

Supplemental digital content is available in the text.
Key Words: ACCELEROMETRY, ADULT, GLOBAL, PHYSICAL ACTIVITY, SEDENTARY, POOLING, SENSOR
ABSTRACT
Purpose
This study aimed to describe the scope of accelerometry data collected internationally in adults and to obtain a consensus from measurement experts regarding the optimal strategies to harmonize international accelerometry data.
Methods
In March 2014, a comprehensive review was undertaken to identify studies that collected accelerometry data in adults (sample size, n ≥ 400). In addition, 20 physical activity experts were invited to participate in a two-phase Delphi process to obtain consensus on the following: unique research opportunities available with such data, additional data required to address these opportunities, strategies for enabling comparisons between studies/countries, requirements for implementing/progressing such strategies, and value of a global repository of accelerometry data.
Results
The review identified accelerometry data from more than 275,000 adults from 76 studies across 36 countries. Consensus was achieved after two rounds of the Delphi process; 18 experts participated in one or both rounds. The key opportunities highlighted were the ability for cross-country/cross-population comparisons and the analytic options available with the larger heterogeneity and greater statistical power. Basic sociodemographic and anthropometric data were considered a prerequisite for this. Disclosure of monitor specifications and protocols for data collection and processing were deemed essential to enable comparison and data harmonization. There was strong consensus that standardization of data collection, processing, and analytical procedures was needed. To implement these strategies, communication and consensus among researchers, development of an online infrastructure, and methodological comparison work were required. There was consensus that a global accelerometry data repository would be beneficial and worthwhile.
Conclusions
This foundational resource can lead to implementation of key priority areas and identification of future directions in physical activity epidemiology, population monitoring, and burden of disease estimates.
Regular participation in moderate- to vigorous-intensity physical activities has well-established benefits for both physical and mental health (49). More recently, the detrimental health effects of sedentary time (too much sitting) (68) and the potential benefits of light-intensity activities have been identified (43,51). These advances in understanding activity across a broadened and more differentiated spectrum have, in large part, been due to advances in activity monitor technology (48), which address several of the limitations associated with self-report measures (21). Wearable, accelerometer-based activity monitors that collect date- and time-stamped posture and/or activity information are becoming increasingly available and affordable. Correspondingly, they are becoming more widely used in observational (including surveillance) and intervention studies as a measure of physical activity and sedentary time levels (i.e., total volumes). Furthermore, the time resolution of data collected from such devices has also provided important insights into the accumulation patterns of physical activity and sedentary time across the day.
Most of these insights have so far been gained from individual studies. Analysis of pooled international accelerometry data (plus other relevant variables) may, however, facilitate more in-depth understanding of (a) the levels and patterns of activity across the intensity spectrum, (b) the effect of physical activity, physical inactivity, and sedentary time on physiological, psychological, and health outcomes, (c) the correlates and determinants of these behaviors, and (d) how these levels and patterns, health associations, and correlates and determinants, as described previously, may vary between subgroups and populations. For brevity, from here onwards, the terminology “physical activity” and “activity” will be used as umbrella terms to cover the whole spectrum of physical activity variables (including the whole intensity spectrum from sedentary to light-, moderate-, and vigorous-intensity activities).
In 2008, the International Children’s Accelerometry Database (ICAD) project (http://www.mrc-epid.cam.ac.uk/research/studies/icad/) was launched, which, for the first time, pooled ActiGraph (ActiGraph LLC, Pensacola, FL) accelerometry data (epoch level) and harmonized accompanying data on children 5–18 yr (63). The database, which holds information on approximately 26,000 children from 20 studies worldwide, has allowed new analyses to generate a clearer understanding of predictors of activity, activity–disease associations, and the types and levels of activity that should be promoted to maximize health benefits (e.g., (22,47)). The ICAD project shows that international groups are prepared to collaborate and share data in a pooled archive, with data access procedures in place after submission of analysis proposal, open to all researchers in the world. This project has also provided insights into some of the benefits (e.g., large sample sizes and increased heterogeneity in activity and accompanying data) and challenges (e.g., varying protocols and measures for the activity or accompanying data) associated with such pooling efforts. Researchers have now expressed interest to extend pooling to include adults, different accelerometer models/versions, and a broader range of accompanying data (including data relating to correlates, determinants and health outcomes, as well as to the accelerometer technology and study design).
However, differences among monitor types, models, calibration methods, attachment procedures and wear locations, deployment strategies, monitor setup, and data processing procedures of existing studies, together with further developments in measurement methodology, pose evolving challenges in this research field (48). To better understand and to begin to address these challenges, this article reports on the following:
(a) a comprehensive review describing the scope of accelerometry data collected internationally in adults and
(b) an expert consensus, via a two-phase Delphi process, regarding optimal strategies to harmonize international accelerometry data.
It is intended that the data reported in this article will provide a foundational resource for implementing key priority areas and identifying future directions in the field of physical activity and sedentary behavior epidemiology.
PART A: COMPREHENSIVE REVIEW
The first part of this article provides the results of a comprehensive review, reporting on the amount of accelerometry data collected internationally in adults, types of monitors used, wear location, study designs, sampling frames, and other study-specific information.
Methods
Search strategy
Three different search strategies were used. A PubMed electronic literature database search was undertaken on March 7, 2014, using the search syntax “acceleromet* AND adult* AND physical activity.” Second, authors’ own literature databases were screened for publications that matched the inclusion criteria but were not identified from the PubMed database search, as was authors’ knowledge of unpublished studies with completed or ongoing data collection.
Inclusion and exclusion criteria
Studies that used an accelerometer-based activity monitor that measured activity across the movement intensity spectrum with a sample size of n ≥ 400 adults (18+ yr) were eligible to be included. We excluded the following: nonhuman studies, studies with a mean age of <18 yr, nontime-stamped pedometer (steps-only) studies, HR monitoring-only studies, studies that purposely recruited a specific population (i.e., populations with functional or cognitive limitations, pregnant women, military and athlete groups, students, and patients (studies involving overweight/obese adults and those at high risk for diabetes were included)), methodological studies (i.e., reliability, validity, and feasibility studies), laboratory studies, sleep-only studies, and studies not relating to physical activity.
Data extraction
Data were extracted using a standardized form, which included study name, country, monitor type/model, anatomical site worn, n, age, gender, study design, sampling frame/strategy, and timing of data collection. For multiphase studies, only data of the first phase providing accelerometry data were extracted. In cohorts with an age range covering childhood/adolescence and adulthood, the total age range was provided but n was derived for adults only, given the focus of this review. When needed, more than one information source was used per study to enable complete data extraction. For studies sourced from published documents, any information not provided in the corresponding document was determined by contacting the corresponding author. Data extraction from published manuscripts were performed by one author (K. Wi.) and double-checked by a second author (G. N. H.). Included studies were stratified into national population-based studies and other (which includes nonnational population-based studies, birth or twin studies, intervention studies, and case–control studies).
