

Abstract
Background:
Human immunodeficiency virus (HIV) infected individuals frequently suffer from anxiety and depression. Depression has been associated with rapid decline in CD4 counts and worsened treatment outcomes in HIV-infected patients. Yoga has been used to reduce psychopathology and improve immunity.
Aim:
To study the effect of 1-month integrated yoga (IY) intervention on anxiety, depression, and CD4 counts in patients suffering from HIV-1 infection.
Methods:
Forty four HIV-1 infected individuals from two HIV rehabilitation centers of Manipur State of India were randomized into two groups: Yoga (n = 22; 12 males) and control (n = 22; 14 males). Yoga group received IY intervention, which included physical postures (asanas), breathing practices (pranayama), relaxation techniques, and meditation. IY sessions were given 60 min/day, 6 days a week for 1 month. Control group followed daily routine during this period. All patients were on anti-retroviral therapy (ART) and dosages were kept stable during the study. There was no significant difference in age, gender, education, CD4 counts, and ART status between the two groups. Hospital anxiety and depression scale was used to assess anxiety and depression, CD4 counts were measured by flow cytometry before and after intervention. Analysis of variance – repeated measures was applied to analyze the data using SPSS version 10.
Results:
Within group comparison showed a significant reduction in depression scores (F [1, 21] =4.19, P < 0.05) and non-significant reduction in anxiety scores along with non significant increment in CD4 counts in the yoga group. In the control group, there was a non-significant increase in anxiety and depression scores and reduction in CD4 counts. Between-group comparison revealed a significant reduction in depression scores (F [1, 21] =5.64, P < 0.05) and significant increase in CD4 counts (F [1, 21] =5.35, P < 0.05) in the yoga group as compared to the control.
Conclusion:
One month practice of IY may reduce depression and improve immunity in HIV-1 infected adults.
Keywords: Anxiety, CD4 count, depression, human immunodeficiency virus, yoga
INTRODUCTION
Human immunodeficiency virus (HIV) infection is a communicable disease leading to significant morbidity, mortality, and poor quality of life. Approximately, 2.5 million individuals were found to be infected with HIV-1 infection in the 2009 survey. Though anti-retroviral therapy (ART) has significantly increased the life span and treatment outcome in HIV-infected patients, social stigma, depression, substance abuse, and wrong cultural beliefs significantly impair their quality of life.[1] Mental disorders such as major depressive disorder, generalized anxiety, and agoraphobia are commonly found in patients with HIV.[2] Out of all these, depression is the most prevalent comorbid mental disorder with a prevalence of 22–38% among HIV-infected patients.[3,4,5] Unemployment, lack of health insurance, low CD4+ cell counts, not having a partner, and poor quality of social support are significant contributors for depression in HIV-infected patients.[6] Depression is found to be associated with poor adherence to ART,[7] and also influences CD4 counts and viral loads (VLs) negatively.[8] Antidepressant medications are helpful, but they are not free from side effects.
Complementary and alternative medicine is becoming popular as rehabilitation measures in patients living with HIV/AIDS.[9] Yoga is the most commonly used mind–body intervention.[10] It is cost-effective and easy to implement and offers benefit for emotional, psychological, and physical health.[11] Yoga encompasses asanas (Yogic postures), pranayama (Yogic breathing practices), yoga-based relaxation techniques, and meditation.
Many studies demonstrated the broad positive impact of yoga in health and many disease conditions.[12] Yoga can augment current treatment modalities of HIV infection.[13] Yoga helps in many psychological conditions such as anxiety, depression, and schizophrenia. It improves overall well-being and quality of life in many chronic medical illnesses. Earlier studies reported the potential role of yoga in resisting the impairment of cellular immunity.[14] In a study in healthy volunteers, Yoganidra (a yogic relaxation technique) practice given for 30 min daily for 6 months showed a significant reduction in erythrocyte sedimentation rate than the control group.[15] In another study, yoga practice improved natural killer cell activity in early breast cancer patients.[16] In a randomized control trial on pulmonary tuberculosis patients, 2 months of yoga practice helped in reducing the infection.[17]
Yoga is proven to be safe and effective in reducing depression and anxiety.[18] In a study, yoga helped reduction of blood pressure in pre-hypertensive HIV-1 infected subjects.[19] Earlier, meditation and Qigong practice had been found useful in reducing anxiety and depression, and increasing T-cell count in HIV-infected patients.[20] But, this study was done on a small sample of HIV-infected patients and lacked control group. Hence, there is a need for exploration of this area with a better design. Therefore, present study was planned with an intention to assess the effect of a month-long Integrated Yoga (IY)intervention on psychological health and CD4 counts of HIV-1 infected individuals using a randomized controlled design.
