CSF: Granulocyte colony-stimulating factor; P: Plerixafor; PLT: Platelet.
The secondary age-adjusted International Prognostic Index score (saaIPI), early relapse <12 months after diagnosis, and prior rituximab treatment were reported to be independent factors affecting response rate after salvage therapy.[20] A nonrandomized study[19] demonstrated that adding rituximab to ICE in patients with relapsed or primary refractory diffuse large B-cell lymphoma (DLBCL) appeared to achieve double CR rates, from 27% to 53%. When added to CHOP, rituximab significantly increased the CR rate among patients with DLBCL.[22] In our study, CR rate was somewhat higher than that reported in previous studies investigating mobilization by ICE-based regimens.[4,6,19] However, this conclusion should be interpreted in cautiously given the limitation in our study. First, the younger age may contribute to the higher CR rate. Second, a potential concern as to the limitation of the current study was that the response assessment of mobilization was not universally performed by integrated PET-CT. Third, patients with the refractory disease were in a minority, who appeared to have a poorer prognosis.[15,20]
A critical question is whether the improved CR rate will be translated into improved outcomes after ASCT. The 5-year OS rate of patients who were mobilized without rituximab was similar to that with rituximab (72.7% vs. 75.4%), and 5-year PFS rate of the two groups were almost the same (64.2% vs. 64.0%). Therefore, new therapies for relapsed or refractory patients which could improve outcomes in a large proportion of patients are needed. A recent study, using ofatumumab instead of rituximab as the immunotherapy component of the second-line therapy, reported a higher CR rate compared to that in CORAL study, in which the median PFS and OS were 9.5 months and 16.7 months, respectively. However, rituximab plus with chemotherapy appeared to improve outcomes for patients with transformed indolent NHL, compared with those mobilized without rituximab.[23]
The CORAL study[20] found that the response to the first-line treatment, saaIPI, and early relapse were the powerful predictors of outcomes following the salvage therapy, consistent with the results of the earlier international prospective randomized phase III PARMA trial.[24] Similarity, in a recent study which employed ofatumumab combined with ICE or DHAP for relapsed or refractory lymphoma, the independent prognostic factors in CORAL retained their prognostic relevance.[25] Furthermore, it was reported that elevated lactate dehydrogenase, lymphopenia, bulk >10 cm and response to induction regimen were prognostic factors.[14,15] However, based on this retrospective and small sample study, the number of prior regimens, chemotherapy failure before mobilization and the time to relapse were not prognostic factors.
This study has several limitations. It was uncontrolled, retrospective, single center study, which included the patients treated over many years. However, it was believed that our results to be reliable for selecting an effective chemomobilization regimen because the clinical characteristics that might affect the APBSC mobilization yield were comparable and all apheresis procedures were usually performed according to similar guidelines.
In conclusion, taking the limitations of the retrospective nature of analysis and the small size into account, our data suggests that ICE-based regimen is an effective mobilization regimen for patients with relapsed or refractory NHL or HL, which achieved excellent APBSC mobilization and a higher chance of proceeding to ASCT. APBSC mobilization and engraftment were not negatively affected by adding rituximab to ICE.
Financial support and sponsorship
This work was supported in part by grants from National Science-Technology Support Plan Projects (No. 2014BAI09B01), Research Special Fund for Public Welfare Industry of Health (No. 200902002-1), Chinese National Major Project for New Drug Innovation (No. 2008ZX09312, No. 2012ZX09303012), Chinese National High Technology Research and Development Program of China (No. 2011AA02A110), the Ministry of Education Doctor Foundation of China (No. 20010023018, No. 20050023045 and No. 200800230019).
Conflicts of interest
There are no conflicts of interest.
