

Abstract
Objectives
To systematically review and examine the psychometric properties of established resilience scales in older adults, i.e. ≥60 years.
Methods
A systematic review of Scopus and Web of Science databases was undertaken using the search strategy “resilience” AND (ageing OR aging)”. Independent title/abstract and fulltext screening were undertaken, identifying original peer-reviewed English articles that conducted psychometric validation studies of resilience metrics in samples aged ≥60 years. Data on the reliability/validity of the included metrics were extracted from primary studies.
Results
Five thousand five hundred nine studies were identified by the database search, 426 used resilience psychometrics, and six psychometric analysis studies were included in the final analysis. These studies conducted analyses of the Connor Davidson Resilience Scale (CD-RISC) and its shortened 10-item version (CD-RISC10), the Resilience Scale (RS) and its shortened 5- (RS-5) and 11- (RS-11) item versions, and the Brief Resilient Coping Scale (BRCS). All scales demonstrated acceptable levels of internal consistency, convergent/discriminant validity and theoretical construct validity. Factor structures for the RS, RS-11 and CD-RISC diverged from the structures in the original studies.
Conclusion
The RS, RS-5, RS-11, CD-RISC, CD-RISC10 and BRCS demonstrate psychometric robustness adequate for continued use in older populations. However, results from the current study and pre-existing theoretical construct validity studies most strongly support the use of the RS, with modest and preliminary support for the CD-RISC and BRCS, respectively. Future studies assessing the validity of these metrics in older populations, particularly with respect to factor structure, would further strengthen the case for the use of these scales.
Background
The examination of aspects of ageing beyond pathological and deficit-based models is on the rise [1–3]. Conceptual frameworks that focus on healthy ageing and resilience complement frameworks that focus on the identification and remediation of deficits, e.g. frailty [4]. Rather than merely avoiding clinical outcomes, e.g. depression, healthy ageing emphasises the high end of the functioning spectrum. Resilience involves the ability of the organism or individual to respond positively to environmental challenges (physiologically, psychologically or socially), with roots in both biomedical and psychological disciplines [5–8]
Resilience features strongly in developmental psychology, examining how children positively adapt to negative circumstances, for example having injection-drug using parents, but not developing psychopathology [9]. “Bouncing back” from adversity is a fundamental principle of resilience, which has subsequently been applied beyond early-life populations to those in mid- and later-life [10]. The environmental challenges faced in early-life differ from those in later life and we know little about continuities and discontinuities in resilience across life and whether the factors that promote resilience also change. Therefore, the relevance of current models of resilience and the applicability of resilience scales should also be examined in older populations. For researchers, this information will be important in the accurate identification of variables fostering resilience. These data can then be used by clinicians to advise patients on how to increase their resilience. However, if a resilience scale is not accurately capturing resilience, any research (and subsequent clinical recommendations) resulting from the scale may provide misleading information.
A number of methodological procedures and psychometrics have been developed to capture resilience; however, according to recent reviews of resilience scales the majority of thesescales have been developed and validated in young and mid-life populations, i.e. <60 years [11, 12]. Previous studies have examined the psychometric properties of resilience scales and the theoretical underpinnings of their development by reviewing validation studies and the conceptual frameworks used in the development of these scales [11, 12]. These reviews provide insights into the validity of resilience scales in younger populations. However, these metrics should be validated in older populations. The aim of the present study is to systematically review the literature examining the reliability and validity of resilience scales that have undergone psychometric examination in older populations.
Methods
Search strategy
A systematic review across Scopus and Web of Science databases. Scopus is described as the largest abstract and indexing database, providing 100 % coverage Medline, Embase, and Compendex databases [13]. Web of Science is, similarly, a large abstract and indexing database, providing 100 % coverage of Science Citation, Arts & Humanities Indexes, and Social Sciences Citation databases. Searches were conducted between 05/02/2015 and 11/02/2015 using terms “resilience” AND (ageing OR aging)” for articles published on any date prior to the date of the search. . Additionally, reference lists and relevant articles were hand searched.
