

Abstract
Background
Despite its beneficial role on insulin resistance and atherosclerosis, adiponectin has been repeatedly reported as an independent positive predictor of cardiovascular mortality.
Methods
A Mendelian randomization approach was used, in order to evaluate whether such counterintuitive association recognizes a cause-effect relationship. To this purpose, single nucleotide polymorphism rs822354 in the ADIPOQ locus which has been previously associated with serum adiponectin at genome-wide level, was used as an instrument variable. Our investigation was carried out in the Gargano Heart Study-prospective design, comprising 356 patients with type 2 diabetes, in whom both total and high molecular weight (HMW) adiponectin were measured and cardiovascular mortality was recorded (mean follow-up = 5.4 ± 2.5 years; 58 events/1922 person-year).
Results
The A allele of rs822354 was associated with both total and HMW adiponectin [β (SE) = 0.10 (0.042), p = 0.014 and 0.17 (0.06), p = 0.003; respectively]. In a Poisson model comprising age, sex, smoking habits, BMI, HbA1c, total cholesterol, HDL-cholesterol, triglycerides, insulin therapy and hypertension, both rs822354 (IRR = 1.94, 95 % CI 1.23–3.07; p = 0.005), as well as the genetic equivalent of total adiponectin change (IRR = 1.07, 95 % CI 1.02–1.12; p = 0.003) were significantly associated with cardiovascular mortality. The observed genetic effect was significantly greater than that exerted by the genetic equivalent change of serum adiponectin (p for IRR heterogeneity = 0.012). In the above-mentioned adjusted model, very similar results were obtained when HMW, rather than total, adiponectin was used as the exposure variable of interest.
Conclusions
Our data suggest that the paradoxical association between high serum adiponectin levels and increased cardiovascular mortality rate is based on a cause-effect relationship, thus pointing to an unexpected deleterious role of adiponectin action/metabolism on atherosclerotic processes.
Keywords: Adiponectin, ADIPOQ, Mortality, Mendelian randomization, Type 2 diabetes
Background
Despite insulin-sensitizing, anti-inflammatory and endothelial protective effects [1–4], adiponectin is an independent positive predictor of cardiovascular (CV) mortality in the general population [5] as well as several clinical sets [6–15] including type 2 diabetes (T2D) [16]. Because of such paradox, it is logical to suspect that high adiponectin rather than being a true risk factor is simply a marker of other metabolic disturbances, which, in fact, are able to causally shape the risk of CV mortality.
Genetic variants, which are robustly associated with a given modifiable variable, are strong and easy-to-use tools for assessing if causality underlines the association between that variable, used as an exposure, and outcomes of interest [17–19]. In our case, if genetic variants, firmly associated with circulating adiponectin levels, prove to be also associated with CV death, a strong case is made in favor of a causal role of adiponectin on CV mortality.
We and others have recently reported that single nucleotide polymorphism (SNP) rs822354, located in the locus of ADIPOQ, the gene which encodes for adiponectin [20], is associated with serum adiponectin at genome-wide level of statistical significance [21, 22].
Based on this background, we used rs822354 as an instrumental variable to investigate the causal nature of the counterintuitive independent association between adiponectin and CV mortality we have previously reported in patients with T2D [16].
Methods
Study population
Gargano Heart Study (GHS)-prospective design
This study comprises 368 patients with T2D (ADA 2003 criteria) and coronary artery disease (CAD) who were consecutively recruited at the Endocrine Unit of IRCCS “Casa Sollievo della Sofferenza” in San Giovanni Rotondo (Gargano, Center East Coast of Italy) from 2001 to 2008, as recently described [16, 23, 24]. All patients had either a stenosis >50 % in at least one coronary major vessel at coronary angiography or a previous myocardial infarction (MI). Follow-up information on outcomes was collected yearly from 2002 to 2011. The only exclusion criterion was the presence of poor life expectancy for non diabetes-related diseases. The end-point was CV mortality. Confirmation of the event was obtained from death certificates (i.e. according to the international classification of diseases’ codes: 428.1—ninth edition- and I21.0–21.9, I25.9, I46.9–50.9, I63.0, I63.9, I70.2-tenth edition). Clinical data at baseline were obtained from a standardized interview and examination. Smoking habits and history of hypertension, dyslipidemia and MI as well as glucose-lowering treatment were also recorded at time of examination. Data regarding medications were confirmed by review of medical records.
Serum total and high-molecular weight (HMW) adiponectin and genotyping of SNP rs822354 were assessed in 356 (96.7 %) participants.