METHODS
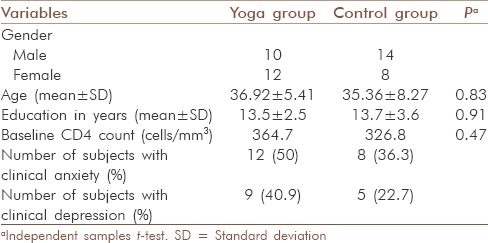
Forty-four HIV-1 infected patients from two HIV rehabilitation centers in Manipur, were selected in this study; subjects were randomly divided into a yoga group (n = 22) and control group (n = 22) using online random number generator software.[21] Subject with active infection, severe weakness, and those under psychiatric medications were excluded from the study. All the participants were educated at least up to 12th standard [Table 1].
Table 1.
Demographic data of subjects
Intervention
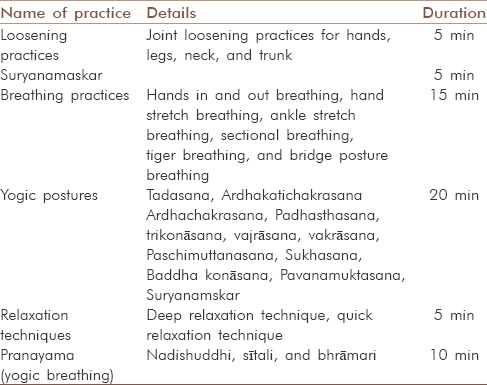
All the subjects in the yoga group performed asanas (Yogic postures), pranayama (Yogic breathing techniques), and yoga-based relaxation techniques [Table 2] 1 h daily, 6 days in a week for 1 month. Control group followed their normal routine activity. Regular attendance was monitored by maintaining attendance register and subjects who attended <70% of sessions were excluded from the study. The yoga module implemented in this study followed typical IAYT session module and details of these practices were given elsewhere.[22]
Table 2.
List of the practices given to the yoga group
Assessments
Hospital anxiety and depression scale
Both groups were administered hospital anxiety and depression scale (HADS), before and after 1 month of yoga intervention. HADS is considered as a valid tool to assess symptom severity and cases of anxiety disorders and depression in both somatic, psychiatric, and primary care patients and in the general population.[23]
CD4 counts
Whole blood samples were collected from all 44 HIV-infected individuals from HIV rehabilitation centers in Manipur for their CD4+ T-cell estimation. To avoid any diurnal variation in the T-cell subset counts, all the samples were collected between 8:00 am and 10:00 am in K2/K3 EDTA vacutainer tubes (Becton Dickinson, Franklin Lakes, NJ, USA) after obtaining an informed consent. The most common technique for measuring CD4 counts in developed country settings is flow cytometry. Flow cytometers use lasers to excite fluorescent antibody probes specific for various cell surface markers, such as CD3, CD4, and CD8, which distinguish one type of lymphocyte from another. We used FACSCount system (Becton Dickinson, San Jose, USA) for CD4 T enumeration. The enumeration of the T cell subsets by the FACSCount system was performed using respective reagents (liquid format). Reagents were maintained at a temperature range of 2–8°C. Strict cold chain was maintained throughout the procedure. The technical details of the procedure are provided elsewhere.[24]
Data analysis
All data were found to be normally distributed by Shapiro–Wilk test. Analysis of variance – repeated measures with Bonferroni's correction was performed to analyze the data using SPSS (IBM, Pvt Ltd) version 10.
RESULTS
Yoga group
In the yoga group, at the baseline, out of 22, 12 (50%) suffered from clinical anxiety (HADS scores >11) and 9 (40.9%) suffered from clinical depression (HADS scores >11). After 1 month of IY, number of subjects with clinical anxiety came down to 9 (40.9%) and those with clinical depression reduced to 2 (9.09%).
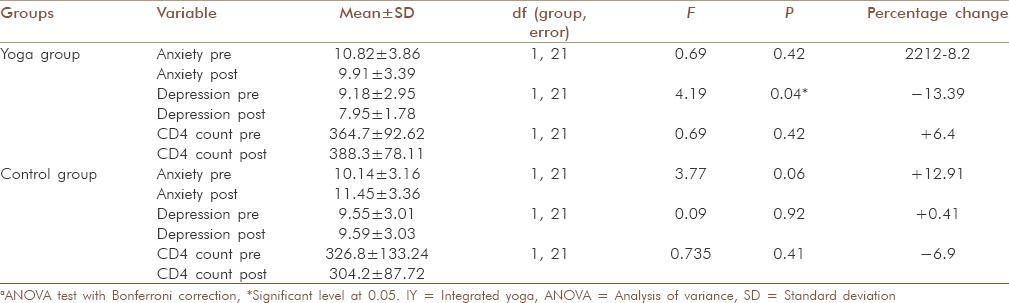
Within-group comparison showed significant reduction in depression (P = 0.04, −13.39%), a nonsignificant improvement in CD4 count (P = 0.42, +6.4%), and a nonsignificant reduction in anxiety scores (P = 0.13, −8.2%) in the yoga group [Table 3 and Graphs 1-3].