Results
Supplemental Digital Content Table 1 provides an overview of all 76 included studies providing accelerometry data in adults (see Table, Supplemental Digital Content 1, Overview of all identified studies with accelerometry data in adults, http://links.lww.com/MSS/A531). Sixty-one published studies were identified (1–8,10–15,17–20,23–37,39–42,45,46,48,50,52–67,69,71–75), with 39 of these identified via the PubMed literature database search and 22 sourced from authors’ literature databases (some of them published after March 7, 2014). Fifteen additional studies were identified through authors’ knowledge of studies in progress.
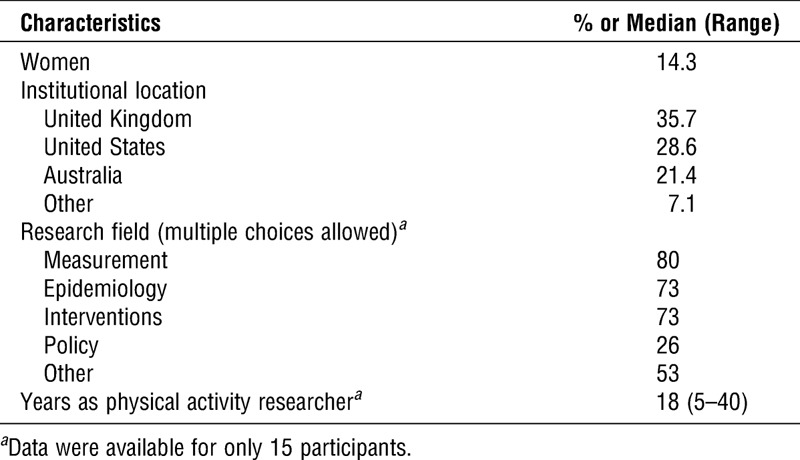
TABLE 1.
Characteristics of the 18 experts who contributed to either round 1 or 2 of the Delphi process.
The 76 included studies represented studies in 36 different countries across six different continents (Africa (5), Asia (4), Europe (21), North America (3), Oceania (2), and South America (1)). This is illustrated in Figure 1. Here, countries with national population-based cohorts are represented in dark gray whereas countries with any other study types (nonnational population-based, birth and twin cohorts, and others) are represented in light gray. Globally, accelerometry data are/will be collected in more than 275,000 adults. Sixteen percent of this total participant number is available from national population-based cohorts (Canada, Greenland, Hong Kong, Norway, Portugal, the United Kingdom, the United States, and Sweden) (see Table, Supplemental Digital Content 1, Overview of all identified studies with accelerometry data in adults, http://links.lww.com/MSS/A531).
FIGURE 1.
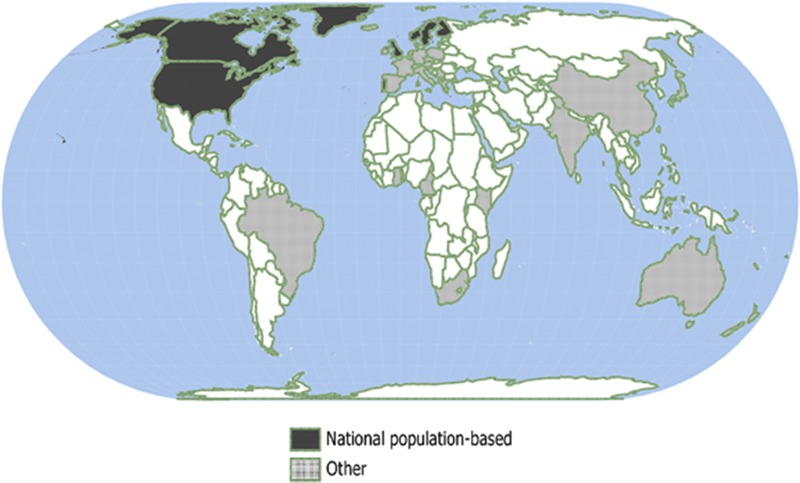
Global overview of countries with accelerometry data (n ≥ 400) in adults. Countries with national population-based cohorts are represented in dark gray (all with n > 1000), whereas countries with any other study types (i.e., nonnational population based, birth and twin cohorts, and other) are represented in light gray.
As shown in Figure 2A, more than one-third (38%) of the global pool of 277,370 adults with accelerometry data was collected using the Axivity accelerometer (Axivity Ltd., United Kingdom), with nearly one-third (30%) using different versions of the ActiGraph accelerometer, followed by smaller contributions from the Actiheart (CamNtech Ltd., United Kingdom), Actical (Philips Respironics), activPAL (PAL Technologies Ltd., United Kingdom), and GENEActiv (Activinsights Ltd., United Kingdom) monitors. When considered by studies using the monitors (Fig. 2B), more than half (51%) of studies have used an ActiGraph activity monitor, with 16% using the Actiheart monitor and 12% using the Actical monitor. Other monitors, including the Axivity accelerometer, were used in a minority of studies. A range of different anatomical positions have been used, including variations within monitor type (e.g., the ActiGraph monitor, which was worn on the hip, waist, lower back, and wrist) (see Table, Supplemental Digital Content 1, Overview of all identified studies with accelerometry data in adults, http://links.lww.com/MSS/A531).
FIGURE 2.
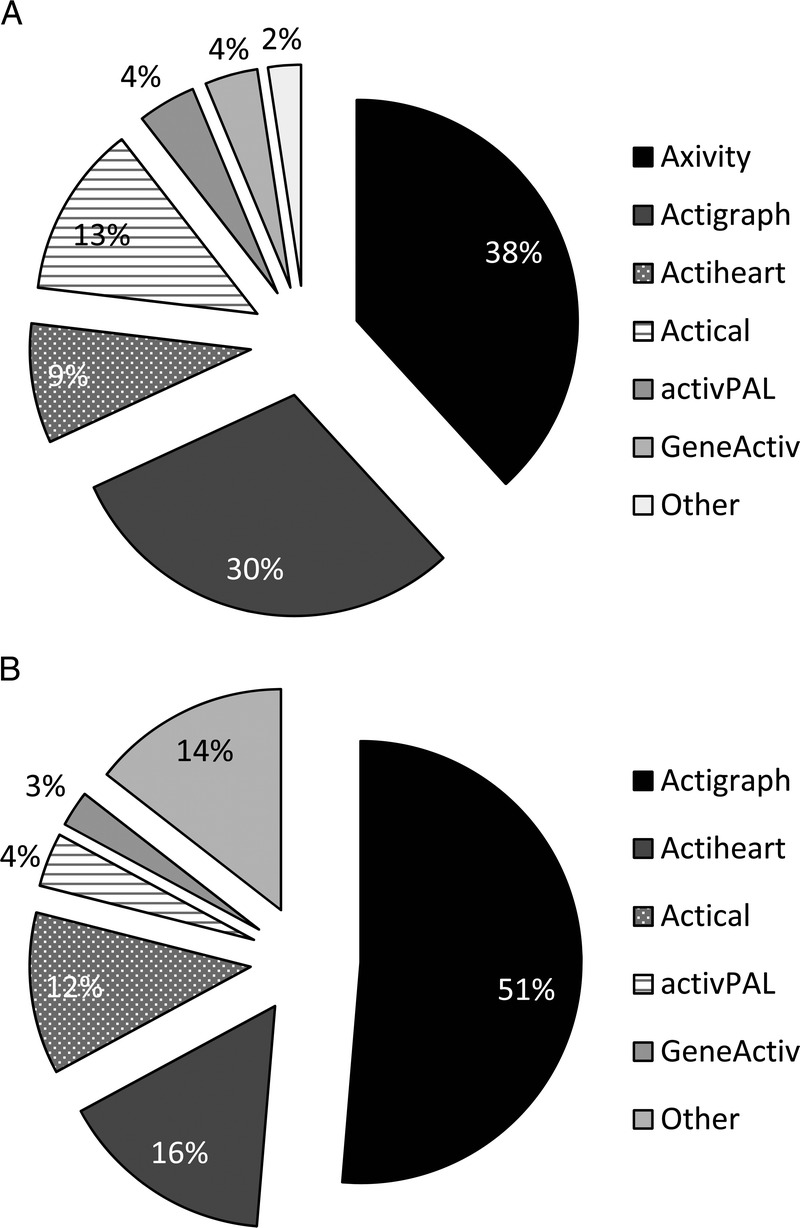
Contribution by sample size (A) or by study (B) of the different monitor types to the global pool of accelerometry data.