Screening
Independent title/abstract and full text screening was conducted (TDC, AK, MS). Screening results were compared and disagreements concerning inclusion/exclusion were resolved via discussion.
Inclusion criteria
Studies were included in the final analysis if they met the following criteria: i) original peer-reviewed research, ii) sample population aged ≥60 years, iii) conducted a psychometric evaluation of an existing resilience scale.
Exclusion criteria
Studies were excluded if they met the following criteria: i) ineligible article type, i.e. conference proceeding, editorial, commentary, perspective, book chapter, book review, dissertation, or ii) published in a language other than English.
Data extraction
Psychometric scales that had validation studies conducted with older adults were identified for extraction. Data on the psychometric robustness of the scales were collected, specifically with regards to: internal consistency, which reflects the extent to which components of a scale all measure the same construct (using Cronbach’s alpha [14]); convergent validity, which reflects the degree to which a scale’s scores align with other scales that measure similar constructs; discriminant validity, which reflects the degree to a scale’s scores diverge from other scales that measure contrasting constructs; construct validity, which reflects the degree to which a scale captures the phenomena it intends to, e.g. factor structure [15].
Results
Included studies
The database search returned 5909 articles (after removing duplicates) of which 426 studies had used psychometric scales. The six studies that met inclusion criteria used three different psychometrics: the Connor-Davidson Resilience Scale [16], the Wagnild & Young Resilience Scale [17], the Brief Resilient Coping Scale [18] (Fig. 1) (Table 1).
Fig. 1.
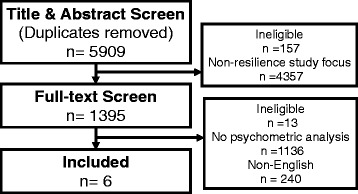
Study inclusion flowchart
Table 1.
Demographic characteristics of studies included in the review
| Study | n | Age | Country | Female (%) | Married (%) | Population | Language | |||
|---|---|---|---|---|---|---|---|---|---|---|
| Min | Max | Mean | SD | |||||||
| Girtler, et al. (2010)a [26] | 178 | – | – | 63.9 | 14.6 | Italy | – | – | Community–dwelling | Italian |
| Goins, et al. (2013)b [25] | 160 | – | – | 67.9 | 9.9 | USA | 68.8 | 47.8 | American Indians | English |
| Lamond, et al. (2008) [24]b | 1395 | 60 | 91 | 72.7 | 7.2 | USA | 100 | – | Community-dwelling | English |
| Resnick & Inguito (2011)a [28] | 163 | 67 | 99 | 86.3 | 5.8 | USA | – | – | Continuing care retirement community | English |
| 101 | 65 | 97 | 80.0 | 7.6 | USA | – | – | Continuing care retirement community | English | |
| Tomas, et al. (2012)c [30] | 133 | 60 | 84 | 71.7 | 6.9 | Spain | – | 66.9 | Community-dwelling | Spanish |
| von Eisenhart Rothe, et al. (2013)a [27] | 3712 | 64 | 94 | 72.0 | 5.8 | Germany | 52.0 | – | Community-dwelling | German |
aValidation of Resilience Scale 37
bValidation of Connor-Davidson Resilience Scale (CD-RISC) 15
cValidation of Brief Resilient Coping Scale 17
Included psychometrics
Connor-Davidson Resilience Scale
The Connor Davidson Resilience Scale (CD-RISC) is a 25-item metric developed from previous work by Kobasa [19], Rutter [7], and Lyons [20], with a theoretical grounding in stress, coping and adaptation research [12]. Items are scored on a 5-point scale (0–4) with higher scores reflecting higher levels of resilience. The scale was originally piloted with samples from the general population (n = 577), primary care (n = 139), psychiatric outpatients (n = 43), generalised anxiety patients (n = 24), and post-traumatic stress disorder patients (n = 22) with a mean age of 43.8 years (SD 15.4 years) [16]. In its development, five latent factors were identified: personal competence, trust/tolerance/strengthening effects of stress, acceptance of change and secure relationships, control, and spiritual influences.
