

Abstract
Default from tuberculosis (TB) treatment could exacerbate the disease and result in the emergence of drug resistance. This study identified the risk factors for default from TB treatment in Korea. This single-center case–control study analyzed 46 default cases and 100 controls. Default was defined as interrupting treatment for 2 or more consecutive months. The reasons for default were mainly incorrect perception or information about TB (41.3%) and experience of adverse events due to TB drugs (41.3%). In univariate analysis, low income (< 2,000 US dollars/month, 88.1% vs. 68.4%, P = 0.015), absence of TB stigma (4.3% vs. 61.3%, P < 0.001), treatment by a non-pulmonologist (74.1% vs. 25.9%, P < 0.001), history of previous treatment (37.0% vs. 19.0%, P = 0.019), former defaulter (15.2% vs. 2.0%, P = 0.005), and combined extrapulmonary TB (54.3% vs. 34.0%, P = 0.020) were significant risk factors for default. In multivariate analysis, the absence of TB stigma (adjusted odd ratio [aOR]: 46.299, 95% confidence interval [CI]: 8.078–265.365, P < 0.001), treatment by a non-pulmonologist (aOR: 14.567, 95% CI: 3.260–65.089, P < 0.001), former defaulters (aOR: 33.226, 95% CI: 2.658–415.309, P = 0.007), and low income (aOR: 5.246, 95% CI: 1.249–22.029, P = 0.024) were independent predictors of default from TB treatment. In conclusion, patients with absence of disease stigma, treated by a non-pulmonologist, who were former defaulters, and with low income should be carefully monitored during TB treatment in Korea to avoid treatment default.
Keywords: Lost to Follow up, Tuberculosis, Chemotherapy, Risk Factors
Graphical Abstract
INTRODUCTION
Standard tuberculosis (TB) treatment is highly efficacious, but curing TB requires a long treatment duration and many drugs (1), which may lead to non-adherence to a full course of anti-TB treatment. The WHO 2013 revised definitions and reporting defines default from TB treatment as “lost to follow-up,” i.e., a TB patient who did not start treatment or whose treatment was interrupted for 2 consecutive months or more (2). Defaulted patients have higher risks of a second default, multidrug-resistant TB development, and mortality (3,4,5). Patients who default in high-burden settings also have a higher rate of subsequent smear-positive TB, suggesting a high risk of transmission to other persons (6). Therefore, knowing the risk factors for default is important for the effectiveness of TB control program.
Risk factors for treatment discontinuation have been widely investigated, especially in countries where human immunodeficiency virus is endemic and developing countries (7,8,9,10,11,12). In contrast to most developed countries, which have low incidences of TB, new cases in Korea have plateaued at approximately 100 per 100,000 persons over the past decade (13). Thus, TB remains a major health concern and incurs a large burden on public health despite the well-appointed medical delivery system in Korea. Therefore, this study investigated the individual sociodemographic and clinical characteristics of defaulted patients and identified the risk factors associated with default from TB treatment.
MATERIALS AND METHODS
Study subjects
This single-center case–control study retrospectively reviewed the data of 2,072 patients aged more than 18 years who were registered and treated for pulmonary TB or extrapulmonary TB (EPTB) at Chonnam National University Hospital from January 2010 to December 2014. TB was diagnosed on the basis of Mycobacterium tuberculosis identification by culture or polymerase chain reaction (PCR) from clinical specimens or clinical, radiological, or histological findings compatible with TB and responses to TB treatment. All TB patients received TB health education as well as monitoring for drug compliance and adverse drug reactions during treatment by specially trained nurses who participated in the Public–Private Mix (PPM) project for TB control in Korea.
TB drugs were self-administered with the support of trained PPM nurses during treatment. At each clinical visit, treatment adherence was assessed by asking patients about their drug intake and checking the remnant tablets of the previously prescribed regimen.