Summary
In summary, this comprehensive review highlights the enormous scope and potential of accelerometry data available, with data from more than 275,000 participants across 76 studies (with ≥400 participants) and 36 countries. North America, Europe, and Oceania are well represented in terms of available accelerometry data. Most other regions are less well represented, and investment in data collection in these regions will be important to understand variations between populations. Other important opportunities for future accelerometry data collection include an expansion in nationally representative cohorts, which are currently only available for North American and some European countries, Hong Kong, as well as follow-up of these national cohorts, which is currently lacking.
The analytical opportunities available with these data (both historic and in future data collections) along with the short- and long-term priorities, steps to take advantage of these opportunities, and ways to harmonize this diversity of data are discussed in Part B: An Expert Consensus on the Harmonization of Accelerometry Data.
PART B: DELPHI SURVEY. CONSENSUS FROM AN INTERNATIONAL EXPERT PANEL ON THE HARMONIZATION OF INTERNATIONAL PHYSICAL ACTIVITY DATA DERIVED FROM ACCELEROMETER-BASED ACTIVITY MONITORS
In October 2012, an invitation-only meeting was held at the 4th International Congress on Physical Activity and Health (Sydney, Australia) to discuss the potential opportunities to utilize the increasing amount of accelerometry data being collected internationally. As a result of that meeting (13 attendees from five countries), it was decided to run a Delphi process with the aim of achieving expert consensus on the harmonization of internationally available accelerometry data.
Methods
Participants
Twenty researchers (see Table, Supplemental Digital Content 2, Alphabetical list of the twenty individuals with recognized expertise in physical activity monitoring, epidemiological studies, surveillance, advocacy, and/or measurement expertise, who were invited to participate in the Delphi survey, http://links.lww.com/MSS/A532) with recognized expertise in physical activity monitoring, epidemiological studies, surveillance, advocacy, and/or measurement expertise were invited to participate in the survey.
Process
The Delphi expert consensus process consisted of two rounds. Both rounds were administered via an online questionnaire (Limeservice, https://www.limeservice.com/en/). Consistent with Delphi principles (16,38), responses were anonymous.
Round 1
In round 1, experts were given a brief overview of the aims of the study (as presented in the introduction) and were then asked to provide responses to the following five open-ended questions. They were also given the opportunity to provide any additional comments or observations with regard to the survey.
What do you consider to be the unique research opportunities for utilizing the large amount of internationally available activity monitor data?
Which additional data (i.e., other than activity monitor data) would this require?
What strategies do you think will be effective in enabling comparisons of activity monitor data between studies/countries, both for historical and future data collection?
What may be required to implement or progress such strategies?
Do you think that the development of an International Activity Monitor Database (IAMD), i.e., a global repository of objectively measured activity monitor data, would be a worthwhile/valuable investment? If no, please clarify. If yes, what would be the additional value of the IAMD?
Answers from the first round were then collated and summarized (K. Wi., S. S., and G. N. H.) and used to form the second online survey (round 2).
Round 2
In round 2, experts were asked to comment on the summary of the responses from round 1 and as appropriate, rank the responses provided in order of priority. On the basis of the responses provided, it was considered that no further rounds were required.
Ethics
The Delphi study was approved by the School of Population Health Ethics Committee, University of Queensland, Australia. Participants were provided with information about the study, and consent was required before commencing the survey. All experts who participated in the process were invited as coauthors.
Results
Characteristics of the expert panel
An overview of the characteristics of the expert panel is provided in Table 1. In round 1, 14 experts participated, in round 2, 16 experts participated, with 12 experts providing data for both rounds and 18 experts participating in either round.
Findings from the Delphi process
1. Unique research opportunities for utilizing the large amount of internationally available activity monitor data
The two key themes highlighted by the expert panel were the ability for cross-country/cross-population comparisons and the analytic opportunities available with the larger heterogeneity and the greater statistical power. More specifically, the unique research opportunities for utilizing the large amount of internationally available accelerometry data, as agreed by absolute consensus (100% of experts), were identified as follows:
the estimation and comparison of the prevalence of physical activity (levels and patterns) as well as trends over time (surveillance) around the world and in different contexts, including in populations that are typically underrepresented;
more statistically powerful etiological analyses on dose–response associations with health outcomes, including detection of more subtle associations, consistency of associations across populations, and gene–environment interactions; and
more comprehensive and powerful analyses of the correlates/determinants of physical activity and identification of target groups for future intervention.
2. Collection of data in addition to the accelerometry data
In the first round of the Delphi survey, the participants’ responses regarding the additional data that should be collected in addition to the accelerometry data fell into nine different categories. During the second round, participants were asked to indicate the categories they considered essential to be included in data pooling. For any categories deemed nonessential, participants indicated the level of scientific priority and feasibility of harmonization. Table 2 provides an overview of all nine categories, with categories presented in order of priority (i.e., most essential listed first).
TABLE 2.
Additional data, other than accelerometry data, required (most essential listed first).