Footnotes
Edited by: Li-Min Chen
REFERENCES
- 1.Philip T, Guglielmi C, Hagenbeek A, Somers R, Van der Lelie H, Bron D, et al. Autologous bone marrow transplantation as compared with salvage chemotherapy in relapses of chemotherapy-sensitive non-Hodgkin's lymphoma. N Engl J Med. 1995;333:1540–5. doi: 10.1056/NEJM199512073332305. [DOI] [PubMed] [Google Scholar]
- 2.Baldomero H, Gratwohl M, Gratwohl A, Tichelli A, Niederwieser D, Madrigal A, et al. The EBMT activity survey 2009: Trends over the past 5 years. Bone Marrow Transplant. 2011;46:485–501. doi: 10.1038/bmt.2011.11. [DOI] [PubMed] [Google Scholar]
- 3.Mikesch JH, Kuhlmann M, Demant A, Krug U, Thoennissen GB, Schmidt E, et al. DexaBEAM versus ICE salvage regimen prior to autologous transplantation for relapsed or refractory aggressive peripheral T cell lymphoma: A retrospective evaluation of parallel patient cohorts of one center. Ann Hematol. 2013;92:1041–8. doi: 10.1007/s00277-013-1738-9. [DOI] [PubMed] [Google Scholar]
- 4.Hertzberg MS, Crombie C, Benson W, Taper J, Gottlieb D, Bradstock KF. Outpatient fractionated ifosfamide, carboplatin and etoposide as salvage therapy in relapsed and refractory non-Hodgkin's and Hodgkin's lymphoma. Ann Oncol. 2006;17(Suppl 4):iv25–30. doi: 10.1093/annonc/mdj995. [DOI] [PubMed] [Google Scholar]
- 5.Kim MK, Kim S, Lee SS, Sym SJ, Lee DH, Kim SW, et al. Rituximab-ESHAP as a mobilization regimen for relapsed or refractory B-cell lymphomas: A comparison with ESHAP. Transfusion. 2007;47:1447–54. doi: 10.1111/j.1537-2995.2007.01285.x. [DOI] [PubMed] [Google Scholar]
- 6.Jerkeman M, Leppä S, Kvaløy S, Holte H. ICE (ifosfamide, carboplatin, etoposide) as second-line chemotherapy in relapsed or primary progressive aggressive lymphoma – The Nordic Lymphoma Group experience. Eur J Haematol. 2004;73:179–82. doi: 10.1111/j.1600-0609.2004.00294.x. [DOI] [PubMed] [Google Scholar]
- 7.Swerdllow SH, Campo E, Harris NL. France: IARC Press; 2008. WHO Classification of Tumours of Haematopoietic and Lymphoid Tissues. [Google Scholar]
- 8.Shi YK, Yang S, Han XH, Ma J, Ren HY, Cen XN, et al. A prospective multicenter study of rituximab combined with high-dose chemotherapy and autologous peripheral blood stem cell transplantation for aggressive B-cell lymphoma (in Chinese) Chin J Oncol. 2009;31:592–6. [PubMed] [Google Scholar]
- 9.Han X, Ma L, Zhao L, He X, Liu P, Zhou S, et al. Predictive factors for inadequate stem cell mobilization in Chinese patients with NHL and HL: 14-year experience of a single-center study. J Clin Apher. 2012;27:64–74. doi: 10.1002/jca.21204. [DOI] [PubMed] [Google Scholar]
- 10.Li B, Yang JL, Shi YK, He XH, Han XH, Zhou SY, et al. Etoposide 1.0 g/m2 or 1.5 g/m2 combined with granulocyte colony-stimulating factor for mobilization of peripheral blood stem cells in patients with malignancy: Efficacy and toxicity. Cytotherapy. 2009;11:362–71. doi: 10.1080/14653240802582067. [DOI] [PubMed] [Google Scholar]
- 11.Gertz MA, Wolf RC, Micallef IN, Gastineau DA. Clinical impact and resource utilization after stem cell mobilization failure in patients with multiple myeloma and lymphoma. Bone Marrow Transplant. 2010;45:1396–403. doi: 10.1038/bmt.2009.370. [DOI] [PubMed] [Google Scholar]
- 12.Cheson BD, Horning SJ, Coiffier B, Shipp MA, Fisher RI, Connors JM, et al. Report of an international workshop to standardize response criteria for non-Hodgkin's lymphomas. NCI Sponsored International Working Group. J Clin Oncol. 1999;17:1244. doi: 10.1200/JCO.1999.17.4.1244. [DOI] [PubMed] [Google Scholar]
- 13.Gui L, Shi YK, He XH, Lei YH, Zhang HZ, Han XH, et al. High-dose therapy and autologous stem cell transplantation in peripheral T-cell lymphoma: Treatment outcome and prognostic factor analysis. Int J Hematol. 2014;99:69–78. doi: 10.1007/s12185-013-1465-y. [DOI] [PubMed] [Google Scholar]