Data collection and definitions
Once TB was diagnosed at our institute or a TB patient was transferred from another clinic, the patient was enrolled in the national TB registry. Physicians reported the patients’ data to the registry, and PPM nurses entered the data into registry database and updated it as necessary. The following patient information was obtained through electronic medical records: baseline clinical data, comorbidities, history and outcome of previous TB treatment, radiologic findings at diagnosis, microbiological characteristics at diagnosis (acid-fast bacilli stain, mycobacterial culture, and PCR in clinical specimens; drug resistance; and culture conversion after treatment), and side effects during TB treatment. Employment was categorized as “regular” if the patient was employed in a year-round position or was a full-time student and “irregular or unemployed” if the patient had a seasonal or day-labor position (12). Education was classified into three groups according to the highest level the patient completed: elementary school, middle or high school, and college or university education was classified as primary, secondary, and post-secondary, respectively. Income was categorized on the basis of the average monthly income of the patient or their household in Korea with reference to national statistics (Korean Statistical Information Service, http://kosis.kr) according to a cut-off corresponding to the fourth quartile. Health insurance was categorized into two groups on the basis of qualification for national health insurance. Public assistance was applicable to people who were unable to support their family. In underlying diseases, chronic pulmonary disease was defined as a non-infectious chronic pulmonary disease such as chronic obstructive pulmonary disease and asthma. Chronic kidney disease was defined as a disease causing a progressive loss in renal function. Chronic cardiac disease was defined as a disease which needed a long term use of cardiac medications such as coronary artery disease, valvular heart disease, cardiomyopathy, and cardiac arrhythmias. Chronic liver disease was defined as a disease casing progressive destruction and regeneration of liver parenchyma such as chronic viral hepatitis, alcoholic liver disease, and liver cirrhosis.
Patients were classified into two groups according to treatment outcome (2). The case group comprised defaulters, i.e., TB patients who did not start treatment or whose treatment was interrupted for 2 consecutive months or more. Meanwhile, the control group comprised non-defaulters who had been cured or completed treatment. Patients with TB-related death or those who were transferred out were excluded from the control group.
To track defaulters, PPM nurses tried to contact all of the listed patients by telephone and ascertained individual clinical and socioeconomic data. For non-defaulters, the data were obtained by one or two in-person interviews by PPM nurses during follow-up at the outpatient department. Questionnaires were administered to collect information about personal details, disease perception (i.e., TB), and causes of default. The questions were selected from among several factors found to be significantly associated with default in previous studies (7,8,9,10,12). Disease stigma was defined as feeling ashamed to have TB, trying to hide from or disclose to others, or attempting to be isolated (8,9). Incorrect perception or information about the disease was defined as a patient’s lack of adequate knowledge and education about TB or their recent disease status, such as the efficacy of anti-TB treatment, possibility of feeling better or being cured, and treatment duration (7,8). A low level of satisfaction with the clinic or doctors reflected poor healthcare worker attitude towards patients, long waiting times at the clinic, or lack of opportunity to express feelings (8,10).
Statistical analysis
All data are expressed as median (interquartile range [IQR]) or numbers and percentages. Intergroup comparisons were performed using the Mann–Whitney U-test for continuous variables, and Pearson’s χ 2 test or Fisher’s exact test for categorical variables. We evaluated trends using the χ 2 test for trends. Multivariate analysis was performed to determine the predictors of default from TB treatment. Possible predictors found to be significant in univariate analysis were entered into binary logistic regression. The level of significance was set at P < 0.05.
We planned a study of independent cases and controls with two controls per case. Data of the entire population with TB at our clinic indicate the probability of default (i.e., default rate) was 0.049. If the true odds ratio for disease in exposed subjects relative to unexposed subjects is 5, we would need to study 49 case patients and 98 control patients to be able to reject the null hypothesis that this odds ratio equals 1 with a probability (i.e., power) of 0.8. We tried to contact all 102 defaulted patients using telephone, but we could connect 58 patients. Of these patients, 46 patients agreed to telephone interview. Ultimately, we recruited 46 cases and randomly selected 100 controls who were eligible for personal interview and regularly followed up. The type I error probability associated with this test of this null hypothesis is 0.05.