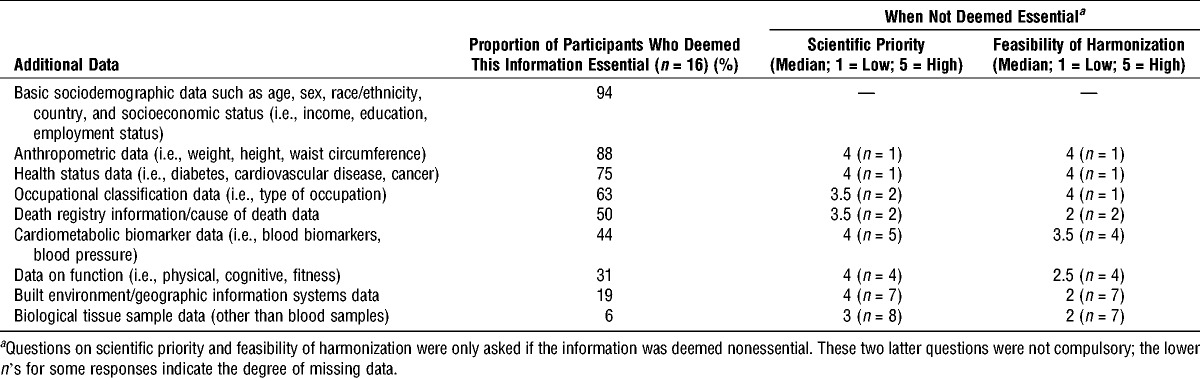
In summary, there was strong agreement on the necessity of basic sociodemographic and anthropometric data and most participants also rated health status and occupational classification data as essential to pool. Half or less than half of participants deemed data on death registration, cardiometabolic profile, function (physical, cognitive, and fitness), the environment, and biological tissue sample data as essential. However, although these items were deemed nonessential, participants rated their scientific priority as relatively high (median, ≥3 for each category), indicating that adding these data would be of significant value. The dependence between data necessity and research aims was raised, with surveillance applications generally requiring less information to be pooled. Most items rated highly essential were perceived to be relatively feasible to harmonize between studies. In contrast, participants indicated that less essential items may be less feasible to harmonize and pool. Notably, the questions relating to scientific priority and feasibility of harmonization (for data considered nonessential) were not compulsory, and therefore, not all experts provided responses for these (Table 2). For categories such as death registry information, differences in data quality between countries/studies were acknowledged as a consideration. Other categories, such as environmental data, were rated as nonfeasible, given the high volume of work required to process and harmonize such data. Cost and potential deterrence of studies participating in a pooling effort were other salient characteristics raised, especially for categories such as biological tissue sample data.
3. Effective strategies enabling comparisons of activity monitor data between studies/countries
In general, there was strong consensus that standardization of monitor calibration, data collection, data processing, and data analytical procedures are needed. Disclosure of monitor information and protocols for data collection and processing were deemed essential to enable comparison, with access to raw (i.e., unprocessed waveform) data preferred.
3a. Historically collected data
Following responses from the first round of the survey, two different approaches were broadly proposed for historically collected data, specifically as follows:
centralized reprocessing of the highest resolution of data with uniform methodology based on a developed consensus and
decentralized reprocessing by the original researchers on their own data with uniform methodology, relative to the different research questions of interest and meta-analysis of results.
Participants were asked which approach was preferable and why. As shown in Table 3, the vast majority of experts preferred centralized reprocessing of data, followed by a preference for a mixed approach (i.e., providing either option for the researcher), then for decentralized data reprocessing. Table 3 also summarizes the perceived benefits, caveats, and facilitating utilities needed for each of the proposed approaches, as indicated by the experts.
TABLE 3.
Preferred approach, perceived benefits and caveats of the approach, as well as utilities needed to enable comparisons of historically collected accelerometry data (n = 16).
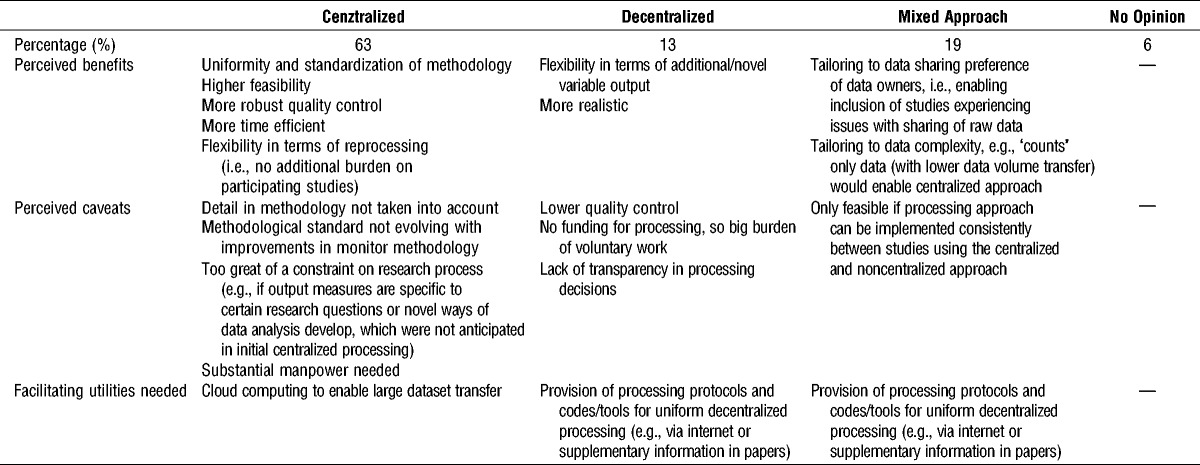
Four additional strategies were identified as important for enabling comparisons of the historically collected data. In order of priority, these were the following:
the availability of raw signal data instead of proprietary data processing and outputs (e.g., “counts”), where possible (and transparency where not);
development of criteria to determine the types of monitor that data can be pooled;
disclosure of data collection protocols; and
standardization of cut points within each monitor type/model.
3b. Future data collection
The panel (n = 16) identified five main strategies to enable comparison of monitor data collected in the future. The two main priorities identified were the following:
the development, public availability, and ensured implementation of standardized protocols, tools, and analytical methods and
the use of raw signal data (rather than outputs resulting from proprietary data processing).
The secondary priorities identified were the following:
obtaining better wear compliance;
ensuring data collection in representative samples; and
convergence in terms of monitor types used.
4. Requirements for implementation of these strategies
In general, the following three key requirements for the implementation of these strategies were highlighted:
communication and consensus among researchers;
development of an online infrastructure; and
methodological comparison work.
For the online infrastructure, user friendliness and high-speed access, capacity to host a database (with adequate data storage space) and data sharing agreements, as well as capacity for centralized data processing and analysis were identified as potentially important characteristics. Modifying or adapting existing accelerometry data processing systems (e.g., MOVE-e-Cloud (Newcastle University, United Kingdom), DataSHaPER (http://www.datashaper.org), MeterPlus (Santech, Inc.), KineSoft (Loughborough, United Kingdom, http://www.kinesoft.org)), which are already available or in development, was generally preferred because this was deemed more efficient, robust, and financially viable.
