

Abstract
Patient: Male, 68
Final Diagnosis: Unusual clinical course
Symptoms: None
Medication: —
Clinical Procedure: Angio CT
Specialty: Surgery
Objective:
Challenging differential diagnosis
Background:
High-resolution contrast-enhanced ultrasound is one of methods used in the detection and characterization of endoleaks, which is a frequent complication after EVAR. A new technology provided by Toshiba’s AplioTM 500 ultrasound system, called Superb Micro-Vascular Imaging (SMI), is dedicated specifically to imaging very low flow states and appears to be a promising new method for detection of endoleaks.
Case Report:
After endovascular treatment, a 68-year-old patient who had stent-graft implantation underwent clinical examinations, including contrast-enhanced ultrasound (CEUS), superb micro-vascular imaging (SMI), and computed tomographic angiography (CTA), revealing additional information about abnormal blood flow localized in the periphery of the sack of the left common iliac artery aneurysm. By using CEUS and SMI, the endoleak was clearly visible.
Conclusions:
This case report illustrates the potential clinical value of this advanced Doppler technology (SMI) and how it could influence clinical management.
MeSH Keywords: Endoleak; Endovascular Procedures; Ultrasonography, Doppler
Background
Ultrasound is non-invasive imaging method that is used as a first-line examination to diagnose disease and rapidly develop treatment plans, especially in vascular imaging where precise hemodynamic data are crucial. Clinically significant challenges exist in detecting small or microflow conditions without the use of contrast media [1].
Toshiba’s AplioTM 500 ultrasound system provides a new technology, specifically for imaging very low flow states. This new feature, called superb micro-vascular imaging (SMI), is an innovative ultrasound Doppler technique. There are several benefits of SMI: low-velocity flow visualization, high resolution of image, minimal motion artefact, and high frame rates. This innovative vascular imaging technique can visualize smaller vessels and lower-velocity blood flows without the use of contrast medium [2].
The primary goal of conventional Doppler techniques is visualizing blood flows at higher resolution. SMI is able to visualize lower-velocity blood flows without the negative impact of the presence of extraneous Doppler signals (motion artefacts) arising from nearby structures. Conventional Doppler techniques are unable to distinguish these motion artefacts from actual blood flow.
The SMI technique is available in 2 modes:
cSMI – The color mode: demonstrates B-mode and color information simultaneously;
mSMI – The monochrome (grayscale) mode: improving sensitivity by subtracting the background information, and focuses only on the vasculature [2].
Case Report
A 68-year-old man with diagnosed bilateral common iliac artery aneurysm was admitted to the hospital for endovascular treatment. Common iliac artery aneurysms were found during the computed tomographic angiography (CTA). He also had hypertension and hyperlipidemia. The patient reported that he had never smoked cigarettes. The size of the right iliac artery aneurysm, measured based on CTA, was 57 mm, and the left was 37 mm. The abdominal aorta was not widened, and was 21 mm. The patient was advised to undergo stent-graft implantation within the next year.
The abdominal aneurysm was repaired through the deployment of a 28×12 mm COOK device with a 12-mm contralateral limb. No endoleak was found on a final angiogram. The procedure was completed successfully.
Doppler ultrasonography (DUS) was performed on the 4th day after the stent-graft implantation. The DUS examination was performed by an experienced vascular surgeon using Toshiba’s AplioTM 500, equipped with a 4–6 MHz curved-array transducer.
The first part of the examination was a standard morphological investigation in 2D presentation (B-mode) followed by the blood flow analysis using color Doppler, power Doppler, and advanced dynamic flow (ADF) modality. The second part was a cSMI and mSMI approach. Finally, the CEUS was performed after the administration of an intravenous bolus of 2 mL of ultrasound contrast SonoVue (Bracco, Italy). During the B-mode examination the correct location of the stent-graft and the preserved continuity of its walls were clearly visible, while the color Doppler, power Doppler, and ADF examination revealed the presence of blood flow around the lumen of the stent-graft. The blood follow inside of the sack of the aneurysm was not observed (Figure 1A–1C).
