

Abstract
Despite developments in acute stroke therapies, stroke continues to be a leading cause of death and disability worldwide. One major limitation from intravenous thrombolysis with tissue plasminogen activator (t-PA) is patient’s arrival to the emergency room at a tertiary care hospital after the therapeutic time-window, which is generally 270 minutes. The problem is worse for people living in suburban areas where stroke expertise can be missing. Therefore, telestroke networks were developed at several sites where a stroke neurologist at a tertiary hospital participates through synchronous audio-video teleconference in confirming diagnosis of stroke, assessing risks and benefits of giving IV t-PA, and making the decision with the patient and emergency physician at the local hospital. In this article, we will review the experience of major telestroke networks in North America and Europe, and the evidence of its safety and cost-effectiveness. Telestroke complexity, with regard to practice, manpower, quality assurance, and legal issues will be discussed briefly.
Stroke is the third leading cause of death after coronary heart disease and cancers, and the most common cause of disability in adults with huge social and economic burdens.1 In Western countries, around 85% of strokes in adults are ischemic. Accurate stroke statistics are lacking in Saudi Arabia; however, based on the updated WHO records, stroke incidence in Saudi Arabia seems comparable to the USA at approximately 200 cases per 100,000 per year. However, the incidence of “stroke in young” has been reported the highest in certain Middle East countries where data exists. The median age in Saudi Arabia is 25.3 years, with life expectancy at birth of 72 years, while they are 36.9 years and 78.6 years in the USA. These figures suggest stroke will affect the younger population in Saudi Arabia, with an expected higher stroke burden measured in lost quality adjusted life years (QALYs) and money. Intravenous tissue plasminogen activator (IV t-PA) remains the only approved treatment since 1996 for acute ischemic stroke. It has to be administered by stroke experts for selected acute stroke patients, and within a certain setup and an acceptable therapeutic time-window, which is 270 minutes from stroke onset for most acute stroke cases. However, still most of new stroke patients do not receive IV t-PA as part of treatment mainly because they arrive late to the emergency room (ER) beyond the therapeutic time-window. While the IV t-PA administration rate exceeds 20% in some regions in North America,2 it is less than 1% in urban Saudi Arabia, and almost 0% in medically under served areas of small cities and rural areas (unpublished data from tertiary care hospitals in Saudi Arabia). Literature review using EMBASE, PubMed, and MEDLINE was carried out, with a lack of articles found to have a comprehensive review including safety, functionality, and legality of telestroke. The purpose of this review is to create a handy but comprehensive reference for stroke neurologists, emergency room physicians, and hospital directors when planning to develop a telestroke program in Saudi Arabia.
Telemedicine
Telemedicine can be defined as the use of telecommunication technologies to provide medical information and service. Historically, it started more than 4 decades ago to allow communication and discussion between physicians of small hospitals and those of large tertiary care hospitals for non-acute cases where advanced treatment must be planned and agreed on. Therefore, telemedicine started in an asynchronous module where data can be stored and forwarded and then reviewed offline. However, acute care has developed significantly in the last few decades as well as telecommunication technologies, which made synchronous telemedicine possible and in a different format from telephone-based to audio-video teleconference, and this may go further with the attachment of peripheral devices for robotic surgery or procedures under tele-guidance.
Telestroke
We can define telestroke as the emergency use of telecommunication technologies to provide appropriate acute stroke therapy at a distance. A telestroke program using telephone consultation is cheap and takes less time to initiate and to complete, however, it is associated with significant limitations and the risk of making a wrong diagnosis or at least inaccurate acute stroke related deficit evaluation, and then the wrong thrombolysis decision. Most of the current telestroke programs use synchronous two-way audio-video teleconferences, and this is our area of interest in this article. The patient is clinically evaluated using the National Institute of Health Stroke Scale (NIHSS) and the brain image is reviewed by a stroke neurologist from a distance, and then a thrombolysis decision is taken. In one randomized controlled study, the audio-video teleconference was compared to the telephone-based telestroke and was found to be more sensitive, more specific, and more likely to lead to the right thrombolysis decision.3,4 After confirming the diagnosis of acute stroke, there are 2 important measures to increase the recanalization rate with significant clinical benefit: thrombolysis rate (percentage of acute stroke patients who received IV t-PA within the therapeutic window) and IV t-PA needle time (time from stroke onset to IV t-PA bolus). Currently, 2 options exist for acute stroke patients’ care in medically under served areas: either urgent patient transfer to a tertiary care hospital where acute stroke treatment can be administered, or managing the patient at the local hospital. Patient transfer can be via ambulance or air evacuation, which is associated with high transportation costs, smaller increase in thrombolysis rate, and smaller chance for significant recovery if they were treated, because most likely the IV t-PA needle time will be within the last third of the therapeutic time-window, which is associated with higher number needed to treat.5 The second option necessitates telestroke technology so stroke experts share with local physicians the duty of applying evidence-based acute stroke therapy.