The study was approved by the Institutional Ethic Committee IRCCS “Casa Sollievo della Sofferenza”, San Giovanni Rotondo.
Measurement of circulating total adiponectin levels
Serum total and HMW adiponectin concentrations were measured by ELISA (Alpco, Salem, NH) as previously described [25, 26]. The intra-assay coefficients of variation were 5.4 and 4.9, and 5.0 and 4.8 % for total adiponectin and HMW adiponectin, respectively [16].
Genotyping
SNP rs822354 was genotyped by Taqman SNP allelic discrimination technique by means of an ABI 7000 (Applied Biosystems, Foster City, CA). Call rate and concordance rate were ≥96 and >99 %, respectively. The SNP was in Hardy–Weinberg equilibrium (HWE) (p > 0.05).
Statistical methods
Patients’ baseline characteristics were reported as mean ± standard deviation (SD) and percentages for continuous and categorical variables, respectively. Deviation from HWE of the rs822354 was investigated by exact χ2 test.
Univariable linear regression analysis was performed to model the effect of the rs822354 polymorphism (assuming an additive genetic model of inheritance) on adiponectin levels (expressed in terms of log transformed because of its non-normal distribution) and results were reported as regression coefficient β (standard error, SE).
The time variable was defined as the time between the baseline examination and date of the event (CV mortality), or, for subjects who did not experience the event, the date of the last available clinical follow-up. Incidence rate (IR) for CV mortality was expressed as the number of events per total number of 100 person-years (py).
To estimate the causal effect of adiponectin levels on CV mortality, we performed mediation analyses using SNP rs822354 as instrumental variable.
Poisson regression models were performed to assess the association between rs822354 (per one risk allele increase), adiponectin values and the event occurrence. Risks were reported as incidence rate ratio (IRR) along with 95 % confidence interval (95 % CI).
Such models were used to estimate the effect size per minor allele of rs822354 polymorphism on adiponectin levels (β1) and on CV mortality (β2), and the effect size of adiponectin levels (rescaled by β1) on CV mortality (β3). Mendelian randomization holds if β2 and β3 are not statistically different. To test such difference, we introduced a bivariate generalized linear model with Poisson distribution, which allowed to simultaneously estimate both adjusted models (CV mortality vs. SNP rs822354 and CV mortality vs. adiponectin levels), using an appropriate statistical contrast.
Our sample size of 356 patients achieved a statistical power of 80 % (two-sided type I error rate = 0.05) to detect an allelic IRR on CV mortality at least equal to 1.70, given its annual IR of 3 % and a risk allele frequency of 0.37 we observed in our sample.
Two-sided p values <0.05 were considered for statistical significant.
All analyses were performed using SPSS version 15.0 (Chicago, IL) and SAS release 9.3 (SAS Institute, Cary, NC).
Results
Clinical features of patients from GHS are summarized in Table 1. During follow-up (5.4 ± 2.5 years), 58 CV deaths occurred, corresponding to an overall annual IR of 3.0 % (58 events/1922 py).
Table 1.
Baseline clinical characteristics of participants from GHS (N = 356)
| Males (%) | 67.4 |
| Age (years) | 64.5 ± 8.2 |
| Smokers (%) | 63 (17.7) |
| BMI (kg/m2) | 30.2 ± 4.8 |
| HbA1C (%) | 8.6 ± 1.9 |
| Total cholesterol (mg/dl) | 176.0 ± 45.8 |
| HDL-cholesterol (mg/dl) | 43.6 ± 14.6 |
| Tryglicerides (mg/dl) | 152.3 ± 91.8 |
| Insulin w/wh oral agents (%) | 192 (54.0) |
| Hypertension (%) | 302 (84.8) |
| HMW-adiponectin (µg/ml) | 3.1 ± 2.5 |
| Total adiponectin (µg/ml) | 4.9 ± 2.9 |
Continuous variables were reported as mean ± SD whereas categorical variables as total frequency and percentages
GHS Gargano heart study, BMI body mass index, HbA1c glycated haemoglobin A1c HDL-cholesterol high density lipoprotein-cholesterol, HMW-adiponectin high molecular weight-adiponectin
In these patients, the A allele of rs822354 was significantly associated with total adiponectin (β (SE) = 0.10 (0.042); p = 0.014). In addition, in a model comprising several variables relevant to the risk of death, including age, sex, smoking habits, BMI, HbA1c, total cholesterol, HDL-cholesterol, triglycerides, insulin therapy and hypertension, both the same allele at rs822354 (IRR = 1.94, 95 % CI 1.23–3.07; p = 0.005), as well as the genetic equivalent of total adiponectin change (IRR = 1.07, 95 % CI 1.02–1.12; p = 0.003), were significantly associated with CV mortality. Of note, the observed genetic effect was significantly greater than that exerted by the genetic equivalent change of serum adiponectin (i.e. change per one rs822354 allele) (p for IRR heterogeneity = 0.012) (Fig. 1a).