Figure 1.
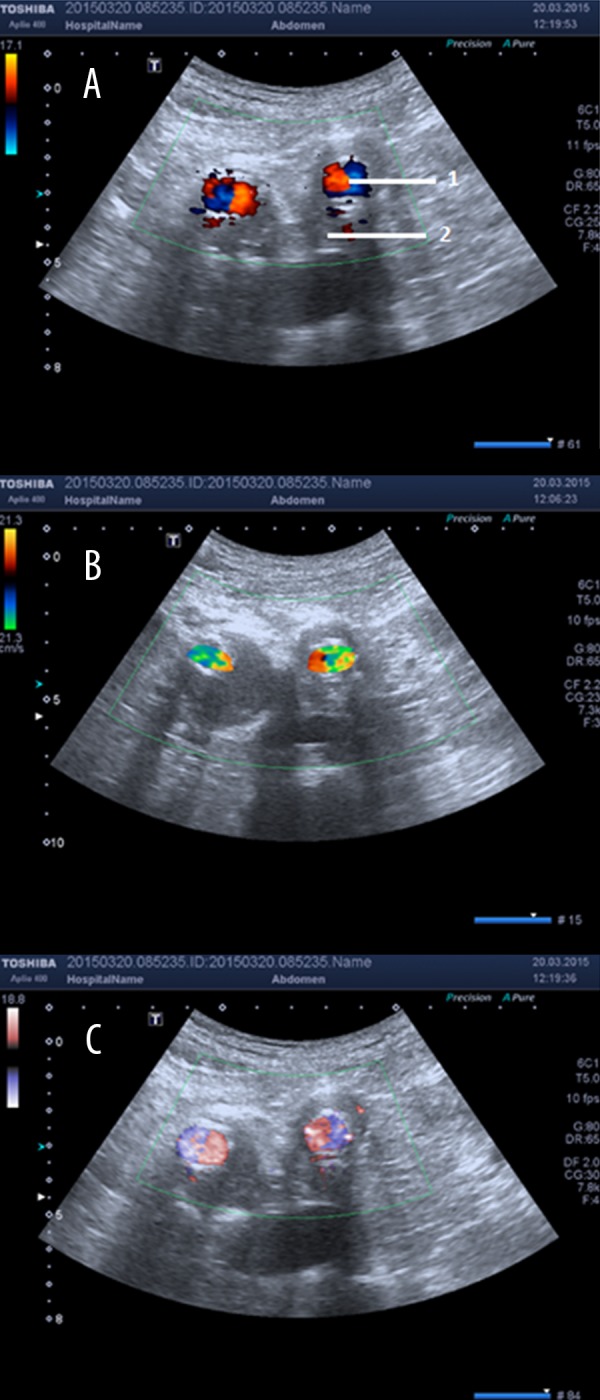
Cross-section through the 2 common iliac artery aneurysms. Retained patency of both legs of the stent-graft is shown by using the color Doppler mode. The blood flow in the aneurysm leg was not visualized, in addition to the lumen of the stent-graft; 1 – stent-graft lumen; 2 – aneurysm sack. Modality: (A) color Doppler, (B) power Doppler, (C) advanced dynamic flow (ADF).
In the mSMI imaging, the presence of flow in the iliac artery aneurysm was observed. The flow zone was seen in trans-verse and longitudinal sections (Figure 2A, 2B). cSMI imaging enabled the visualization of similar images (Figure 3) but it was less pronounced than in the case of mSMI imaging. By the end of the examination, CEUS imaging was obtained and the presence of an endoleak into the iliac artery aneurysm was revealed (Figure 4). Images obtained using cSMI, mSMI, and CEUS showed the presence of an endoleak in the same location and extent. On the CTA scanning taken 4 days after intervention, the endoleak was visible (Figure 5). Type II endoleak was suspected.
Figure 2.