Ethics statement
Permission to review and publish patient records was obtained from the institutional review board of Chonnam National University Hospital (IRB No. CNUH-2014-260). Informed consent was obtained from patients personally, and confidentiality and anonymity were assured. In cases of defaulters who would not or could not visit the hospital, assistants asked for consent to participate in this study by telephone.
RESULTS
Patient characteristics
Among 2,072 patients with TB treated at Chonnam National University Hospital from January 2010 to December 2014, 102 were defaulted from treatment, giving a default rate of 4.9%. Among them, 46 defaulters were assigned to the case group, and 100 patients were randomly selected as controls.
Regarding sociodemographic characteristics, a larger proportion of defaulters had low income (< 2,000 US dollars per month) than controls. Other factors such as body mass index, smoking, alcohol, employment, marriage, education, insurance, and hospital accessibility did not differ significantly between groups (Table 1).
Table 1. Sociodemographic characteristics of the control and default groups.
| Characteristics | Total (n = 146) |
Control (n = 100) |
Default (n = 46) |
P value |
|---|---|---|---|---|
| Age, yr | 52.5 (31.0-70.0) | 53.5 (31.0-70.5) | 52.0 (30.0-69.0) | 0.745 |
| Sex | 0.643 | |||
| Female | 58 (39.7) | 41 (41.0) | 17 (37.0) | |
| Male | 88 (60.3) | 59 (59.0) | 29 (63.0) | |
| BMI, kg/m2 | 21.0 (19.5-23.2) | 20.4 (19.2-22.3) | 21.9 (20.3-24.5) | 0.062 |
| < 18.5 | 17 (11.6) | 15 (15.0) | 2 (4.3) | |
| ≥ 18.5 | 130 (88.4) | 85 (85.0) | 44 (95.7) | |
| Smoking | 0.086 | |||
| Never smoker | 66 (45.2) | 50 (50.0) | 16 (34.8) | |
| Ever smoker | 80 (54.8) | 50 (50.0) | 30 (65.2) | |
| Alcohol consumption | 0.219 | |||
| No | 90 (61.6) | 65 (65.0) | 25 (54.3) | |
| Yes | 56 (38.4) | 35 (35.0) | 21 (45.7) | |
| Herbal medication | 9 (6.2) | 6 (6.0) | 3 (6.5) | 1.000 |
| Employment | 0.245 | |||
| Regular | 69 (47.3) | 44 (44.0) | 25 (54.3) | |
| Irregular or unemployed | 77 (52.7) | 56 (56.0) | 21 (45.7) | |
| Marriage | 0.640 | |||
| Married | 96 (65.8) | 67 (67.0) | 29 (63.0) | |
| Single/divorced/bereaved | 50 (34.2) | 33 (33.0) | 17 (37.0) | |
| Family members | 0.951 | |||
| Living together | 117 (80.1) | 80 (80.0) | 37 (80.4) | |
| Living alone | 29 (19.9) | 20 (20.0) | 9 (19.6) | |
| Education | 144 | 98 | 46 | 0.673 |
| Primary | 45 (31.3) | 32 (32.7) | 13 (28.3) | |
| Secondary | 20 (13.9) | 12 (12.2) | 8 (17.4) | |
| Post-secondary | 79 (54.9) | 54 (55.1) | 25 (54.3) | |
| Income/month | 137 | 95 | 42 | 0.015 |
| < 2,000 US dollars | 102 (74.5) | 65 (68.4) | 37 (88.1) | |
| ≥ 2,000 US dollars | 35 (25.5) | 30 (31.6) | 5 (11.9) | |
| Insurance | 0.549 | |||
| National health insurance | 132 (90.4) | 89 (89.0) | 43 (93.5) | |
| Public assistance | 14 (9.6) | 11 (11.0) | 3 (6.5) | |
| Distance from home to clinic, km | 24.3 (7.6-85.3) | 25.2 (11.2-88.0) | 20.4 (6.5-75.3) | 0.190 |
| < 50 | 85 (58.2) | 57 (57.0) | 28 (60.9) | 0.258 |
| 50-100 | 38 (26.0) | 24 (24.0) | 14 (30.4) | |
| > 100 | 23 (15.8) | 19 (19.0) | 4 (8.7) |
Values are expressed as median (interquartile range) or number of patients (%). BMI, Body mass index.