The CD-RISC demonstrated adequate reliability and construct validity in its initial development. Cronbach’s alpha (a reliability metric for capturing internal consistency with cutoffs above 0.7 deemed acceptable) for the scale was 0.89 in the pilot study [16]. Subsequent reviews of studies examining the CD-RISC’s psychometric rigor in adolescent/adult samples support these initial findings [11, 12].
Wagnild & Young’s Resilience Scale
Items in the Resilience Scale (RS) were derived from a qualitative study of 24 older women (aged 67–92) [17, 21]. Verbatim components of these interviews were used in the pilot RS, which was conducted with 39 undergraduate nursing students [17]. All 25 items are positively scored on a 7-point scale from 1 (disagree) to 7 (agree), with possible scores ranging from 25 to 175. Higher scores indicate greater resilience. Internal consistency in the initial development of the RS was 0.89 [17]. The RS has demonstrated adequate reliability and construct validity in subsequent studies of teenagers and young adults [22, 23] as well as in a sample of adults aged 53–95 [17] (that did not meet inclusion criteria, i.e. minimum age ≥60 years, for the present study).
Brief Resilient Coping Scale
The Brief Resilient Coping Scale (BRCS) [18] is a four-item scale originally developed in two samples of adults with rheumatoid arthritis (n = 90, 140) with mean ages of 46.0 (SD 11.8) and 57.8 (SD 1.25) years. Each item is scored from 1 to 5, therefore scores range from 4 to 20 with a mean of 14.81 (SD 2.95) in the pilot study. Internal consistency for the pooled sample was 0.69. Exploratory factor analysis revealed a two factor structure [18].
Psychometric properties in older samples
Connor-Davidson Resilience Scale
Two studies investigated the psychometric properties of the full CD-RISC [24, 25], additionally Goins, et al. [25] examined the abbreviated 10-item CD-RISC (CD-RISC10). Mean CD-RISC scores were 75.7 (SD 13.0) and 83.0 (SD13.4); CD-RISC10 mean score was 33.5 (SD 6.2). CD-RISC mean item correlation was 0.61 (SD 0.13) [24]. Principal components analysis revealed a four-factor structure [24] using Kaiser criterion to determine the number of factors, i.e. Eigenvalues >1. Confirmatory factor analysis suggested a uni-dimensional factor structure [25]. Significant positive correlations were observed between self-efficacy, self-mastery and social support scales while a significant negative correlation was observed with depression. Internal consistency, i.e. Cronbach’s alpha, ranged from 0.88 to 0.93 (Table 2).
Table 2.
Psychometrics characteristics of the Connor-Davidson Resilience Scale
| Number of factors | Correlation (r) | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Scale | n | Mean score | SD | Cronbach’s α | EFA | CFA | CES-D | GSES | PSMS | MOS-SSS | |
| Lamond, et al. (2008) [24] | CD-RISC | 1395 | 75.7 | 13.0 | 0.92 | 4 | – | – | – | – | – |
| Goins, et al. (2013) [25] | CD-RISC | 160 | 83.0 | 13.4 | 0.93 | – | 1 | –0.51** | 0.47** | 0.29** | 0.27** |
| CD-RISC10 | 33.5 | 6.2 | 0.88 | – | – | –0.51** | 0.45** | 0.31** | 0.21* | ||
SD standard deviation; EFA Exploratory Factor Analysis; CFA Confirmatory Factor Analysis; CES-D Center for Epidemiologic Studies Depression Scale 42; GSES General Self-Efficacy Scale 43; PSMS Personal Self-Mastery Scale 44; MOS-SSS Medical Outcomes Study Social Support Survey 45
*p < .01
**p < .001
Wagnild & Young’s Resilience Scale
The full RS was psychometrically examined in two studies [26], additionally the five- (RS-5) and 11-item (RS-11) RS were examined in a single study [27]. The Resnick & Inguito [28] study conducted RS validations in two samples (Table 1).