Fig. 1.
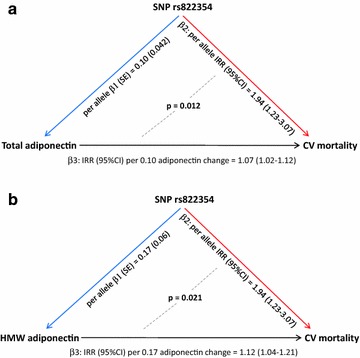
a Instrumental variable analysis for total adiponectin circulating levels. β1 effect size of association between each minor allele of rs822354 and total adiponectin levels; β2 effect size of association between each minor allele of SNP rs822354 and CV mortality; β3 effect size of association between change of total adiponectin levels attributable to the effect of rs822354 (i.e. genetic equivalent of total adiponectin change) and CV mortality. b Instrumental variable analysis for HMW adiponectin circulating levels. β1 effect size of association between each minor allele of rs822354 and HMW adiponectin levels; β2 effect size of association between each minor allele of SNP rs822354 and CV mortality; β3 effect size of association between change of HMW adiponectin levels attributable to the effect of rs822354 (i.e. genetic equivalent of HMW adiponectin change) and CV mortality
Similarly, rs822354 was associated with HMW adiponectin (β (SE) = 0.17 (0.06); p = 0.003), whose genetic equivalent change was, in turn, associated with CV mortality (adjusted IRR = 1.12, 95 % CI 1.04–1.21; p = 0.003). Also in this case, the association of CV mortality with either rs822354 or the genetic equivalent change of serum HMW adiponectin was significantly different (p for IRR heterogeneity = 0.021) (Fig. 1b).
Discussion
Many cardiovascular risk factors recognize a genetic background [27–29]. Beside unraveling new pathogenic pathways, such genetic markers may be used as a tool for addressing the intrinsic nature underlying the relationship between metabolic variables and a given outcome of interest, an approach known as Mendelian randomization [30, 31].
Our data clearly show that the A allele of SNP rs822354 (in the ADIPOQ locus, which encodes for adiponectin [20]), is associated not only with high serum adiponectin levels (both total and HMW isoform), but also and most importantly with high CV mortality rate.
This finding is perfectly in line with a previous study showing that the G allele of SNP rs4783244 (in CDH13, encoding for the HMW adiponectin receptor T-cadherin [32]) is associated with both high HMW adiponectin levels [33–35] and increased mortality rate [35].
Although the exact mechanism through which SNP rs4783244 (or others in linkage disequilibrium, LD, with it) affects serum adiponectin is a matter of debate [33, 34], previous [35] and our present findings strongly suggest that the paradoxical association between increased mortality risk and high serum adiponectin, rather than recognizing the latter as only a marker of yet unknown biologically-unlinked abnormalities, is explained by a causal, deleterious effect of adiponectin action and/or metabolism [36, 37] on mortality rate.
Given the well-known beneficial effect of adiponectin on several metabolic and vascular phenotypes [4, 38–40], the intrinsic biological nature underlying such deleterious effect(s) is difficult to understand or even only to speculate; otherwise, we would not be talking of “paradoxical effect/association”. Having acknowledge this, some deleterious actions of adiponectin on processes possibly involved in atherogenesis, including stimulatory effect on secretion of pro-atherogenic cytokines [41–43] and angiogenesis [42, 44], have been recently reported in specific cell types. Whether such effects are observable also in human tissues involved in atherogenesis and whether they may play a role in increasing atherosclerotic processes is a possibility that deserves further, specifically designed studies, to be addressed. As a matter of fact, the available literature on the association with human traits does not unequivocally point to adiponectin as a metabolic and vascular protecting hormone. In fact, while low adiponectin has been associated with obesity, metabolic syndrome [39], some macro- and micro-vascular damages [38, 40] and T2D [39], so to make reasonable hypothesize that drugs activating adiponectin signaling pathways improve all the above mentioned metabolic and vascular disturbances [4], on the other hand, adiponectin levels are positively associated with subclinical atherosclerosis in patients with type 1 diabetes [45] and with all-cause mortality in patients with T2D [46, 47].
