

Abstract
Background
Optic neuritis is an inflammatory disease of the optic nerve. It usually presents with an abrupt loss of vision and recovery of vision is almost never complete. It occurs more commonly in women than in men. Closely linked in pathogenesis, optic neuritis may be the initial manifestation for multiple sclerosis. In some people, no underlying cause can be found.
Objectives
The objective of this review was to assess the effects of corticosteroids on visual recovery in eyes with acute optic neuritis.
Search methods
We searched CENTRAL (which contains the Cochrane Eyes and Vision Group Trials Register) (The Cochrane Library 2015, Issue 4), MEDLINE (January 1950 to April 2015), EMBASE (January 1980 to April 2015), Latin American and Caribbean Health Sciences Literature (LILACS) (January 1982 to April 2015), PubMed (January 1946 to April 2015), the metaRegister of Controlled Trials (mRCT) (www.controlled-trials.com), ClinicalTrials.gov (www.clinicaltrials.gov), and the World Health Organization (WHO) International Clinical Trials Registry Platform (ICTRP) (www.who.int/ictrp/search/en). There were no date or language restrictions in the electronic searches for trials. The metaRegister of Controlled Trials (mRCT) was last searched on 6 March 2014. The electronic databases were last searched on 7 April 2015. We also searched reference lists of identified trial reports for additional trials.
Selection criteria
We included randomized controlled trials (RCTs) that evaluated systemic corticosteroids, in any form, dose or route of administration, in people with acute optic neuritis.
Data collection and analysis
We used standard methodological procedures expected by Cochrane.
Main results
We included six RCTs with a total of 750 participants. Each trial was conducted in a different country: Denmark, Germany, India, Japan, UK, and United States. Additionally, we identified two ongoing trials not due to be completed until 2016. Among the six trials included in this review, we judged one to be at high risk of bias. The remaining five trials were judged to be at either low or uncertain risk of biases.
Five trials compared only two intervention groups and one trial had a three‐arm comparison of oral corticosteroids or intravenous corticosteroids with placebo. Of the five trials with only two intervention groups, two trials compared oral corticosteroids versus placebo, two trials compared intravenous corticosteroids with placebo, and one trial compared intravenous dexamethasone with intravenous methylprednisolone plus oral prednisolone.
Three trials evaluating oral corticosteroids used varying doses of corticosteroids versus placebo. In the meta‐analyses to assess visual acuity, the risk ratio (RR) was 1.00 (95% confidence interval (CI) 0.82 to 1.23; participants = 398) at one month; 0.92 (95% CI 0.77 to 1.11; participants = 355) at six months; and 0.93 (95% CI 0.70 to 1.24; participants = 368) at one year. In the meta‐analyses of two trials evaluating corticosteroids with total dose greater than 3000 mg administered intravenously, the RR of normal visual acuity (defined as 20/20 Snellen fraction or equivalent) in the intravenous corticosteroids group compared with the placebo group was 1.05 (95% CI 0.88 to 1.26; participants = 346) at six months. The RR of contrast sensitivity in the normal range for the same comparison was 1.11 (95% CI 0.92 to 1.33; participants = 346) at six months follow‐up. The RR of normal visual field for this comparison was 1.08 (95% CI 0.96 to 1.21; 346 participants) at six months; and 1.01 (95% CI 0.86 to 1.19; participants = 316) at one year. Four trials reported adverse events primarily related to gastrointestinal symptoms and sleep disturbance; one trial reported minor adverse event of acne.
Authors' conclusions
There is no conclusive evidence of benefit in terms of recovery to normal visual acuity, visual field or contrast sensitivity six months after initiation with either intravenous or oral corticosteroids at the doses evaluated in trials included in this review.
Plain language summary
Corticosteroids for treating optic neuritis
Review question We reviewed the evidence about the effects of corticosteroids on visual recovery of people with acute optic neuritis.
Background Optic neuritis is inflammation of the optic nerve leading to sudden loss of vision that takes place over the course of several hours or days. The optic nerve, which enters the back of the eye, carries visual information from the eye to the brain. When the optic nerve becomes inflamed, damage may occur. Thus information from the eye to the brain is interrupted, resulting in temporary or permanent vision loss. Optic neuritis is closely linked to multiple sclerosis (MS), an inflammatory disease that affects nerve cells generally. Corticosteroids have been widely used in the treatment of optic neuritis due to their anti‐inflammatory effects.
Study characteristics For this systematic review, we identified six trials conducted in Denmark, Germany, India, Japan, United Kingdom, and United States, which included 750 participants. These trials compared corticosteroid treatment with placebo or another treatment; they varied in the way corticosteroids were given and the dose. Two trials compared oral corticosteroids versus placebo; three trials compared intravenous corticosteroids versus placebo; one trial compared two types of intravenous corticosteroids; and one trial with three groups compared oral corticosteroids versus intravenous corticosteroids versus placebo. Participants in all six trials were followed up for at least three months. Outcomes of visual acuity, contrast sensitivity in the normal range and visual field were assessed at 1, 6, and 12 months. Quality of life also was assessed and reported in one trial. The information is current as of 7 April 2015.
Key results There was no available evidence of beneficial effect from oral or intravenous corticosteroids compared with placebo for the visual acuity, visual field, and contrast sensitivity outcomes. Adverse effects, although not consistently reported, included dermatological symptoms, endocrinological disorders, gastrointestinal problems, headache, fever, sleep disturbance and psychiatric problems. Severe adverse events were reported in the intravenous steroid treatment group of one trial. The investigators of three trials concluded that minor adverse events were more common in steroid groups than in the placebo group.
Quality of the evidence Out of six trials included in this review, we assessed one trial to have high risk of bias due to including a subset of participants who were allowed to choose their intervention. The remaining five trials were of either low or uncertain risk of biases.
Background
Description of the condition
Optic neuritis is an inflammatory disease of the optic nerve. It is second only to glaucoma as the most common acquired optic nerve disorder in persons under 50 years. The majority of people with optic neuritis are between the ages of 20 and 50 years, with a mean age ranging from 30 to 35 years. In population‐based studies in the United States, the annual incidence of optic neuritis has been estimated to be between 1 and 5 per 100,000 (Beck 1998). Koch‐Henriksen and Hyllested reported an annual incidence of 4 to 5 per 100,000 for new onset optic neuritis cases in Denmark from 1948 to 1964 (Koch‐Henriksen 1988). In Olmstead County, Minnesota, United States the prevalence rate of optic neuritis was estimated as 115 per 100,000 (Rodriguez 1995). Women are more often affected than men. Optic neuritis is closely linked to multiple sclerosis (MS) and in most cases has a similar pathogenesis (Lightman 1987). It may be the first manifestation of multiple sclerosis or occur later in its course (Ebers 1985). A similar, yet distinct condition to multiple sclerosis known as neuromyelitis optica, or Devic's disease, also is characterized by optic neuritis. Because neuromyelitis optica is very rare and is treated with a different course than typical cases of optic neuritis, we considered optic neuritis secondary to neuromyelitis optica to be outside the scope of this review.
The presenting symptom of optic neuritis usually is abrupt visual loss in one eye taking place over several hours or days, accompanied by mild pain. In about 10% of cases, symptoms occur in both eyes either simultaneously or sequentially (de la Cruz 2006). A clinical diagnosis of optic neuritis may be made based on the following: age between 18 and 45 years, sudden visual loss with progression within one week, pain with eye movement, absence of inflammation in the vitreous or anterior chamber, and improvement in vision that begins within three to four weeks of initial symptoms. The prognosis for visual recovery after acute optic neuritis is generally good; however, most people have some lasting visual impairment. Even when an individual's visual acuity does return to normal, abnormalities frequently remain in other measures such as contrast sensitivity, color vision, and visual field (Fleishman 1987; Sanders 1986).
Description of the intervention
Corticosteroids have been used since the early 1950s to treat acute optic neuritis because of their anti‐inflammatory effects. Initially, some experts advocated treatment with oral prednisone while others recommended alternative or no treatment. In the 1980s, anecdotal reports suggested that high‐dose intravenous corticosteroids might be effective (Spoor 1988). In 1992, the National Eye Institute of the United States National Institutes of Health funded a randomized controlled trial to test the efficacy of corticosteroids in the treatment of optic neuritis (ONTT 1992‐2006). Based on results of this trial the current guidelines in the United States suggest either administration of high‐dose intravenous methylprednisolone to hasten recovery of vision or no treatment. No other treatment has been shown to aid recovery of vision lost due to acute optic neuritis.
How the intervention might work
By controlling the inflammation associated with optic neuritis, it is believed that visual recovery may be quicker, permanent damage to the optic nerve may be prevented, or both. However, corticosteroids, along with having anti‐inflammatory properties, also have known side effects such as hypertension and may lead to other eye disease such as glaucoma or cataract.
Why it is important to do this review
Prior to the Optic Neuritis Treatment Trial (ONTT) (ONTT 1992‐2006), well‐established guidelines for treating optic neuritis did not exist. Brusaferri and Candelise published a meta‐analysis of steroids for multiple sclerosis and optic neuritis with inclusion criteria for participants and treatment type different from those specified for this review (Brusaferri 2000). A systematic review of available studies is needed to further explore the value of corticosteroids in treating optic neuritis.
We first published a Cochrane review of this topic in 2007 (Vedula 2007), for which we identified five trials of corticosteroid use in participants with acute optic neuritis compared with placebo or no treatment (Kapoor 1998; ONMRG 1999; ONTT 1992‐2006; Sellebjerg 1999; Tübingen Study 1993). In an update of the review in 2012 (Gal 2012), we identified one additional trial that had investigated the effects of two corticosteroids head‐to‐head (Menon 2007).
Objectives
The objective of this review was to assess the effects of corticosteroids on visual recovery in eyes with acute optic neuritis.
Methods
Criteria for considering studies for this review
Types of studies
This review included only randomized controlled trials (RCTs).
Types of participants
We included trials in which the participants had acute optic neuritis. We did not consider participants diagnosed with neuromyelitis optica, or Devic's disease, as this condition is treated differently than cases of optic neuritis due to other causes. There were no age limitations.
Types of interventions
We included trials in which systemic corticosteroid therapy was administered in any form or dosage with the intention to treat or reduce the symptoms of acute optic neuritis and compared with placebo, sham, no treatment, or types of corticosteroid administered via the same route. We excluded studies that only compared routes of administration. We did not limit inclusion of trials in this review based on the duration of treatment or the length of follow‐up.
Types of outcome measures
Primary outcomes
The primary outcomes for comparison of interventions were visual outcomes measured as:
(1) Proportion of participants with normal visual acuity, defined as best‐corrected 20/20 Snellen fraction or equivalent, at six months or more; (2) Proportion of participants with contrast sensitivity in the normal range at six months or more; (3) Proportion of participants with normal visual field, defined as greater than −3.00 dB by Goldmann perimeter test, at six months or more.
Secondary outcomes
Secondary outcomes comparison of interventions were immediate response (rate of recovery) measured as:
(1) Proportion of participants with normal visual acuity at one month; (2) Proportion of participants with contrast sensitivity in the normal range at one month; (3) Proportion of participants with normal visual field at one month.
We compared adverse outcomes related to treatment. We also planned to compare data on quality of life whenever available.
Search methods for identification of studies
Electronic searches
We searched CENTRAL (which contains the Cochrane Eyes and Vision Group Trials Register) (The Cochrane Library 2015, Issue 4), MEDLINE (January 1950 to April 2015), EMBASE (January 1980 to April 2015), Latin American and Caribbean Health Sciences Literature (LILACS) (January 1982 to April 2015), PubMed (January 1946 to April 2015), the metaRegister of Controlled Trials (mRCT) (www.controlled-trials.com), ClinicalTrials.gov (www.clinicaltrials.gov) and the World Health Organization (WHO) International Clinical Trials Registry Platform (ICTRP) (www.who.int/ictrp/search/en). We did not impose any language or date restrictions in the search for trials. The metaRegister of Controlled Trials (mRCT) was last searched 6 March 2014. The electronic databases were last searched on 7 April 2015.
See: Appendices for details of search strategies for CENTRAL (Appendix 1), MEDLINE (Appendix 2), EMBASE (Appendix 3), LILACS (Appendix 4), PubMed (Appendix 5), mRCT (Appendix 6), ClinicalTrials.gov (Appendix 7) and the ICTRP (Appendix 8).
Searching other resources
We searched the reference lists of identified trial reports to find additional trials and used the Science Citation Index to find studies that may have cited the identified trials. We did not conduct manual searches of conference abstracts specifically for this review.
Data collection and analysis
Selection of studies
Two review authors independently assessed the titles and abstracts of all records identified by the electronic and other searches. We retrieved full‐text reports of potentially or definitely relevant trials as assessed by at least one review author and reviewed these according to the definitions in the 'Criteria for considering studies for this review'. For potentially relevant trials published in non‐English languages, we translated the Methods and Results sections and then assessed the trials for inclusion. Two review authors independently categorized the reports as 'include' or 'exclude'. A third review author resolved any disagreements. We documented excluded studies and the reasons for exclusion in the 'Characteristics of excluded studies' table.
Data extraction and management
Two review authors independently extracted data on study characteristics, such as methods, details of participants, interventions, outcomes, and other relevant information. We used paper data collection forms for duplicate data abstraction and resolved discrepancies by consensus. One review author entered data into Review Manager software (RevMan 2014); and a second review author verified all data entered. We contacted trial investigators for data that were missing or unclear in the trial reports. When investigators did not respond within six weeks or we were not able to communicate with them, we used data as available from the reports.
Assessment of risk of bias in included studies
Two review authors, unmasked to the trial lists, institutions and trial results, assessed included trials for risk of bias in several domains of potential bias according to methods set out in Chapter 8 of the Cochrane Handbook for Systematic Reviews of Interventions (Higgins 2011). A third review author resolved any disagreements. We evaluated each trial for bias in the following domains: selection bias (sequence generation and allocation concealment before randomization), performance bias (masking of participants and study personnel), detection bias (masking of outcome assessors), attrition bias (incomplete outcome data), reporting bias (selective outcome reporting), and other sources of bias. We judged each trial as being at 'low', 'high', or 'unclear' risk of bias for each domain. We contacted trial investigators for additional information on issues that were unclear from information available in the trial reports. When investigators did not respond within six weeks or we were not able to communicate with them, we assigned judgment based on the information available.