The full RS demonstrated a Cronbach’s alpha ranging from 0.85 to 0.91. In Resnick, et al. [28] exploratory factor analysis revealed a unidimensional model in the whole sample. Confirmatory factor analysis revealed an unacceptable fit, i.e. factor loadings below 0.50 [29], for 7 of 25 items for the unidimensional model; however, Rasch analysis indicated a fair fit to the data. Girtler, et al.’s [26] exploratory factor analysis revealed a six factor structure (meaningfulness, self-reliance, perseverance, existential aloneness, equanimity A, equanimity B) using the Kaiser criterion.
Analysis of the RS-11 revealed a Cronbach’s alpha of 0.86 and a single latent factor [27]. The RS-5 revealed a Cronbach’s alpha of 0.80. Significant positive correlations were observed with ego-resilience, (a personality trait resilience scale) and general health, as well as a significant negative correlation with depression (Table 3).
Table 3.
Psychometrics characteristics of the Wagnild & Young Resilience Scale
| Number of factors | Correlation (r) | |||||||
|---|---|---|---|---|---|---|---|---|
| Scale | n | Cronbach’s α | EFA | CFA | ER | GHQ | BDI-II | |
| Girtler, et al. (2010) [26] | RS | 178 | 0.86 | 6 | – | 0.59* | 0.45* | −0.31* |
| Resnick & Inguito (2011) [28] | RS | 101 | 0.91 | 1 | 1 | – | – | – |
| RS | 163 | 0.83 | 1 | – | – | – | ||
| von Eisenhart Rothe, et al. (2013) [27] | RS-11 | 3712 | 0.86 | 1 | – | – | – | – |
| RS-5 | 0.80 | – | – | – | – | – | ||
SD standard deviation; EFA Exploratory Factor Analysis; ER Ego-Resilience Scale 46; GHQ General Health Questionnaire 47; BDI-II Beck Depression Inventory Second Edition 48
*p < .0001
Brief Resilient Coping Scale
A single study examined the psychometric properties of the BRCS [30]. Cronbach’s alpha was 0.83 and inter-item correlations ranged from 0.44 to 0.69. Confirmatory factor analysis supported a one-factor structure.
Discussion
The CD-RISC, RS and BRCS (and their abbreviated versions) all attempt to capture psychological resilience. The present review reveals acceptable psychometric properties, i.e. internal consistency, convergent validity, and discriminant validity, in samples of older adults; less robust construct validity, i.e. factor structure, in the CD-RISC and RS. The CD-RISC and its shortened version (CD-RISC10) provided supporting evidence for continued use in older populations. Similarly, Wagnild & Young’s RS and its shortened versions (RS-5, RS-11) were validated in three studies with four sample groups, providing supporting evidence for the continued use of these metrics in older populations. The BRCS provided evidence for use in older populations in the few psychometric properties that were measured; however, the BRCS would benefit from further supporting evidence.
The small number of published studies conducting psychometric validations of resilience metrics in older adults, and the comparatively small sample sizes of these studies, is a notable limitation. With our intention to study only older sample groups, to ensure the validity of the metric was specific to older adults, validity studies that included older adults alongside middle –aged and younger participants were excluded. These exclusion criteria eliminated 20 validation studies from inclusion. Previous validation studies have suggested that there is no difference in the way that resilience scales capture resilience depending on gender in younger sample [31, 32]; however, included studies did not conduct any analysis of the role of gender on resilience in aging. An inherent limitation of reviewing psychometric resilience scales is the assumption that resilience is consistent across demographic and disease states, an area that has not been fully investigated in the literature to date.
In addition to being focused on older adults, studies also sampled characteristics that differed from the original samples, i.e. American community dwelling adults, by ethnicity (American Indian [24]) and language (German [27] and Italian [26]). These additional variations may have resulted in unexpected differences in the psychometric properties of the scales, e.g. factor structure.