An additional, unexpected, finding of our study is that the association between SNP rs822354 and CV mortality is stronger than that expected if it would be entirely mediated by serum adiponectin changes. Such discrepancy might be due to the difference between a totally stable genetic effect, operating since birth on one hand and, conversely the role exerted by serum adiponectin, whose levels are quite variable [48, 49], especially in heavily treated patients as are those with T2D [50, 51], and whose effect has been evaluated only for a few years. As an alternative explanation, we cannot exclude that, beside the role on serum adiponectin, rs822354 exerts additional, distinct (i.e. pleiotropic) effects through other risk factors, which either we cannot account for or are still unknown. At this regard, it is of note that although neither rs822354, nor other SNPs in high LD with it, are associated with CV traits in humans [52, 53], it is located in the 3q27.3 region close to KNG1, a potential contributor in shaping CV risk [54]. In fact, KNG1 encodes for high molecular weight kininogen, the precursor of bradykinin and kallidin, belonging to the pathway activating coagulation factors XI and XII [55] and interrelated with the renin–angiotensin–aldosterone system [56].
We like to acknowledge some limitations of our study. Firstly, the sample we analyzed comprises only 356 individuals, so that the strength of the novel association we here report (i.e. between rs822354 and CV mortality) does not reach genome-wide level of statistical significance. In addition, we lack a second, independent sample on which to replicate our finding. In all, although we cannot exclude the possibility of a false positive result, our study plays the important role of hypothesis generating, thus representing a solid background on which further similar studies can be based on.
Conversely, strengths of our study are the deep clinical phenotyping and the genetic and environmental homogeneity of our sample recruited in a well-defined geographical region. In addition, also the determination of both total and HMW adiponectin, which allowed us to confirm our finding also with the biological active isoform of adiponectin [57], reinforces our study.
Finally, the observation that among community-dwelling Japanese individuals [35], a genetic marker of adiponectin levels is associated with all-cause mortality, suggests that our present finding is generalizable across different ethnicities and is not restricted to CV mortality in the specific subset of patients with T2D.
Conclusions
In conclusion, our present and previous [35] data suggest that adiponectin action/metabolism paradoxically causes increased CV mortality risk. Further studies are needed before this unexpected finding may be considered as established.
Authors’ contributions
LOM, VT and CM participated in study concept and design, acquisition of data, interpretation of results and drafted the manuscript. LOM, MC and AF participated in statistical analysis. CDB and LS provided essential data for analyses. VT and CM are the guarantor of this work and, as such, had full access to all the data in the study and takes responsibility for the integrity of the data and the accuracy of the data. All authors read and approved the final version of the manuscript.
Acknowledgements
We are indebted to the staffs and participants of the GHS for their dedication and contributions. This study was supported by Accordo Programma Quadro in Materia di Ricerca Scientifica nella Regione Puglia-PST 2006 and PO Puglia FESR 2007-2013, Italian Ministry of Health grants RC2011, RC2012, RC2013, RC2014, RC2015, EFSD/Pfizer grant and SID-FO.DI.RI and Italian Ministry of Health RF-2013-02356459 (CM). Dr. Ortega Moreno was supported by a Grant from Società Italiana di Diabetologia-Fondazione Diabete Ricerca.
Competing interests
The authors declare that they have no competing interests.
Abbreviations
- BMI
body mass index
- CV
cardiovascular
- GHS
Gargano heart study
- HbA1c
glycated haemoglobin
- HMW
high molecular weight
- HWE
Hardy Weinberg equilibrium
- IR
incidence rate
- LD
linkage disequilibrium
- MI
myocardial infarction
- py
person-year
- SNP
single-nucleotide polymorphism
- T2D
type 2 diabetes
Footnotes
Vincenzo Trischitta and Claudia Menzaghi equally supervised the entire study
Contributor Information
Lorena Ortega Moreno, Email: l.ortega@operapadrepio.it.
Massimiliano Copetti, Email: m.copetti@operapadrepio.it.
Andrea Fontana, Email: a.fontana@operapadrepio.it.
Concetta De Bonis, Email: c.debonis@operapadrepio.it.
Lucia Salvemini, Email: l.salvemini@operapadrepio.it.
Vincenzo Trischitta, Email: vincenzo.trischitta@uniroma1.it.
Claudia Menzaghi, Phone: ++390882416276, Email: c.menzaghi@operapadrepio.it.