Measures of treatment effect
We calculated summary risk ratios (RRs) with 95% confidence intervals (CIs) for all outcomes. RRs greater than 1 indicate the normality of the outcome (visual acuity, contrast sensitivity and visual field) is achieved more often in the corticosteroid group than the control group.
Unit of analysis issues
The unit of analysis was the individual participant for all outcomes. All trials enrolled unilateral cases of acute optic neuropathy; thus, analyses by participant are equivalent to analyses by eye.
Dealing with missing data
We contacted the primary investigators of included trials to obtain data not reported for some participants. We used available data included in the trial reports when there was no response within six weeks. We did not impute data for the purposes of this review.
Assessment of heterogeneity
We assessed clinical and methodological heterogeneity by examining potential variations in participant characteristics, interventions compared, and assessments of primary and secondary outcomes among included trials. We used the I² statistic (%) to determine the proportion of variation due to statistical heterogeneity, with a value above 50% considered to represent substantial statistical heterogeneity. We also examined results of the Chi² test and the degree of overlap in confidence intervals of included trials to assess heterogeneity. Poor overlap of confidence intervals on treatment effect estimates suggest heterogeneity among trials.
Assessment of reporting biases
We planned to examine funnel plots to assess possible publication bias when 10 or more trials were included in meta‐analysis. We assessed for selective outcome reporting at the trial level as part of the assessment of risk of bias in included trials.
Data synthesis
When there was no important clinical or methodological heterogeneity among trials, we summarized the results of the trials in meta‐analyses. We used a random‐effects model in each analysis. We did not summarize results with meta‐analysis when substantial statistical heterogeneity (I² greater than 50%) was present; instead we reported individual trial results only.
Subgroup analysis and investigation of heterogeneity
We did not conduct subgroup analyses for this review due to insufficient data. Two trials reported subgroup analyses for different outcomes (Kapoor 1998Sellebjerg 1999). One reported visual outcomes separately for long and short lesions (Kapoor 1998); the other reported a post hoc subgroup analysis and concluded that participants with a more severe baseline visual deficit had more pronounced response to high‐dose methylprednisolone treatment. Therefore, we only documented the results from these trials. If sufficient and comparable data are reported in future updates to this review, we will conduct subgroup analyses.
Sensitivity analysis
We did not conduct planned sensitivity analyses to determine the impact of exclusion of trials with high risk of bias, exclusion of unpublished trials, and exclusion of industry‐funded trials because of the lack of a sufficient number of trials in these categories.
Results
Description of studies
Results of the search
The electronic searches for the previous published versions of this review were conducted in January 2006 and February 2012 and yielded 430 and 815 records, respectively. As of February 2012, we had included six trials in the review (Kapoor 1998; Menon 2007; ONMRG 1999; ONTT 1992‐2006; Sellebjerg 1999; Tübingen Study 1993); and identified one ongoing trial (NCT01524250).
In the most recent electronic searches performed on 7 April 2015, we identified 873 additional titles and abstracts along with 57 records in trial registers (Figure 1). We retrieved and excluded the full‐text report of one potentially relevant study (Al‐Eajailat 2014); and identified one ongoing trial (NCT01838174). We identified no new trials for inclusion in this updated review.
1.
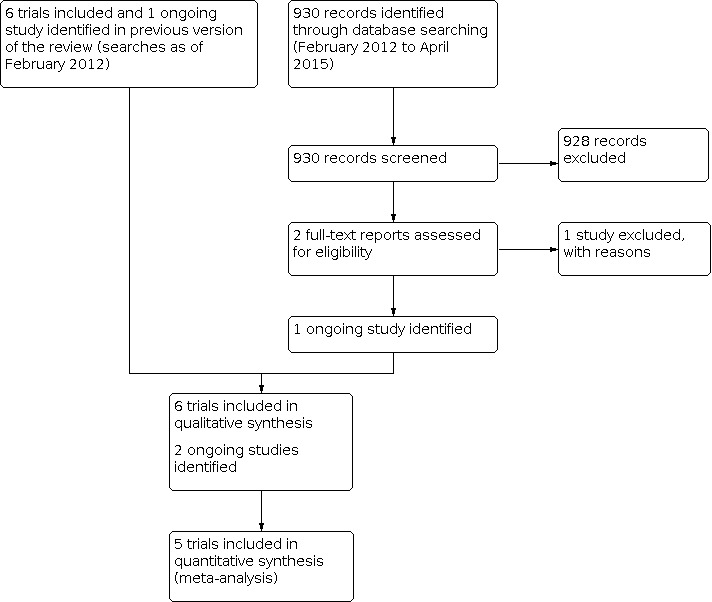
Study flow diagram.
Included studies
We included six trials in which a total of 750 participants had been randomized. Detailed characteristics of the individual trials are presented in the 'Characteristics of included studies' table.
Types of participants
Four trials restricted participants to those with no history of prior attacks of optic neuritis in the affected eye (Kapoor 1998; ONTT 1992‐2006; Menon 2007; Tübingen Study 1993). Kapoor 1998 included only participants with confirmed multiple sclerosis, while the remaining trials included people with optic neuritis of unknown or demyelinating etiologies. ONMRG 1999 enrolled only participants with acute symptoms of unilateral optic neuritis of unknown or demyelinating origin, with relative afferent pupillary defect and a normal or swollen optic disc in the affected eye. Sellebjerg 1999 included participants with optic neuritis and visual acuity of 0.7 or less (Snellen decimal fraction) in the affected eye.
All trials restricted participants to those with a short period since onset of visual symptoms. Participants had visual symptoms for less than two weeks in ONMRG 1999; less than eight days in ONTT 1992‐2006 and Menon 2007; less than three weeks in Tübingen Study 1993; and less than four weeks in Kapoor 1998 and Sellebjerg 1999. Participants with a history of treatment with corticosteroids were excluded from five trials (Menon 2007ONMRG 1999ONTT 1992‐2006Sellebjerg 1999Tübingen Study 1993).
Types of interventions
The six trials had various comparisons. Five trials compared only two intervention groups; whereas ONTT 1992‐2006 was a three‐arm trial comparing oral corticosteroids or intravenous corticosteroids with placebo. In all, three trials compared oral corticosteroids versus placebo (ONTT 1992‐2006; Sellebjerg 1999; Tübingen Study 1993), three trials compared intravenous corticosteroids with placebo (Kapoor 1998; ONMRG 1999; ONTT 1992‐2006), and one trial compared intravenous dexamethasone with intravenous methylprednisolone plus oral prednisolone (Menon 2007).
The description of doses of corticosteroids evaluated in each of the trials in the text of this review refers to the total dose administered over the specified treatment period. The treatment regimens of the individual trials are described in greater detail in the 'Characteristics of included studies' table. The total dose of corticosteroid administered to participants in the treatment arms in the included trials varied from 200 mg in Menon 2007 to more than 3770 mg in the intravenous corticosteroid arm of the ONTT 1992‐2006. The control intervention was intravenous mecobalamin (B12) in ONMRG 1999; and oral thiamine (B1) in Tübingen Study 1993. Because of systemic treatment administration in all included trials, randomization was by participant.
Types of outcomes
Investigators of all trials measured and reported visual acuity as an outcome. Contrast sensitivity was reported from five trials (Kapoor 1998; Menon 2007; ONMRG 1999; ONTT 1992‐2006; Sellebjerg 1999). In all trials, visual field was measured; Sellebjerg 1999 did not assess visual field in a systematic manner (personal communication with Dr. Sellebjerg). In four trials, personnel assessed color vision (Menon 2007; ONMRG 1999; ONTT 1992‐2006; Sellebjerg 1999). Menon 2007 also reported stereoacuity and visual evoked response as outcomes. Only ONTT 1992‐2006 reported quality of life as an outcome, but assessments were made at 5 to 18 years after trial entry.
There was variability in the method employed to assess different outcomes as noted in the 'Characteristics of included studies' table. Menon 2007 presented mean values for visual acuity, visual field (data not shown in report), and contrast sensitivity instead of defining normal values for each. Normal visual acuity was defined as 20/20 Snellen fraction or equivalent in the other five included trials, normal visual field was defined as greater than −3.00 dB by Goldmann perimeter test; contrast sensitivity was measured in various ways. Normal contrast sensitivity was defined as greater than 1.65 log units in ONTT 1992‐2006 and ONMRG 1999. Sellebjerg 1999 measured contrast sensitivity using Arden gratings and defined normal as less than or equal to 80 points. Kapoor 1998 considered normal contrast sensitivity to be greater than 1.35 dB by Humphrey automated perimetry when carried out using the manufacturer’s 30‐2 protocol.
Excluded studies
We excluded 21 studies, listed in the 'Characteristics of excluded studies' table with reasons for exclusion.
Risk of bias in included studies
Figure 2 presents a summary of the 'Risk of bias' assessments for the included trials. For nearly half the total number of domains we could not assess risk of bias from available information and designated the risk of bias to be 'unclear'. Descriptions of our judgments and classifications for each domain are summarized below.
2.

Risk of bias summary: review authors' judgements about each risk of bias item for each included study.
Allocation
All trials were reported as randomized, but only two reported adequate methods of sequence generation and allocation concealment before randomization (ONTT 1992‐2006; Sellebjerg 1999). We judged two trials at high risk of selection bias: Menon 2007 reported that participants were randomized by block randomization, yet in correspondence with the author, the author clarified that the first case was decided by a toss of a coin and all subsequent assignments were decided by alternate assignment; and Tübingen Study 1993 reported a subgroup of participants who chose their own treatment, and therefore the sequence for the treatment assignments was not properly generated and the allocations were not concealed for this subgroup. We deemed the remaining two trials as having had unclear risk of selection bias due to inadequate reporting of information (Kapoor 1998; ONMRG 1999).
Masking (performance bias and detection bias)
We assessed two trials at low risk of performance bias and detection bias as participants, personnel, and outcome assessors were masked (Menon 2007; ONMRG 1999). We judged three trials at unclear risk of bias: only two of the three treatment groups were masked in ONTT 1992‐2006 and two trials were reported as 'double‐blind' but did not provide procedural details (Kapoor 1998; Sellebjerg 1999). In one trial, a group of participants (12 of 50) declined to be randomized and masked, thus we judged this trial to be at high risk of performance and detection bias (Tübingen Study 1993).
Incomplete outcome data
We judged three trials at low risk of attrition bias for low (less than 5%) or no loss to follow‐up through six months (Kapoor 1998; Menon 2007; ONTT 1992‐2006). We judged one trial, in which only a portion of participants could be assessed for some outcomes at each follow‐up time point, as at high risk of attrition bias (ONMRG 1999). We judged Sellebjerg 1999 and Tübingen Study 1993 at unclear risk of attrition bias because there was missing data for more than 10% of participants and participants with protocol violations, poor compliance, or both were excluded from analysis by trial investigators.
Selective reporting
We judged all six trials at low risk of selective reporting bias because the investigators reported pre‐specified primary and secondary outcomes of interest (ONTT 1992‐2006; Sellebjerg 1999); or reported outcomes based on outcomes described in the trial reports (Kapoor 1998; Menon 2007; ONMRG 1999; Tübingen Study 1993).
Other potential sources of bias
We judged three trials to have unclear risk of other bias because they reported receiving funding or study medication from the pharmaceutical companies (ONTT 1992‐2006; Sellebjerg 1999); or modified analysis by pooling treatment and control groups (Kapoor 1998). We judged one trial to be at high risk of other potential bias due to the funding from pharmaceutical industry and because a subgroup of participants chose the assignment by their own decision (Tübingen Study 1993). We considered the remaining trials as having had low risk of other potential sources of bias (Menon 2007; ONMRG 1999).
Effects of interventions
We did not combine all included trials in a single meta‐analysis because the doses and routes of administration of corticosteroids differed among trials, constituting clinical heterogeneity of interventions. Three trials compared oral administration of corticosteroids with no corticosteroids. Oral corticosteroid doses ranged from 1 mg to 500 mg per day with tapered doses up to 5 mg; the treatment periods were 10 days in Sellebjerg 1999, 18 days in ONTT 1992‐2006, and 21 days in Tübingen Study 1993. Three trials compared intravenous administration of corticosteroids with no corticosteroids. Intravenous corticosteroid doses ranged from 1 mg to 1000 mg per day for up to 3 days (Kapoor 1998; ONMRG 1999; ONTT 1992‐2006). One trial compared intravenous dexamethasone versus intravenous methylprednisolone followed by oral prednisone for 3 days (Menon 2007).
Oral corticosteroids versus placebo
Three included trials provided data for this comparison (ONTT 1992‐2006; Sellebjerg 1999; Tübingen Study 1993).
Visual acuity
At one month, data were available from ONTT 1992‐2006, Sellebjerg 1999 and Tübingen Study 1993, and the pooled risk ratio of normal visual acuity was 1.00 (95% CI 0.82 to 1.23; participants = 398). At 6 months, in a meta‐analysis of ONTT 1992‐2006 and Tübingen Study 1993, the risk ratio of normal visual acuity was 0.92 (95% CI 0.77 to 1.11; participants = 355). At one year, data on normal visual acuity were available from ONTT 1992‐2006, Tübingen Study 1993 and Sellebjerg 1999, and the risk ratio was 0.93 (95% CI 0.70 to 1.24; participants = 368) (Analysis 1.1). The risk ratio for normal visual acuity at 6 months was 0.93 (95% CI 0.76 to 1.13) in ONTT 1992‐2006; and 0.89 (95% CI 0.55 to 1.42) in Tübingen Study 1993. The risk ratio for normal visual acuity at one year in ONTT 1992‐2006 was 0.76 and favored placebo (95% CI 0.63 to 0.92). The risk ratio for normal visual acuity at one year was 1.09 (95% CI 0.82 to 1.44) in Tübingen Study 1993, and 1.10 (95% CI 0.67 to 1.80) in Sellebjerg 1999; unlike ONTT 1992‐2006, there was no important difference between outcomes by trial arms.
