

Abstract
Background:
Female hairline correction surgery is becoming increasingly popular. However, no guidelines or methods of female hairline design have been introduced to date.
Methods:
The purpose of this study was to create an initial framework based on the novel principles of female hairline design and then use artistic ability and experience to fine tune this framework. An understanding of the concept of 5 areas (frontal area, frontotemporal recess area, temporal peak, infratemple area, and sideburns) and 5 points (C, A, B, T, and S) is required for female hairline correction surgery (the 5A5P principle). The general concepts of female hairline correction surgery and natural design methods are, herein, explained with a focus on the correlations between these 5 areas and 5 points.
Results:
A natural and aesthetic female hairline can be created with application of the above-mentioned concepts.
Conclusion:
The 5A5P principle of forming the female hairline is very useful in female hairline correction surgery.
Female hairline correction surgery is increasingly popular in East Asians, whose faces are flatter, wider, and more brachycephalic, particularly from side to side.1 The demand for this surgery is expected to continue growing.
Female hairline correction surgery should be performed only as an aesthetic plastic surgical procedure and requires different perspectives, designs, and surgical techniques. The aim of such surgery is to make the face small, slim, feminine, and more attractive. Thus, many hair surgeons should abandon their views of classic male or female hair loss surgery and consider female hairline correction surgery from a new perspective.
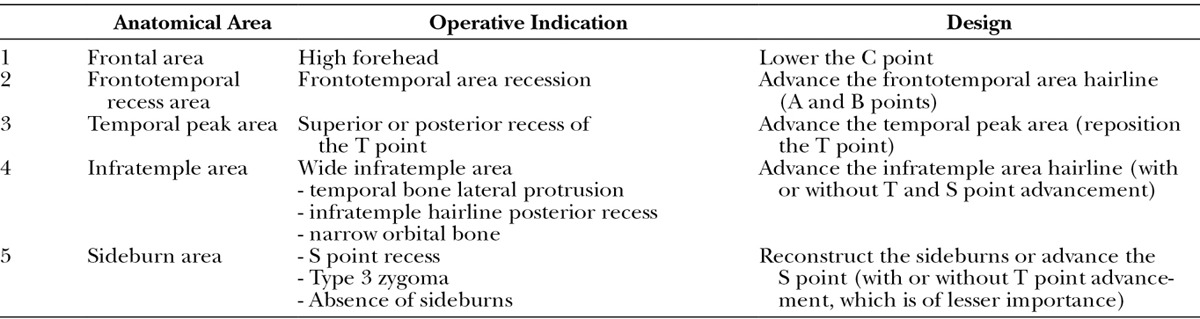
However, little has been published about the most suitable design methods for female hairline correction surgery. This article describes an approach to designing the female hairline based on the most important 5 areas and 5 points in female hairline correction surgery (the 5A5P principle; Table 1).
Table 1.
Surgical Indications and Basic Design Concepts According to the 5A5P Principle
DESIGN TECHNIQUE
The Five Important Areas in Female Hairline Correction Surgery
Frontal Area
The frontal area is similar to the frontal tuft in male hair transplantation surgery (Fig. 1).2 A small triangular area called the widow’s peak or central peak is often present at the very front of the frontal area. Regardless of whether a central peak is present, the most anterior point of the mid-frontal area is called the C point. Nusbaum and Fuentefria3 reported that the central peak is present in approximately 81% of women. However, this is only a description of the phenomenon as it occurs; it is meaningless to refer to any hairline as normal.
Fig. 1.