The median (IQR) time from treatment initiation to default was 101 (35–185) days. Regarding clinical characteristics, patients treated by a non-pulmonologist and patients with EPTB had a significantly higher default rate. Patients with a history of treatment for TB or former default also had a significantly higher default rate (Table 2). Adverse drug reactions predominantly affected the skin (e.g., pruritus, rash, and acne) and gastrointestinal system (e.g., nausea, vomiting, and anorexia). However, there were no differences in adverse drug reactions between groups (Table 3).
Table 2. Clinical and microbiologic characteristics of the control and default groups.
| Parameters | Total (n = 146) |
Control (n = 100) |
Default (n = 46) |
P value |
|---|---|---|---|---|
| Attending physician | < 0.001 | |||
| Non-pulmonologist | 27 (18.5) | 7 (7.0) | 20 (43.5) | |
| Pulmonologist | 119 (81.5) | 93 (93.0) | 26 (56.5) | |
| Underlying diseases | ||||
| Diabetes | 21 (14.4) | 12 (12.0) | 9 (19.6) | 0.226 |
| Chronic liver disease | 17 (11.6) | 12 (12.0) | 5 (10.9) | 0.843 |
| Chronic cardiac disease | 27 (18.5) | 17 (17.0) | 10 (21.7) | 0.493 |
| Chronic kidney disease | 3 (2.1) | 2 (2.0) | 1 (2.2) | 1.000 |
| Cerebrovascular disease | 10 (6.8) | 6 (6.0) | 4 (8.7) | 0.725 |
| Malignancy | 8 (5.5) | 5 (5.0) | 3 (6.5) | 0.707 |
| Chronic pulmonary disease | 10 (6.8) | 5 (5.0) | 5 (10.9) | 0.288 |
| Psychological disorder | 2 (1.4) | 1 (1.0) | 1 (2.2) | 0.532 |
| Previous treatment | 36 (24.7) | 19 (19.0) | 17 (37.0) | 0.019 |
| Number of treatments | 1.0 (1.0-1.0) | 1.0 (1.0-1.0) | 1.0 (1.0-1.0) | 0.071 |
| Duration, months | 6.0 (3.5-8.5) | 6.0 (5.0-9.5) | 6.0 (2.0-8.0) | 0.126 |
| Former defaulter | 9 (6.2) | 2 (2.0) | 7 (15.2) | 0.005 |
| EPTB | ||||
| Combined | 59 (40.4) | 34 (34.0) | 25 (54.3) | 0.020 |
| Alone | 25 (17.1) | 6 (6.0) | 19 (41.3) | < 0.001 |
| Radiologic findings | 145 | 100 | 45 | |
| Cavity | 28 (19.3) | 19 (19.0) | 9 (20.0) | 0.888 |
| Extent | 123 | 94 | 29 | 0.559 |
| Localized | 90 (73.2) | 70 (74.5) | 20 (69.0) | |
| Bilateral disease | 33 (26.8) | 24 (25.5) | 9 (31.0) | |
| AFB smear | 137 | 100 | 37 | 0.163 |
| Positive | 42 (30.7) | 34 (34.0) | 8 (21.6) | |
| Negative | 95 (69.3) | 66 (66.0) | 29 (78.4) | |
| AFB culture | 134 | 96 | 38 | 0.085 |
| Positive | 89 (66.4) | 68 (70.8) | 21 (55.3) | |
| Negative | 45 (33.6) | 28 (29.2) | 17 (44.7) |
Values are expressed as median (interquartile range) or number of patients (%). AFB, acid-fast bacilli; EPTB, extrapulmonary tuberculosis.