1.1. Analysis.

Comparison 1: Oral corticosteroids versus placebo, Outcome 1: Participants with normal visual acuity
Contrast sensitivity
At one month, the risk ratio of contrast sensitivity in the normal range was 1.00 (95% CI 0.90 to 1.12) in ONTT 1992‐2006; and 1.16 (95% CI 0.40 to 3.39) in Sellebjerg 1999. At six months, ONTT 1992‐2006 was the only trial that reported contrast sensitivity. Among 156 participants in oral corticosteroids group, 87 had contrast sensitivity in normal range, among 150 participants in placebo group, 82 of whom had contrast sensitivity in normal range (RR 1.05; 95% CI 0.67 to 1.64). At one year, the risk ratio for contrast sensitivity in the normal range was 0.93 (95% CI 0.86 to 1.00) in ONTT 1992‐2006 and 1.58 (95% CI 0.64 to 3.85) in Sellebjerg 1999 (Analysis 1.2).
1.2. Analysis.

Comparison 1: Oral corticosteroids versus placebo, Outcome 2: Participants with contrast sensitivity in the normal range
Visual field
Visual field data were reported from only two trials (ONTT 1992‐2006; Tübingen Study 1993). The risk ratio for normal visual field at six months was 1.00 (95% CI 0.87 to 1.14) in ONTT 1992‐2006 and 1.05 (95% CI 0.87 to 1.27) in Tübingen Study 1993. Comparison of visual field outcomes at one month and one year similarly showed no benefit to oral corticosteroids from ONTT 1992‐2006 and Tübingen Study 1993. At one month, the risk ratio for normal visual field was 1.16 (95% CI 0.88 to 1.51) in ONTT 1992‐2006 and 1.51 (95% CI 0.92 to 2.49) in Tübingen Study 1993. At one year, the risk ratio for normal visual field was 0.94 (95% CI 0.79 to 1.12) in ONTT 1992‐2006 and 0.99 (95% CI 0.83 to1.17) in Tübingen Study 1993 (Analysis 1.3).
1.3. Analysis.

Comparison 1: Oral corticosteroids versus placebo, Outcome 3: Participants with normal visual field
Adverse effects
Adverse effects were reported in three included trials (ONTT 1992‐2006; Sellebjerg 1999; Tübingen Study 1993). Sellebjerg 1999 reported no serious adverse effects and Tübingen Study 1993 reported only acne. The ONTT 1992‐2006 reported depression, acute pancreatitis, weight gain, sleep disturbance, mild mood change, stomach upset, and facial flushing. The proportion of participants experiencing adverse effects of corticosteroid therapy was not consistently reported by all trials, thereby precluding any comparison.
Quality of life outcomes
Quality of life was assessed and reported only in ONTT 1992‐2006 using participant‐reported responses to the National Eye Institute Visual Functioning Questionnaire (NEI‐VFQ) several years after the initial acute optic neuritis event (Mangione 1998). However, no comparative quality of life data by assigned treatment arm were available.
Intravenous corticosteroids (total dose ≥ 3000 mg) versus placebo
Three included trials provided data for comparison of outcomes (Kapoor 1998; ONMRG 1999; ONTT 1992‐2006).
Visual acuity
Only one study reported data for visual acuity at one month (ONTT 1992‐2006). In ONTT 1992‐2006, 87 of 144 participants in corticosteroid group and 79 of 141 participants in placebo group reported having normal visual acuity at one month (RR 1.08; 95% CI 0.89 to 1.31). In a meta‐analysis of Kapoor 1998 and ONTT 1992‐2006 for evaluating corticosteroid of dose greater than 3000 mg administered intravenously versus placebo, the risk ratio of normal visual acuity at six months follow‐up was 1.05 (95% CI 0.88 to 1.26; participants = 346) (Analysis 2.1). At one year follow‐up, two trials reported visual acuity but used different scales; meta‐analysis was not conducted. In ONTT 1992‐2006, 105 of 137 participants in corticosteroid group versus 96 of 133 in the placebo group had normal visual acuity using a retro‐illuminated ETDRS chart (RR 1.27; 95% CI 0.73 to 2.19). In ONMRG 1999, visual acuity better than Snellen decimal fraction of 1.0 (20/20) was noted in 25 of 33 participants in the corticosteroid group and 23 of 33 participants in the control group (RR 1.36; 95% CI 0.46 to 4.04).
2.1. Analysis.

Comparison 2: Total intravenous corticosteroid dose more than or equal to 3000 mg versus placebo, Outcome 1: Participants with normal visual acuity at 6 months
Contrast sensitivity
At one month, data on contrast sensitivity in the normal range were available from ONMRG 1999 and ONTT 1992‐2006, with risk ratio of 1.85 (95% CI 0.93 to 3.66) reported in ONMRG 1999; and 1.06 (95% CI 0.95 to 1.17) reported in ONTT 1992‐2006 (Analysis 2.2). In a meta‐analysis of Kapoor 1998 and ONTT 1992‐2006, the risk ratio of contrast sensitivity in the normal range was 1.11 (95% CI 0.92 to 1.33; participants = 346) at six months follow‐up (Analysis 2.3). At one year, data on contrast sensitivity in the normal range were available from ONMRG 1999 and ONTT 1992‐2006. The risk ratio of contrast sensitivity in the normal range at one year follow‐up was 1.33 (95% CI 1.02 to 1.72) in ONMRG 1999; and 0.99 (95% CI 0.93 to 1.06) in ONTT 1992‐2006 (Analysis 2.4).
2.2. Analysis.

Comparison 2: Total intravenous corticosteroid dose more than or equal to 3000 mg versus placebo, Outcome 2: Participants with contrast sensitivity in the normal range sensitivity at 1 month
2.3. Analysis.

Comparison 2: Total intravenous corticosteroid dose more than or equal to 3000 mg versus placebo, Outcome 3: Participants with contrast sensitivity in the normal range at 6 months
2.4. Analysis.

Comparison 2: Total intravenous corticosteroid dose more than or equal to 3000 mg versus placebo, Outcome 4: Participants with contrast sensitivity in the normal range at 1 year
We have not reported a meta‐analysis for this outcome at one year because there was substantial statistical heterogeneity (I² = 79%; P value for the Chi² test of homogeneity = 0.01 ). Similarly, we found substantial heterogeneity among estimates of this outcome at one month with data from ONMRG 1999 and ONTT 1992‐2006 (I² = 63% and P value for Chi² test of homogeneity = 0.10). Though the P value for the Chi² test was greater than 0.05, the test has low power when used with few studies.
Visual field
One‐month data were available from ONMRG 1999 and ONTT 1992‐2006 with the pooled risk ratio of normal visual field equaling 1.56, but it is not statistically significant (95% CI 0.88 to 2.76; participants = 330; I² = 33% and P value for Chi² test = 0.22) (Analysis 2.5). Six‐month visual field data were available from Kapoor 1998 and ONTT 1992‐2006. The pooled risk ratio of normal visual field at six months follow‐up was 1.08 (95% CI 0.96 to 1.21; participants = 346) (Analysis 2.6). One‐year data were available from ONMRG 1999 and ONTT 1992‐2006. At one year the pooled risk ratio of normal visual field was 1.01 (95% CI 0.86 to 1.19; participants = 316) (Analysis 2.7).
2.5. Analysis.

Comparison 2: Total intravenous corticosteroid dose more than or equal to 3000 mg versus placebo, Outcome 5: Participants with normal visual field at 1 month
2.6. Analysis.

Comparison 2: Total intravenous corticosteroid dose more than or equal to 3000 mg versus placebo, Outcome 6: Participants with normal visual field at 6 months
2.7. Analysis.

Comparison 2: Total intravenous corticosteroid dose more than or equal to 3000 mg versus placebo, Outcome 7: Participants with normal visual field at 1 year
Adverse events
Adverse events were not reported in Kapoor 1998. In ONMRG 1999, hyperglycemia was noted in four participants; constipation, diarrhea, acneiform eruption and hyperlipidemia were reported for two participants; headache and increasing fever were reported for one participant, and transient diarrhea was reported by two participants. In ONTT 1992‐2006, acute transient depression developed in one participant and acute pancreatitis was diagnosed in another participant in the intravenous‐methylprednisolone group; sleep disturbance, mild mood change, stomach upset, facial flushing, and weight gain were reported for participants in both groups.
Quality of life outcome
Quality of life was assessed and reported only in ONTT 1992‐2006 using participant‐reported responses to the National Eye Institute Visual Functioning Questionnaire (NEI‐VFQ) several years after the initial acute optic neuritis event (Mangione 1998). However, no comparative quality of life data by assigned treatment arm were available.
Intravenous dexamethasone versus intravenous methylprednisolone followed by oral prednisone
Only one trial provided data for this comparison (Menon 2007).
Visual acuity
In Menon 2007, investigators reported LogMAR mean values for visual acuity for both treatment arms. At one month follow‐up, the mean ± SD was 0.42 ± 0.42 in the methylprednisolone group compared to 0.29 ± 0.29 in the dexamethasone group. At three months of follow‐up the mean ± SD was 0.36 ± 0.41 in the methylprednisolone group and 0.28 ± 0.33 in the dexamethasone groups respectively. The difference was not statistically significant but favored methylprednisolone group.
Contrast sensitivity
At one month of follow‐up, mean ± SD contrast sensitivities (by Pelli‐Robson chart) were 1.16 ± 0.48 and 1.25 ± 0.43 in the methylprednisolone and dexamethasone treatment groups respectively in Menon 2007. At three month follow‐up, the mean ± SD was 1.26 ± 0.41 in the methylprednisolone group and 1.37 ± 0.29 in the dexamethasone group, showed the significant improvement during the follow‐up subsequent to the treatments.
Visual field
Limited data were available from Menon 2007 regarding visual field outcomes. Of the two participants in the methylprednisolone group who provided data on visual fields, both had a central scotoma observed in the pretreatment visual field assessment. Following treatment, at three‐month follow‐up the central scotoma had not resolved fully in one participant. Four participants were determined to have a central scotoma among the six participants in the dexamethasone group who underwent the pretreatment visual field assessment. The central field of the eyes of two participants failed to fully recover at three months follow‐up.
Adverse events
In Menon 2007, six participants were reported to have experienced generalized weakness, one participant had sleep disturbance and weight gain, two participants experienced depression and five participants suffered gastric irritation.
Quality of life outcomes
Quality of life was not assessed and reported in Menon 2007.
Discussion
Summary of main results
Acute demyelinating optic neuritis is a common form of optic neuritis, with inflammation of the optic nerve that often is associated with multiple sclerosis. Optic neuritis is the initial manifestation of multiple sclerosis in some people (Kurtzke 1985). In this systematic review performed to evaluate the effects of corticosteroid therapy in participants with optic neuritis, we included six randomized controlled trials. We did not conduct a meta‐analysis including all trials because of clinical heterogeneity resulting from variations in doses and routes of administration of corticosteroids. However, we conducted a meta‐analysis of trials evaluating similar doses of corticosteroids (3000 mg or more) administered by the oral route and the intravenous route. The ONTT was the largest of the included trials and contributed the most weight in all the meta‐analyses, which used the inverse weighting approach (ONTT 1992‐2006). While none of the other included trials reported an evidence of benefit with intravenous corticosteroids, the results of our analyses are consistent with the effects on vision of intravenous corticosteroids reported by the ONTT investigators (ONTT 1992‐2006). The 95% confidence intervals for the pooled risk ratios of normal visual acuity, contrast sensitivity in the normal range, and normal visual field at six months for the oral corticosteroids arm and the intravenous route in ONTT include the null value, thus suggesting no evidence of benefit with either oral or intravenous corticosteroids compared to placebo in this large trial for the outcomes of interest in this review (ONTT 1992‐2006). This observation is consistent with the analyses of ONTT outcome data when adjusted for baseline visual acuity (ONTT 1992‐2006). A life‐table analysis reported in the same article indicated that the rate of return of vision to normal was higher with intravenous corticosteroids than with placebo (P = 0.09 for visual acuity, 0.02 for contrast sensitivity and 0.0001 for visual field). No statistically significant difference was found for the same outcomes for oral corticosteroids compared with placebo in a life‐table analysis in the trial report. However, ONTT participants treated with oral corticosteroids had a higher rate of new episodes of optic neuritis compared with those in the placebo arm. The pooled risk ratio indicated a statistically significant benefit with respect to achieving a normal visual field at one month for participants treated with intravenous corticosteroids.
Finally, there was no evidence of benefit when intravenous corticosteroids were compared to intravenous followed by oral corticosteroids for the visual acuity and contrast sensitivity outcomes (Menon 2007).
Overall completeness and applicability of evidence
The trials evaluating oral corticosteroids were very heterogeneous in dose of medication, method of corticosteroid delivery, and comparison group. For the comparisons where meta‐analysis was possible, there was no evidence of benefit with oral or intravenous corticosteroids for each of the outcomes considered. The 95% confidence intervals for the risk ratio of normal visual acuity, contrast sensitivity and visual field included the null value. Oral corticosteroids, however, resulted in statistically significantly fewer ONTT participants who had achieved normal visual acuity by one year compared with the placebo group and was consistent with our review findings. Our review has included no comparison of outcomes between higher and lower doses of corticosteroids. Adverse effects were inconsistently reported; comparisons of different management strategies were not possible. Therefore, the effectiveness and safety of corticosteroids in treating optic neuritis was not supported by the currently available evidence.
Quality of the evidence
Based on the assessment of trial quality per pre‐specified criteria, we judged the overall quality of evidence as low to moderate. Random sequence generation and allocation concealment before randomization were implemented in only two of the six included trials. Masking of participants, personnel, and outcome assessors was achieved in only two trials. Complete or nearly complete outcome data were reported from four trials. Only one trial was considered to be at high risk of selective outcome reporting bias. In addition, one trial was judged to have high risk of bias because a subgroup of participants was allowed to select their treatment; four trials were judged to be unclear risk of other bias due to source of funding to conduct the trial.
Potential biases in the review process
We are unaware of any potential biases in the review process. We searched multiple databases to identify six RCTs relevant to this review. Data extracted from the trials focused on clinical and functional outcomes and were confirmed by at least two authors. Thus, the findings regarding the effectiveness of corticosteroids on treating optic neuritis is based on established, reproducible methods. Inadequate reporting of adverse events may have led to underestimation of such outcomes.