References
- 1.Kadowaki T, Yamauchi T. Adiponectin and adiponectin receptors. Endocr Rev. 2005;26(3):439–451. doi: 10.1210/er.2005-0005. [DOI] [PubMed] [Google Scholar]
- 2.Turer AT, Scherer PE. Adiponectin: mechanistic insights and clinical implications. Diabetologia. 2012;55(9):2319–2326. doi: 10.1007/s00125-012-2598-x. [DOI] [PubMed] [Google Scholar]
- 3.De Cosmo S, Menzaghi C, Prudente S, Trischitta V. Role of insulin resistance in kidney dysfunction: insights into the mechanism and epidemiological evidence. Nephrol Dial Transplant. 2013;28(1):29–36. doi: 10.1093/ndt/gfs290. [DOI] [PubMed] [Google Scholar]
- 4.Fisman EZ, Tenenbaum A. Adiponectin: a manifold therapeutic target for metabolic syndrome, diabetes, and coronary disease? Cardiovasc Diabetol. 2014;13:103. doi: 10.1186/1475-2840-13-103. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Dekker JM, Funahashi T, Nijpels G, Pilz S, Stehouwer CD, Snijder MB, et al. Prognostic value of adiponectin for cardiovascular disease and mortality. J Clin Endocrinol Metab. 2008;93(4):1489–1496. doi: 10.1210/jc.2007-1436. [DOI] [PubMed] [Google Scholar]
- 6.Cavusoglu E, Ruwende C, Chopra V, Yanamadala S, Eng C, Clark LT, et al. Adiponectin is an independent predictor of all-cause mortality, cardiac mortality, and myocardial infarction in patients presenting with chest pain. Eur Heart J. 2006;27(19):2300–2309. doi: 10.1093/eurheartj/ehl153. [DOI] [PubMed] [Google Scholar]
- 7.Pilz S, Mangge H, Wellnitz B, Seelhorst U, Winkelmann BR, Tiran B, et al. Adiponectin and mortality in patients undergoing coronary angiography. J Clin Endocrinol Metab. 2006;91(11):4277–4286. doi: 10.1210/jc.2006-0836. [DOI] [PubMed] [Google Scholar]
- 8.Wannamethee SG, Whincup PH, Lennon L, Sattar N. Circulating adiponectin levels and mortality in elderly men with and without cardiovascular disease and heart failure. Arch Intern Med. 2007;167(14):1510–1517. doi: 10.1001/archinte.167.14.1510. [DOI] [PubMed] [Google Scholar]
- 9.Poehls J, Wassel CL, Harris TB, Havel PJ, Swarbrick MM, Cummings SR, et al. Association of adiponectin with mortality in older adults: the health, aging, and body composition study. Diabetologia. 2009;52(4):591–595. doi: 10.1007/s00125-009-1261-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Wannamethee SG, Welsh P, Whincup PH, Sawar N, Thomas MC, Gudnarsson V, et al. High adiponectin and increased risk of cardiovascular disease and mortality in asymptomatic older men: does NT-proBNP help to explain this association? Eur J Cardiovasc Prev Rehabil. 2011;18(1):65–71. doi: 10.1097/HJR.0b013e32833b09d9. [DOI] [PubMed] [Google Scholar]
- 11.Kizer JR, Benkeser D, Arnold AM, Mukamal KJ, Ix JH, Zieman SJ, et al. Associations of total and high-molecular-weight adiponectin with all-cause and cardiovascular mortality in older persons: the cardiovascular health study. Circulation. 2012;126(25):2951–2961. doi: 10.1161/CIRCULATIONAHA.112.135202. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Lindberg S, Pedersen SH, Møgelvang R, Bjerre M, Frystyk J, Flyvbjerg A, et al. Usefulness of adiponectin as a predictor of all cause mortality in patients with ST-segment elevation myocardial infarction treated with primary percutaneous coronary intervention. Am J Cardiol. 2012;109(4):492–496. doi: 10.1016/j.amjcard.2011.09.041. [DOI] [PubMed] [Google Scholar]
- 13.Persson J, Folkersen L, Ekstrand J, Helleberg J, Gabrielsen A, Lundman P, et al. High plasma adiponectin concentration is associated with all-cause mortality in patients with carotid atherosclerosis. Atherosclerosis. 2012;225(2):491–496. doi: 10.1016/j.atherosclerosis.2012.09.036. [DOI] [PubMed] [Google Scholar]
- 14.Lee ES, Park SS, Kim E, Yoon YS, Ahn HY, Park CY, et al. Association between adiponectin levels and coronary heart disease and mortality: a systematic review and meta-analysis. Int J Epidemiol. 2013;42(4):1029–1039. doi: 10.1093/ije/dyt087. [DOI] [PubMed] [Google Scholar]