Previous reviews of the CD-RISC have indicated that the metric is psychometrically sound in younger populations [11]. Windle, et al.’s [11] review gave the CD-RISC the highest rating for psychometric soundness in a recent critique of resilience metrics, noting its high reliability, i.e. Cronbach’s alpha and high construct validity, i.e. theory underpinning the scale [11]. The present study supports these findings in the full CD-RISC. The internal consistency in the reviewed studies (α = 0.92, 0.93) was slightly higher than the original study (α = 0.89), which was conducted with middle-aged individuals [16]. Differences in mean scores were relatively small given the size of the confidence intervals and would likely have no clinical significance [24]. Further, convergent and discriminant validity of the scale aligns with previous validations in younger populations, i.e. significant positive correlations with self-efficacy, self-mastery, and medical outcome social support surveys and a significant negative correlation with depression [33, 34].
Despite the high levels of theoretical construct validity indicated in a review of the CD-RISC [12], the factor structures in both Lamond et al. [24] and Goins, et al. [25] differed from the original five-factor structure [16]. This may suggest that the process of resilience differs somewhat in younger cohorts; however, the CD-RISC also failed to reproduce the original five-factor structure in samples in a range of age groups, e.g. American college students [35], military veterans [36], Chinese adults [37], and Australian adolescents/ adults [38]. Given the diversity of adversity experienced throughout life and the variety of positive adaptations to these adverse events, these structural differences may be a result of resilience manifesting itself in different forms at different ages. Challenges faced in adolescence, mid-life and older age are vastly disparate, which may affect the way resilience is manifested; however, a study by Liu, et al. [31] suggests structural invariance in the CD-RISC across life. These differences in factor structure may also be due to underlying differences in the overt manifestation of resilience, or due to cultural, regional or cohort differences. Alternatively, this could be a methodological artefact; the use of Kaiser criterion as the means with which to determine the number of factors to extract has been viewed as an ineffective method [39].
The abbreviated CD-RISC10 performed better than the full version. Despite having slightly lower (although adequate) internal consistency (0.93 vs. 0.83), than the full version, the CD-RISC10 demonstrated a more stable high-order single factor structure [25]. The Goins, et al. [25] study is the first to examine the psychometric properties of the CD-RISC10 in older adults, but these encouraging results suggest that further investigation and continued use is prudent.
The RS is the most widely validated resilience metric, demonstrating appropriate psychometric properties across life in previous reviews [11, 12, 40]; these results are supported by the present review of older samples. The RS was examined in three samples across two studies, demonstrating adequate levels of internal consistency and convergent and discriminant validity in line with previous psychometric analyses in younger samples [26, 41]. The factor structure of the RS varied between studies, which may indicate that the RS quantifies resilience differently in different age groups; an important limitation to be noted by researchers. These studies did, however, also vary from the original RS development study with respect to country and language, which may have obscured the underlying reason for this latent structure inconsistency. Previous studies have also failed to reproduce the original factor structure, e.g. in Dutch [42], Russian [43] and Japanese [44] samples. The RS was developed a priori with a sample of older adults and, therefore, has strong theoretical construct validity [11, 12, 40], which suggests the factor structure should be consistent. The RS was piloted with undergraduate nurses; however, the items included in the RS were taken directly from qualitative interviews with older women [21], indicating a high level of theoretical construct validity. Although findings in the present study reflect an inconsistent factor structure, the theoretical underpinnings suggest that the RS is the most psychometrically robust resilience scale for use with older adults.
The BRCS provided adequate psychometric robustness in the few validation measures collected. The brevity of the BRCS and its ease of administration is also an advantageous attribute for researchers and clinicians. Evidence for the validity of the BRCS has been provided in a few studies; however, more psychometric research is needed, e.g. further examination of factor structure, convergent validity, divergent validity, internal consistency, in order to conclusively establish the BRCS as an effective means of capturing resilience in older adults.
Conclusions
The CD-RISC, CD-RISC10, RS, RS-5, RS-11 and BRCS demonstrate psychometric properties that fall within acceptable ranges of internal consistency, convergent and divergent validity in older populations to warrant their continued usage; however, the factor structure of the scales was inconsistent. Amongst the three resilience scales examined, the RS has been used the most widely used and is most theoretically robust resilience scale in older samples; results from the present review suggest the RS is the most suitable resilience scale for use in older adults. The RS had the greatest number of validation studies and the strongest evidence for its use, whilst the CD-RISC provided encouraging validation studies and the BRCS preliminary evidence of its validity. Given the dearth of studies reporting the psychometric properties of resilience scales it would be prudent for prospective studies of resilience to report these data whenever a resilience scale is employed. More research will be required to further existing evidence of the utility of these resilience metrics or to develop new resilience metrics specifically for use in older populations.