Agreements and disagreements with other studies or reviews
Since the Optic Neuritis Treatment Trial (ONTT) was the first major study to examine corticosteroid treatment for optic neuritis, most other review articles also use data from the ONTT as the basis for their conclusions (ONTT 1992‐2006). In a narrative review article by Bennett 2014, authors came to the same conclusions as this review: that short‐term benefits were seen in the methylprednisolone arm of ONTT, but by one year, there was no clinically or statistically significant difference between treated and untreated participants. Another review on optic neuritis diagnosis and treatment explained corticosteroid treatment in much the same manner, reporting that treatment with corticosteroids hastens recovery but does not affect the final outcome (Toosy 2014). Brusaferri and Candelise published a meta‐analysis of steroids for multiple sclerosis and optic neuritis and although the inclusion criteria and treatment type differed from this review, the conclusions were the same (corticosteroid treatment improved visual acuity at 30 days but the improvement did not differ between treatment arms to a statistically significant degree during longer follow‐up) (Brusaferri 2000).
Authors' conclusions
Implications for practice.
There was no conclusive treatment benefit with return to normal visual acuity, visual field or contrast sensitivity with either intravenous or oral corticosteroids at the doses evaluated by trials included in this review. Either no treatment or treatment with intravenous corticosteroid therapy followed by oral corticosteroids is appropriate; intravenous corticosteroids may benefit the patient in terms of faster recovery to normal vision. As suggested by analyses reported in the ONTT, oral corticosteroid therapy has been associated with an increase in rate of new episodes of optic neuritis (ONTT 1992‐2006).
Implications for research.
Among participant cohorts evaluated as part of this review, there was no conclusive treatment benefit with return to normal visual function measures within one year as the outcome of interest. Future research efforts could focus on the identification of participant subgroups who are predisposed to have permanent visual deficits and would benefit from therapy that could reduce neural damage.
The trial database included a total number of 750 participants enrolled in the six trials. Except for the ONTT, individual trials likely did not have adequate power to detect or rule out a statistically significant difference in one‐year outcomes that favored corticosteroids; larger trials with longer follow‐up may yield different results. Future trials evaluating the role of high dose oral corticosteroids (greater than 3000 mg) as a treatment option for optic neuritis may be warranted.
Neurological outcomes were not the focus of this review but future research to evaluate the role of high‐dose oral corticosteroids as a treatment option for optic neuritis, and including the observation of neurological outcomes, may be warranted.
What's new
| Date | Event | Description |
|---|---|---|
| 11 November 2021 | Amended | Editorial note added. See Published notes for further information. |
History
Protocol first published: Issue 1, 1999 Review first published: Issue 1, 2007
| Date | Event | Description |
|---|---|---|
| 29 July 2015 | New citation required but conclusions have not changed | Issue 8, 2015: No new trials found for inclusion; one additional ongoing study identified |
| 9 April 2015 | New search has been performed | Issue 8, 2015: Electronic searches were updated. |
| 27 February 2012 | New citation required but conclusions have not changed | Issue 4, 2012: Some of the text of the review has been modified to reflect the methodological changes made by The Cochrane Collaboration. |
| 27 February 2012 | New search has been performed | Issue 4, 2012: Updated searches yielded one new trial for inclusion. |
| 27 August 2008 | Amended | Converted to new review format. |
Notes
Acknowledgements
We acknowledge:
Kay Dickersin for conceiving of this review;
Fabio Brusaferri and Livia Candelise for developing the protocol for this review;
Suzanne Brodney‐Folse for conceiving of this review and contributions to the protocol and original version of this review;
Richard Wormald, Graziella Filippini, Roberta Scherer, Kate Henshaw, Barbara Hawkins and Catey Bunce for comments and input on previous versions of this review;
Karen Blackhall, Iris Gordon, Lori Rosman for devising and running the electronic search strategies
Xuan Hui, Elizabeth Clearfield, Andrew Law and Kristina Lindsley, CEVG@US; and Anupa Shah, Managing Editor for CEVG, for support and guidance in completing this review.
Appendices
Appendix 1. CENTRAL search strategy
#1 MeSH descriptor Optic Neuritis #2 (optic* or retrobul*) near/2 (neuritis) #3 (#1 OR #2) #4 MeSH descriptor Adrenal Cortex Hormones #5 MeSH descriptor Glucocorticoids #6 glucocorticoid* #7 MeSH descriptor Pregnadienediols #8 prednisone* #9 prednisolone* #10 methylprednisolone* #11 triamcinolone* #12 dexamethasone* #13 anecortave* #14 (#4 OR #5 OR #6 OR #7 OR #8 OR #9 OR #10 OR #11 OR #12 OR #13) #15 (#3 AND #14)
Appendix 2. MEDLINE (OvidSP) search strategy
1. Randomized Controlled Trial.pt. 2. Controlled Clinical Trial.pt. 3. (randomized or randomised).ab,ti. 4. placebo.ab,ti. 5. drug therapy.fs. 6. randomly.ab,ti. 7. trial.ab,ti. 8. groups.ab,ti. 9. 1 or 2 or 3 or 4 or 5 or 6 or 7 or 8 10. exp animals/ not humans.sh. 11. 9 not 10 12. exp optic neuritis/ 13. ((optic* or retrobul*) adj2 neuritis).tw. 14. or/12‐13 15. exp adrenal cortex hormones/ 16. exp glucocorticoids/ 17. glucocorticoid*.tw. 18. exp pregnadienediols/ 19. prednisone*.tw. 20. prednisolone*.tw. 21. methylprednisolone*.tw. 22. triamcinolone*.tw. 23. dexamethasone*.tw. 24. anecortave*.tw. 25. or/15‐24 26. 14 and 25 27. 11 and 26
The search filter for trials at the beginning of the MEDLINE strategy is from the published paper by Glanville et al (Glanville 2006).
Appendix 3. EMBASE.com search strategy
#1 'randomized controlled trial'/exp #2 'randomization'/exp #3 'double blind procedure'/exp #4 'single blind procedure'/exp #5 random*:ab,ti #6 #1 OR #2 OR #3 OR #4 OR #5 #7 'animal'/exp OR 'animal experiment'/exp #8 'human'/exp #9 #7 AND #8 #10 #7 NOT #9 #11 #6 NOT #10 #12 'clinical trial'/exp #13 (clin* NEAR/3 trial*):ab,ti #14 ((singl* OR doubl* OR trebl* OR tripl*) NEAR/3 (blind* OR mask*)):ab,ti #15 'placebo'/exp #16 placebo*:ab,ti #17 random*:ab,ti #18 'experimental design'/exp #19 'crossover procedure'/exp #20 'control group'/exp #21 'latin square design'/exp #22 #12 OR #13 OR #14 OR #15 OR #16 OR #17 OR #18 OR #19 OR #20 OR #21 #23 #22 NOT #10 #24 #23 NOT #11 #25 'comparative study'/exp #26 'evaluation'/exp #27 'prospective study'/exp #28 control*:ab,ti OR prospectiv*:ab,ti OR volunteer*:ab,ti #29 #25 OR #26 OR #27 OR #28 #30 #29 NOT #10 #31 #30 NOT (#11 OR #23) #32 #11 OR #24 OR #31 #33 'optic neuritis'/exp #34 ((optic* OR retrobul*) NEAR/2 neuritis):ab,ti #35 #33 OR #34 #36 'corticosteroid'/exp #37 'glucocorticoid'/exp #38 glucocorticoid*:ab,ti #39 prednisone*:ab,ti #40 prednisolone*:ab,ti #41 methylprednisolone*:ab,ti #42 triamcinolone*:ab,ti #43 dexamethasone*:ab,ti #44 'pregnane derivative'/exp #45 'anecortave'/exp #46 anecortave*:ab,ti #47 #36 OR #37 OR #38 OR #39 OR #40 OR #41 OR #42 OR #43 OR #44 OR #45 OR #46 #48 #35 AND #47 #49 #32 AND #48
Appendix 4. LILACS search strategy
MH:C10.292.700.550$ or MH:C11.640.576$ or "Neuritis Óptica" or "Neurite Óptica" or "Retrobulbar Neuritis" or ((optic or retrobul$) and neuritis)
Appendix 5. PubMed search strategy
#1 ((randomized controlled trial[pt]) OR (controlled clinical trial[pt]) OR (randomised[tiab] OR randomized[tiab]) OR (placebo[tiab]) OR (drug therapy[sh]) OR (randomly[tiab]) OR (trial[tiab]) OR (groups[tiab])) NOT (animals[mh] NOT humans[mh]) #2 ((optic*[tw] OR retrobul*[tw]) AND (neuritis[tw])) NOT Medline[sb] #3 glucocorticoid*[tw] NOT Medline[sb] #4 prednisone*[tw] NOT Medline[sb] #5 prednisolone*[tw] NOT Medline[sb] #6 methylprednisolone*[tw] NOT Medline[sb] #7 triamcinolone*[tw] NOT Medline[sb] #8 dexamethasone*[tw] NOT Medline[sb] #9 anecortave*[tw] NOT Medline[sb] #10 (#3 OR #4 OR #5 OR #6 OR #7 OR #8 OR #9) #11 (#2 AND #10) #12 (#1 AND #11)
Appendix 6. metaRegister of Controlled Trials search strategy
Optic Neuritis AND (Corticosteroids OR Adrenal Cortex Hormones OR Glucocorticoids OR Pregnadienediols OR Prednisone OR Prednisolone OR Methylprednisolone OR Triamcinolone OR Dexamethasone OR Anecortave)
Appendix 7. ClinicalTrials.gov search strategy
Optic Neuritis AND (Corticosteroids OR Adrenal Cortex Hormones OR Glucocorticoids OR Pregnadienediols OR Prednisone OR Prednisolone OR Methylprednisolone OR Triamcinolone OR Dexamethasone OR Anecortave)
Appendix 8. ICTRP search strategy
Optic Neuritis AND Corticosteroids OR Optic Neuritis AND Adrenal Cortex Hormones OR Optic Neuritis AND Glucocorticoids OR Optic Neuritis AND Pregnadienediols OR Optic Neuritis AND Prednisone OR Optic Neuritis AND Prednisolone OR Optic Neuritis AND Methylprednisolone OR Optic Neuritis AND Triamcinolone OR Optic Neuritis AND Dexamethasone OR Optic Neuritis AND Anecortave
Data and analyses
Comparison 1. Oral corticosteroids versus placebo.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1.1 Participants with normal visual acuity | 3 | Risk Ratio (M‐H, Random, 95% CI) | Subtotals only | |
| 1.1.1 Participants with normal visual acuity at 1 month | 3 | 398 | Risk Ratio (M‐H, Random, 95% CI) | 1.00 [0.82, 1.23] |
| 1.1.2 Participants with normal visual acuity at 6 months | 2 | 355 | Risk Ratio (M‐H, Random, 95% CI) | 0.92 [0.77, 1.11] |
| 1.1.3 Participants with normal visual acuity at 1 year | 3 | 368 | Risk Ratio (M‐H, Random, 95% CI) | 0.93 [0.70, 1.24] |
| 1.2 Participants with contrast sensitivity in the normal range | 2 | Risk Ratio (M‐H, Random, 95% CI) | Totals not selected | |
| 1.2.1 Participants with contrast sensitivity in the normal range at 1 month | 2 | Risk Ratio (M‐H, Random, 95% CI) | Totals not selected | |
| 1.2.2 Participants with contrast sensitivity in the normal range at 1 year | 2 | Risk Ratio (M‐H, Random, 95% CI) | Totals not selected | |
| 1.3 Participants with normal visual field | 2 | Risk Ratio (M‐H, Random, 95% CI) | Totals not selected | |
| 1.3.1 Participants with normal visual field at 1 month | 2 | Risk Ratio (M‐H, Random, 95% CI) | Totals not selected | |
| 1.3.2 Participants with normal visual field at 6 months | 2 | Risk Ratio (M‐H, Random, 95% CI) | Totals not selected | |
| 1.3.3 Participants with normal visual field at 1 year | 2 | Risk Ratio (M‐H, Random, 95% CI) | Totals not selected |
Comparison 2. Total intravenous corticosteroid dose more than or equal to 3000 mg versus placebo.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 2.1 Participants with normal visual acuity at 6 months | 2 | 346 | Risk Ratio (M‐H, Random, 95% CI) | 1.05 [0.88, 1.26] |
| 2.2 Participants with contrast sensitivity in the normal range sensitivity at 1 month | 2 | 322 | Risk Ratio (M‐H, Random, 95% CI) | 1.27 [0.74, 2.16] |
| 2.3 Participants with contrast sensitivity in the normal range at 6 months | 2 | 346 | Risk Ratio (M‐H, Random, 95% CI) | 1.11 [0.92, 1.33] |
| 2.4 Participants with contrast sensitivity in the normal range at 1 year | 2 | Risk Ratio (M‐H, Random, 95% CI) | Subtotals only | |
| 2.5 Participants with normal visual field at 1 month | 2 | 330 | Risk Ratio (M‐H, Random, 95% CI) | 1.56 [0.88, 2.76] |
| 2.6 Participants with normal visual field at 6 months | 2 | 346 | Risk Ratio (M‐H, Random, 95% CI) | 1.08 [0.96, 1.21] |
| 2.7 Participants with normal visual field at 1 year | 2 | 316 | Risk Ratio (M‐H, Random, 95% CI) | 1.01 [0.86, 1.19] |
Characteristics of studies
Characteristics of included studies [ordered by study ID]
Kapoor 1998.
