

Abstract
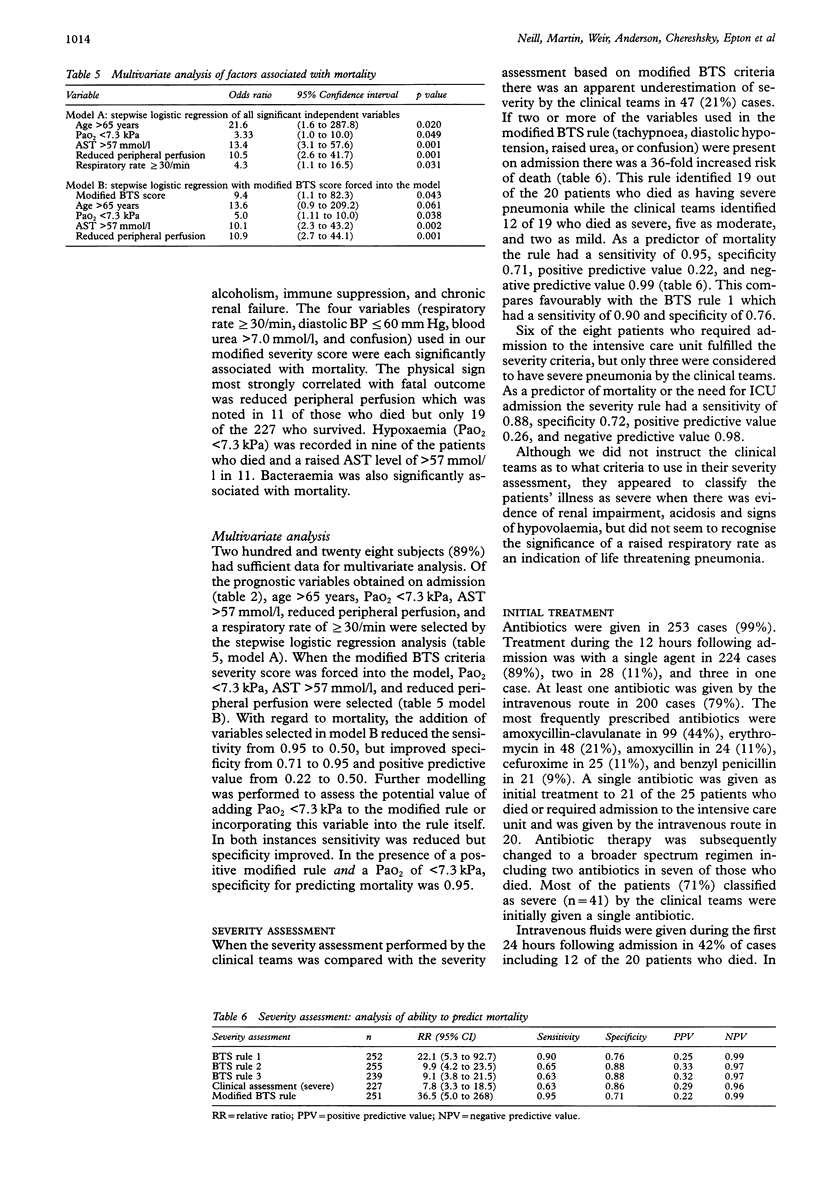
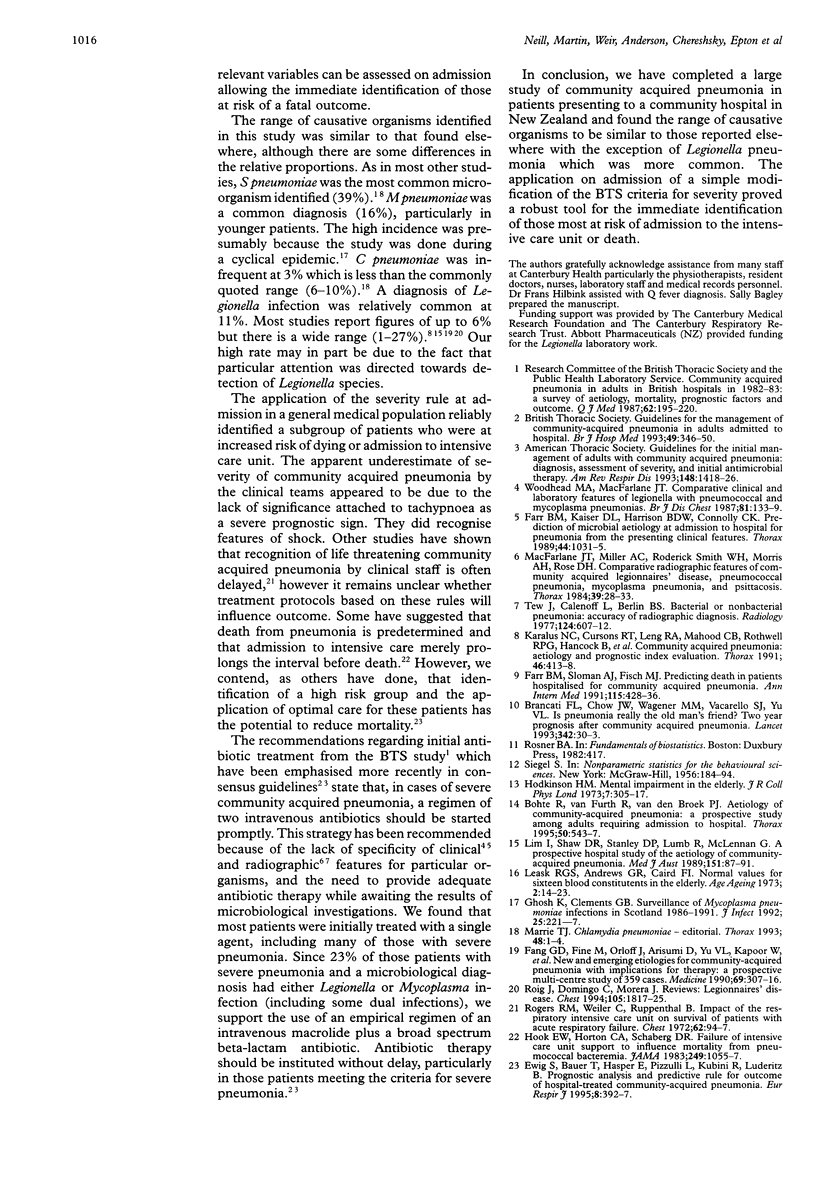
BACKGROUND: Community acquired pneumonia remains an important cause of hospital admission and carries an appreciable mortality. Criteria for the assessment of severity during admission have been developed by the British Thoracic Society (BTS). A study was performed to determine the sensitivity and specificity of a severity rule based on a modification of the BTS prognostic rules applied on admission, to compare severity as assessed by medical staff with the modified rule, and to determine the microbiological cause of community acquired pneumonia in Christchurch. METHODS: A 12 month study of all adults admitted to Christchurch Hospital with community acquired pneumonia was undertaken. Three hundred and sixteen consecutive patients with suspected community acquired pneumonia were screened for inclusion. Variables obtained from the history, examination, investigations, and initial treatment were examined for association with mortality. RESULTS: Two hundred and fifty five patients met the inclusion criteria. Their mean age was 58 years (range 18-97). A microbiological diagnosis was made in 181 cases (71%), Streptococcus pneumonia (39%), Mycoplasma pneumoniae (16%), Legionella species (11%), and Haemophilus influenzae (11%) being the most commonly identified organisms. Patients had a 36-fold increased risk of death if any two of the following were present on admission: respiratory rate > or = 30/min, diastolic BP < or = 60 mm Hg, urea > 7 mmol/l, or confusion. The severity rule identified 19 of the 20 patients who died and six of eight patients admitted to the intensive care unit as having life threatening community acquired pneumonia. The sensitivity of the modified rule for predicting death was 0.95 and the specificity 0.71. In 47 cases (21%) the clinical team appeared to underestimate the severity of the illness. CONCLUSIONS: The organisms responsible for community acquired pneumonia in Christchurch are similar to those reported from other centres except for Legionella species which were more common than in most studies. The modification of the BTS prognostic rules applied as a severity indicator at admission performed well and could be incorporated into management guidelines.