Table 3. Drug resistance, therapeutic characteristics, adverse drug reactions, and perceptions of disease in the control and default groups.
| Variables | Total (n = 146) |
Control (n = 100) |
Default (n = 46) |
P value |
|---|---|---|---|---|
| Resistance | 90 | 75 | 15 | |
| Susceptible | 71 (78.9) | 58 (77.3) | 13 (86.7) | 1.000 |
| Non-MDR drug resistance | 9 (10.0) | 8 (10.7) | 1 (6.7) | |
| MDR | 10 (11.1) | 9 (12.0) | 1 (6.7) | |
| Admission during intensive treatment phase | 70 (47.9) | 52 (52.0) | 18 (39.1) | 0.148 |
| Regimen | 0.371 | |||
| With pyrazinamide | 132 (90.4) | 92 (92.0) | 40 (87.0) | |
| Without pyrazinamide | 14 (9.6) | 8 (8.0) | 6 (13.0) | |
| Improvement of symptoms after treatment | 137 | 98 | 39 | |
| Improved | 96 (70.1) | 71 (72.4) | 25 (64.1) | 0.336 |
| Not improved | 41 (29.9) | 27 (27.6) | 14 (35.9) | |
| Adverse drug reactions | 144 | 100 | 44 | |
| Present | 82 (56.9) | 58 (58.0) | 24 (54.5) | 0.700 |
| Gastrointestinal | 39 (27.3) | 28 (28.0) | 11 (25.0) | 0.766 |
| Liver | 19 (13.2) | 13 (13.0) | 6 (13.6) | 0.917 |
| Skin | 41 (28.5) | 30 (30.0) | 11 (25.0) | 0.540 |
| Optic | 8 (5.6) | 8 (8.0) | 0 (0.0) | 0.106 |
| Joint | 9 (6.3) | 7 (7.0) | 2 (4.5) | 0.722 |
| Drug fever | 5 (3.5) | 2 (2.0) | 3 (6.8) | 0.167 |
| Peripheral neuropathy | 9 (6.3) | 7 (7.0) | 2 (4.5) | 0.722 |
| Others* | 7 (4.9) | 6 (6.0) | 1 (2.3) | |
| Disease perception | 139 | 93 | 46 | |
| Disease stigma | 59 (42.4) | 57 (61.3) | 2 (4.3) | < 0.001 |
| Incorrect perception or information | 61 (43.9) | 42 (45.2) | 19 (41.3) | 0.666 |
Values are expressed as median (interquartile range) or number of patients (%). MDR, multidrug resistant.
*Includes headache (n = 3), dizziness (n = 2), tinnitus (n = 1), and cytopenia (n = 1).
The results regarding disease perception are shown in Table 3. Interestingly, most defaulters did not feel stigma about their disease, whereas more than half of non-defaulters did.
The most common cause of treatment default according to patients’ personal opinions was incorrect perception or information about their disease (19/46, 41.3%) and side effects of anti-TB treatment (19/46, 41.3%). Poor treatment tolerability such as work interference with adherence or unwillingness to taking medicine (12/46, 26.1%) and low level of satisfaction with the clinic or doctors (5/46, 10.9%) were less common reasons.
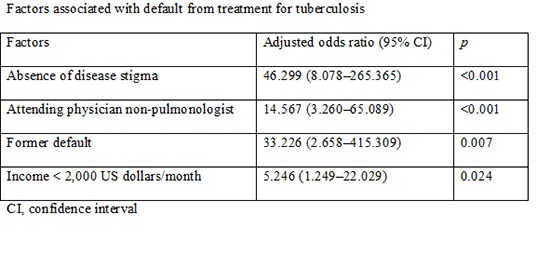
Predictors of treatment default
Significant risk factors for default in univariate analysis, including low income (< 2,000 US dollars/month), treatment by a non-pulmonologist, history of previous treatment, former default, combined EPTB, and absence of TB stigma, were included in multivariate analysis. In multivariate analysis, low income (adjusted odd ratio [aOR]: 5.246, 95% confidence interval [CI]: 1.249–22.029, P = 0.024), treatment by a non-pulmonologist (aOR: 14.567, 95% CI: 3.260–65.089, P < 0.001), former defaulters (aOR: 33.226, 95% CI: 2.658–415.309, P = 0.007), and absence of TB stigma (aOR: 46.299, 95% CI: 8.078–265.365, P < 0.001) were independent predictors of default from TB treatment.