| Study characteristics | ||
| Methods |
Study design: parallel group randomized controlled trial Number randomized: 66 total participants; number per group not reported Exclusions after randomization: none reported Losses to follow up: 2 at last follow‐up (26 weeks) Number analyzed: 64; 33 in steroid group and 31 in placebo group Unit of analysis: participant How were missing data handled?: excluded from the analyses Power calculation: none reported |
|
| Participants |
Country: United Kingdom Age: mean 32 years Gender: 17/66 (25.8%) men and 49/66 (74.2%) women Inclusion criteria: unilateral acute optic neuritis; corrected visual acuity in the affected eye of 6/9 or worse within 30 days of symptoms; patients with multiple sclerosis but without prior history of optic neuritis Exclusion criteria: evidence of improved vision at the time of study entry; bilateral involvement; previous ocular pathology; previous episodes of optic neuritis; psychosis; significant systemic disease including active infection, diabetes mellitus, systemic hypertension; history of tuberculosis; other contraindications to steroid treatment such as active peptic ulceration Equivalence of baseline characteristics: not reported |
|
| Interventions |
Intervention 1: intravenous methylprednisolone (1 gram/day given as a single bolus) Intervention 2: intravenous saline Length of follow‐up: 26 weeks |
|
| Outcomes |
Primary outcomes, as specified: (1) Visual acuity at 26 weeks; (2) Contrast sensitivity at 26 weeks (measured using circular patches of luminance modulated vertical sine wave gratings); (3) Visual field at 26 weeks or more (Humphrey automatic perimetry using 30‐2 protocol) Secondary outcomes: not reported Adverse events reported: not reported Intervals at which outcomes were assessed: visual acuity assessed at weeks 1, 2, 4, 8, 13, and 26, and visual function measured at 26 weeks |
|
| Notes |
Study period: March 1991 to June 1994 Funding sources: supported by the Multiple Sclerosis Society of Great Britain and Northern Ireland and by the Scarfe Trust Declarations of interest: not reported Reported subgroup analyses: yes; long‐lesion and short‐lesion subgroups were analyzed by the trial investigators separately to assess effects of treatment on visual outcome |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Method of sequence generation not reported. |
| Allocation concealment (selection bias) | Unclear risk | Method of allocation concealment before randomization not reported. |
| Masking (performance bias and detection bias) | Unclear risk | "Patients in either subgroup were randomized double blind to receive IV saline or IVMP"; masking of study personnel and outcome assessors not reported otherwise. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | "Sixty‐four of 66 patients completed 6 months clinical follow‐up (33 treated, 31 placebo)"; "The MRI was repeated after 6 months in 61 of 66 patients"; "VEPs were repeated after 6 months in 43 of 66 cases". |
| Selective reporting (reporting bias) | Low risk | Outcomes reported as described in the methods section, though we did not have access to the original trial protocol. |
| Other bias | Unclear risk | "Because treatment did not appear to influence outcome, some of the results obtained in the treated and placebo groups were analyzed together". |
Menon 2007.
| Study characteristics | ||
| Methods |
Study design: parallel group randomized controlled trial Number randomized: 21 total participants: 11 in dexamethasone group and 10 in methylprednisolone group Exclusions after randomization: none reported Losses to follow up: none reported Number analyzed: 21: 11 in dexamethasone group and 10 in methylprednisolone group Unit of analysis: participant Power calculation: none reported |
|
| Participants |
Country: India Age: mean 29 years (range 7 to 53 years) Gender: 12/21 (57.1%) men and 9/21 (42.9%) women Inclusion criteria: previously untreated acute optic neuritis within 8 days of onset; visual acuity worse than 20/60 in affected eye Exclusion criteria: known systemic disease other than multiple sclerosis; history of optic neuritis attacks; prior diagnosis of multiple sclerosis treated with corticosteroids; evidence of optic disc pallor in affected eye; pre‐existing ocular abnormalities that affect assessment of visual function Equivalence of baseline characteristics: yes |
|
| Interventions |
Intervention 1: intravenous dexamethasone 200 mg (in 150 ml 5% dextrose solution) given over 1.5 to 2 hours once a day for 3 days Intervention 2: intravenous methylprednisolone 250 mg/six‐hourly (in 150 ml 5% dextrose solution) given over 1.5 to 2 hours once a day for 3 days followed by oral prednisolone for 11 days Length of follow‐up: 90 days |
|
| Outcomes |
Primary and secondary outcomes were not differentiated Outcomes as reported: (1) Visual acuity (ETDRS at 4 meters distance and Snellen at 6 meters distance) (2) Visual field (Goldmann perimeter) (3) Contrast sensitivity (Pelli‐Robson chart at 1 meter) (4) Color vision (Ishihara pseudoisochromatic color vision plates) (5) Stereoacuity (Randot stereoacuity test, Wirt circle) (6) Visually evoked response (Lace electronica EREV m99 machine at 33 centimeters) (7) Other: hemogram, fasting blood glucose, immunohistocytological analysis for toxoplasmosis, chest X‐ray, X‐ray paranasal sinuses, aerobic and anaerobic blood cultures, orbital ultrasound and neuroimaging for cases not showing any improvement with standard therapy in either group Adverse events reported: generalized weakness, sleep disturbance and weight gain, depression and gastric irritation Intervals at which outcomes were assessed: 3 days, 1 week, 1 month, and 90 days |
|
| Notes |
Study period: not reported Funding sources: not reported Declarations of interest: not reported Reported subgroup analyses: none reported |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | High risk | According to the published report: "The patients were randomized into two groups by block randomization; however, in correspondence with the author "The first case was decided by a toss of a coin. All subsequent were by rotation of patients (patients were alternatively assigned to group 1 and group 2)." |
| Allocation concealment (selection bias) | High risk | Method of allocation concealment before randomization not reported, but could not have been concealed very long once the first few assignments had been made. |
| Masking (performance bias and detection bias) | Low risk | Both participants and outcome assessors were masked (blinded) to the treatment assignment (author correspondence). |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | No missing data reported. |
| Selective reporting (reporting bias) | Low risk | Outcomes reported as described in the methods section, though we did not have access to the original trial protocol. |
| Other bias | Low risk | None observed. |
ONMRG 1999.
| Study characteristics | ||
| Methods |
Study design: parallel group randomized controlled trial Number randomized: 102 total participants; number per group not reported Exclusions after randomization: exclusions per group not explicitly stated 32 dismissed after start of trial due to different reasons including misdiagnosis and lost data; 2 participants excluded before treatment; 2 participants excluded during treatment due to withdrawal of consent by the participants Losses to follow up: none reported Number analyzed (total and per group): 66: corticosteroids group: 33; control group: 33 Unit of analysis: participant Power calculation: none reported |
|
| Participants |
Country: Japan Age: 14 to 58 (mean 36.3 years) Gender: 22/66 (33.3%) men and 44/66 (66.7%) women Inclusion criteria: “The criteria for eligibility were the same as specified previously.” Acute symptoms indicative of unilateral optic neuritis of unknown or demyelinating origin; visual symptoms of 14‐day duration or less; relative afferent pupillary defect in affected eye; normal or swollen optic disc of affected eye Exclusion criteria: not reported Equivalence of baseline characteristics: yes |
|
| Interventions |
Intervention 1: intravenous methylprednisolone (1 gram/day) for 3 days followed by oral corticosteroid for 7 to 10 days. Intravenous administration was carried out over 45 to 60 minutes once a day in the morning Intervention 2: intravenous mecobalamin (a control drug) (500 microgram/day) for 3 days, followed by oral mecobalamin for at least 7 days. Intravenous administration was carried out over 45 to 60 minutes once a day in the morning Length of follow‐up: 1 year |
|
| Outcomes |
Primary and secondary outcomes were not differentiated Outcomes as reported: (1) Visual acuity: measured using Landolt rings at 5 meters after full refractive correction. Results expressed as decimal acuity, measured before and at 1, 3, 4, 12 weeks and 1 year after the initiation of treatment (2) Visual field: Humphrey 30‐2 for central 30 degrees of visual field and Goldmann perimetry for peripheral field if HFA unsuitable, measured before and at 1, 3, 4, 12 weeks and 1 year after the initiation of treatment (3) Color vision: measured before and at 1, 3, 4, 12 weeks and 1 year after the initiation of treatment (4) Contrast sensitivity: Visual Contrast Test System at a testing distance of 1 meter, measured before and at 1, 3, 4, 12 weeks and 1 year after the initiation of treatment (5) Others: central critical flicker fusion frequency tested before and at 1, 3, 4, 12 weeks and 1 year after the initiation of treatment Adverse events reported: hyperglycemia, constipation, diarrhea (chronic or transient), acneiform eruption, hyperlipidemia, headache, and increasing fever Intervals at which outcomes were assessed: 1, 3, 4, 12 weeks and 1 year |
|
| Notes |
Study period: March 1991 to December 1996 Funding sources: not reported Declarations of interest: not reported Reported subgroup analyses: none reported Information about allocation concealment and outcomes provided by Masato Wakakura |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Method of sequence generation not reported. |
| Allocation concealment (selection bias) | Unclear risk | “treatment was randomly assigned by the envelope method” – details of envelopes (e.g. sequentially numbered, opaque, sealed, etc.) not reported. |
| Masking (performance bias and detection bias) | Low risk | "In this study, it was the policy to inform neither the patient nor examiner which treatment was being used, although it was known by the attending physician". |
| Incomplete outcome data (attrition bias) All outcomes | High risk | “Data for 70 patients were analyzed in the baseline study. Four patients were subsequently eliminated just before the start of treatment (n = 2) or during treatment (n = 2), because they had decided not to give their consent”. “HFA mean deviation could be determined for only 46 cases…Color vision could be examined in 52 eyes in the first 12 weeks of the study…Contrast sensitivity data were obtained for 37 eyes. CFF was measured for 51 eyes” . "No patient was required to drop out of the study". |
| Selective reporting (reporting bias) | Low risk | Outcomes reported as described in the methods section, though we did not have access to the original trial protocol. |
| Other bias | Low risk | In both groups, intravenous administrations (systemic) of the drugs were given to the participants, though some data were presented using "eye" as the unit in the analysis. |
ONTT 1992‐2006.
| Study characteristics | ||
| Methods |
Study design: parallel group randomized controlled trial Number randomized: 457 total participants: 151 in intravenous methylprednisolone group, 156 in oral prednisone group, and 150 in oral placebo group Exclusions after randomization: no exclusions, 9 participants ineligible but randomized and followed Losses to follow up: 19 at 6 months; 48 at 1 year Number analyzed (total and per group): 438 at 6 months: 144 in intravenous methylprednisolone group, 151 in oral prednisone group, and 143 in oral placebo group Unit of analysis: participant How were the missing data handled?: excluded from the analyses Power calculation: none reported |
|
| Participants |
Country: USA Age: mean 32 years (range 18 to 46) Gender: 105/457 (23%) men and 352/457 (77%) women Inclusion criteria: between the ages of 18 to 46 years; history of acute unilateral optic neuritis with visual symptoms lasting 8 days or less; evidence of a relative afferent pupillary defect and a visual‐field defect in the affected eye on examination Exclusion criteria: previous diagnosis with optic neuritis in the same eye or had clinical evidence of a systemic disease, other than multiple sclerosis, that might cause optic neuritis Equivalence of baseline characteristics: yes |
|
| Interventions |
Intervention 1: intravenous methylprednisolone 250 mg every 6 hours for 3 days followed by 1 mg/kg body weight of oral prednisone for 11 days Intervention 2: oral prednisone 1mg/kg/day for 14 days, tapered with administration of 20 mg on day 15 and 10 mg on days 16 and 18 Intervention 3: oral placebo 1 mg/kg/day for 14 days with similar treatment as oral corticosteroid group on days 15, 16 and 18 Length of follow‐up: 12 months |
|
| Outcomes |
Primary outcomes, as defined: (1) Visual field (Humphrey Visual Field Analyzer and Goldmann perimeter) at 6 months (2) Contrast sensitivity (Pelli‐Robson chart) at 6 months Secondary outcomes: (1) Visual acuity (Retro illuminated ETDRS chart) (2) Color vision (Farnsworth‐Munsell 100‐hue test) (3) Quality of life: (National Eye Institute Visual Function Questionnaire (NEI‐VFQ) ‐ administered 5 to 8 years after initial acute optic neuritis, at 10 to 12 years, and at 15 to 18 years after acute optic neuritis Adverse events reported: acute transient depression, acute pancreatitis, sleep disturbance, mild mood change, stomach upset, facial flushing, and weight gain Intervals at which outcomes were assessed: days 4, 15, 30; 7, 13, 19 weeks; 6, 12 months, then yearly. The data collected at the 6‐month visit was used as the major measurements of visual outcome data |
|
| Notes |
Study period: July 1, 1988 to June 30, 1991 Funding sources: cooperative agreements with the National Eye Institute, U.S. National Institutes of Health Declarations of interest: not reported Reported subgroup analyses: none reported Data provided by the Jaeb Center for Health Research in personal communication |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | “A permuted‐blocks design with a separate sequence for each clinical center was used to assign patients randomly in equal numbers to three treatment groups”. |
| Allocation concealment (selection bias) | Low risk | “Each bottle for the prednisone and placebo groups had a numbered envelope type sealed label, within which the actual contents of the bottle was identified for emergency purposes. On dispensing the medication a portion of the label was torn off and placed in the patient's chart.” |
| Masking (performance bias and detection bias) | Unclear risk | “Patients in the oral‐prednisone and placebo groups were blinded to their treatment assignment, whereas those in the intravenous‐methylprednisolone group were not”. “The personnel assessing visual function were always unaware of whether the patient was assigned to the placebo or prednisone group, and as often as possible they were unaware of whether the patient was receiving methylprednisolone”. “When examining visual function in the patients in the intravenous‐methylprednisolone group, technicians were unaware of the patient’s treatment assignment during 86 percent of all follow‐up visits overall and 94 percent of the six‐month visits”. “Upon completion of treatment, the portion of the label that had been removed was returned to the DCC, which verified that the correct bottle had been dispensed to the patient and that masking had not been compromised (i.e., label intact)”. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | “The overall rate of visits missed among the seven scheduled follow‐up visits in the first six months was 3.4 percent.” The reasons for missed follow‐up visits not reported. |
| Selective reporting (reporting bias) | Low risk | “Visual field and contrast sensitivity were the primary measures of outcome; visual acuity and color vision were secondary measures”. Outcomes reported as described in the methods section, though we did not have access to the original trial protocol. |
| Other bias | Unclear risk | Study medication provided by industry. |
Sellebjerg 1999.