For methodological comparison work, standardization and harmonization of methods and procedures for data collection, processing, and analysis were deemed important. The following two components were highlighted as key requirements:
Convergent validity studies (particularly free living) to establish models to equate outputs from different monitors, anatomical sites, decision rules, etc. A global Web-based dashboard is needed to map what has been done and what needs doing, as this is work in progress; and
An international consensus process, potentially in the form of an international task force, to define, publish, and publicize internationally agreed standards for collection and processing of data.
Strong support was identified for the organization of an international consensus to set standards as mentioned previously, acknowledging that this would be a worthwhile but challenging process. Considerations raised included the necessity of scrutinizing agreed standards before implementation to ensure that they result in valid activity parameters, to allow for multiple standards for different purposes, to involve a sufficiently wide range of experts, to avoid overly strict standards imposing on researchers’ creativity, and to ensure that standards are updated to keep pace with changing technology.
Participants indicated that convergent validation research would benefit from a well-structured approach, potentially in the form of a separately funded program of coherent and coordinated studies. A global Web-based dashboard would need to clearly characterize the knowledge already gathered, including quantification of uncertainty and what is still unknown. Some participants anticipated that the potential increase in the use of wrist-worn monitors collecting raw acceleration signals may diminish the need for convergent validity studies in the future.
5. Value of an IAMD, i.e., a global repository of objectively measured activity monitor data
There was full (100%) consensus that an IAMD would be beneficial and worthwhile but that the success of this would be dependent on several factors, including the following:
the development/existence of strong international standards for data collection, management, and analysis, which are published and easily accessible;
sufficient quality control and good governance;
perception from data contributors that their contribution is worthwhile; and
perception that the benefits for researchers in general are greater than the resources required to develop an IAMD.
5a. Priorities and aims of an IAMD
The following three key short-term priorities were proposed:
The development of goals and strong international standards and protocols for data collection, management, analysis, and quality assurance. This could be facilitated through a working group holding consultations at various international conferences.
Securing funding to start with a demonstration project involving a limited number (e.g., 10) of studies/countries involved, which has a relatively simple objective as a proof of principle, before increasing complexity. Such a demonstration project could, for example, only include a few accelerometry brands and primarily focus on mapping between those.
Commence examination of the equivalence between monitors, anatomical sites, etc. as well as harmonization of variable naming conventions.
The following four key long-term priorities were proposed:
Securing funding to support an IAMD and to ensure its long-term sustainability.
Creating a widespread appreciation among researchers of the importance of following the international standards and protocols for data collection, management, analysis, and quality assurance, as developed in the short term, and of providing their data to an IAMD. This could be facilitated by ensuring easy data access for investigator-driven research use, such as in the National Health and Nutrition Examination Survey dataset (http://www.cdc.gov/nchs/nhanes.htm).
Building international capacities and recruiting multiple countries, following examples such as the International Physical Activity and the Environment Network project (44).
Keeping a strong emphasis on quality control throughout this process.
Several potential mechanisms were suggested to enable high-quality control and wider scrutiny of the whole process. These included utilities to ensure easy accessibility to the internationally established standards and protocols, the development of minimum criteria for information sharing at each level of the process (e.g., logs of routine calibration checks for raw data), sharing information and protocols (e.g., syntaxes) in the public domain, and setting up a data monitoring council. Methodologically, moving on to more generalized inference on body movement including all accelerometry data was considered a long-term priority. Other types of biosignals (such as temperature, HR, breathing etc.) could be included in the inference of generalized body movement information in the long run to keep up with new measurement approaches.
5b. Potential funding sources for an IAMD
1. Short-term funding
A variety of potential sources was identified by participants as options for short-term funding. These included national funding bodies, some of which provide specific international network/collaboration grants, such as the Wellcome Trust (United Kingdom), Bupa Foundation (Australia), US National Institutes of Health, the Leverhulme Trust (United Kingdom), Economic and Social Research Council (United Kingdom), and large philanthropic groups. Funding from individual countries and international funding sources, such as European project funding and the World Health Organization (WHO), were also proposed. The possibility of partial cost absorption by local departments in the initial stages was suggested as well. Finally, because many funders typically do not like to fund international studies, the idea to focus the IAMD database to a certain health outcome to increase attractiveness to specific funders was also brought forward.
2. Long-term funding
In general, suggestions for long-term funding predominantly involved international funding bodies, some of which focus on advancing global health, such as the WHO, the National Institutes of Health Fogarty International Center, the United Nations, the European Union, large philanthropic groups, and international consortia of research councils, with industry funding being another proposed candidate.
5c. Governance of an IAMD
Other large international projects, including multicountry self-report data collection initiatives, were recommended as important models to follow when organizing an IAMD (e.g., International Physical Activity Questionnaire (https://sites.google.com/site/theipaq/), WHO STEPS chronic disease risk factor surveillance, and the Global Physical Activity Questionnaire (http://www.who.int/chp/steps/en/index.html). An important common element in each of these projects is that they involve substantial manpower and require a dedicated team of full-time staff. Securing funding for a coordinating center, which provides sufficient resources and support staff, was therefore suggested. In addition, installation of an advisory board consisting of a strong group of high-level, well-connected experts to oversee the development of the IAMD was proposed. In general, the governance structure would need representation of researchers from multiple countries involved. Capacity-building resources enabling face-to-face meetings were recommended because they may provide a lot of momentum to the project.
Discussion
This article reported on the findings from a comprehensive review describing the scope of accelerometry data collected internationally from adults and conclusions from an expert consensus regarding the most optimal strategies to harmonize international accelerometry data.
The review—which included data from both published and ongoing studies—highlighted the now-considerable amount of accelerometry data available internationally, with data collected from more than 275,000 participants across 36 countries. As such, it provides an important resource for identifying not only opportunities with the existing data but also evidence gaps, which could direct future data collection priority areas/countries. The review also highlighted the multitude of accelerometer-based activity monitors, models, and attachment procedures used across studies. Of note is that although comprehensive, it was not a systematic review and relevant studies may have been missed.
The expert consensus provided strategies and short- and long-term priorities as well as potential funding sources for addressing the current challenges in comparing the data across studies and populations. A key strength of the consensus was the inclusion of experts (median of 18 yr of expertise in physical activity) across a diverse range of physical activity interest areas. However, it should be noted that not all experts in the field were contacted for inclusion in the Delphi process, which may have resulted in some key considerations, strategies, priorities, and/or funding sources being misrepresented in terms of priorities or even remaining unidentified. For example, one consideration not made explicit during the Delphi process is the wide variety of calibration procedures that have been used for different monitor types (e.g., locomotion calibration, multiple activity type calibration)—most of which are laboratory-based studies, with some studies using free-living protocols. Harmonization of existing data without reprocessing will require the use of scoring approaches that were derived from the same type of calibration studies.