- 15.Wu ZJ, Cheng YJ, Gu WJ, Aung LH. Adiponectin is associated with increased mortality in patients with already established cardiovascular disease: a systematic review and meta-analysis. Metabolism. 2014;63(9):1157–1166. doi: 10.1016/j.metabol.2014.05.001. [DOI] [PubMed] [Google Scholar]
- 16.Menzaghi C, Xu M, Salvemini L, De Bonis C, Palladino G, Huang T, et al. Circulating adiponectin and cardiovascular mortality in patients with type 2 diabetes mellitus: evidence of sexual dimorphism. Cardiovasc Diabetol. 2014;13:130. doi: 10.1186/s12933-014-0130-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Smith GD, Ebrahim S. Mendelian randomization: prospects, potentials, and limitations. Int J Epidemiol. 2004;33(1):30–42. doi: 10.1093/ije/dyh132. [DOI] [PubMed] [Google Scholar]
- 18.Lawlor DA, Harbord RM, Sterne JA, Timpson N, Davey Smith G. Mendelian randomization: using genes as instruments for making causal inferences in epidemiology. Stat Med. 2008;27(8):1133–1163. doi: 10.1002/sim.3034. [DOI] [PubMed] [Google Scholar]
- 19.Ebrahim S, Davey Smith G. Mendelian randomization: can genetic epidemiology help redress the failures of observational epidemiology? Hum Genet. 2008;123(1):15–33. doi: 10.1007/s00439-007-0448-6. [DOI] [PubMed] [Google Scholar]
- 20.Maeda K, Okubo K, Shimomura I, Funahashi T, Matsuzawa Y, Matsubara K. cDNA cloning and expression of a novel adipose specific collagen-like factor, apM1 (AdiPose Most abundant Gene transcript 1) Biochem Biophys Res Commun. 1996;221(2):286–289. doi: 10.1006/bbrc.1996.0587. [DOI] [PubMed] [Google Scholar]
- 21.Qi L, Menzaghi C, Salvemini L, De Bonis C, Trischitta V, Hu FB. Novel locus FER is associated with serum HMW adiponectin levels. Diabetes. 2011;60(8):2197–2201. doi: 10.2337/db10-1645. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Dastani Z, Hivert MF, Timpson N, Perry JR, Yuan X, Scott RA, et al. Novel loci for adiponectin levels and their influence on type 2 diabetes and metabolic traits: a multi-ethnic meta-analysis of 45,891 individuals. PLoS Genet. 2012;8(3):e1002607. doi: 10.1371/journal.pgen.1002607. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Bacci S, Rizza S, Prudente S, Spoto B, Powers C, Facciorusso A, et al. The ENPP1 Q121 variant predicts major cardiovascular events in high-risk individuals: evidence for interaction with obesity in diabetic patients. Diabetes. 2011;60(3):1000–1007. doi: 10.2337/db10-1300. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Menzaghi C, Bacci S, Salvemini L, Mendonca C, Palladino G, Fontana A, et al. Serum resistin, cardiovascular disease and all-cause mortality in patients with type 2 diabetes. PLoS One. 2013;8(6):e64729. doi: 10.1371/journal.pone.0064729. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Menzaghi C, Salvemini L, Paroni G, De Bonis C, Mangiacotti D, Fini G, et al. Circulating high molecular weight adiponectin isoform is heritable and shares a common genetic background with insulin resistance in nondiabetic White Caucasians from Italy: evidence from a family-based study. J Intern Med. 2010;267(3):287–294. doi: 10.1111/j.1365-2796.2009.02141.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Menzaghi C, De Cosmo S, Copetti M, Salvemini L, De Bonis C, Mangiacotti D, et al. Relationship between ADIPOQ gene, circulating high molecular weight adiponectin and albuminuria in individuals with normal kidney function: evidence from a family-based study. Diabetologia. 2011;54(4):812–818. doi: 10.1007/s00125-010-2037-9. [DOI] [PubMed] [Google Scholar]