| Study characteristics | ||
| Methods |
Study design: parallel group randomized controlled trial Number randomized: 60 total participants: 30 in steroid group and 30 in placebo group Exclusions after randomization: none Losses to follow up: 0 at 8 weeks; 1 from 8 weeks to 1 year: 1 in methylprednisolone group; 8 after 1 year: 4 in methylprednisolone group, 4 in placebo group Number analyzed (total and per group): 60 at 8 weeks: 30 in steroid group and 30 in placebo group Unit of analysis: participant Power calculation: "A formal power calculation was not performed, but based on the results obtained in a previous study, the 60 patients included in the trial were estimated to be sufficient to disclose a clinically relevant treatment effect because we assessed as efficacy measures changes from baseline rather than absolute values." |
|
| Participants |
Country: Denmark Age: 27 to 41 Gender: 23/60 (38.3%) men and 37/60 (61.7%) women Inclusion criteria: participants with optic neuritis; age 18 to 55 years; visual acuity of 0.7 or less (Snellen decimal fraction); duration of no more than 4 weeks Exclusion criteria: glucocorticoid treatment within 1 month of trial start; treatment with disease‐modifying drugs (e.g., interferons or cytotoxic drugs) within 6 months; pregnancy, lactation, other diseases precluding glucocorticoid treatment; any degree of subjective or objective remission Equivalence of baseline characteristics: yes |
|
| Interventions |
Intervention 1: methylprednisolone tablets 500 mg once daily for 5 days, tapering to 400, 300, 200, 100, 64, 48, 32, 16, 8 and 8 mg on each of the 10 following days Intervention 2: identical looking tablets for 15 days Length of follow‐up: 12 months |
|
| Outcomes |
Primary outcomes, as defined: (1) Spatial vision at 1, 3 weeks (2) VAS at 1, 3 weeks (3) The changes in spatial vision at 8 weeks (2) The changes in VAS scores at 8 weeks Secondary outcomes: (1) The changes in spatial vision, color vision and VAS scores (2) Normalization of the visual acuity, color vision and contrast sensitivity scores at the individual visits (3) An increase of 1 point in the visual functional system of Kurtzke’s Expanded Disability Status Scale based on clinical measurements Adverse events reported: gastrointestinal symptoms, insomnia, palpitations, dysphoria or euphoria, hot flashes, edema, musculoskeletal pain, acne, headache, unpleasant or metallic taste, weight gain Intervals at which outcome were assessed: 1, 3, 8 weeks and 12 months |
|
| Notes |
Study period: August 1993 to January 1997 Funding sources: grants from the Danish Multiple Sclerosis Society, the Johnsen Memorial Foundation, and Pharmacia & Upjohn Declarations of interest: not reported Reported subgroup analyses: yes, "… post hoc subgroup analyses suggested that patients with a more severe baseline visual deficit had a somewhat more pronounced response to high‐dose methylprednisolone treatment" |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | “Individual randomization in blocks of 10 was performed by the producer using a random numbers table. Consecutive patients were allocated to consecutive randomization numbers in each stratum”. |
| Allocation concealment (selection bias) | Low risk | “The treatment assignment of each patient was concealed in a numbered, sealed envelope at the department of neurology and was not opened by the investigators before all patients had completed the trial” |
| Masking (performance bias and detection bias) | Unclear risk | "The treatment assignment of each patient was concealed in a numbered, sealed envelope at the department of neurology and was not opened by the investigators before all patients had completed the trial." “Visual function was tested by a technician unaware of the clinical status of the patient”. |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | "Five patients in the methylprednisolone group and four placebo‐treated patients did not participate in the 1‐year follow‐up study. Follow‐up data on one patient from each treatment arm was censored because interferon treatment was initiated within 1 year", but the percentage is higher than 10%. "One patient in the methylprednisolone group discontinued treatment after 4 days due to nausea, migraine, and diarrhea. Another methylprednisolone‐treated patient discontinued treatment after 10 days due to heartburn, abdominal discomfort, palpitations, dysphoria, and insomnia. One patient in the placebo group discontinued treatment after 2 days due to vertigo, vomiting, and headache, presumably caused by a demyelinating lesion in the brainstem". Trial reported intention‐to‐treat analysis in the methods but performed available cases analyses. |
| Selective reporting (reporting bias) | Low risk | "The four primary efficacy measures were the spatial vision and VAS scores at the 1‐week and 3‐week visits". "Secondary outcome measures were changes in spatial vision, color vision, and VAS scores; normalization of the visual acuity, color vision, and contrast sensitivity scores at the individual visits; and an increase of one point in the visual functional system of Kurtzke’s Expanded Disability Status Scale (EDSS)". "The primary efficacy measures were chosen before unblinding. In patients with bilateral symptoms only, the results obtained in the eye with the worse baseline visual acuity were analyzed". |
| Other bias | Unclear risk | "Supported by grants from the Danish Multiple Sclerosis Society, the Johnsen Memorial Foundation, and Pharmacia & Upjohn." |
Tübingen Study 1993.
| Study characteristics | ||
| Methods |
Study design: parallel group RCT (44 participants) and non‐RCT (12 participants who selected treatment group) Number randomized: 44 total participants; 17 in prednisolone group and 27 in vitamin B1 group Exclusions after randomization: 6 due to poor adherence: 3 in prednisolone group and 3 in vitamin B1 group Losses to follow up: 3 at 6 months: 1 in prednisolone group and 2 in vitamin B1 group; 6 at 12 months: 3 in prednisolone group and 3 in vitamin B1 group Number analyzed: 35 RCT participants at 6 months (13 in prednisolone group and 22 in vitamin B1 group) plus 12 non‐RCT participants at 6 months (2 in prednisolone group and 10 in vitamin B1 group) Unit of analysis: participant How were missing data handled?: excluded from the analyses Power calculation: none reported |
|
| Participants |
Country: Germany Age: 30 years Gender: 14/50 (28%) men and 36/50 (72%) women Inclusion criteria: acute unilateral optic neuritis of presumed demyelinative origin; maximal disease duration of 3 weeks; without any improvement since onset; first attack in the involved eye/no previous history of ON; no previous treatment with corticosteroids; no acute symptoms of multiple sclerosis present Exclusion criteria: not reported Equivalence of baseline characteristics: yes |
|
| Interventions |
Intervention 1: oral methylprednisolone 100, 80, 60, 40, 30, 20, 10, 5 mg for 3 days each Intervention 2: oral vitamin B1 Length of follow‐up: follow up at 1, 2, 3, 4, 6, 8 weeks and 3, 4, 5, 6, 9, 12 months |
|
| Outcomes |
Primary and secondary outcomes were not differentiated Outcomes as reported: (1) Profile perimetry: a nearly normal level was reached when the light difference sensitivity was reduced by 2 to 3 decibel (2) Kinetic perimetry: was defined as normal when the isopter for 0.63 candela/m² was situated at 1 to 2 degree, the isopter for 1 candela/m² at 5 degree (3) Visual acuity: complete normalization was reached in 1.0 to 1.25 (20/20 to 20/16), nearly normal level was defined when it reached 0.8 (20/25) (4) Aulhorn flicker test: the flicker test result was categorized as nearly normal when the two criteria were no longer fulfilled Adverse events reported: acne Intervals at which outcomes were assessed: all participants were monitored for 1, 2, 3, 4, 6, 8 weeks and 3, 4, 5, 6, 9, 12 months for follow up; neurological examination was performed in the first week and after 3 months |
|
| Notes |
Study period: between 1980 and 1986 Funding sources: Hoechst and Goedecke/Parke‐Davis Pharma Industries and by H. and L. Schilling Foundation, TS 013/54/87 Declarations of interest: not reported Reported subgroup analyses: not performed; "A detailed analysis of these questions is not possible in this study, because when our group is divided into subgroups, the samples’ size becomes too small for statistical evaluation. The limitation by sample size is mainly due to the strict criteria for patient selection (see Methods) and to the fact that fewer patients are available in one single centre" |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | High risk | "In addition, 12 ON patients who refused to participate under double‐blind conditions, were treated in an unmasked manner, two with methylprednisolone and 10 with vitamin B1 according to their own choice." |
| Allocation concealment (selection bias) | High risk | "In addition, 12 ON patients who refused to participate under double‐blind conditions, were treated in an unmasked manner, two with methylprednisolone and 10 with vitamin B1 according to their own choice." |
| Masking (performance bias and detection bias) | High risk | “In addition, 12 ON patients who refused to participate under double‐blind conditions, were treated in an unmasked manner, two with methylprednisolone and 10 with vitamin B1 according to their own choice.” “In all patients their treatment assignment was not known during data evaluation.” |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Exclusion of 6 participants after randomization due to poor treatment compliance; 3 in corticosteroid arm (3/17) and 3 in placebo arm (3/27). |
| Selective reporting (reporting bias) | Low risk | Outcomes reported as described in the methods section, though we did not have access to the original trial protocol. |
| Other bias | High risk | Funded by pharmaceutical industry. There was a deviation from randomization: 12 participants chose the assignment according to their decision (2 in methylprednisolone group and 10 in vitamin B1 group). |
IV: intravenous IVMP: intravenous methylprednisolone RCT: randomized controlled trial MRI: magnetic resonance imaging VEP: visual evoked potential ETDRS: Early Treatment Diabetic Retinopathy Study HFA: Humphrey Field Analyzer VAS: visual analog scale
Characteristics of excluded studies [ordered by study ID]
| Study | Reason for exclusion |
|---|---|
| Al‐Eajailat 2014 | This article is a report of a trial with no clear information for randomization. Could not reach the author for further information |
| Alejandro 1994 | This article was translated and reviewed. It describes a study that examined two routes of administration of corticosteroids and hence is outside the scope of this review |
| Beran 1973 | This article is a retrospective comparison of those treated by glucocorticosteroids and foreign protein therapy |
| Bhatti 2005 | This article is a review with no additional trials |
| Bird 1976 | This article is a review and describes studies that were already reviewed by the authors of this study |
| Bowden 1974 | Evaluated adrenocorticotropic hormone, a precursor of corticosteroids |
| Brusa 1999 | This article examines a convenience sample from an RCT and hence does not satisfy the inclusion criteria for this review |
| Brusaferri 2000 | This article is a meta‐analysis of RCT on steroid treatment for optic neuritis. The articles included in this paper have already been reviewed by the authors of this review and determined not to contain additional data |
| Chuman 2004 | This article reports a discussion of one of the included trials |
| Gould 1977 | This trial originally was selected for inclusion in the review, but after further assessment we excluded it because of inadequate randomization method. This trial compared a single injection of triamcinolone into the orbit versus no injection |
| Hallermann 1983 | This study is not an RCT and hence does not satisfy the inclusion criteria for this review |
| Hickman 2002 | Trial was not initiated as per personal communication with Dr. Hickman |
| Kommerell 1994 | Summary and discussion of ONTT 1992‐2006 |
| Kott 1997 | The intervention 'copaxone' is an amino acid polymer, not a corticosteroid and hence outside the scope of this review |
| Midgard 2005 | This article was translated and was determined not to be an RCT (retracted literature review) |
| Park 2013 | This is a randomized controlled trial with 30 included patients, but the study compared retrobulbar triamcinolone injection versus treatment from conventional ONTT protocol, which is outside the scope of this review |
| Pirko 2004 | This is not an RCT; discusses natural history of optic neuritis |
| Rawson (1966‐69) | Evaluated adrenocorticotropic hormone, a precursor of corticosteroids |
| Roed 2005 | Compares interventions not eligible for inclusion in this review |
| Soderstrom 1995 | This article was translated; not an RCT |
| Toczolowski 1995 | This article was translated; not an RCT |
Characteristics of ongoing studies [ordered by study ID]
NCT01524250.
| Study name | Optic Neuritis Recovery After Oral or IV Corticosteroids |
| Methods |
Study design: RCT (parallel assignment) Estimated enrollment: 46 participants Study centers: London Health Sciences Center and St. Joseph's Health Care Center in London, Ontario, Canada Length of follow‐up: 6 months |
| Participants |
Inclusion criteria: age 18 to 65 years; unilateral acute demyelinating optic neuritis; within 14 days of symptom onset; visual acuity in study eye of 20/40 or better Exclusion criteria: received corticosteroids within 30 days; change in dose of any medication taken for comorbid conditions; any medical condition affecting visual acuity; history of optic neuritis in study eye |
| Interventions |
Intervention 1: 1250 mg oral prednisone daily for 3 days Intervention 2: 1000 mg IV methylprednisolone daily for 3 days |
| Outcomes |
Primary outcome, as defined: P100 latency of the Visual Evoked Potential in the study eye at 6 months
Secondary outcomes, as defined: high contrast visual acuity at one and six months; contrast sensitivity at one and six months; P100 latency of the Visual Evoked Potential in the study eye at one month Intervals at which outcomes to be assessed: one and six months post‐corticosteroid treatment |
| Starting date | March 2012 (estimated completion September 2016) |
| Contact information | Sarah A Morrow, MD, FRCPC, MSc; London Health Sciences Center |
| Notes | Funding source: London Health Sciences Centre and The Physicians' Services Incorporated Foundation |
NCT01838174.
| Study name | A Phase IV Trial of Neuroprotection With ACTH in Acute Optic Neuritis (ACTHAR) |
| Methods |
Study design: RCT (parallel assignment) Estimated enrollment: 60 participants Study centers: University of Texas Southwestern Medical Center; University of Colorado Denver Length of follow‐up: six months |
| Participants |
Inclusion criteria: age 18 to 55 years; diagnosed with clinically unilateral acute demyelinating optic neuritis; within 14 days of symptom onset prior to intended randomization; the qualifying episode of optic neuritis must be the first clinical episode of optic neuritis in the affected eye; ability to undergo treatment with intravenous methylprednisolone or Acthar gel Exclusion criteria: functionally or clinically relevant comorbidity of the affected eye; bilateral optic neuritis; concurrent functionally or clinically relevant disturbances of the eye not affected by acute demyelinating optic neuritis (ADON); high clinical likelihood of a form of optic neuritis other than ADON; non‐assessable ocular coherence tomography (OCT) at screening; refractive error greater than ±5 diopters or pre‐surgical value to be used for patients having undergone refractive surgery; an immune system disorder other than Multiple Sclerosis (MS) or ADON or with a known immunodeficiency syndrome; prior treatment with IV methylprednisolone (IVMP) or Acthar gel within the past 30 days; treatment with rituximab, mitoxantrone, cyclophosphamide, mycophenolate, azathioprine, alemtuzumab, ocrelizumab, or other non‐approved agents for the treatment of relapsing forms of MS; concurrent use of 4‐aminopyridine |
| Interventions |
Intervention 1: Acthar Gel (ACTH) 15 days of daily injections Intervention 2: IV steroids with oral taper (3 days of intravenous methylprednisolone followed by 11 days of oral taper, details for oral taper not provided) |
| Outcomes |
Primary outcome, as defined: retinal nerve fiber layer (RNFL) thickness at 6 months
Secondary outcomes, as defined: the frequency of optic nerves with RNFL swelling between the IV methylprednisolone‐treated and Acthar‐treated groups at 1 and 3 months Intervals at which outcomes to be assessed: at months 1, 3, and 6 |
| Starting date | May 2013 (estimated completion April 2015) |
| Contact information | Gina Remington, RN, BSN (214‐645‐0560; gina.remington@utsouthwestern.edu) |
| Notes | No funding source given |
IV: intravenous RCT: randomized controlled trial
Differences between protocol and review
Cochrane methodology regarding assessments of the risk of bias in included studies have been modified and the review authors updated the 'Assessment of risk of bias in included studies' section of the methods to reflect updated methodological considerations.