Footnotes
Competing interests
The authors declare that they have no competing interests.
Authors’ contributions
TDC, AK and MS conducted independent title, abstract and fulltext screening. TDC conducted the data analysis and wrote the first draft. All authors contributed to the editing and revision of the manuscript and have approved the final manuscript.
References
- 1.Haskett ME, Nears K, Ward CS, McPherson AV. Diversity in adjustment of maltreated children: Factors associated with resilient functioning. Clin Psychol Rev. 2006;26:796–812. doi: 10.1016/j.cpr.2006.03.005. [DOI] [PubMed] [Google Scholar]
- 2.Cosco TD, Prina AM, Perales J, Stephan BCM, Brayne C. Operational definitions of successful aging: A systematic review. Int Psychogeriatr. 2014;26:373–381. doi: 10.1017/S1041610213002287. [DOI] [PubMed] [Google Scholar]
- 3.Kuh D, Karunananthan S, Bergman H, Cooper R. A life-course approach to healthy ageing: maintaining physical capability. Proc Nutr Soc. 2014;73:237–248. doi: 10.1017/S0029665113003923. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Rockwood K, Fox RA, Stolee P, Robertson D, Beattie BL. Frailty in elderly people: an evolving concept. CMAJ. 1994;150:489–495. [PMC free article] [PubMed] [Google Scholar]
- 5.Seligman ME, Csikszentmihalyi M. Positive psychology. An introduction. Am Psychol. 2000;55:5–14. doi: 10.1037/0003-066X.55.1.5. [DOI] [PubMed] [Google Scholar]
- 6.Garmezy N. Resilience in children’s adaptation to negative life events and stressed environments. Pediatr Ann. 1991;20:459–460. doi: 10.3928/0090-4481-19910901-05. [DOI] [PubMed] [Google Scholar]
- 7.Rutter M. Resilience in the face of adversity. Protective factors and resistance to psychiatric disorder. Br J Psychiatry. 1985;147:598–611. doi: 10.1192/bjp.147.6.598. [DOI] [PubMed] [Google Scholar]
- 8.Dubos R. Adapting man adapting: curing, helping, consoling. Yale J Biol Med. 1979;52:211–218. [PMC free article] [PubMed] [Google Scholar]
- 9.Pilowsky DJ, Zybert PA, Vlahov D. Resilient children of injection drug users. J Am Acad Child Adolesc Psychiatry. 2004;43:1372–1379. doi: 10.1097/01.chi.0000138355.29099.2a. [DOI] [PubMed] [Google Scholar]
- 10.Ong AD, Bergeman CS, Bisconti TL, Wallace KA. Psychological resilience, positive emotions, and successful adaptation to stress in later life. J Pers Soc Psychol. 2006;91:730–749. doi: 10.1037/0022-3514.91.4.730. [DOI] [PubMed] [Google Scholar]
- 11.Windle G, Bennett KM, Noyes J. A methodological review of resilience measurement scales. Health Qual Life Outcomes 2011, 9:8-8. [DOI] [PMC free article] [PubMed]
- 12.Ahern NR, Kiehl EM, Sole ML, Byers J. A review of instruments measuring resilience. Issues Compr Pediatr Nursi. 2006;29:103–125. doi: 10.1080/01460860600677643. [DOI] [PubMed] [Google Scholar]
- 13.Burnham JF. Scopus database: a review. Biomed Digital Libr. 2006;3:1–1. doi: 10.1186/1742-5581-3-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Cronbach L. Coefficient alpha and the internal structure of tests. Psychometrika. 1951;16:297–334. doi: 10.1007/BF02310555. [DOI] [Google Scholar]
- 15.Bryman A. Social research methods. 3. Oxford; New York: Oxford University Press; 2008. [Google Scholar]