Full text
PDF





Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Bohte R., van Furth R., van den Broek P. J. Aetiology of community-acquired pneumonia: a prospective study among adults requiring admission to hospital. Thorax. 1995 May;50(5):543–547. doi: 10.1136/thx.50.5.543. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Brancati F. L., Chow J. W., Wagener M. M., Vacarello S. J., Yu V. L. Is pneumonia really the old man's friend? Two-year prognosis after community-acquired pneumonia. Lancet. 1993 Jul 3;342(8862):30–33. doi: 10.1016/0140-6736(93)91887-r. [DOI] [PubMed] [Google Scholar]
- Ewig S., Bauer T., Hasper E., Pizzulli L., Kubini R., Lüderitz B. Prognostic analysis and predictive rule for outcome of hospital-treated community-acquired pneumonia. Eur Respir J. 1995 Mar;8(3):392–397. doi: 10.1183/09031936.95.08030392. [DOI] [PubMed] [Google Scholar]
- Fang G. D., Fine M., Orloff J., Arisumi D., Yu V. L., Kapoor W., Grayston J. T., Wang S. P., Kohler R., Muder R. R. New and emerging etiologies for community-acquired pneumonia with implications for therapy. A prospective multicenter study of 359 cases. Medicine (Baltimore) 1990 Sep;69(5):307–316. doi: 10.1097/00005792-199009000-00004. [DOI] [PubMed] [Google Scholar]
- Farr B. M., Kaiser D. L., Harrison B. D., Connolly C. K. Prediction of microbial aetiology at admission to hospital for pneumonia from the presenting clinical features. British Thoracic Society Pneumonia Research Subcommittee. Thorax. 1989 Dec;44(12):1031–1035. doi: 10.1136/thx.44.12.1031. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ghosh K., Clements G. B. Surveillance of Mycoplasma pneumoniae infections in Scotland 1986-1991. J Infect. 1992 Sep;25(2):221–227. doi: 10.1016/0163-4453(92)94196-5. [DOI] [PubMed] [Google Scholar]
- Hodkinson H. M. Mental impairment in the elderly. J R Coll Physicians Lond. 1973 Jul;7(4):305–317. [PMC free article] [PubMed] [Google Scholar]
- Hook E. W., 3rd, Horton C. A., Schaberg D. R. Failure of intensive care unit support to influence mortality from pneumococcal bacteremia. JAMA. 1983 Feb 25;249(8):1055–1057. [PubMed] [Google Scholar]
- Karalus N. C., Cursons R. T., Leng R. A., Mahood C. B., Rothwell R. P., Hancock B., Cepulis S., Wawatai M., Coleman L. Community acquired pneumonia: aetiology and prognostic index evaluation. Thorax. 1991 Jun;46(6):413–418. doi: 10.1136/thx.46.6.413. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Leask R. G., Andrews G. R., Caird F. I. Normal values for sixteen blood constituents in the elderly. Age Ageing. 1973 Feb;2(1):14–23. doi: 10.1093/ageing/2.1.14. [DOI] [PubMed] [Google Scholar]
- Lim I., Shaw D. R., Stanley D. P., Lumb R., McLennan G. A prospective hospital study of the aetiology of community-acquired pneumonia. Med J Aust. 1989 Jul 17;151(2):87–91. doi: 10.5694/j.1326-5377.1989.tb101168.x. [DOI] [PubMed] [Google Scholar]
- Macfarlane J. T., Miller A. C., Roderick Smith W. H., Morris A. H., Rose D. H. Comparative radiographic features of community acquired Legionnaires' disease, pneumococcal pneumonia, mycoplasma pneumonia, and psittacosis. Thorax. 1984 Jan;39(1):28–33. doi: 10.1136/thx.39.1.28. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Marrie T. J. Chlamydia pneumoniae. Thorax. 1993 Jan;48(1):1–4. doi: 10.1136/thx.48.1.1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rogers R. M., Weiler C., Ruppenthal B. Impact of the respiratory intensive care unit on survival of patients with acute respiratory failure. Chest. 1972 Jul;62(1):94–97. doi: 10.1378/chest.62.1.94. [DOI] [PubMed] [Google Scholar]
- Roig J., Domingo C., Morera J. Legionnaires' disease. Chest. 1994 Jun;105(6):1817–1825. doi: 10.1378/chest.105.6.1817. [DOI] [PubMed] [Google Scholar]
- Tew J., Calenoff L., Berlin B. S. Bacterial or nonbacterial pneumonia: accuracy of radiographic diagnosis. Radiology. 1977 Sep;124(3):607–612. doi: 10.1148/124.3.607. [DOI] [PubMed] [Google Scholar]
- Woodhead M. A., Macfarlane J. T. Comparative clinical and laboratory features of legionella with pneumococcal and mycoplasma pneumonias. Br J Dis Chest. 1987 Apr;81(2):133–139. doi: 10.1016/0007-0971(87)90130-6. [DOI] [PubMed] [Google Scholar]