Contributions of authors
Conceiving the review: Kay Dickersin, Suzanne Brodney‐Folse (SBF) Designing the review: RB, RG, SBF Coordinating the review: SBF, SSV Data collection for the review ‐ Designing search strategies: RG, SBF, Karen Blackhall, Iris Gordon, Lori Rosman ‐ Undertaking searches: Karen Blackhall, Iris Gordon, Lori Rosman ‐ Screening search results: SBF, RG ‐ Organizing retrieval of papers: SBF, RG ‐ Screening retrieved papers against inclusion criteria: SBF, RG ‐ Appraising quality of papers: SBF, RG, SSV ‐ Extracting data from papers: SBF, RG ‐ Writing to authors of papers for additional information: SBF, SSV ‐ Providing additional data about papers: SBF, SSV ‐ Obtaining and screening data on unpublished studies: RG, SBF Data management for the review ‐ Entering data into RevMan: SBF, SSV ‐ Analysis of data: SBF, SSV, RG, RB Interpretation of data ‐ Providing a methodological perspective: SBF, RG, SSV, RB ‐ Providing a clinical perspective: RB ‐ Providing a policy perspective: RB ‐ Providing a consumer perspective: SBF, RG, SSV, RB Writing the review SBF, SSV, RG, RB Securing funding for the review SBF, RB, RG, SSV Guarantor for review: RG
Updating the review: RG, SSV, Cochrane Eyes and Vision Group US Project
Sources of support
Internal sources
Brown University, USA
Johns Hopkins University, USA
External sources
-
National Eye Institute, National Institutes of Health, US Department of Health and Human Services, Bethesda, MD, USA
Methodological support provided by the Cochrane Eyes and Vision Group US Project, cooperative agreement 1 U01 EY020522
-
National Institute of Health Research (NIHR), UK
Richard Wormald, Co‐ordinating Editor for the Cochrane Eyes and Vision Group (CEVG) acknowledges financial support for his CEVG research sessions from the Department of Health through the award made by the National Institute for Health Research to Moorfields Eye Hospital NHS Foundation Trust and UCL Institute of Ophthalmology for a Specialist Biomedical Research Centre for Ophthalmology.
The NIHR also funds the CEVG Editorial Base in London.
The views expressed in this publication are those of the authors and not necessarily those of the NIHR, NHS, or the Department of Health.
Declarations of interest
Roy Beck is the primary investigator for the Optic Neuritis Treatment Trial.
Edited (no change to conclusions)
References
References to studies included in this review
Kapoor 1998 {published data only}
- Hickman SJ, Kapoor R, Jones SJ, Altmann DR, Plant GT, Miller DH. Corticosteroids do not prevent optic nerve atrophy following optic neuritis. Journal of Neurology, Neurosurgery and Psychiatry 2003;74(8):1139-41. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Jones SJ, Miller DH, Kapoor R, Brusa A, Plant G. Double-blind controlled trial of methylprednisolone treatment for acute optic neuritis: 6-month follow-up with visual evoked potential measurement. Multiple Sclerosis 1996;2 Suppl:32-3. [Google Scholar]
- Kapoor R, Miller DH, Jones SJ, Plant GT, Brusa A, Gass A, et al. Effects of intravenous methylprednisolone on outcome in MRI-based prognostic subgroups in acute optic neuritis. Neurology 1998;50(1):230-7. [DOI] [PubMed] [Google Scholar]
Menon 2007 {published data only}
- Menon V, Mehrotra A, Saxena R, Jaffery NF. Comparative evaluation of megadose methylprednisolone with dexamethasone for treatment of primary typical optic neuritis. Indian Journal of Ophthalmology 2007;55(5):355-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
ONMRG 1999 {published data only}
- Tabuchi A, Kimura H, Inoue M. Optic neuritis treatment trial: Contrast sensitivity; assessment and results. Neuro-Ophthalmology Japan 1998;15(1):30-6. [Google Scholar]
- Wakakura M, Mashimo K, Oono S, Matsui Y, Tabuchi A, Kani K, et al. Multicenter clinical trial for evaluating methylprednisolone pulse treatment of idiopathic optic neuritis in Japan. Optic Neuritis Treatment Trial Multicenter Cooperative Research Group (ONMRG). Japanese Journal of Ophthalmology 1999;43(2):133-8. [DOI] [PubMed] [Google Scholar]
- Wakakura M, Minei Higa R, Oono S, Matsui Y, Tabuchi A, Kani K, et al. Baseline features of idiopathic optic neuritis as determined by a multicenter treatment trial in Japan. Optic Neuritis Treatment Trial Multicenter Cooperative Research Group (ONMRG). Japanese Journal of Ophthalmology 1999;43(2):127-32. [DOI] [PubMed] [Google Scholar]
ONTT 1992‐2006 {published data only}
- Beck R. The Optic Neuritis Treatment trial: three-year follow-up results. Archives of Ophthalmology 1995;113(2):136-7. [DOI] [PubMed] [Google Scholar]
- Beck RW, Cleary PA, Andersen MMJ, Keltner JL, Shults WT, Kaufman DI, et al. A randomized controlled trial of corticosteroids in the treatment of acute optic neuritis. The Optic Neuritis Study Group. New England Journal of Medicine 1992;326(9):581-8. [DOI] [PubMed] [Google Scholar]
- Beck RW, Cleary PA, Backlund JC. The course of visual recovery after optic neuritis. Experience of the Optic Neuritis Treatment Trial. Ophthalmology 1994;101(11):1771-8. [DOI] [PubMed] [Google Scholar]
- Beck RW, Cleary PA, Trobe JD, Kaufman DI, Kupersmith MJ, Paty DW, et al. The effect of corticosteroids for acute optic neuritis on the subsequent development of multiple sclerosis. New England Journal of Medicine 1993;329(24):1764-9. [DOI] [PubMed] [Google Scholar]
- Beck RW, Cleary PA. Optic neuritis treatment trial. One year follow-up results. Archives of Ophthalmology 1993;111(6):773-5. [DOI] [PubMed] [Google Scholar]
- Beck RW, Gal RL, Bhatti MT, Brodsky MC, Buckley EG, Chrousos GA, et al. Visual function more than 10 years after optic neuritis: experience of the Optic Neuritis Treatment Trial. American Journal of Ophthalmology 2004;137(1):77-83. [DOI] [PubMed] [Google Scholar]
- Beck RW, Gal RL, et al. Optic Neuritis Treatment Trial: 10-Year Follow-up Results - Reply. American Journal of Ophthalmology 2004;138(4):695. [DOI] [PubMed] [Google Scholar]
- Beck RW, Gal RL. Treatment of acute optic neuritis - A summary of findings from the Optic Neuritis Treatment Trial. Archives of Ophthalmology 2008;126(7):994-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Beck RW, Kupersmith MJ, Clearly PA, Katz B, The Optic Neuritis Study Group. Fellow eye abnormalities in acute unilateral optic neuritis - Experience of the Optic Neuritis Treatment Trial. Ophthalmology 1993;100(5):691-8. [DOI] [PubMed] [Google Scholar]
- Beck RW, Trobe JD. The Optic Neuritis Treatment Trial - Putting the results in perspective. Journal of Neuro-Ophthalmology 1995;15(3):131-5. [PubMed] [Google Scholar]
- Beck RW, Trobe JD. What we have learned from the Optic Neuritis Treatment Trial. Ophthalmology 1995;102(10):1504-8. [DOI] [PubMed] [Google Scholar]
- Chrousos GA, Kattah JC, Beck RW, Cleary PA. Side effects of glucocorticoid treatment. Experience of the Optic Neuritis Treatment Trial. JAMA 1993;269(16):2110-2. [PubMed] [Google Scholar]
- Cleary PA, Beck RW, Anderson MMJ, Kenny DJ, Backlund JY, Gilbert PR. Design, methods, and conduct of the Optic Neuritis Treatment Trial. Controlled Clinical Trials 1993;14(2):123-42. [DOI] [PubMed] [Google Scholar]
- Cleary PA, Beck RW, Bourque LB, Backlund JC, Miskala PH. Visual symptoms after optic neuritis - Results from the Optic Neuritis Treatment Trial. Journal of Neuro-Ophthalmology 1997;17(1):18-28. [DOI] [PubMed] [Google Scholar]
- Cole SR, Beck RW, Moke PS, Gal RL, Long DT. The National Eye Institute Visual Function Questionnaire: experience of the ONTT. The Optic Neuritis Treatment Trial. Investigative Ophthalmology and Visual Science 2000;41(5):1017-21. [PubMed] [Google Scholar]
- Keltner JK, Johnson CA, Cello KE, Dontchev M, Gal RL, Beck RW, et al. Visual field profile of optic neuritis - A final follow-up report from the Optic Neuritis Treatment Trial from baseline through 15 years. Archives of Ophthalmology 2010;128(3):330-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Keltner JK, Johnson CA, Spurr JO, Beck RW, the Optic Neuritis Study Group. Baseline visual field profile of optic neuritis - The experience of the Optic Neuritis Treatment Trial. Archives of Ophthalmology 1993;111(2):231-4. [DOI] [PubMed] [Google Scholar]
- Keltner JL, Johnson CA, Spurr JO, Beck RW. Comparison of central and peripheral visual field properties in the Optic Neuritis Treatment Trial. American Journal of Ophthalmology 1999;128(5):543-53. [DOI] [PubMed] [Google Scholar]
- Keltner JL, Johnson CA, Spurr JO, Beck RW. Visual field profile of optic neuritis. One year follow-up in the Optic Neuritis Treatment Trial. Archives of Ophthalmology 1994;112(7):946-53. [DOI] [PubMed] [Google Scholar]
- Long DT, Beck RW, Moke PS, Blair RC, Kip KE, Gal RL, et al. The SKILL card test in optic neuritis: experience of the Optic Neuritis Treatment Trial. Journal of Neuro-Ophthalmology 2001;21(2):124-31. [DOI] [PubMed] [Google Scholar]
- Noseworthy J. Corticosteroids for optic neuritis and subsequent development of multiple sclerosis. Annals of Neurology 1994;120(Suppl 3):61. [Google Scholar]
- Optic Neuritis Study Group. High- and low-risk profiles for the development of multiple sclerosis within 10 years after optic neuritis. Archives of Ophthalmology 2003;121(7):944-9. [DOI] [PubMed] [Google Scholar]
- Optic Neuritis Study Group. Multiple sclerosis risk after optic neuritis: final Optic Neuritis Treatment Trial follow-up. Archives of Neurology 2008;65(6):727-32. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Optic Neuritis Study Group. Neurologic impairment 10 years after optic neuritis. Archives of Neurology 2004;61(9):1386-9. [DOI] [PubMed] [Google Scholar]
- Optic Neuritis Study Group. The 5-year risk of MS after optic neuritis: Experience of the Optic Neuritis Treatment Trial. Neurology 1997;49(5):1404-13. [DOI] [PubMed] [Google Scholar]
- Optic Neuritis Study Group. Visual function 15 years after optic neuritis: a final follow-up report from the Optic Neuritis Treatment Trial. Ophthalmology 2008;115(6):1079-82. [DOI] [PubMed] [Google Scholar]
- Optic Neuritis Study Group. Visual function 5 years after optic neuritis: Experience of the Optic Neuritis Treatment Trial. Archives of Ophthalmology 1997;115(12):1545-52. [PubMed] [Google Scholar]
- Trobe JD, Arbor A, The Optic Neuritis Study Group. One-year results in the Optic Neuritis Treatment Trial. Neurology 1993;43:A280. [Google Scholar]
- Trobe JD, Beck RW, Moke PS, Cleary PA. Contrast sensitivity and other vision tests in the Optic Neuritis Treatment Trial. American Journal of Ophthalmology 1996;121(5):547-53. [DOI] [PubMed] [Google Scholar]
Sellebjerg 1999 {published data only}
- Frederiksen JL. A double-blind randomized study of oral prednisolone versus placebo in patients with acute optic neuritis. Canadian Journal of Neurological Sciences 1993;20(Suppl 4):Abstract no. 7-18-15. [Google Scholar]
- Sellebjerg F, Christiansen M, Jensen J, Frederiksen J. Immunological effects of oral high-dose methylprednisolone in acute optic neuritis and multiple sclerosis. European Journal of Neurology 2000;7(3):281-9. [DOI] [PubMed] [Google Scholar]
- Sellebjerg F, Jensen CV, Larsson HB, Frederiksen JL. Gadolinium-enhanced magnetic resonance imaging predicts response to methylprednisolone in multiple sclerosis. Multiple Sclerosis 2003;9(1):102-7. [DOI] [PubMed] [Google Scholar]
- Sellebjerg F, Nielsen HS, Frederiksen JL, Olesen J. A randomized, controlled trial of oral high-dose methylprednisolone in acute optic neuritis. Neurology 1999;52(7):1479-84. [DOI] [PubMed] [Google Scholar]
- Sellebjerg F, Schaldemose Nielsen H, Frederiksen JL, Olesen J. A placebo-controlled treatment trial of oral high-dose methylprednisolone in acute optic neuritis. Multiple Sclerosis 1998;4:381. [Google Scholar]
Tübingen Study 1993 {published data only}
- Katz B. The Tübingen Study on Optic Neuritis Treatment--a prospective, randomized and controlled trial. Survey of Ophthalmology 1994;39(3):262-3. [DOI] [PubMed] [Google Scholar]