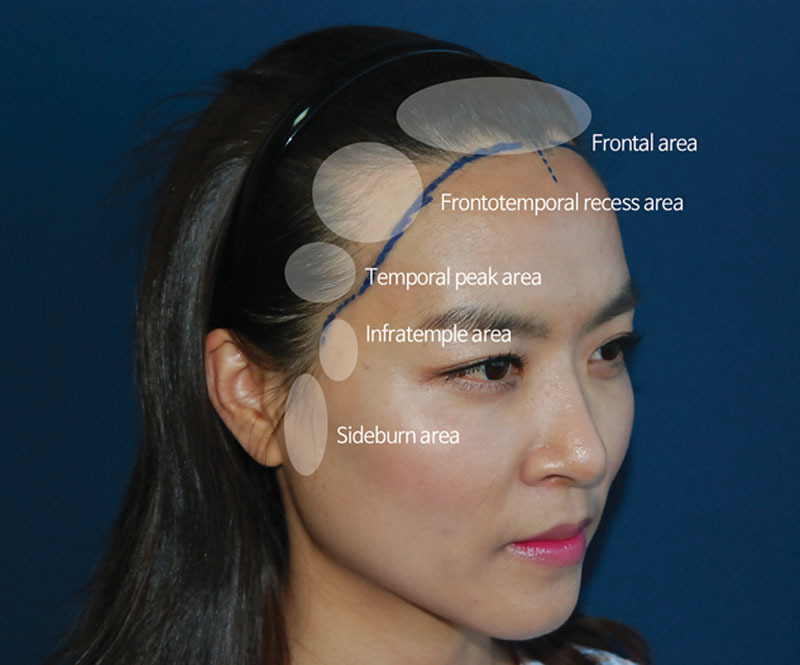
Five areas contributing to the frame of the female hairline.
Frontotemporal Recess Area
An M-shaped frontotemporal recess area is the most common reason that female patients request hairline correction because this hairline shape creates an older, more masculine look; is less attractive; and tends to make the face appear larger.4
Because East Asians have a brachycephalic facial skeleton in contrast to Caucasians’ dolichocephalic shape, the definition of the frontotemporal recess area is quite different between these 2 groups. Considering the facial skeleton as a cube, the frontotemporal recess area is located on the frontal plane in the brachycephalic face, making the face look much larger and older or more masculine. However, the frontotemporal recess area is not apparent in the frontal view of dolichocephalic white faces. This is because the frontotemporal recess area is 3-dimensionally located not in the frontal plane but in the lateral plane.
Temporal Peak Area
The area of the temporal hairline that protrudes over the anterior side in a triangular shape is called the temporal peak area. If the temporal peak is recessed into the superior or posterior side, the face does not appear slim but rather appears round, flattish, large, and unattractive.
Infratemple Area
The small area between the temporal peak area and the sideburn area has very important clinical significance. If the infratemple hairline is corrected during side hairline correction, an attractive egg-shaped face can be created (Fig. 2). The hairline in the infratemple area is usually made into a concave shape, similar to the lateral orbital rim. A slightly concave shape design should be made along the straight line connecting the T point and S point. Thus, the infratemple area can essentially be determined according to the positions of the T point and S point.5
Fig. 2.
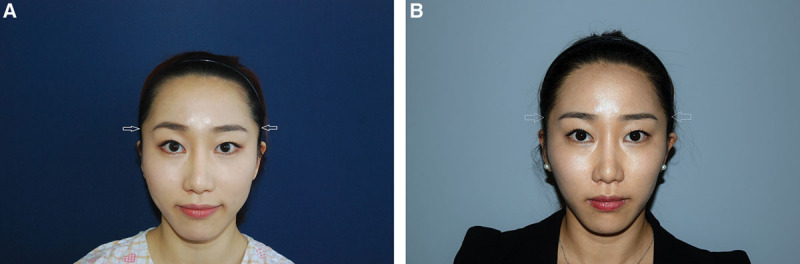
Infratemple area correction effectively creates a feminine and slim facial outline. A, Preoperative view. B, Three-year postoperative view.
There are 3 typical cases in which the infratemple area appears wide: (1) in the case of lateral protrusion of the temporal bone, (2) when the hairline of the infratemple area is receding, and 3) when both sides of the orbital bone are small. In such cases, hairline correction at this site is advanced to create a smooth, slim, and aesthetic facial outline and hairline.
Sideburn Area
The sideburn area is located in same horizontal plane with the zygomatic arch, and their positions overlap. Thus, the type of zygomatic arch influences the design around the sideburn area. More precisely, the infratemple area exists on a horizontal plane, as do the temporal and orbital bones. The infratemple area is located midway between the temporal and orbital areas and serves as a bridge that connects the 2 parts. Thus, the design of the infratemple area is affected by the type of temporal bone and orbital bone. In contrast, the sideburn area is affected by the shape of the zygomatic bone. Park1 classified the zygomatic bone into 4 types according to its form and proposed specific criteria for choosing the most suitable method (zygomatic reduction or side hairline correction) for slimming the mid-face depending on these 4 zygomatic bone types. He explained the meaning of the S point, the indications and operative techniques for anterior advancement of the S point, and sideburn reconstruction instead of zygoma reduction surgery. He also explained that this is useful only for patients with a type 3 zygoma according to his zygomatic bone classification.