Effectiveness of telestroke
We need to look here for 2 measures, the validity of patient assessment using the NIHSS through teleconference, and the effectiveness, including success, and complication rate, of telestroke based intravenous thrombolysis. Few studies have looked into the accuracy of patient assessment using the NIHSS. In one study,6 the NIHSS scores of 20 patients were compared to their NIHSS scores carried out remotely through a broadband-connected workstation. Both assessments were carried out by qualified neurologists. Paired T tests and Pearson correlation coefficients were very strong (r=0.9552, p=0.0001) indicating that high scores in bedside correlate with high scores remotely. For the second measure, we will review published data from major telestroke programs in Europe and North America.
The Reach telestroke network started in 2003 in Georgia, USA.7 By 2005, the network had 7 hospitals in rural areas connected to the Medical College of Georgia via one-way video and two-way audio teleconference system. Between March 2003 and May 2005, 194 acute stroke consultations were made within the 3-hour therapeutic window and 30 patients with a median NIHSS of 12.5 were treated with IV t-PA. Rapid improvement defined as a drop of 4 or more NIHSS points within 24 hours occurred in 18 out of 30 treated patients, and no symptomatic intracerebral hemorrhage occurred. The study interestingly showed a significant reduction in onset to treatment after one year of operation from 143 to 111 minutes. The most common reasons for not treating were rapid improvement, NIHSS was below 4, beyond therapeutic window, or presence of seizure or hemorrhage prior to treatment.
Some other data recently published represents the experience of the University of Pittsburg Medical Center telestroke network with its 12 spoke facilities through audio-video conferencing equipment.8 Between July 2008 and December 2009, 351 telestroke consultations were performed. Eighty-three stroke patients received IV t-PA at the spoke hospitals, and 59 patients at the hub center. The 2 groups were similar in their baseline characteristics including median NIHSS scores and mean “onset to treatment” time. The mean “arrival to treatment” time was longer in the telestroke patients (67.8 versus 98.9 minutes). The study showed no statistical significant difference between the 2 groups in favorable outcomes, symptomatic intracerebral hemorrhage, and mortality rates.
The Northern Alberta telestroke service started in 2003.9 By 2007, 7 spoke centers were connected to the University of Alberta hospital (4 via audio-video teleconference, and 3 via telephone only). In their first 2 years of experience, the telestroke was activated 210 times and only 44 patients were candidates for thrombolysis using IV t-PA. Ten (23%) of them were assessed by the ER physician at the spoke centers without video assessment by a stroke neurologist. Sixteen (40%) patients had a modified Rankin Scale less than 2 by 90 days from IV t-PA, and 9 deaths occurred within 90 days from IV thrombolysis. Only 2 (4.5%) of the treated patients had t-PA complications with intracerebral hemorrhage, and the rest died due to other mechanisms. The rates of benefits and side effects were comparable to those treated on site.
The Telemedical Project for Integrative Stroke Care (TEMPiS) was established in 2003 serving a large area in South East Bavaria, Germany.10 It comprised 12 spoke hospitals connected to 2 academic centers in Munich via video teleconference and CT/MRI image transfer. Each spoke hospital had a multidisciplinary stroke team and monitoring facilities. Currently, TEMPiS is considered to be the largest telemedical stroke service in the world. TEMPiS was associated with significant improvement of acute in-hospital stroke treatment in terms of quality indicators such as rapid brain imaging, thrombolysis rate, assessment of swallowing disorders, and early rehabilitation therapy.11 When patients served with TEMPiS were compared to similar acute stroke patients within the same region, but not served with telemedicine, TEMPiS showed significant reduction in “death and dependency” outcome at 3, 12, and 30 months,10,12 without a significant difference in “mortality rate” alone.