- Trauzettel-Klosinski S, Aulhorn E, Diener HC, Minder C, Pfluger D. The influence of prednisolone on the course of optic neuritis. Results of a double-blind study [Der einfluss von prednisolon auf den verlauf der neuritis nervi optici. Ergebnisse einer doppelblindstudie]. Fortschritte Der Ophthalmologie 1991;88(5):490-501. [PubMed] [Google Scholar]
- Trauzettel-Klosinski S, Axmann D, Diener HC. The Tübingen Study on Optic Neuritis Treatment - A prospective, randomized and controlled trial. Clinical Vision Sciences 1993;8(4):385-94. [Google Scholar]
- Trauzettel-Klosinski S, Diener HC, Dietz K, Zrenner E. The effect of oral prednisolone on visual evoked potential latencies in acute optic neuritis monitored in a prospective, randomized, controlled study. Documenta Ophthalmologica 1996;91(2):165-79. [DOI] [PubMed] [Google Scholar]
- Trauzettel-Klosinski S. The Aulhorn flicker test: possibilities and limits. Its use in optic neuritis for diagnosis, differential diagnosis, monitoring the course of the disease, and assessing the effect of oral prednisolone. German Journal of Ophthalmology 1992;1(6):415-23. [PubMed] [Google Scholar]
References to studies excluded from this review
Al‐Eajailat 2014 {published data only}
- Al-Eajailat SM, Al-Madani Senior MV. The role of magnetic resonance imaging and visual evoked potential in management of optic neuritis. Pan African Medical Journal 2014;17:54. [DOI] [PMC free article] [PubMed] [Google Scholar]
Alejandro 1994 {published data only}
- Alejandro PM, Castanon Gonzalez JA, Miranda Ruiz R, Edgar Echeverria R, Adriana Montano M. Comparative treatment of acute optic neuritis with "boluses" of intravenous methylprednisolone or oral prednisone [Tratamiento comparativo de la neuritis optica aguda con "bolos" de metilprednisolona endovenosa o prednisona oral]. Gaceta Medica de Mexico 1994;130(4):227-30. [PubMed] [Google Scholar]
Beran 1973 {published data only}
- Beran V, Hradecka V, Kohoutova O. Comparison of stimulation therapy with glucocorticoid therapy in optic nerve inflammation [Porovnani popudove terapie s lecbou glukokortikoidy u zanetu zrakoveho nervu]. Ceskoslovenska Oftalmologie 1973;29(5):372-4. [PubMed] [Google Scholar]
Bhatti 2005 {published data only}
- Bhatti MT, Schmitt NJ, Beatty RL. Acute inflammatory demyelinating optic neuritis: current concepts in diagnosis and management. Optometry 2005;76(9):526-35. [DOI] [PubMed] [Google Scholar]
Bird 1976 {published data only}
- Bird AC. Treatment of acute optic neuritis. Transactions of the Ophthalmological Societies of the United Kingdom 1976;96(3):412-4. [PubMed] [Google Scholar]
Bowden 1974 {published data only}
- Bowden AN, Bowden PMA, Friedman AI, Perkin GD, Rose FC. A trial of corticotrophin gelatin injection in acute optic neuritis. Journal of Neurology, Neurosurgery and Psychiatry 1974;37(8):869-73. [DOI] [PMC free article] [PubMed] [Google Scholar]
Brusa 1999 {published data only}
- Brusa A, Jones SJ, Kapoor R, Miller DH, Plant GT. Long-term recovery and fellow eye deterioration after optic neuritis, determined by serial visual evoked potentials. Journal of Neurology 1999;246(9):776-82. [DOI] [PubMed] [Google Scholar]
Brusaferri 2000 {published data only}
- Brusaferri F, Candelise L. Steroids for multiple sclerosis and optic neuritis: a meta-analysis of randomized controlled clinical trials. Journal of Neurology 2000;247(6):435-42. [DOI] [PubMed] [Google Scholar]
Chuman 2004 {published data only}
- Chuman H. 41st Annual Meeting of the Japanese Neuro-Ophthalmology Society, Kyoto, Japan, December 12-13, 2003. Journal of Neuro-Ophthalmology 2004;24(2):170-4. [DOI] [PubMed] [Google Scholar]
Gould 1977 {published data only}
- Gould ES, Bird AC, Leaver PK, McDonald WI. Treatment of optic neuritis by retrobulbar injection of triamcinolone. British Medical Journal 1977;1(6075):1495-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
Hallermann 1983 {published data only}
- Hallermann W, Haller P, Krüger C, Schiemann M, Patzold U. Progress of optic neuritis with and without corticosteroid treatment. Findings in a long-term investigation with static perimetry. Fortschritte der Ophthalmologie 1983;80(1):30-4. [PubMed] [Google Scholar]
Hickman 2002 {published data only}
- Hickman S. NOON. Nitric oxide in optic neuritis: A phase I randomised double-blind study of rapid corticosteroid treatment of optic neuritis. National Research Register, UK 2002.
Kommerell 1994 {published data only}
- Kommerell G. Treatment of optic neuritis with corticosteroids. Discussion at the 10th Meeting of the International Neuro-ophthalmological Society (Freiburg 5 to 9 June 1994) [Die Behandlung der Neuritis nervi optici mit Kortikosteroiden. Diskussion bei der 10. Tagung der International Neuro-ophthalmological Society (Freiburg, 5. bis 9. Juni 1994)]. Klinische Monatsblatter Fur Augenheilkunde 1994;205(3):126-7. [PubMed] [Google Scholar]
Kott 1997 {published data only}
- Kott E, Kessler A, Biran S. Optic neuritis in multiple sclerosis patients treated with copaxone. Journal of Neurology 1997;244:S23-4. [Google Scholar]
Midgard 2005 {published data only}
- Midgard R, Seland JH, Hovdal H, Celius EG, Eriksen K, Jensen D, et al. Optic neuritis: diagnosis, treatment and follow-up. Tidsskrift for Den Norske Laegeforening 2005;125(4):425-8. [PubMed] [Google Scholar]
- Midgard R, Seland JH, Hovdal H, Celius EG, Eriksen K, Jensen D, et al. Retraction of article [Tilbaketrekking av artikkel.]. Tidsskrift for den Norske Laegeforening 2005;125(15):2056. [PubMed]
Park 2013 {published data only}
- Park JH, Shin JP, Chun BY. Additional retrobulbar triamcinolone acetonide injection for retrobulbar optic neuritis patients. Journal of the Korean Ophthalmological Society 2013;54(1):117-22. [Google Scholar]
Pirko 2004 {published data only}
- Pirko I, Blauwet LK, Lesnick TG, Weinshenker BG. The natural history of recurrent optic neuritis. Archives of Neurology 2004;61(9):1401-5. [DOI] [PubMed] [Google Scholar]
Rawson (1966‐69) {published data only}
- Rawson M, Liversedge LA, Goldfarb G. Treatment of acute retrobulbar neuritis with corticotrophin. Lancet 1966;2(7472):1044-6. [DOI] [PubMed] [Google Scholar]
- Rawson MD, Liversedge LA. Treatment of retrobulbar neuritis with corticotrophin. Lancet 1969;294(7613):222. [DOI] [PubMed] [Google Scholar]
Roed 2005 {published data only}
- Roed HG, Langkilde A, Sellebjerg F, Lauritzen M, Bang P, Morup A, et al. A double-blind randomized trial of IV immunoglobulin treatment in acute optic neuritis. Neurology 2005;64(5):804-10. [DOI] [PubMed] [Google Scholar]
Soderstrom 1995 {published data only}
- Soderstrom M. Corticosteroids and acute optic nerve neuritis. A therapeutic method requiring further studies. [Kortikosteroider och akut opticusneurit. Behandlingsmetod kräver ytterligare studier]. Lakartidningen 1995;92(5):387-90. [PubMed] [Google Scholar]
Toczolowski 1995 {published data only}
- Toczolowski J, Lewandowska-Furmanik M, Stelmasiak Z, Wozniak D, Chmiel M. Treatment of acute optic neuritis with large doses of corticosteroids [Leczenie ostrego zapalenia nerwu wzrokowego za pomoca duzych dawek kortykosterydow]. Klinika Oczna 1995;97(5):122-5. [PubMed] [Google Scholar]
References to ongoing studies
NCT01524250 {unpublished data only}
- NCT01524250. Optic neuritis recovery after oral or IV corticosteroids. clinicaltrials.gov/ct2/show/NCT01524250 (accessed 11 June 2015).
NCT01838174 {unpublished data only}
- NCT01838174. A phase IV trial of neuroprotection with ACTH in acute optic neuritis (ACTHAR). clinicaltrials.gov/ct2/show/NCT01838174 (accessed 11 June 2015).
Additional references
Beck 1998
- Beck RW. Optic Neuritis. In: Miller NR, Newman NJ, editors(s). Walsh and Hoyt's Neuro-ophthalmology. 5th edition. Baltimore: Williams and Wilkins, 1998:599-647. [Google Scholar]
Bennett 2014
- Bennett JL, Nickerson M, Costello F, Sergott RC, Calkwood JC, Galetta SL, et al. Re-evaluating the treatment of acute optic neuritis. Journal of Neurology, Neurosurgery and Psychiatry 2015;86(7):799-808. [DOI] [PMC free article] [PubMed] [Google Scholar]
de la Cruz 2006
- la Cruz J, Kupersmith MJ. Clinical profile of simultaneous bilateral optic neuritis in adults. British Journal of Ophthalmology 2006;90(5):551-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
Ebers 1985
- Ebers GC. Optic neuritis and multiple sclerosis. Archives of Neurology 1985;42(7):702-4. [DOI] [PubMed] [Google Scholar]
Fleishman 1987
- Fleishman JA, Beck RW, Linares OA, Klein JW. Deficits in visual function after resolution of optic neuritis. Ophthalmology 1987;94(8):1029-35. [DOI] [PubMed] [Google Scholar]
Glanville 2006
- Glanville JM, Lefebvre C, Miles JN, Camosso-Stefinovic J. How to identify randomized controlled trials in MEDLINE: ten years on. Journal of the Medical Library Association 2006;94(2):130-6. [PMC free article] [PubMed] [Google Scholar]
Higgins 2011
- Higgins JPT, Altman DG, Sterne JAC (editors). Chapter 8: Assessing risk of bias in included studies. In: Higgins JPT, Green S (editors). Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 (updated March 2011). The Cochrane Collaboration, 2011. Available from www.cochrane-handbook.org.
Koch‐Henriksen 1988
- Koch-Henriksen N, Hyllested K. Epidemiology of multiple sclerosis: incidence and prevalence rates in Denmark 1948-64 based on the Danish Multiple Sclerosis Registry. Acta Neurologica Scandinavica 1988;78(5):369-80. [DOI] [PubMed] [Google Scholar]
Kurtzke 1985
- Kurtzke JF. Optic neuritis or multiple sclerosis. Archives of Neurology 1985;42(7):704-10. [DOI] [PubMed] [Google Scholar]
Lightman 1987
- Lightman S, McDonald WI, Bird AC, Francis DA, Hoskins A, Batchelor JR, et al. Retinal venous sheathing in optic neuritis. Its significance for the pathogenesis of multiple sclerosis. Brain 1987;110(Pt 2):405-14. [DOI] [PubMed] [Google Scholar]
Mangione 1998
- Mangione CM, Lee PP, Pitts J, Gutierrez P, Berry S, Hays RD, et al. Psychometric properties of the National Eye Institute Visual Function Questionnaire (NEI-VFQ). NEI-VFQ. Archives of Ophthalmology 1998;116(11):1496-504. [DOI] [PubMed] [Google Scholar]
RevMan 2014 [Computer program]
- The Nordic Cochrane Centre, The Cochrane Collaboration Review Manager (RevMan). Version 5.3. Copenhagen: The Nordic Cochrane Centre, The Cochrane Collaboration, 2014.
Rodriguez 1995
- Rodriguez M, Siva A, Cross SA, O'Brien PC, Kurland LT. Optic neuritis: a population-based study in Olmsted County, Minnesota. Neurology 1995;45(2):244-50. [DOI] [PubMed] [Google Scholar]
Sanders 1986
- Sanders EA, Volkers AC, Poel JC, Lith GH. Estimation of visual function after optic neuritis: a comparison of clinical tests. British Journal of Ophthalmology 1986;70(12):918-24. [DOI] [PMC free article] [PubMed] [Google Scholar]
Spoor 1988
- Spoor TC, Rockwell DL. Treatment of optic neuritis with intravenous megadose corticosteroids. A consecutive series. Ophthalmology 1988;95(1):131-4. [DOI] [PubMed] [Google Scholar]
Toosy 2014
- Toosy AT, Mason DF, Miller DH. Optic neuritis. Lancet Neurology 2104;13(1):83-99. [DOI] [PubMed] [Google Scholar]
References to other published versions of this review
Gal 2002
- Gal R, Brodney-Folse S, Beck R. Corticosteroids for treating optic neuritis. Cochrane Database of Systematic Reviews 2002, Issue 3. Art. No: CD001430. [DOI: 10.1002/14651858.CD001430] [DOI] [PMC free article] [PubMed] [Google Scholar]
Gal 2012
- Gal RL, Vedula SS, Beck R. Corticosteroids for treating optic neuritis. Cochrane Database of Systematic Reviews 2012, Issue 4. Art. No: CD001430. [DOI: 10.1002/14651858.CD001430.pub3] [DOI] [PMC free article] [PubMed] [Google Scholar]
Vedula 2007
- Vedula SS, Brodney Folse S, Gal RL, Beck R. Corticosteroids for treating optic neuritis. Cochrane Database of Systematic Reviews 2007, Issue 1. Art. No: CD001430. [DOI: 10.1002/14651858.CD001430.pub2] [DOI] [PMC free article] [PubMed] [Google Scholar]