Notably, some of the strategies identified through the consensus are already occurring. This includes data pooling (such as in the ICAD [63] and the DEDIPAC European knowledge hub: https://www.dedipac.eu/) and standardization (such as through the Sensor Methods Collaboratory [70], the Sittonomy [9]), and the Database of Genotypes and Phenotypes (dbGaP, http://www.ncbi.nlm.nih.gov/gap). Given the rapid evolution of both monitor technology and methodology, regular revision (e.g., every 3 yr) of the key priorities and most optimal strategies to harmonize international accelerometry data is recommended.
In summary, the accelerometry data collected across the globe provide a key opportunity to further understand the distribution, determinants, health effects, and burden of disease for physical activity across the intensity spectrum as well as how these may vary between subgroups and populations. By identifying the scope of the data available and obtaining an expert consensus on the strategies, priorities, and potential funding sources, this article provides a foundational resource to maximize this opportunity.
Supplementary Material
Acknowledgments
This work and authors involved in this work were supported by the United Kingdom Medical Research Council (grants MC_UU_12015/3 and MRC Centenary Award to K. Wi., S. B.), the British Heart Foundation (grant FS/12/58/29709 to K. Wi.), the Australian Heart Foundation (grant PH 12B 7054 to G. N. H.), the Australian National Health and Medical Research Council (fellowship to N. O., program grant to N. O., and National Health and Medical Research Council Centre for Research Excellence Grant in the Translational Science of Sedentary Behaviour APP1041056 to G. N. H., N. O., and D. D.), an Australian postgraduate award (to S. S.), the Coca-Cola Company, Body Media, US National Institutes of Health and Technogym (to S. B.), MRC, Chartered Society of Physiotherapy, Engineering, and Physical Sciences Research Council, Greater Manchester Academic Health Science Network (to M. G.), and Australian Research Council (Future Fellowship, FT100100918, to D. D.).
D. E. is the founder and CEO of KineSoft, an accelerometry analytics software; S. N. B. is supported by unrestricted research grants from the University of South Carolina from the Coca-Cola Company, Body Media, and Technogym; M. H. G. is the director of PAL Technologies Ltd., Glasgow, United Kingdom; and Soren Brage is an advisor for the UK Biobank.
The results of the present study do not constitute endorsement by the American College of Sports Medicine.
Footnotes
Supplemental digital content is available for this article. Direct URL citations appear in the printed text and are provided in the HTML and PDF versions of this article on the journal’s Web site (www.acsm-msse.org).
REFERENCES
- 1. Aresu M, Becares L, Brage S, et al. Health Survey for England 2008—Volume 1 Physical Activity and Fitness. Leeds (United Kingdom): NHS Information Centre; 2009. p. 385. [Google Scholar]
- 2. Arnardottir NY, Koster A, Van Domelen DR, et al. Objective measurements of daily physical activity patterns and sedentary behaviour in older adults: age, gene/environment susceptibility-Reykjavik study. Age Ageing. 2013; 42 (2): 222– 9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3. Assah FK, Ekelund U, Brage S, Mbanya JC, Wareham NJ. Urbanization, physical activity, and metabolic health in sub-Saharan Africa. Diabetes Care. 2011; 34 (2): 491– 6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4. Ayabe M, Yahiro T, Yoshioka M, Higuchi H, Higaki Y, Tanaka H. Objectively measured age-related changes in the intensity distribution of daily physical activity in adults. J Phys Act Health. 2009; 6 (4): 419– 25. [DOI] [PubMed] [Google Scholar]
- 5. Baptista F, Santos DA, Silva AM, et al. Prevalence of the Portuguese population attaining sufficient physical activity. Med Sci Sports Exerc. 2012; 44 (3): 466– 73. [DOI] [PubMed] [Google Scholar]
- 6. Bento TC, Romero F, Leitão JC, Mota MP. Portuguese adults’ physical activity during different periods of the year. Eur J Sport Sci. 2014; 14: S352– 60. [DOI] [PubMed] [Google Scholar]
- 7. Buman MP, Hekler EB, Haskell WL, et al. Objective light-intensity physical activity associations with rated health in older adults. Am J Epidemiol. 2010; 172 (10): 1155– 65. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8. Burgoine T, Forouhi NG, Griffin SJ, Wareham NJ, Monsivais P. Associations between exposure to takeaway food outlets, takeaway food consumption, and body weight in Cambridgeshire, UK: population based, cross sectional study. BMJ. 2014; 348: g1464. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9. Chastin SF, Schwarz U, Skelton DA. Development of a consensus taxonomy of sedentary behaviors (SIT): report of Delphi Round 1. PLoS One. 2013; 8 (12): e82313. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10. Christensen DL, Faurholt-Jepsen D, Boit MK, et al. Cardiorespiratory fitness and physical activity in Luo, Kamba, and Maasai of rural Kenya. Am J Hum Biol. 2012; 26 (6): 723– 9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11. Coleman KJ, Rosenberg DE, Conway TL, et al. Physical activity, weight status, and neighborhood characteristics of dog walkers. Prev Med. 2008; 47 (3): 309– 12. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12. Colley RC, Garriguet D, Janssen I, Craig CL, Clarke J, Tremblay MS. Physical activity of Canadian adults: accelerometer results from the 2007 to 2009 Canadian Health Measures Survey. Health Rep. 2011; 22 (1): 7– 14. [PubMed] [Google Scholar]
- 13. Coulon SM, Wilson DK, Egan BM. Associations among environmental supports, physical activity, and blood pressure in African-American adults in the PATH trial. Soc Sci Med. 2013; 87: 108– 15. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14. da Silva IC, van Hees VT, Ramires VV, et al. Physical activity levels in three Brazilian birth cohorts as assessed with raw triaxial wrist accelerometry. Int J Epidemiol. 2014; 43: 1959– 68. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15. Dahl-Petersen IK, Bjerregaard P, Brage S, Jørgensen ME. Physical activity energy expenditure is associated with 2-h insulin independently of obesity among Inuit in Greenland. Diabetes Res Clin Pract. 2013; 102 (3): 242– 9. [DOI] [PubMed] [Google Scholar]
- 16. Dalkey N, Helmer O. An experimental application of the Delphi method to the use of experts. Manage Sci. 1963; 9 (3): 458– 67. [Google Scholar]
- 17. Dallal CM, Brinton LA, Matthews CE, et al. Accelerometer-based measures of active and sedentary behavior in relation to breast cancer risk. Breast Cancer Res Treat. 2012; 134 (3): 1279– 90. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18. de Mutsert R, den Heijer M, Rabelink TJ, et al. The Netherlands Epidemiology of Obesity (NEO) study: study design and data collection. Eur J Epidemiol. 2013; 28 (6): 513– 23. [DOI] [PubMed] [Google Scholar]