The thrombolysis rate in most of the published data of different telestroke networks ranges from 18-51%.7-10 Reasons for no IV t-PA include stroke onset beyond 270 minutes, presence of contraindication that was not recognized by the ER physician at the spoke hospital, or patient having a stroke mimic like seizure with Todd’s paralysis, CNS neoplasm with sudden deterioration, CNS infection, and others. Considering the threat of these acute stroke mimics, on-call stroke neurologists are still of great benefit to the patients and the spoke hospitals. The small waste of telestroke resources on acute stroke mimics is well compensated by the gain of managing these urgent neurological conditions despite the fact that some patients were required to be transferred to the University hospital anyway. With time and experience, the thrombolysis rate tends to increase at active spoke centers.
Three different methods of practicing telestroke
There are 3 nonexclusive methods of clinical operation of telestroke: “Drip and keep,” which means after telestroke consultation and approval for IV t-PA, the IV t-PA is infused at the spoke center followed by admission there for observation and stroke work up. This requires a local stroke unit with at least minimal acceptable quality of care with multidisciplinary teams to have an integrative telestroke network. A follow up assessment by a stroke neurologist can also be carried out by telestroke, or through outpatient visit to the hub center a few weeks later. For further complications during the acute phase of treatment, urgent telestroke consultation can be initiated again by the treating physician at the hub hospital. The second method is the “ship” method, which is recommended for patients with an acute stroke with contraindication for IV t-PA, but that can still have intraarterial t-PA, or an endovascular procedure, and mechanical removal/disruption of the clot (for example: patients on anti-coagulation with INR >1.6). Here, the patient gets transferred directly to the hub center for urgent treatment and intervention. The third way is “drip and ship” and indicated for those acute stroke patients who are candidates for IV t-PA. However, the consulting spoke hospital cannot provide appropriate post-tPA care or stroke workup. The patient can have the IV t-PA infused locally, and then shipped to the hub center. Developing telestroke networks may better encourage more spoke centers to participate if they choose “drip and ship” since it put less load on the spoke centers, and with time and experience, spoke centers can start admitting patients after thrombolysis. It is also important to mention that the type of clinical practice can be influenced by financial incentives and reimbursements for physicians and hospitals, and by clear job descriptions and duties at each end of the telestroke network, in case of complications or medico-legal claims.
Manpower for a successful telestroke network
The quantity and type of manpower required for a telestroke network varies, and depends on the proposed size of the network, type of clinical operation, and complexity of care. It also varies from one spoke center to another within the same telestroke network. Based on experience, each hub center needs 4 or more stroke neurologists, one of them assigned as the medical director of the network, one telestroke manager, one data manager, 2 telestroke nurses, and 2 information technologists, plus the clinical and administrative back up support from the tertiary hospital. For each spoke center, you need to involve at least the emergency physicians, emergency nurses directed by the head of ER there, plus a program manager. For drip and keep practice, the multidisciplinary teams including the internists should be added. Effective and interactive relationships between different network sites, frequent sites visits between hub and spoke personnel, continuing medical educational activities, and sharing data, and successful stories are mandatory for sustainability and further development.
Telestroke quality measures
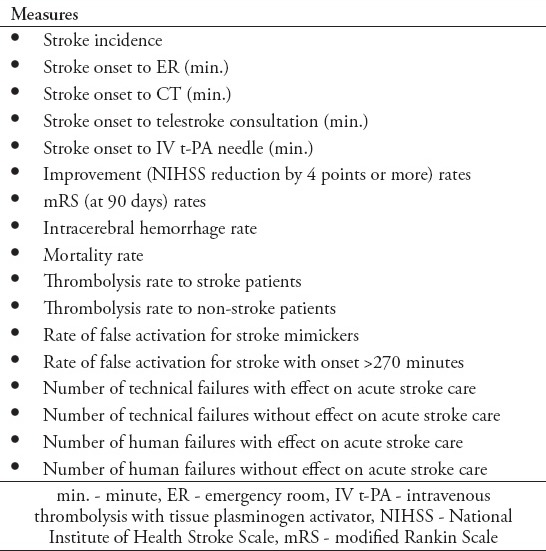
The recommended quality and performance measures for acute stroke units should be used to assess quality and performance of the telestroke networks plus other measures that are specific to telestroke, such as those concerned with communication (Table 1). The director of the telestroke network must obtain the data regularly from each spoke, and hub center, and discuss them at least once annually with all network staff in a transparent fashion with the intention to improve quality and reduce failures. Professionals of each telestroke network should also compare their network performance with other networks nationally and internationally.
Table 1.
Common quality measures for telestroke networks.