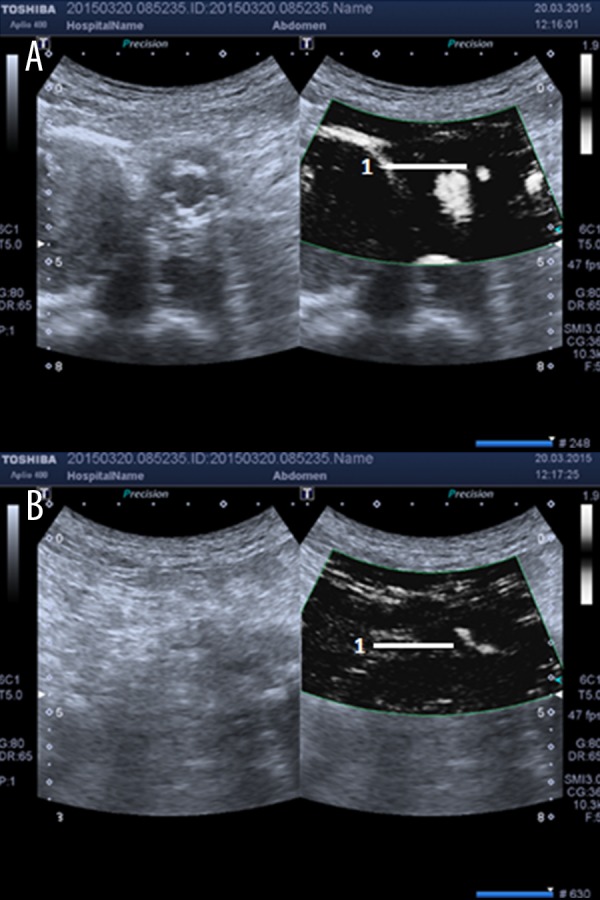
(A) mSMI: the cross-section through the two common iliac artery aneurysms. 1 The zone flow in the aneurysm sack of the left common iliac artery. (B) mSMI: a longitudinal section through the sack of the left common iliac artery aneurysm. 1. The zone flow in the aneurysm sack of the left common iliac artery.
Figure 3.

cSMI: The cross-section through the 2 common iliac artery aneurysms, showing retained patency of both legs of the stent-graft. 1. The zone flow in the aneurysm sack of the left common iliac artery.
Figure 4.
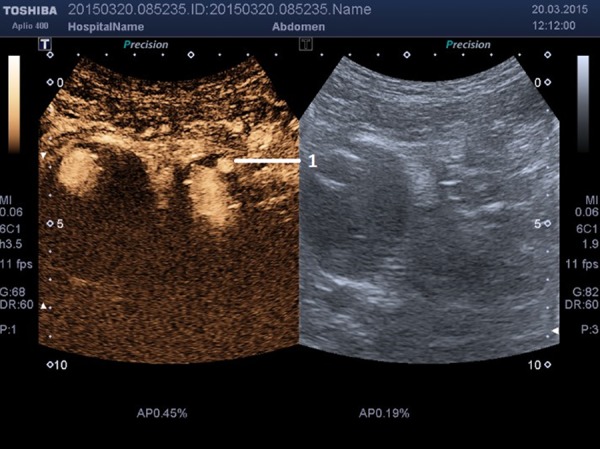
CEUS: The cross-section through the iliac artery aneurysms showing retained patency of both legs of the stent-graft. 1. The zone flow in the aneurysm sack of the left common iliac artery.
Figure 5.
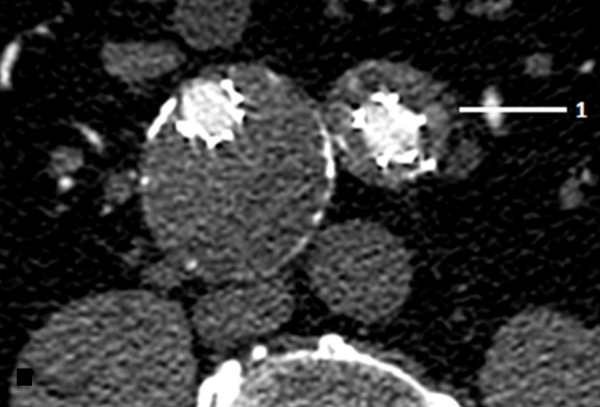
CT angiography: The cross-section through the 2 common iliac artery aneurysms. 1. The zone flow in the aneurysm sack of the left common iliac artery.