- 19. den Hoed M, Brage S, Zhao JH, et al. Heritability of objectively assessed daily physical activity and sedentary behavior. Am J Clin Nutr. 2013; 98 (5): 1317– 25. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20. Denkinger MD, Lukas A, Herbolsheimer F, Peter R, Nikolaus T. Physical activity and other health-related factors predict health care utilisation in older adults: the ActiFE Ulm study. Z Gerontol Geriatr. 2012; 45 (4): 290– 7. [DOI] [PubMed] [Google Scholar]
- 21. Dunstan DW, Thorp AA, Healy GN. Prolonged sitting: is it a distinct coronary heart disease risk factor? Curr Opin Cardiol. 2011; 26 (5): 412– 9. [DOI] [PubMed] [Google Scholar]
- 22. Ekelund U, Luan J, Sherar LB, et al. Moderate to vigorous physical activity and sedentary time and cardiometabolic risk factors in children and adolescents. JAMA. 2012; 307 (7): 704– 12. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23. Evenson KR, Sotres-Alvarez D, Deng Y, et al. Accelerometer adherence and performance in a cohort study of US Hispanic adults. Med Sci Sports Exerc. 2014; 47 (4): 725– 34. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24. Fraser A, Macdonald-Wallis C, Tilling K, et al. Cohort profile: the Avon Longitudinal Study of Parents and Children: ALSPAC mothers cohort. Int J Epidemiol. 2013; 42 (1): 97– 110. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25. Gando Y, Yamamoto K, Murakami H, et al. Longer time spent in light physical activity is associated with reduced arterial stiffness in older adults. Hypertension. 2010; 56 (3): 540– 6. [DOI] [PubMed] [Google Scholar]
- 26. Garcia-Ortiz L, Recio-Rodriguez JI, Martin-Cantera C, et al. Physical exercise, fitness and dietary pattern and their relationship with circadian blood pressure pattern, augmentation index and endothelial dysfunction biological markers: EVIDENT study protocol. BMC Public Health. 2010; 10: 233. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27. Glazer NL, Lyass A, Esliger DW, et al. Sustained and shorter bouts of physical activity are related to cardiovascular health. Med Sci Sports Exerc. 2013; 45 (1): 109– 15. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28. Golubic R, Martin KR, Ekelund U, et al. Levels of physical activity among a nationally representative sample of people in early old age: results of objective and self-reported assessments. Int J Behav Nutr Phys Act. 2014; 11: 58. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29. Gordon-Larsen P, Boone-Heinonen J, Sidney S, Sternfeld B, Jacobs DR, Jr, Lewis CE. Active commuting and cardiovascular disease risk: the CARDIA study. Arch Intern Med. 2009; 169 (13): 1216– 23. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30. Hagströmer M, Oja P, Sjöström M. Physical activity and inactivity in an adult population assessed by accelerometry. Med Sci Sports Exerc. 2007; 39 (9): 1502– 8. [DOI] [PubMed] [Google Scholar]
- 31. Hamer M, Venuraju SM, Urbanova L, Lahiri A, Steptoe A. Physical activity, sedentary time, and pericardial fat in healthy older adults. Obesity (Silver Spring). 2012; 20 (10): 2113– 7. [DOI] [PubMed] [Google Scholar]
- 32. Hansen BH, Kolle E, Dyrstad SM, Holme I, Anderssen SA. Accelerometer-determined physical activity in adults and older people. Med Sci Sports Exerc. 2012; 44 (2): 266– 72. [DOI] [PubMed] [Google Scholar]
- 33. Harris T, Kerry SM, Victor CR, et al. PACE-UP (pedometer and consultation evaluation—UP)—a pedometer-based walking intervention with and without practice nurse support in primary care patients aged 45–75 years: study protocol for a randomised controlled trial. Trials. 2013; 14: 418. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34. Hayat SA, Luben R, Keevil VL, et al. Cohort profile: a prospective cohort study of objective physical and cognitive capability and visual health in an ageing population of men and women in Norfolk (EPIC-Norfolk 3). Int J Epidemiol. 2014; 43 (4): 1063– 72. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35. Henson J, Yates T, Biddle SJ, et al. Associations of objectively measured sedentary behaviour and physical activity with markers of cardiometabolic health. Diabetologia. 2013; 56 (5): 1012– 20. [DOI] [PubMed] [Google Scholar]
- 36. Hesketh KR, Goodfellow L, Ekelund U, et al. Activity levels in mothers and their preschool children. Pediatrics. 2014; 133 (4): e973– 80. [DOI] [PubMed] [Google Scholar]
- 37. Howard VJ, Rhodes JD, Hutto B, et al. Successful use of telephone and mail for obtaining usable accelerometer data from a national cohort: the experience of the Reasons for Geographical and Racial Differences in Stroke (REGARDS) study. Circulation. 2013; 127: AP145. [Google Scholar]
- 38. Hsu C, Sandford BA. The Delphi technique: making sense of consensus. Pract Assess Res Eval. 2007; 12 (10): 1– 8. [Google Scholar]
- 39. Husu P, Suni J, Vähä-Ypyä H, et al. Suomalaisten aikuisten kiihtyvyysmittarilla mitattu fyysinen aktiivisuus ja liikkumattomuus. Suomen lääkärilehti (Finnish Med J). 2014; 69 (25–32): 1871– 7. [Google Scholar]
- 40. Inoue S, Ohya Y, Odagiri Y, et al. Characteristics of accelerometry respondents to a mail-based surveillance study. J Epidemiol. 2010; 20 (6): 446– 52. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41. Jefferis BJ, Sartini C, Lee IM, et al. Adherence to physical activity guidelines in older adults, using objectively measured physical activity in a population-based study. BMC Public Health. 2014; 14: 382. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42. Kang B, Moudon AV, Hurvitz PM, Reichley L, Saelens BE. Walking objectively measured: classifying accelerometer data with GPS and travel diaries. Med Sci Sports Exerc. 2013; 45 (7): 1419– 28. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43. Katzmarzyk PT. Standing and mortality in a prospective cohort of Canadian adults. Med Sci Sports Exerc. 2014; 46 (5): 940– 6. [DOI] [PubMed] [Google Scholar]
- 44. Kerr J, Sallis JF, Owen N, et al. Advancing science and policy through a coordinated international study of physical activity and built environments: IPEN adult methods. J Phys Act Health. 2013; 10 (4): 581– 601. [DOI] [PubMed] [Google Scholar]
- 45. Kim J, Tanabe K, Yokoyama N, Zempo H, Kuno S. Association between physical activity and metabolic syndrome in middle-aged Japanese: a cross-sectional study. BMC Public Health. 2011; 11: 624. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46. Kozàkovà M, Palombo C, Morizzo C, Nolan JJ, Konrad T, Balkau B. Effect of sedentary behaviour and vigorous physical activity on segment-specific carotid wall thickness and its progression in a healthy population. Eur Heart J. 2010; 31 (12): 1511– 9. [DOI] [PubMed] [Google Scholar]