Legal issues
Today, most tertiary care hospitals are either practicing some form of telemedicine or considering it soon. The practice can be limited to certain health care networks of similar financial and legal jurisdiction, or may go beyond different states’ borders. Therefore, the first legal issue is getting the license from an appropriate body based on the defined map of telemedicine practice, and making sure the practice does not exceed that map. The second challenge is staff accreditation as different hospitals may have different regulations and requirements. For example in Saudi Arabia, although the Saudi Commission for Health Specialties has a set of regulations concerning staff accreditation to designated positions, tertiary care hospitals like King Khalid University Hospital have added further requirements. Therefore, mutual agreement on staff accreditation between the spoke and hub centers is needed with defined rules and areas of practice, and then hospitals do not need to change their accreditation requirements in order to practice telemedicine. The third challenge is agreement on sharing electronic medical records and patient’s data without breaking rules of confidentiality and privacy. It requires a detailed description of data transfer, use, and storage. This agreement can be initiated by the hospitals’ boards, but needs to be approved by the appropriate licensing/legal body.
The general regulations of patient care are still applicable and mandatory in telestroke practice. As the telestroke network expands and more cases are treated, the hub stroke neurologists may become overwhelmed between their regular hospital duties and telestroke cases, but they will still be legally responsible for delivering the telestroke service on time; otherwise, they may be blamed for negligence. The director of the telestroke network needs to adequately estimate the required number of stroke neurologists based on the size of the population served, and ensure a fair and stable reimbursement system; otherwise, staff-recruitment failure may occur.
A medical error or failure to serve the acute stroke patient on time can be related to the staff at the spoke center, staff at the hub center, technology related, patient related, or mixed. Therefore, a 24/7 documentation and auditing system is needed. The job description of every staff member within the network must be clearly written and defined. Patient/proxy consent must be obtained prior to thrombolysis. Regular telestroke morbidity and mortality educational activities must run and be shared between all network sites to enhance the learning curve at different levels as well as discussing successful stories.
Economics
Stroke has a huge economic burden on patients and societies. For example in the USA alone, the direct and indirect costs associated with stroke for 2008 are approximately US$65.5 billion.13 Fagan and colleagues14 showed that acute stroke treatment with IV t-PA is associated with an incremental cost savings of US$8,000 per QALY gained,and telestroke was proved to increase thrombolysis rates mainly in patients living in suburban and rural areas.15 There are 2 cost categories associated with telestroke: equipment costs and telestroke running costs, including physician’s compensations and salaries for network employees. The annual telestroke hub equipment cost is approximately US$16,204/site, and the annual telestroke spoke equipment costs are approximately US$5,309/site,16 which are cheap when we consider today’s medical costs. When looking into the cost-effectiveness of telestroke, we consider the telestroke running costs from one side, which are more or less predictable per network’s size, versus the thrombolysis-related savings, such as less or no disability, shorter length of stay at hospital, and savings from less patients’ transportation. The cost-effectiveness ratio can be non-constant and affected by the network’s performance and number of cases treated. Too reduce its costs further, it can be part of a synchronous telemedicine network so some resources are shared with other acute medical consultation services.
In conclusion, telestroke is the only solution in many countries to serve suburban areas and to increase the thrombolysis rate. The evidence shows that it is safe and cost-effective. New regulations are needed to ensure its legality and stability, and initiatives should come from stroke neurologists, ER physicians, and medical directors of small hospitals.
Footnotes
Disclosure.