Table 3.
Within-group comparisons of both the groups (yoga and control) showing mean and SD of anxiety, depression, and CD4 counts before and after
Graph 1.

Pre- and post-changes in mean and standard deviation in anxiety scores in yoga and control group before and after the study
Graph 3.
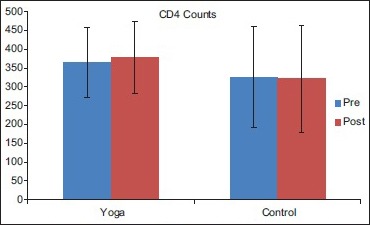
Pre- and post-changes in CD4 counts in yoga and control group before and after the study
Graph 2.
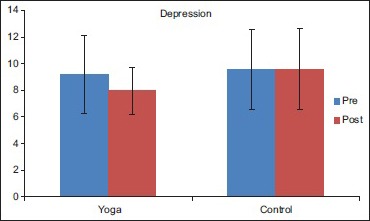
Pre- and post-changes in mean depression scores in yoga and control group before and after the study
Control group
At the baseline, out of 22, 8 (36.3%) suffered from clinical anxiety (HADS scores >11) and 5 (22.7%) suffered from clinical depression (HADS scores >11). After 1 month, 5 (22.7%) had clinical anxiety and 7 (31.81%) had clinical depression.
Nonsignificant increase both in anxiety scores (P = 0.06, +12.91%) and CD4 count (P = 0.41, −6.9%) was observed in control group.
Between-group
There was significant reduction in depression scores (F [1,21] =5.65, P = 0.02) and significant improvement in CD4 counts (F [1,21] =5.35, P = 0.04) in yoga group as compared to control group at the end of one month yoga intervention [Table 4].
Table 4.
Between-group comparison for anxiety, depression, and CD4 counts before and after one-month IY intervention

DISCUSSION
The aim of this study was to observe the effect of 1 month IY intervention on depression, anxiety, and CD4 counts in patients living with HIV-1 infection. Significant reduction in depression and improvement in CD4 counts was observed at the end of 1 month of IY practice, as compared to the control group.
To the best of our knowledge, present work is the first attempt to explore the effect of IY intervention on anxiety, depression, and CD4 counts in HIV-infected individuals. Previously, Koar (1995) assessed the effect of 3-month Qigong practice on anxiety, depression, and CD4 counts of 26 HIV-infected patients in his pilot work.[20] At the end of 1 month, there was an improvement in anxiety by 0.65%, depression by 19.82%, and CD4 counts by 10.89%. We observed an improvement in anxiety, depression, and CD4 counts by 8.2%. 13.39%, and 6.4%, respectively. Higher percentage improvement in CD4 counts in the previous study[20] as compared to that found by us may be due to longer duration of intervention (3 months) than compared to our study (1 month). Similarly, in another controlled study, 1 month of stress management program (biweekly sessions of progressive muscle relaxation, biofeedback, meditation, and hypnosis) reduced anxiety, improved mood, self-esteem, and T cell counts in 20 HIV-positive individuals and found it to be effective in improving all the variables measured.[25] These results are similar to our findings. This suggests an important role of stress management through various mind–body interventions in the clinical care of HIV-infected individuals.
At the baseline, we observed that out of 44 subjects who participated in the study, 20 (45.4%) had scores on HADS above 11, which suggests clinical anxiety and 20 (45.4%) had scores of depression above 11 suggesting clinical depression. Stress and depression are clearly linked and stress may precipitate or exacerbate depressive symptoms and depression.[26] Psychological stress due to HIV-1 diagnosis, social stigma, poor health, and ART medication are the basic causes of depression and anxiety in HIV-1 infected patients. Stress not only leads progression of HIV-1, but also suppress the immunity by affecting immune-neuroendocrine axis.[27] Depression is common among HIV-1 infected patients and it is associated with low CD4 cell counts,[28] presence of depression brings a rapid decline in CD4 counts.[29] Probably, the reduction in depression that we observed in this study is because of reduction in stress levels through yoga. Reduction in depression would have led to increase in the CD4 counts as well.