- 47. Kwon S, Janz KF, International Children’s Accelerometry Database C. Tracking of accelerometry-measured physical activity during childhood: ICAD pooled analysis. Int J Behav Nutr Phys Act. 2012; 9: 68. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48. Lee IM, Shiroma EJ. Using accelerometers to measure physical activity in large-scale epidemiological studies: issues and challenges. Br J Sports Med. 2014; 48 (3): 197– 201. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49. Lee IM, Shiroma EJ, Lobelo F, Puska P, Blair SN, Katzmarzyk PT. Effect of physical inactivity on major non-communicable diseases worldwide: an analysis of burden of disease and life expectancy. Lancet. 2012; 380 (9838): 219– 29. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50. Lee PH, Yu YY, McDowell I, Leung GM, Lam TH. A cluster analysis of patterns of objectively measured physical activity in Hong Kong. Public Health Nutr. 2013; 16 (8): 1436– 44. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51. Loprinzi PD. Objectively measured light and moderate-to-vigorous physical activity is associated with lower depression levels among older US adults. Aging Ment Health. 2013; 17 (7): 801– 5. [DOI] [PubMed] [Google Scholar]
- 52. Luke A, Bovet P, Forrester TE, et al. Protocol for the modeling the epidemiologic transition study: a longitudinal observational study of energy balance and change in body weight, diabetes and cardiovascular disease risk. BMC Public Health. 2011; 11: 927. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53. Moore C, Sambrook J, Walker M, et al. The INTERVAL trial to determine whether intervals between blood donations can be safely and acceptably decreased to optimise blood supply: study protocol for a randomised controlled trial. Trials. 2014; 15: 363. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54. Murakami H, Iemitsu M, Sanada K, et al. Associations among objectively measured physical activity, fasting plasma homocysteine concentration, and MTHFR C677T genotype. Eur J Appl Physiol. 2011; 111 (12): 2997– 3005. [DOI] [PubMed] [Google Scholar]
- 55. Oakes JM, Forsyth A, Schmitz KH. The effects of neighborhood density and street connectivity on walking behavior: the Twin Cities walking study. Epidemiol Perspect Innov. 2007; 4: 16. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 56. Ostbye T, Stroo M, Brouwer RJ, et al. The steps to health employee weight management randomized control trial: rationale, design and baseline characteristics. Contemp Clin Trials. 2013; 35 (2): 68– 76. [DOI] [PubMed] [Google Scholar]
- 57. Panter J, Griffin S, Ogilvie D. Correlates of reported and recorded time spent in physical activity in working adults: results from the commuting and health in Cambridge study. PLoS One. 2012; 7 (7): e42202. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 58. Paul DR, Kramer M, Stote KS, et al. Estimates of adherence and error analysis of physical activity data collected via accelerometry in a large study of free-living adults. BMC Med Res Methodol. 2008; 8: 38. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 59. Peters T, Brage S, Westgate K, et al. Validity of a short questionnaire to assess physical activity in 10 European countries. Eur J Epidemiol. 2012; 27 (1): 15– 25. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 60. Peters TM, Moore SC, Xiang YB, et al. Accelerometer-measured physical activity in Chinese adults. Am J Prev Med. 2010; 38 (6): 583– 91. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 61. Schram MT, Sep SJ, van der Kallen CJ, et al. The Maastricht study: an extensive phenotyping study on determinants of type 2 diabetes, its complications and its comorbidities. Eur J Epidemiol. 2014; 29 (6): 439– 51. [DOI] [PubMed] [Google Scholar]
- 62. Shephard RJ, Park H, Park S, Aoyagi Y. Objectively measured physical activity and progressive loss of lean tissue in older Japanese adults: longitudinal data from the Nakanojo study. J Am Geriatr Soc. 2013; 61 (11): 1887– 93. [DOI] [PubMed] [Google Scholar]
- 63. Sherar LB, Griew P, Esliger DW, et al. International children’s accelerometry database (ICAD): design and methods. BMC Public Health. 2011; 11: 485. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 64. Sigmund E, De Ste Croix M, Miklánkova L, Frömel K. Physical activity patterns of kindergarten children in comparison to teenagers and young adults. Eur J Public Health. 2007; 17 (6): 646– 51. [DOI] [PubMed] [Google Scholar]
- 65. Smitherman TA, Dubbert PM, Grothe KB, et al. Validation of the Jackson heart study physical activity survey in African Americans. J Phys Act Health. 2009; 6: S124– 32. [DOI] [PubMed] [Google Scholar]
- 66. Sundquist K, Eriksson U, Kawakami N, Skog L, Ohlsson H, Arvidsson D. Neighborhood walkability, physical activity, and walking behavior: the Swedish Neighborhood and Physical Activity (SNAP) study. Soc Sci Med. 2011; 72 (8): 1266– 73. [DOI] [PubMed] [Google Scholar]
- 67. Tanamas SK, Magliano DJ, Lynch BM, et al. The Australian Diabetes, Obesity and Lifestyle Study. Melbourne (Australia): Baker IDI; 2013. [Google Scholar]
- 68. Thorp AA, Owen N, Neuhaus M, Dunstan DW. Sedentary behaviors and subsequent health outcomes in adults: a systematic review of longitudinal studies, 1996–2011. Am J Prev Med. 2011; 41 (2): 207– 15. [DOI] [PubMed] [Google Scholar]
- 69. Troiano RP, Berrigan D, Dodd KW, Mâsse LC, Tilert T, McDowell M. Physical activity in the United States measured by accelerometer. Med Sci Sports Exerc. 2008; 40 (1): 181– 8. [DOI] [PubMed] [Google Scholar]
- 70. Troiano RP, McClain JJ, Brychta RJ, Chen KY. Evolution of accelerometer methods for physical activity research. Br J Sports Med. 2014; 48 (13): 1019– 23. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 71. Tudor-Locke C, Johnson WD, Katzmarzyk PT. Accelerometer-determined steps per day in US adults. Med Sci Sports Exerc. 2009; 41 (7): 1384– 91. [DOI] [PubMed] [Google Scholar]
- 72. Van Dyck D, Cardon G, Deforche B, Sallis JF, Owen N, De Bourdeaudhuij I. Neighborhood SES and walkability are related to physical activity behavior in Belgian adults. Prev Med. 2010; 50 (1 Suppl): S74– 9. [DOI] [PubMed] [Google Scholar]
- 73. Webber LS, Rice JC, Johnson CC, Rose D, Srinivasan SR, Berenson GS. Cardiovascular risk factors and physical activity behavior among elementary school personnel: baseline results from the ACTION! worksite wellness program. J Sch Health. 2012; 82 (9): 410– 6. [DOI] [PubMed] [Google Scholar]
- 74. Witten K, Blakely T, Bagheri N, et al. Neighborhood built environment and transport and leisure physical activity: findings using objective exposure and outcome measures in New Zealand. Environ Health Perspect. 2012; 120 (7): 971– 7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 75. Yoshioka M, Ayabe M, Yahiro T, et al. Long-period accelerometer monitoring shows the role of physical activity in overweight and obesity. Int J Obes (Lond). 2005; 29 (5): 502– 8. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.