References
- 1.World Health Organization. Cardiovascular disease: The atlas of heart disease and stroke [homepage on the Internet]. [Accessed 2014 June 7] Geneva (CH): WHO; Available from: http://www.who.int/cardiovascular_diseases/en/cvd_atlas_16_death_from_stroke.pdf?ua=1 . [Google Scholar]
- 2.van Wijngaarden JD, Dirks M, Huijsman R, Niessen LW, Fabbricotti IN, Dippel DW, et al. Hospital rates of thrombolysis for acute ischemic stroke: the influence of organizational culture. Stroke. 2009;40:3390–3392. doi: 10.1161/STROKEAHA.109.559492. [DOI] [PubMed] [Google Scholar]
- 3.Meyers BC, Raman R, Hemmen T, Obler R, Zivin JA, Roa R, et al. Efficacy of site-independent telemedicine in the STRokE DOC trial: a randomized, blinded, prospective study. Lancet Neurol. 2008;7:787–795. doi: 10.1016/S1474-4422(08)70171-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Capampangan DJ, Wellik KE, Bobrow BJ, Aguilar MI, Ingall TJ, Kiernan TE, et al. Telemedicine versus telephone for remote emergency stroke consultations: a critically appraised topic. Neurologist. 2009;15:163–166. doi: 10.1097/NRL.0b013e3181a4b79c. [DOI] [PubMed] [Google Scholar]
- 5.Hacke W, Kaste M, Bluhmki E, Brozman M, Dávalos A, Guidetti D, et al. Thrombolysis with alteplase 3 to 4.5 hours after acute ischemic stroke. N Engl J Med. 2008;359:1317–1329. doi: 10.1056/NEJMoa0804656. [DOI] [PubMed] [Google Scholar]
- 6.Wang S, Lee SB, Pardue C, Ramsingh D, Waller J, Gross H, et al. Remote evaluation of acute ischemic stroke: National Institutes of Health Stroke Scale via telestroke. Stroke. 2003;34:e188–e192. doi: 10.1161/01.STR.0000091847.82140.9D. [DOI] [PubMed] [Google Scholar]
- 7.Hess DC, Wang S, Hamilton W, Lee S, Pardue C, Waller JL, et al. REACH: clinical feasibility of a rural telestroke network. Stroke. 2005;36:2018–2020. doi: 10.1161/01.STR.0000177534.02969.e4. [DOI] [PubMed] [Google Scholar]
- 8.Zaidi SF, Jumma MA, Urra XN, Hammer M, Massaro L, Reddy V, et al. Telestroke-guided intravenous tissue type plasminogen activator treatment achieves a similar clinical outcome as thrombolysis at a comprehensive stroke center. Stroke. 2011;42:3291–3293. doi: 10.1161/STROKEAHA.111.625046. [DOI] [PubMed] [Google Scholar]
- 9.Khan K, Shuaib A, Whittaker T, Saqqur M, Jeerakathil T, Butcher K, et al. Telestroke in Northern Alberta: a two year Experience with remote hospitals. Can J Neurol Sci. 2010;37:808–813. doi: 10.1017/s0317167100051489. [DOI] [PubMed] [Google Scholar]
- 10.Audebert HJ, Schenkel J, Heuschmann PU, Bogdahn U, Haberl RL Telemedic Pilot Project for Integrative Stroke Care Group. Effects of the implementation of a telemedical stroke network: the Telemedic Pilot Project for Integrative Stroke Care (TEMPiS) in Bavaria, Germany. Lancet Neurol. 2006;5:742–748. doi: 10.1016/S1474-4422(06)70527-0. [DOI] [PubMed] [Google Scholar]
- 11.Audebert HJ, Wimmer ML, Hahn R, Schenkel J, Bogdahn U, Horn M, et al. Can telemedicine contribute to fulfill WHO Helsingborg Declaration of specialized stroke sare? Cerebrovascr Dis. 2005;20:362–369. doi: 10.1159/000088064. [DOI] [PubMed] [Google Scholar]
- 12.Audebert HJ, Schultes K, Tietz V, Heuschmann PU, Bogdahn U, Haberl RL, et al. Long term effects of specialized stroke care with telemedicine support in community hospitals on the behalf of Telemedical Project for Integrative Stroke Care (TEMPiS) Stroke. 2009;40:902–908. doi: 10.1161/STROKEAHA.108.529255. [DOI] [PubMed] [Google Scholar]
- 13.Rosamond W, Flegal K, Furie K, Go A, Greenlund K, Haase N, et al. Heart disease and stroke statistics--2008 update: a report from the American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Circulation. 2008;117:e25–e146. doi: 10.1161/CIRCULATIONAHA.107.187998. [DOI] [PubMed] [Google Scholar]
- 14.Fagan SC, Morgenstern LB, Petitta A, Ward RE, Tilley BC, Marler JR, et al. Cost-effectiveness of tissue plasminogen activator for acute ischemic stroke. NINDS rt-PA Stroke Study Group. Neurology. 1998;50:883–890. doi: 10.1212/wnl.50.4.883. [DOI] [PubMed] [Google Scholar]
- 15.LaMonte MP, Bahouth MN, Xiao Y, Hu P, Baquet CR, Mackenzie CF. Outcomes from a comprehensive stroke telemedicine program. Telemed J E Health. 2008;14:339–344. doi: 10.1089/tmj.2007.0062. [DOI] [PubMed] [Google Scholar]
- 16.Nelson RE, Saltzman GM, Skalabrin EJ, Demaerschalk BM, Majersik JJ. The cost-effectiveness of telestroke in the treatment of acute ischemic stroke. Neurology. 2011;77:1590–1598. doi: 10.1212/WNL.0b013e318234332d. [DOI] [PMC free article] [PubMed] [Google Scholar]