Five Critical Points in Female Hairline Design
Upon understanding the following 5 points, a female hairline that seems very complex becomes very simple and easy to understand. These 5 points are easy to explain, remember, and reproduce (Fig. 3).
Fig. 3.

Five important landmark points in female hairline design. A, Preoperative design concept with 5 points. In this case, A ≠ C, A–C distance = 2 cm, B ≠ T, B–T distance = 0.8 cm, and S point is fixed. B, Six-month postoperative view.
C Point
The C point is the most anterior point of the mid-frontal area and is defined regardless of whether a central peak is present. The location of the C point serves as the reference point for hairline symmetry and indicates the height of the frontal hairline. If the C point deviates to the right or left, centralization will achieve symmetry and greater aesthetics. A height of 6.0–6.5 cm from the mid-glabella point is common for the C point, but the present author prefers a height of about 7.0 cm for surgical lowering of the hairline. However, 7 cm is not a definite rule that must always be followed; this distance can vary depending on the patient’s overall facial features, facial symmetry, personal preference, and other factors.
A Point
The A point refers to the starting point of the newly made hairline from the existing frontal area hairline. The A point should be brought as close as possible to the C point, if not to the same location, to make a face appear shorter. The A point should be moved laterally away from the C point to make a face appear longer.
B Point
The B point refers to the ending point at which the newly made hairline meets the existing temporal peak area hairline. The relationship between the B and T points is important in determining the hairline design. When the B point is closer to the T point, a face appears slimmer; as the B point moves away from the T point, the face above the T point appears larger. However, movement toward the T point is not always indicated; this can differ depending on the overall face shape, personal preference, hair characteristics, and other patient-related factors.
T Point
The T point refers to the most anterior point of the temporal peak area. If the temporal peak area is recessed superiorly, correction surgery should move it inferiorly. If the temporal peak area is recessed posteriorly, it should be moved and repositioned anteriorly.
S Point
The most anterior point of the sideburns is called the S point. It is closely related to the shape of the zygomatic arch.
The basic principle of female hairline correction is to determine the location of the 5 important landmark points discussed above. Once these 5 areas and 5 points are understood, approximately 90% of the design of a female hairline correction surgery is complete.
Relationship Between A and C Points
When the A point is closer to the C point, the face appears more round because the height appears lower. When the A point is more distant from the C point, the height of the face appears greater, but the overall shape appears slim.
The positions of the A and C points are determined by comprehensive consideration of the direction of the frontal hairline, including the hair thickness, presence of cowlicks, presence of a frontal whorl, rotation direction of the hair, characteristics of the hair in the donor area, overall face type, and similar factors.
Hairline Design Around the T Point (Relationship Between B and T Points)
In general, the hairline design in the vicinity of the T point can be divided into 3 patterns. The most important single rule is that a new hairline that starts at the A point and leads to the S point through the B and T points should not appear to be straight. This creates a doll-like appearance that looks awkward and artificial.6 To accomplish a natural look, the hairline is designed in the shape of 3 patterns in the vicinity of the T point (Fig. 4), as described below.
Fig. 4.

Variations in hairline design around the T point. A, Lazy-S line. B, Reversed lazy-S line. C, Wavy line.
Lazy-S Line (B–T Distance >0.8–1.0 cm)
The lazy-S line is a design that reduces the infratemple area to a greater degree than the area immediately above the T point. The B–T distance should be longer than 0.8–1.0 cm according to the overall size of the face; when it is shorter than 0.8–1.0 cm, it still appears to be a straight line when viewed from a distance.
Reversed Lazy-S Line (B = T)
The reversed lazy-S line is the opposite of lazy-S line. It reduces the area immediately above the T point as much as possible with a B = T design. Similarly, to avoid creating a straight line, the infratemple area line should be curved slightly to the rear side.
Wavy Line (B = T)
A wavy line is an intermediate form of the lazy-S line and reversed lazy-S lines with B = T design. It is a moderately shaped line above and below the T point.