- 16.Connor KM, Davidson JR. Development of a new resilience scale: the Connor-Davidson Resilience Scale (CD-RISC) Depress Anxiety. 2003;18:76–82. doi: 10.1002/da.10113. [DOI] [PubMed] [Google Scholar]
- 17.Wagnild GM, Young HM. Development and psychometric evaluation of the Resilience Scale. J Nurs Meas. 1993;1:165–178. [PubMed] [Google Scholar]
- 18.Sinclair VG, Wallston KA. The development and psychometric evaluation of the brief resilient coping scale. Assessment. 2004;11:94–101. doi: 10.1177/1073191103258144. [DOI] [PubMed] [Google Scholar]
- 19.Kobasa SC. Stressful life events, personality, and health: an inquiry into hardiness. J Pers Soc Psychol. 1979;37:1–11. doi: 10.1037/0022-3514.37.1.1. [DOI] [PubMed] [Google Scholar]
- 20.Lyons J. Strategies for assessing the potential for positive adjustment following trauma. J Trauma Stress. 1991;4:93–111. doi: 10.1002/jts.2490040108. [DOI] [Google Scholar]
- 21.Wagnild G, Young HM. Resilience among older women. Image J Nurs Sch. 1990;22:252–255. doi: 10.1111/j.1547-5069.1990.tb00224.x. [DOI] [PubMed] [Google Scholar]
- 22.Las Hayas C, Calvete E, Gomez del Barrio A, Beato L, Munoz P, Angel Padierna J. Resilience Scale-25 Spanish version: Validation and assessment in eating disorders. Eat Behav. 2014;15:460–463. doi: 10.1016/j.eatbeh.2014.06.010. [DOI] [PubMed] [Google Scholar]
- 23.Ruiz R, de la Vega R, Poveda J, Rosado A, Serpa S. Psychometric analysis of the resilience scale in the sport of football. Revista De Psicologia Del Deporte. 2012;21:143–151. [Google Scholar]
- 24.Lamond AJ, Depp CA, Allison M, Langer R, Reichstadt J, Moore DJ, et al. Measurement and predictors of resilience among community-dwelling older women. J Psychiatr Res. 2008;43:148–54. [DOI] [PMC free article] [PubMed]
- 25.Goins RT, Gregg JJ, Fiske A. Psychometric properties of the Connor-Davidson Resilience Scale with older American Indians: the Native Elder Care Study. Res Aging. 2013;35:123–143. doi: 10.1177/0164027511431989. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Girtler N, Casari EF, Brugnolo A, Cutolo M, Dessi B, Guasco S, et al. Italian validation of the Wagnild and Young Resilience Scale: a perspective to rheumatic diseases. Clin Exp Rheumatol. 2010;28:669–78. [PubMed]
- 27.von Eisenhart RA, Zenger M, Lacruz ME, Emeny R, Baumert J, Haefner S, et al. Validation and development of a shorter version of the resilience scale RS-11: results from the population-based KORA-age study. BMC Psychol. 2013;1:25. [DOI] [PMC free article] [PubMed]
- 28.Resnick BA, Inguito PL. The Resilience Scale: Psychometric Properties and Clinical Applicability in Older Adults. Arch Psychiatr Nurs. 2011;25:11–20. doi: 10.1016/j.apnu.2010.05.001. [DOI] [PubMed] [Google Scholar]
- 29.Nunnally JC, Bernstein I. Psychometric theory. 3. New York: McGraw-Hill; 1994. [Google Scholar]
- 30.Tomas JM, Melendez JC, Sancho P, Mayordomo T. Adaptation and Initial Validation of the BRCS in an Elderly Spanish Sample. Eur J Psychol Assess. 2012;28:283–289. doi: 10.1027/1015-5759/a000108. [DOI] [Google Scholar]
- 31.Liu DWY, Fairweather-Schmidt AK, Burns RA, Roberts RM. The Connor-Davidson Resilience Scale: Establishing Invariance Between Gender Across the Lifespan in a Large Community Based Study. J Psychopathol Behav Assess. 2015;37:340–348. doi: 10.1007/s10862-014-9452-z. [DOI] [Google Scholar]