Strength of the present study includes a randomized controlled design, implementation of a specific validated yoga protocol, and important assessment tools. Major limitations are relatively small sample size, lack of objective assessments tools such as VLs, bio-markers of depression, or imaging techniques.
In future, studies should be planned with large sample size using important biochemical (VLs, markers of inflammation) and radiological variables. Future studies should also assess the effect of long-term IY intervention on these variables.
CONCLUSION
Regular practice of yoga helps to improve psychological well-being by reducing depression and improves immunity by increasing CD4 counts in patients suffering from HIV1. Hence, yoga can be a useful adjuvant in the conventional management of HIV-1 infection.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- 1.Aranda NB. Quality of life in HIV-1 – Positive patient. J Assoc Nurses AIDS Care. 2004;15:20–7. doi: 10.1177/1055329004269183. [DOI] [PubMed] [Google Scholar]
- 2.Shacham E, Onen NF, Donovan MF, Rosenburg N, Overton ET. Psychiatric diagnoses among an HIV-infected outpatient clinic population. J Int Assoc Provid AIDS Care. 2014 doi: 10.1177/2325957414553846. pii: 2325957414553846. [DOI] [PubMed] [Google Scholar]
- 3.Masiello A, De Guglielmo C, Giglio S, Acone N. Beyond depression: Assessing personality disorders, alexithymia and socio-emotional alienation in patients with HIV-1 infection. Infez Med. 2014;22:193–9. [PubMed] [Google Scholar]
- 4.Hays RB, Turner H, Coates TJ. Social support, AIDS-related symptoms, and depression among gay men. J Consult Clin Psychol. 1992;60:463–9. doi: 10.1037//0022-006x.60.3.463. [DOI] [PubMed] [Google Scholar]
- 5.Wagner GJ, Rabkin JG, Rabkin R. A comparative analysis of standard and alternative antidepressants in the treatment of human immunodeficiency virus patients. Compr Psychiatry. 1996;37:402–8. doi: 10.1016/s0010-440x(96)90023-1. [DOI] [PubMed] [Google Scholar]
- 6.Bogart LM, Catz SL, Kelly JA, Gray-Bernhardt ML, Hartmann BR, Otto-Salaj LL, et al. Psychosocial issues in the era of new AIDS treatments from the perspective of persons living with HIV. J Health Psychol. 2000;5:500–16. doi: 10.1177/135910530000500408. [DOI] [PubMed] [Google Scholar]
- 7.Blashill AJ, Bedoya CA, Mayer KH, O’Cleirigh C, Pinkston MM, Remmert JE, et al. Psychosocial syndemics are additively associated with worse ART adherence in HIV-infected individuals. AIDS Behav. 2015;19:981–6. doi: 10.1007/s10461-014-0925-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Attonito J, Dévieux JG, Lerner BD, Hospital MM, Rosenberg R. Antiretroviral treatment adherence as a mediating factor between psychosocial variables and HIV viral load. J Assoc Nurses AIDS Care. 2014;25:626–37. doi: 10.1016/j.jana.2014.08.001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Mulkins AL, Ibáñez-Carrasco F, Boyack D, Verhoef MJ. The living well lab: A community-based HIV/AIDS research initiative. J Complement Integr Med. 2014;11:213–22. doi: 10.1515/jcim-2013-0057. [DOI] [PubMed] [Google Scholar]
- 10.Cramer H, Lauche R, Langhorst J, Dobos G. Yoga for depression: A systematic review and meta-analysis. Depress Anxiety. 2013;30:1068–83. doi: 10.1002/da.22166. [DOI] [PubMed] [Google Scholar]
- 11.Shapiro D, Cook IA, Dmitry M, Davydov, Ottaviani C, Leuchter AF, et al. Yoga as a complementary treatment of depression: Effects of traits and moods on treatment outcome. Evid Based Complement Alternat Med. 2007;4:493–502. doi: 10.1093/ecam/nel114. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Cheema BS, Marshall PW, Chang D, Colagiuri B, Machliss B. Effect of an office worksite-based Yoga program on heart rate variability: A randomized controlled trial. BMC Public Health. 2012;11:578. doi: 10.1186/1471-2458-11-578. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Uebelacker LA, Epstein-Lubow G, Gaudiano BA, Tremont G, Battle CL, Miller IW. Hatha Yoga for depression: Critical review of the evidence for efficacy, plausible mechanisms of action, and directions for future research. J Psychiatr Pract. 2010;16:22–33. doi: 10.1097/01.pra.0000367775.88388.96. [DOI] [PubMed] [Google Scholar]