DISCUSSION
This is the first study to evaluate the predictors of default from TB treatment in Korea, which is a high-income country with an intermediate TB incidence. The default rate during TB treatment varies with respect to the condition of enrolled patients, treatment, healthcare system, patients’ knowledge and attitude about TB, and socioeconomic status (9,10). The default rate in the present study was 4.9%, which is lower than that in a previous study in Korea (7.3%) (14); however, that study was performed in 2008, before the implementation of the PPM project in Korea. The PPM project, which started in 2009, has increased the treatment success rate and decreased losses to follow-up (15,16). All patients in the present study received TB health education and monitoring by specially trained nurses participating in the PPM project, which might have reduced the default rate. Since starting the PPM project at our institute in 2010, the default rate has decreased significantly from 6.2% in 2010 to 2.9% in 2014 (Ptrend = 0.003), which might be due to greater nurses’ experience with proper education and monitoring of TB patients.
Regarding the timing of default, our finding that the median time from treatment start to default was 101 days is consistent with previous studies including a systematic review reporting that the majority of defaulters completed the two-month intensive phase of treatment (17). This might be related to rapid symptom improvement after starting TB treatment. In the present study, more than half of patients who defaulted had experienced symptom improvement when they defaulted and there was no difference between the default and control groups with respect to the rate of symptom improvement, even after treatment completion in the control group.
Higher default rates and worse outcomes in patients with low income have been reported in previous study (7). The present study also shows that a larger proportion of defaulters had lower income than controls. Nevertheless, more than two thirds of controls patients had a low income < 2,000 US dollars per month. Therefore, the results not only demonstrate the importance of economic status in default from TB treatment, but also the overall poor economic status of TB patients in Korea.
Interestingly, TB treatment by a non-pulmonologist was an independent predictor of default. Accordingly, medical personnel who have low motivation to treat TB patients might increase the default rate (11). Pulmonologists might communicate with patients more effectively, which could decrease the default rate. Another possible explanation for this finding is that in Korea including our institute, there has been trend of treating patients with EPTB by non-pulmonologists and with pulmonary TB by pulmonologists, respectively. The diagnosis of EPTB can be elusive, requiring a high index of suspicion. Moreover, cases have a low probability of culturing M. tuberculosis. Furthermore, the standards for the assessment of therapeutic response tend to be uncertain. All of these factors might increase the risk of default in patients with EPTB. In the present study, patients with EPTB had a higher default rate than patients with pulmonary TB in univariate analysis, although this association lost statistical significance in multivariate analysis.
Former default status was an independent predictor of default in the present study, which has also been reported in previous studies in different settings (7,8). Therefore, history of TB treatment and treatment outcome could be important when determining patients’ risk of default from TB treatment.
TB stigma is reported to delay TB diagnosis and decrease treatment compliance. Furthermore, disease stigma is reported to be a risk factor for default (8,18). In contrast, some studies report that TB stigma is a predictor of treatment adherence, and TB patients who were ashamed of TB contacted healthcare facilities early (9,19). In the present study, absence of disease stigma was an independent predictor of treatment default; therefore, TB stigma might motivate patients to receive TB treatment, thus increasing adherence to TB treatment.
The predominant causes of default were incorrect perception or information about TB and experience of adverse events due to TB drugs. Concordantly, studies in other countries report similar causes of default despite socioeconomic and cultural differences (7,8) as well as in drug-resistant TB patients (20). One study reports the reasons for completing treatment include desire to be cured (93%), doctor’s advice to complete treatment (41%), not wanting to transmit TB to others (24%), and fear for one’s health (20%) (21). Therefore, patients’ better awareness and fewer misconceptions about TB could decrease the default rate. Education about TB should be tailored to individual patients’ needs and continued throughout the course of treatment in combination with awareness and monitoring of the side effects of drugs.