- 14.Menzel H, Müller A, Von Schilling C, Licht T, Peschel C, Keller U. Ifosfamide, epirubicin and etoposide rituximab in refractory or relapsed B-cell lymphoma: Analysis of remission induction and stem cell mobilization. Leuk Lymphoma. 2008;49:1337–44. doi: 10.1080/10428190802094229. [DOI] [PubMed] [Google Scholar]
- 15.Vijay A, Duan Q, Henning JW, Duggan P, Daly A, Shafey M, et al. High dose salvage therapy with dose intensive cyclophosphamide, etoposide and cisplatin may increase transplant rates for relapsed/refractory aggressive non-Hodgkin lymphoma. Leuk Lymphoma. 2013;54:2620–6. doi: 10.3109/10428194.2013.783211. [DOI] [PubMed] [Google Scholar]
- 16.Elstrom RL, Andemariam B, Martin P, Ruan J, Shore TB, Coleman M, et al. Bortezomib in combination with rituximab, dexamethasone, ifosfamide, cisplatin and etoposide chemoimmunotherapy in patients with relapsed and primary refractory diffuse large B-cell lymphoma. Leuk Lymphoma. 2012;53:1469–73. doi: 10.3109/10428194.2012.656629. [DOI] [PubMed] [Google Scholar]
- 17.Wood WA, Whitley J, Goyal R, Brown PM, Sharf A, Irons R, et al. Effectiveness of etoposide chemomobilization in lymphoma patients undergoing auto-SCT. Bone Marrow Transplant. 2013;48:771–6. doi: 10.1038/bmt.2012.216. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.DiPersio JF, Micallef IN, Stiff PJ, Bolwell BJ, Maziarz RT, Jacobsen E, et al. Phase III prospective randomized double-blind placebo-controlled trial of plerixafor plus granulocyte colony-stimulating factor compared with placebo plus granulocyte colony-stimulating factor for autologous stem-cell mobilization and transplantation for patients with non-Hodgkin's lymphoma. J Clin Oncol. 2009;27:4767–73. doi: 10.1200/JCO.2008.20.7209. [DOI] [PubMed] [Google Scholar]
- 19.Kewalramani T, Zelenetz AD, Nimer SD, Portlock C, Straus D, Noy A, et al. Rituximab and ICE as second-line therapy before autologous stem cell transplantation for relapsed or primary refractory diffuse large B-cell lymphoma. Blood. 2004;103:3684–8. doi: 10.1182/blood-2003-11-3911. [DOI] [PubMed] [Google Scholar]
- 20.Gisselbrecht C, Glass B, Mounier N, Singh Gill D, Linch DC, Trneny M, et al. Salvage regimens with autologous transplantation for relapsed large B-cell lymphoma in the rituximab era. J Clin Oncol. 2010;28:4184–90. doi: 10.1200/JCO.2010.28.1618. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Kirschey S, Flohr T, Wolf HH, Frickhofen N, Gramatzki M, Link H, et al. Rituximab combined with DexaBEAM followed by high dose therapy as salvage therapy in patients with relapsed or refractory B-cell lymphoma: Mature results of a phase II multicentre study. Br J Haematol. 2015;168:824–34. doi: 10.1111/bjh.13234. [DOI] [PubMed] [Google Scholar]
- 22.Rieger M, Osterborg A, Pettengell R, White D, Gill D, Walewski J, et al. Primary mediastinal B-cell lymphoma treated with CHOP-like chemotherapy with or without rituximab: Results of the Mabthera International Trial Group study. Ann Oncol. 2011;22:664–70. doi: 10.1093/annonc/mdq418. [DOI] [PubMed] [Google Scholar]
- 23.Villa D, Crump M, Keating A, Panzarella T, Feng B, Kuruvilla J. Outcome of patients with transformed indolent non-Hodgkin lymphoma referred for autologous stem-cell transplantation. Ann Oncol. 2013;24:1603–9. doi: 10.1093/annonc/mdt029. [DOI] [PubMed] [Google Scholar]
- 24.Hamlin PA, Zelenetz AD, Kewalramani T, Qin J, Satagopan JM, Verbel D, et al. Age-adjusted International Prognostic Index predicts autologous stem cell transplantation outcome for patients with relapsed or primary refractory diffuse large B-cell lymphoma. Blood. 2003;102:1989–96. doi: 10.1182/blood-2002-12-3837. [DOI] [PubMed] [Google Scholar]
- 25.Matasar MJ, Czuczman MS, Rodriguez MA, Fennessy M, Shea TC, Spitzer G, et al. Ofatumumab in combination with ICE or DHAP chemotherapy in relapsed or refractory intermediate grade B-cell lymphoma. Blood. 2013;122:499–506. doi: 10.1182/blood-2012-12-472027. [DOI] [PMC free article] [PubMed] [Google Scholar]