- 14.Gopal A, Mondal S, Gandhi A, Arora S, Bhattacharjee J. Effect of integrated Yoga practices on immune responses in examination stress – A preliminary study. Int J Yoga. 2011;4:26–32. doi: 10.4103/0973-6131.78178. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Kumar K, Pandya P. A study on the impact on ESR level through Yogic relaxation technique Yoganidra. Indian J Tradit Knowl. 2012;11:358–61. [Google Scholar]
- 16.Rao RM, Telles S, Nagendra HR, Nagarathna R, Gopinath K, Srinath S, et al. Effects of Yoga on natural killer cell counts in early breast cancer patients undergoing conventional treatment. Comment to: Recreational music-making modulates natural killer cell activity, cytokines, and mood states in corporate employees Masatada Wachi, Masahro Koyama, Masanori Utsuyama, Barry B. Bittman, Masanobu Kitagawa, Katsuiku Hirokawa Med Sci Monit. 2007;13:CR57–70. Med Sci Monit 2008;14:LE3-4. [PubMed] [Google Scholar]
- 17.Visweswaraiah NK, Telles S. Randomized trial of Yoga as a complementary therapy for pulmonary tuberculosis. Respirology. 2004;9:96–101. doi: 10.1111/j.1440-1843.2003.00528.x. [DOI] [PubMed] [Google Scholar]
- 18.Pilkington K, Kirkwood G, Rampes H, Richardson J. Yoga for depression: The research evidence. J Affect Disord. 2005;89:13–24. doi: 10.1016/j.jad.2005.08.013. [DOI] [PubMed] [Google Scholar]
- 19.Cade WT, Reeds DN, Mondy KE, Overton ET, Grassino J, Tucker S, et al. Yoga lifestyle intervention reduces blood pressure in HIV-infected adults with cardiovascular disease risk factors. HIV Med. 2010;11:379–88. doi: 10.1111/j.1468-1293.2009.00801.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Koar WH. Meditation, T-cells, anxiety, depression and HIV infection. Subtle Energies Energy Med J Arch. 1995;6:91–7. [Google Scholar]
- 21.Available from: https://www.randomizer.org/ . [Last accessed on 2014 Jan].
- 22.Bhargav H, Raghuram N, Rao NH, Tekur P, Koka PS. Potential Yoga modules for treatment of hematopoietic inhibition in HIV-1 infection. J Stem Cells. 2009;5:129–48. [PubMed] [Google Scholar]
- 23.Bjelland I, Dahl AA, Haug TT, Neckelmann D. The validity of the hospital anxiety and depression scale. An updated literature review. J Psychosom Res. 2002;52:69–77. doi: 10.1016/s0022-3999(01)00296-3. [DOI] [PubMed] [Google Scholar]
- 24.Kandathil AJ, Kannangai R, David S, Nithyanandam G, Solomon S, Balakrishnan P, et al. Comparison of microcapillary cytometry technology and flow cytometry for CD4+ and CD8+ T-cell estimation. Clin Diagn Lab Immunol. 2005;12:1006–9. doi: 10.1128/CDLI.12.8.1006-1009.2005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Taylor DN. Effects of a behavioral stress-management program on anxiety, mood, self-esteem, and T-cell count in HIV positive men. Psychol Rep. 1995;76:451–7. doi: 10.2466/pr0.1995.76.2.451. [DOI] [PubMed] [Google Scholar]
- 26.Hammen C. Stress and depression. Annu Rev Clin Psychol. 2005;1:293–319. doi: 10.1146/annurev.clinpsy.1.102803.143938. [DOI] [PubMed] [Google Scholar]
- 27.Antoni MH, Schneiderman N, Fletcher MA, Goldstein DA, Ironson G, Laperriere A. Psychoneuroimmunology and HIV-1. J Consult Clin Psychol. 1990;58:38–49. doi: 10.1037//0022-006x.58.1.38. [DOI] [PubMed] [Google Scholar]
- 28.Frank MK, Rebecca BL, Susan M, David WP, Winnie BK. Depression and CD4 cell count among persons with HIV-1 infect Uganda. AIDS Behav. 2006;10:105–11. doi: 10.1007/s10461-006-9142-2. [DOI] [PubMed] [Google Scholar]
- 29.Ickovics J, Hamburger M, Vlahov D, Schoenbaum E, Schuman P, Boland R, et al. Mortality CD4 cell count decline and depressive symptoms among HIV-1 – Seropositive women: Longitudinal analysis from HIV-1 epidemiology research study. JAMA. 2001;285:1460–5. doi: 10.1001/jama.285.11.1466. [DOI] [PubMed] [Google Scholar]