This study has several limitations that should be mentioned. First, this study was performed in a single center in Korea, which may limit the generalizability of our findings to other countries and different settings. Second, we could not investigate all 102 defaulters; we only enrolled the 46 patients available for interviews. Therefore, this may have caused a selection bias in the case group. Third, only questionnaires filled in by patients and not physicians were used in the assessment of causes of default; this might influence the objectivity of reasons for default and might have resulted in other causes linked with important clinical manifestations being overlooked.
In summary, TB patients with absence of disease stigma, being treated by a non-pulmonologist, who have previously defaulted, and have low income should be carefully monitored during TB treatment in Korea in order to avoid treatment default. Health departments should develop effective measures to prevent treatment default in order to ensure therapy completion and improve treatment outcomes.
Footnotes
Funding: This study was supported by a grant (CRI14039-21) from Chonnam National University Hospital.
DISCLOSURE: All authors declare that they have no competing interests.
AUTHOR CONTRIBUTION: Guarantor of integrity of entire study: Kwon YS. Study concept and design: Kwon YS, Park CK. Data acquisition: all authors. Data analysis and interpretation: all authors. Manuscript drafting or revision for important intellectual content: all authors. Manuscript final version approval: all authors. Literature research, Kwon YS, Park CK. Clinical studies: all authors. Statistical analysis: Kwon YS, Park CK, Shin HJ, Kim YI, Lim SC, Kim JC. Manuscript editing: Kwon YS.
References
- 1.Kwon YS, Jeong BH, Koh WJ. Tuberculosis: clinical trials and new drug regimens. Curr Opin Pulm Med. 2014;20:280–286. doi: 10.1097/MCP.0000000000000045. [DOI] [PubMed] [Google Scholar]
- 2.World Health Organization. Definitions and reporting framework for tuberculosis-2013 revision. WHO/HTM/TB/2013.2. Geneva: World Health Organization; 2013. Available at http://apps.who.int/iris/bitstream/10665/79199/1/9789241505345_eng.pdf. [Google Scholar]
- 3.Ottmani SE, Zignol M, Bencheikh N, Laâsri L, Chaouki N, Mahjour J. Results of cohort analysis by category of tuberculosis retreatment cases in Morocco from 1996 to 2003. Int J Tuberc Lung Dis. 2006;10:1367–1372. [PubMed] [Google Scholar]
- 4.Gler MT, Macalintal LE, Raymond L, Guilatco R, Quelapio MI, Tupasi TE. Multidrug-resistant tuberculosis among previously treated patients in the Philippines. Int J Tuberc Lung Dis. 2011;15:652–656. doi: 10.5588/ijtld.10.0400. [DOI] [PubMed] [Google Scholar]
- 5.Kolappan C, Sr, Subramani R, Kumaraswami V, Santha T, Narayanan PR. Excess mortality and risk factors for mortality among a cohort of TB patients from rural South India. Int J Tuberc Lung Dis. 2008;12:81–86. [PubMed] [Google Scholar]
- 6.Marx FM, Dunbar R, Enarson DA, Beyers N. The rate of sputum smear-positive tuberculosis after treatment default in a high-burden setting: a retrospective cohort study. PLoS One. 2012;7:e45724. doi: 10.1371/journal.pone.0045724. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Muture BN, Keraka MN, Kimuu PK, Kabiru EW, Ombeka VO, Oguya F. Factors associated with default from treatment among tuberculosis patients in Nairobi province, Kenya: a case control study. BMC Public Health. 2011;11:696. doi: 10.1186/1471-2458-11-696. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Finlay A, Lancaster J, Holtz TH, Weyer K, Miranda A, van der Walt M. Patient- and provider-level risk factors associated with default from tuberculosis treatment, South Africa, 2002: a case-control study. BMC Public Health. 