Selection of New T Point Location
Height of the T Point
The eyebrow is a reference structure used to determine the new location of the T point. It should be equal to or higher than the horizontal plane of the highest point of the eyebrow body. If the T point is located below this plane, the side hairline (framework) appears to be dragged downward, resulting in an awkward appearance (Fig. 5).
Fig. 5.
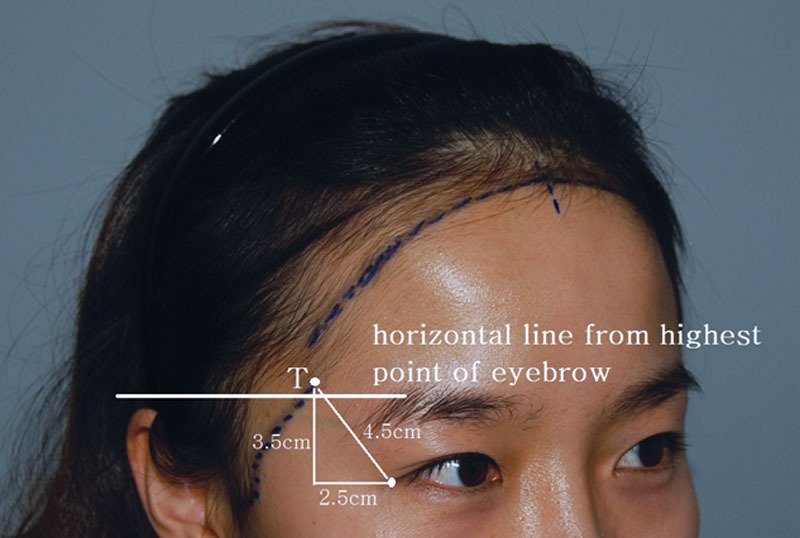
Height selection of the T point. The height of the T point should be equal to or higher than the horizontal plane of highest point of the eyebrow body.
Anterior and Posterior Positioning of the T Point
In contrast to the height of the T point, the frontal view is usually considered when making decisions regarding the frontal appearance of the total face. Because it mainly reflects the frontal appearance, the position of the T point should also be considered when determining the locations of the A and B points (or T point) that connect the new hairline (Fig. 6). A vertical distance of 3.5 cm is common for the lateral canthus, along with 2.5 cm horizontally and 4.5 cm directly (Fig. 5). However, the type of frontal bone, overall face shape, and facial symmetry should be considered comprehensively. The T point is rarely located within 2 cm of the eyebrow tail. If the new hairline design is this close, special caution is required to avoid an awkward appearance.
Fig. 6.

Horizontal position of the T point. The horizontal position of the T point is mainly determined by the appearance of the frontal view. A, Preoperative view. B, Preoperative hairline design. C, Postoperative 12 months view.
Hairline Design of Frontotemporal Recess Area, Which Connects A and B Points
The future hairline should cover the line extending from points A and B to the M area. This should be slightly concave (1), reflect a nearly straight line (2), or protrude slightly to the front (3; Fig. 7). The most important criterion in the selection of option 1, 2, or 3 is the overall facial line from the frontal view. The form of the frontal bone, the whole face shape, and the symmetry of the whole face should also be taken into account. To achieve an aesthetically pleasing facial outline, the surgeon should consider separating the top and bottom of the face using the zygomatic arch level as the middle reference point of the face’s vertical height. The most aesthetic and harmonious facial line is created when the top contour line (the line that connects point A to point S through points B and T) appears to be the same as the bottom contour or slightly slimmer.
Fig. 7.