- 27.Kraja AT, Chasman DI, North KE, Reiner AP, Yanek LR, Kilpeläinen TO, et al. Pleiotropic genes for metabolic syndrome and inflammation. Mol Genet Metab. 2014;112(4):317–338. doi: 10.1016/j.ymgme.2014.04.007. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Menzaghi C, Paroni G, De Bonis C, Soccio T, Marucci A, Bacci S, et al. The 318 C > G single-nucleotide polymorphism in GNAI2 gene promoter region impairs transcriptional activity through specific binding of Sp1 transcription factor and is associated with high blood pressure in Caucasians from Italy. J Am Soc Nephrol. 2006;17(4 Suppl 2):S115–S119. doi: 10.1681/ASN.2005121340. [DOI] [PubMed] [Google Scholar]
- 29.Rankinen T, Sarzynski MA, Ghosh S, Bouchard C. Are there genetic paths common to obesity, cardiovascular disease outcomes, and cardiovascular risk factors? Circ Res. 2015;116(5):909–922. doi: 10.1161/CIRCRESAHA.116.302888. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Fall T, Hägg S, Mägi R, Ploner A, Fischer K, Horikoshi M, et al. The role of adiposity in cardiometabolic traits: a Mendelian randomization analysis. PLoS Med. 2013;10(6):e1001474. doi: 10.1371/journal.pmed.1001474. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Raman K, Chong M, Akhtar-Danesh GG, D’Mello M, Hasso R, Ross S, et al. Genetic markers of inflammation and their role in cardiovascular disease. Can J Cardiol. 2013;29(1):67–74. doi: 10.1016/j.cjca.2012.06.025. [DOI] [PubMed] [Google Scholar]
- 32.Hug C, Wang J, Ahmad NS, Bogan JS, Tsao TS, Lodish HF. T-cadherin is a receptor for hexameric and high-molecular-weight forms of Acrp30/adiponectin. Proc Natl Acad Sci. 2004;101(28):10308–10313. doi: 10.1073/pnas.0403382101. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Jee SH, Sull JW, Lee JE, Shin C, Park J, Kimm H, et al. Adiponectin concentrations: a genome-wide association study. Am J Hum Genet. 2010;87(4):545–552. doi: 10.1016/j.ajhg.2010.09.004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Gao H, Kim YM, Chen P, Igase M, Kawamoto R, Kim MK, et al. Genetic variation in CDH13 is associated with lower plasma adiponectin levels but greater adiponectin sensitivity in East Asian populations. Diabetes. 2013;62(12):4277–4283. doi: 10.2337/db13-0129. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Uetani E, Tabara Y, Kawamoto R, Onuma H, Kohara K, Osawa H, et al. CDH13 genotype-dependent association of high-molecular weight adiponectin with all-cause mortality: the J-SHIPP study. Diabetes Care. 2014;37(2):396–401. doi: 10.2337/dc13-1658. [DOI] [PubMed] [Google Scholar]
- 36.Van Berendoncks AM, Garnier A, Beckers P, Hoymans VY, Possemiers N, Fortin D, et al. Functional adiponectin resistance at the level of the skeletal muscle in mild to moderate chronic heart failure. Circ Heart Fail. 2010;3(2):185–194. doi: 10.1161/CIRCHEARTFAILURE.109.885525. [DOI] [PubMed] [Google Scholar]
- 37.Khan RS, Kato TS, Chokshi A, Chew M, Yu S, Wu C, et al. Adipose tissue inflammation and adiponectin resistance in patients with advanced heart failure: correction after ventricular assist device implantation. Circ Heart Fail. 2012;5(3):340–348. doi: 10.1161/CIRCHEARTFAILURE.111.964031. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Chiara TD, Argano C, Scaglione A, Corrao S, Pinto A, Scaglione R. Circulating adiponectin: a cardiometabolic marker associated with global cardiovascular risk. Acta Cardiol. 2015;70(1):33–40. doi: 10.1080/ac.70.1.3064591. [DOI] [PubMed] [Google Scholar]
- 39.Medina-Urrutia A, Posadas-Romero C, Posadas-Sánchez R, Jorge-Galarza E, Villarreal-Molina T, MeC González-Salazar, et al. Role of adiponectin and free fatty acids on the association between abdominal visceral fat and insulin resistance. Cardiovasc Diabetol. 2015;14:20. doi: 10.1186/s12933-015-0184-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Beltrami-Moreira M, Qi L, Maestri MK, Fuchs FD, Pakter HM, Moreira LB, et al. Association between plasma adiponectin and arteriolar vessel caliber among elderly hypertensive subjects. J Am Soc Hypertens. 2015;9(8):620–627. doi: 10.1016/j.jash.2015.05.008. [DOI] [PubMed] [Google Scholar]