2012;12:56. doi: 10.1186/1471-2458-12-56. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Bhardwaj AK, Kashyap S. Factors influencing early health facility contact and low default rate among new sputum smear positive tuberculosis patients, India. Pulm Med. 2014;2014:132047. doi: 10.1155/2014/132047. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Rutherford ME, Hill PC, Maharani W, Sampurno H, Ruslami R. Risk factors for treatment default among adult tuberculosis patients in Indonesia. Int J Tuberc Lung Dis. 2013;17:1304–1309. doi: 10.5588/ijtld.13.0084. [DOI] [PubMed] [Google Scholar]
- 11.Kizub D, Ghali I, Sabouni R, Bourkadi JE, Bennani K, El Aouad R, Dooley KE. Qualitative study of perceived causes of tuberculosis treatment default among health care workers in Morocco. Int J Tuberc Lung Dis. 2012;16:1214–1220. doi: 10.5588/ijtld.11.0626. [DOI] [PubMed] [Google Scholar]
- 12.Kendall EA, Theron D, Franke MF, van Helden P, Victor TC, Murray MB, Warren RM, Jacobson KR. Alcohol, hospital discharge, and socioeconomic risk factors for default from multidrug resistant tuberculosis treatment in rural South Africa: a retrospective cohort study. PLoS One. 2013;8:e83480. doi: 10.1371/journal.pone.0083480. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Park YK, Park YS, Na KI, Cho EH, Shin SS, Kim HJ. Increased tuberculosis burden due to demographic transition in Korea from 2001 to 2010. Tuberc Respir Dis (Seoul) 2013;74:104–110. doi: 10.4046/trd.2013.74.3.104. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Park YS, Hong SJ, Boo YK, Hwang ES, Kim HJ, Cho SH, Na KI, Cho EH, Shin SS. The national status of tuberculosis using nationwide medical records survey of patients with tuberculosis in Korea. Tuberc Respir Dis (Seoul) 2012;73:48–55. doi: 10.4046/trd.2012.73.1.48. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Park JS. Increasing the treatment success rate of tuberculosis in a private hospital through Public-Private Mix (PPM) project. Tuberc Respir Dis (Seoul) 2011;70:143–149. [Google Scholar]
- 16.Kim HJ, Bai GH, Kang MK, Kim SJ, Lee JK, Cho SI, Lew WJ. A public-private collaboration model for treatment intervention to improve outcomes in patients with tuberculosis in the private sector. Tuberc Respir Dis (Seoul) 2009;66:349–357. [Google Scholar]
- 17.Kruk ME, Schwalbe NR, Aguiar CA. Timing of default from tuberculosis treatment: a systematic review. Trop Med Int Health. 2008;13:703–712. doi: 10.1111/j.1365-3156.2008.02042.x. [DOI] [PubMed] [Google Scholar]
- 18.Courtwright A, Turner AN. Tuberculosis and stigmatization: pathways and interventions. Public Health Rep. 2010;125(Suppl 4):34–42. doi: 10.1177/00333549101250S407. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Woith WM, Larson JL. Delay in seeking treatment and adherence to tuberculosis medications in Russia: a survey of patients from two clinics. Int J Nurs Stud. 2008;45:1163–1174. doi: 10.1016/j.ijnurstu.2007.07.014. [DOI] [PubMed] [Google Scholar]
- 20.Sanchez-Padilla E, Marquer C, Kalon S, Qayyum S, Hayrapetyan A, Varaine F, Bastard M, Bonnet M. Reasons for defaulting from drug-resistant tuberculosis treatment in Armenia: a quantitative and qualitative study. Int J Tuberc Lung Dis. 2014;18:160–167. doi: 10.5588/ijtld.13.0369. [DOI] [PubMed] [Google Scholar]
- 21.Cherkaoui I, Sabouni R, Ghali I, Kizub D, Billioux AC, Bennani K, Bourkadi JE, Benmamoun A, Lahlou O, Aouad RE, et al. Treatment default amongst patients with tuberculosis in urban Morocco: predicting and explaining default and post-default sputum smear and drug susceptibility results. PLoS One. 2014;9:e93574. doi: 10.1371/journal.pone.0093574. [DOI] [PMC free article] [PubMed] [Google Scholar]