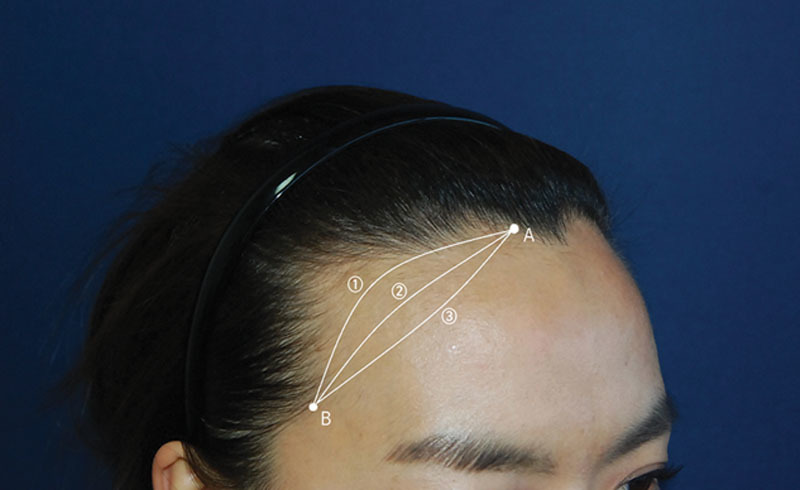
Hairline design of the frontotemporal recess area, which connects the A and B points. The future hairline should cover the line from points A and B to the M area. 1, concave; 2, straight; 3, convex.
The line of option 1 makes the overall face shape somewhat rounder, and it appears to be slightly slimmer because the triangular forehead appears to be closer to the line of 3. The lines of 1 and 2 are usually selected, and special care is required when determining the line of 3 because of its awkward appearance. The line of 3 can be implemented selectively and carefully for patients with thin hair and a convex, protruding forehead rather than a flat forehead if a patient strongly desires it.
Diverting Point
The concept of the diverting point (DP) can be understood when points A and B are determined. The so-called part line (PL) is the line that parts the hair between left and right from the frontal hairline and is connected to the parietal whorl. The concepts of both the DP and PL are essential in female hairline correction. Unlike male hair, which grows toward the front and upward in the frontal area, female hair in the frontal hairline grows toward both lateral sides and at a very acute angle. Thus, there is a point at which the direction of the hair is converted from left to right or vice versa somewhere between the T point on the left and right sides; this is the DP (Fig. 8). The hairline does not suddenly convert from left to right or right to left but changes gradually. Therefore, the DP refers to the midpoint of the zone in which the change in direction is made, and the focal area where the change in direction is made is called the diverting zone.
Fig. 8.

Diverting point (DP). The DP refers to the point at which the hair direction in the frontal hairline is converted from left to right or vice versa. When performing hairline correction surgery in female patients with a high forehead and M-shaped hairline, DP repositioning may be necessary, as shown in this patient. Such a case involves redirecting the hair direction from left to right or vice versa and requires a high level of surgical expertise.
Many people confuse the DP and the PL. However, the DP is not always in the same position as the PL. Therefore, the DP and PL must be distinguished surgically, and each plays a very important role as a surgical landmark in female hairline correction surgery.
All female individuals originally have 100% of their DPs. The reason is unknown, but more than 80–90% of DPs exist on the left side. The most common location is within 2–3 cm from the C point of the mid-frontal line.
A new DP is also made by moving the position of the existing DP anteriorly. It is especially important that the A point moves forward from the preexisting DP position. The change in hair direction that is made along the preexisting DP should, thus, be naturally expressed in a new DP area.
Because the thicker hairs from the occipital donor area are transplanted into the frontal hairline, it is not easy to create a natural appearance by gradually changing the hair exit angle and direction around the DP. Accordingly, the DP is an important design landmark when deciding on the location of the new hairline that will connect points A and B while covering the frontotemporal recess area. Care should be taken in moving the DP forward because of a potentially high level of surgical difficulty (Fig. 8).
Case 1
A 32-year old woman with wide frontotemporal recess area and recession of T and S points (Fig. 9).
Fig. 9.