- 41.Fayad R, Pini M, Sennello JA, Cabay RJ, Chan L, Xu A, et al. Adiponectin deficiency protects mice from chemically induced colonic inflammation. Gastroenterology. 2007;132(2):601–614. doi: 10.1053/j.gastro.2006.11.026. [DOI] [PubMed] [Google Scholar]
- 42.Liu D, Luo S, Li Z. Multifaceted roles of adiponectin in rheumatoid arthritis. Int Immunopharmacol. 2015;28(2):1084–1090. doi: 10.1016/j.intimp.2015.08.013. [DOI] [PubMed] [Google Scholar]
- 43.Kaur K, Saxena A, Larsen B, Truman S, Biyani N, Fletcher E, et al. Mucus mediated protection against acute colitis in adiponectin deficient mice. J Inflamm (Lond) 2015;12:35. doi: 10.1186/s12950-015-0079-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Jia Z, Liu Y, Cui S. Adiponectin induces breast cancer cell migration and growth factor expression. Cell Biochem Biophys. 2014;70(2):1239–1245. doi: 10.1007/s12013-014-0047-9. [DOI] [PubMed] [Google Scholar]
- 45.Aguilera E, Serra-Planas E, Granada ML, Pellitero S, Reverter JL, Alonso N, et al. Relationship of YKL-40 and adiponectin and subclinical atherosclerosis in asymptomatic patients with type 1 diabetes mellitus from a European Mediterranean population. Cardiovasc Diabetol. 2015;14:121. doi: 10.1186/s12933-015-0287-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Singer JR, Palmas W, Teresi J, Weinstock R, Shea S, Luchsinger JA. Adiponectin and all-cause mortality in elderly people with type 2 diabetes. Diabetes Care. 2012;35(9):1858–1863. doi: 10.2337/dc11-2215. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Ortega Moreno L, Lamacchia O, Salvemini L, De Bonis C, De Cosmo S, Cignarelli M, et al. The paradoxical association of adiponectin with mortality rate in patients with type 2 diabetes: evidence of synergism with kidney function. Atherosclerosis. 2015;245:222–227. doi: 10.1016/j.atherosclerosis.2015.12.026. [DOI] [PubMed] [Google Scholar]
- 48.Moghadasi M, Mohebbi H, Rahmani-Nia F, Hassan-Nia S, Noroozi H, Pirooznia N. High-intensity endurance training improves adiponectin mRNA and plasma concentrations. Eur J Appl Physiol. 2012;112(4):1207–1214. doi: 10.1007/s00421-011-2073-2. [DOI] [PubMed] [Google Scholar]
- 49.Lakhdar N, Denguezli M, Zaouali M, Zbidi A, Tabka Z, Bouassida A. Six months training alone or combined with diet alters HOMA-AD, HOMA-IR and plasma and adipose tissue adiponectin in obese women. Neuro Endocrinol Lett. 2014;35(5):373–379. [PubMed] [Google Scholar]
- 50.Zoungas S, Patel A. Cardiovascular outcomes in type 2 diabetes: the impact of preventative therapies. Ann N Y Acad Sci. 2010;1212:29–40. doi: 10.1111/j.1749-6632.2010.05837.x. [DOI] [PubMed] [Google Scholar]
- 51.Lim S, Quon MJ, Koh KK. Modulation of adiponectin as a potential therapeutic strategy. Atherosclerosis. 2014;233(2):721–728. doi: 10.1016/j.atherosclerosis.2014.01.051. [DOI] [PubMed] [Google Scholar]
- 52.Public Health Genomics Knowledge Base (v1.0). https://phgkb.cdc.gov/HuGENavigator/gWAHitStartPage.do.
- 53.Broad Institute. http://www.broadinstitute.org/mammals/haploreg/haploreg.php.
- 54.Sharma JN. Role of tissue kallikrein-kininogen-kinin pathways in the cardiovascular system. Arch Med Res. 2006;37(3):299–306. doi: 10.1016/j.arcmed.2005.08.001. [DOI] [PubMed] [Google Scholar]
- 55.Sainz IM, Pixley RA, Colman RW. Fifty years of research on the plasma kallikrein-kinin system: from protein structure and function to cell biology and in vivo pathophysiology. Thromb Haemost. 2007;98(1):77–83. [PubMed] [Google Scholar]
- 56.Campbell DJ. The renin-angiotensin and the kallikrein-kinin systems. Int J Biochem Cell Biol. 2003;35(6):784–791. doi: 10.1016/S1357-2725(02)00262-5. [DOI] [PubMed] [Google Scholar]
- 57.Wang Y, Lam KS, Yau MH, Xu A. Post-translational modifications of adiponectin: mechanisms and functional implications. Biochem J. 2008;409(3):623–633. doi: 10.1042/BJ20071492. [DOI] [PubMed] [Google Scholar]