- 32.Lundman B, Strandberg G, Eisemann M, Gustafson Y, Brulin C. Psychometric properties of the Swedish version of the resilience scale. Scand J Caring Sci. 2007;21:229–237. doi: 10.1111/j.1471-6712.2007.00461.x. [DOI] [PubMed] [Google Scholar]
- 33.Campbell-Sills L, Forde DR, Stein MB. Demographic and childhood environmental predictors of resilience in a community sample. J Psychiatr Res. 2009;43:1007–1012. doi: 10.1016/j.jpsychires.2009.01.013. [DOI] [PubMed] [Google Scholar]
- 34.Karairmak O. Establishing the psychometric qualities of the Connor-Davidson Resilience Scale (CD-RISC) using exploratory and confirmatory factor analysis in a trauma survivor sample. Psychiatry Res. 2010;179:350–356. doi: 10.1016/j.psychres.2009.09.012. [DOI] [PubMed] [Google Scholar]
- 35.Campbell-Sills L, Stein MB. Psychometric analysis and refinement of the Connor-davidson Resilience Scale (CD-RISC): Validation of a 10-item measure of resilience. J Trauma Stress. 2007;20:1019–1028. doi: 10.1002/jts.20271. [DOI] [PubMed] [Google Scholar]
- 36.Green KT, Hayward LC, Williams AM, Dennis PA, Bryan BC, Taber KH, et al. Examining the factor structure of the Connor-Davidson Resilience Scale (CD-RISC) in a post-9/11 U.S. military veteran sample. Assessment. 2014;21:443–51. [DOI] [PMC free article] [PubMed]
- 37.Yu X-N, Lau JTF, Mak WWS, Zhang J, Lui WWS. Factor structure and psychometric properties of the Connor-Davidson Resilience Scale among Chinese adolescents. Compr Psychiatry. 2011;52:218–224. doi: 10.1016/j.comppsych.2010.05.010. [DOI] [PubMed] [Google Scholar]
- 38.Gucciardi DF, Jackson B, Coulter TJ, Mallett CJ. The Connor-Davidson Resilience Scale (CD-RISC): Dimensionality and age-related measurement invariance with Australian cricketers. Psychol Sport Exerc. 2011;12:423–433. doi: 10.1016/j.psychsport.2011.02.005. [DOI] [Google Scholar]
- 39.Steger MF. An illustration of issues in factor extraction and identification of dimensionality in psychological assessment data. J Pers Assess. 2006;86:263–272. doi: 10.1207/s15327752jpa8603_03. [DOI] [PubMed] [Google Scholar]
- 40.Wagnild G. A review of the Resilience Scale. J Nurs Meas. 2009;17:105–113. doi: 10.1891/1061-3749.17.2.105. [DOI] [PubMed] [Google Scholar]
- 41.Abiola T, Udofia O. Psychometric assessment of the Wagnild and Young’s resilience scale in Kano, Nigeria. BMC Res Notes. 2011;4:509–9. [DOI] [PMC free article] [PubMed]
- 42.Portzky M, Wagnild G, De Bacquer D, Audenaert K. Psychometric evaluation of the Dutch Resilience Scale RS-nl on 3265 healthy participants: a confirmation of the association between age and resilience found with the Swedish version. Scand J Caring Sci. 2010;24:86–92. doi: 10.1111/j.1471-6712.2010.00841.x. [DOI] [PubMed] [Google Scholar]
- 43.Aroian KJ, Schappler-Morris N, Neary S, Spitzer A, Tran TV. Psychometric evaluation of the Russian Language version of the Resilience Scale. J Nurs Meas. 1997;5:151–164. [PubMed] [Google Scholar]
- 44.Nishi D, Uehara R, Kondo M, Matsuoka Y. Reliability and validity of the Japanese version of the Resilience Scale and its short version. BMC Res Notes. 2010;3:310. doi: 10.1186/1756-0500-3-310. [DOI] [PMC free article] [PubMed] [Google Scholar]