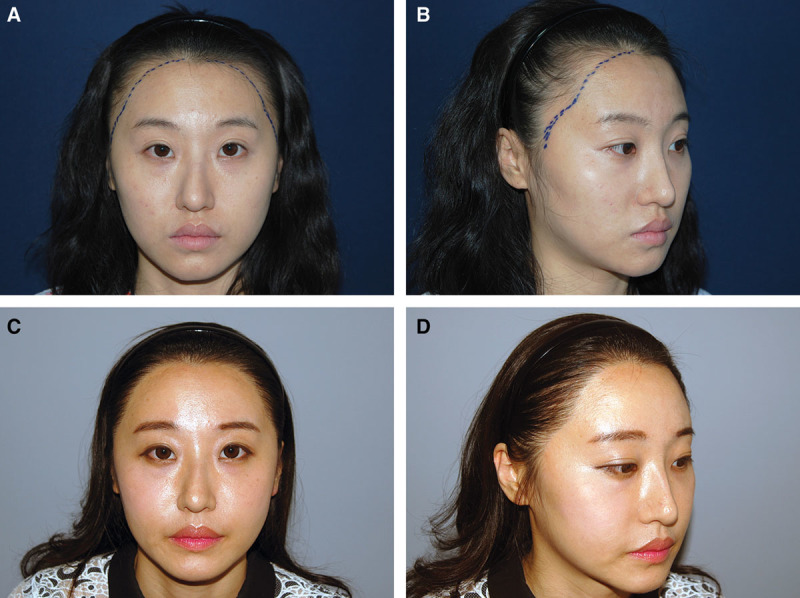
Case 1. A and B, Preoperative design of a 32-year old female patient with wide frontotemporal recess area and recession of T and S points. Following designs were incorporated to improve such facial features: A = C, wavy line (B = T), T point anterior and inferior movement, and slightly anterior movement of S point. C and D, Thirty-two-month postoperative view. The facial contour has been slimmed.
Following designs were incorporated to improve such facial features: A = C, wavy line (B = T), T point anterior and inferior movement, and slightly anterior movement of S point. Clinically satisfactory results were achieved.
Case 2
A 33-year-old woman with severe recession of the frontotemporal area, which was complemented by the following designs; A = C and B = T, while leaving T and S points fixed. As delineated in the photographs, the detailed design points led to successful results (Fig. 10).
Fig. 10.
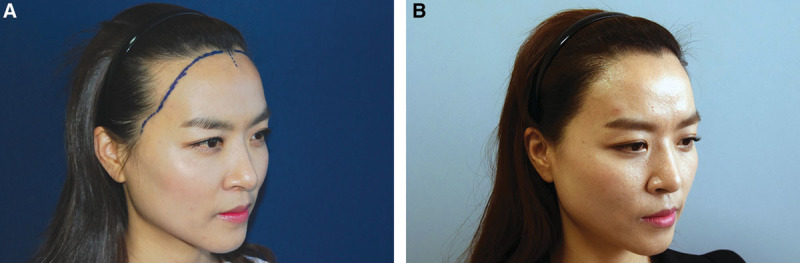
Case 2. A. Preoperative design of a 33-year-old female patient with severe recession of the frontotemporal area. Following designs were implemented: A = C and B = T, while leaving T and S points fixed. B, 2.6-year postoperative view.
CONCLUSION
The 5A5P principle of forming the female hairline design is very useful in female hairline correction surgery.
PATIENT CONSENT
Patients provided written consent for the use of their images.
Footnotes
Disclosure: The authors have no financial interest to declare in relation to the content of this article. The Article Processing Charge was paid for by the authors.
REFERENCES
- 1.Park JH. Side-hairline correction in Korean female patients. Plast Reconstr Surg Glob Open. 2015;3:e336. doi: 10.1097/GOX.0000000000000304. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Shapiro R, Shapiro P. Hairline design and frontal hairline restoration. Facial Plast Surg Clin North Am. 2013;21:351–362. doi: 10.1016/j.fsc.2013.06.001. [DOI] [PubMed] [Google Scholar]
- 3.Nusbaum BP, Fuentefria S. Naturally occurring female hairline patterns. Dermatol Surg. 2009;35:907–913. doi: 10.1111/j.1524-4725.2009.01154.x. [DOI] [PubMed] [Google Scholar]
- 4.Jung JH, Rah DK, Yun IS. Classification of the female hairline and refined hairline correction techniques for Asian women. Dermatol Surg. 2011;37:495–500. doi: 10.1111/j.1524-4725.2011.01910.x. [DOI] [PubMed] [Google Scholar]
- 5.Park JH, Moh JS. Camouflaging the posterior zygomatic arch protrusion after zygoma reduction surgery. Aesthet Surg J. 2012;32:661–664. doi: 10.1177/1090820X12448816. [DOI] [PubMed] [Google Scholar]
- 6.Park JH. Secondary female hairline correction surgery in Korean: Various operative techniques and methods. Arch Aesth Plast Surg. 2013;19:129–135. [Google Scholar]