Discussion
Endoleaks after endovascular aortic repair (EVAR) are a frequent cause of secondary interventions or treatment failure and can be classified into 5 categories, according to the blood flow into the aneurysm sack [3]. CT angiography is usually the first radiological approach for follow-up in patients after EVAR. Although there is a high dose of ionizing irradiation during CT angiography, the nephrotoxic X-ray contrast media is not harmful to patient health [4,5]. The role for differential diagnosis of various endoleaks is still limited. According to most authors, CEUS is generally more sensitive in detection of endoleaks after EVAR than is Doppler ultrasonography [5]. The use of CEUS gives the first opportunity to solve the crucial problem, but use of this method is limited. Actually, the advent of CEUS imaging using sulphur hexafluoride microbubbles, improved the sensitivity and resolution of the blood flow, which can be imaged but requires an intravenous administration of contrast agents [6]. Furthermore, CEUS is hardly available and its use requires an additional cost [1,2]. With the improvement of ultrasound Doppler technology, the SMI mode enables clinicians to visualize the vascular patterns of lesions in detail without additional use of contrast agent [6]. The use of SMI modality requires a longer imaging time, whereas CEUS takes only a few minutes. However, both CEUS and SMI require the use of expensive and advanced ultrasonography equipment and long operator experience.
According to the actual reports, SMI has demonstrated significant clinical value in the evaluation of the shape and density of tumor vessels. By combining CEUS and SMI, additional information can be gained. Potential clinical applications of SMI are: hepatocellular, bladder, gastric carcinoma; cervical lymph nodes (malignant lymphoma); skin lesions- malignant melanoma; inflammation (rheumatoid arthritis, ulcerative colitis, Crohn’s disease); thyroid-reactive lymph nodes, and liver hemangioma [2,6,7].
Although the type II endoleak presented in this case report was not clinically significant, we demonstrated that the SMI method has sensitivity comparable to that of CEUS. The SMI should be considered as a quick and non-invasive method to follow up the patient after EVAR, as we have shown in this case. Further studies are needed to evaluate the real differences between SMI and CEUS and they can complement each other.
Conclusions
Our early experiences with SMI show that it has excellent sensitivity, comparable to CEUS, which is unable to achieve with the routine Doppler technology. This new technique has great value for early diagnosis of endoleaks and treatment planning in patients after EVAR. The use of SMI mode can increase sensitivity and improve diagnostic accuracy.
Footnotes
Statement
No disclosures or conflicts of interest.
Conflict of interest
None declared.
References:
- 1.O’Hara S. Toshiba Medical System. Superb Micro-Vascular Imaging (SMI) Available from: URL: http://medical.toshiba.com/products/ul/general/aplio-500/clinical-applications (23 march 2015, date last accessed)
- 2.Hata J. Toshiba Medical System. Seeing the Unseen New Techniques in Vascular Imaging Superb Micro-Vascular Imaging. Available from: URL: http://www.toshibamedicalsystems.com (23 march 2015, date last accessed)
- 3.Heye S. Diagnosis and treatment of endoleaks after endovascular repair of thoracic and abdominal aortic aneurysms. JBR-BTR. 2013;4:189–95. doi: 10.5334/jbr-btr.271. [DOI] [PubMed] [Google Scholar]
- 4.Abbas A, Hansrani V, Sedgwick N, et al. 3D contrast enhanced ultrasound for detecting endoleak following endovascular aneurysm repair (EVAR) Eur J Vasc Endovasc Surg. 2014;5:487–92. doi: 10.1016/j.ejvs.2014.02.002. [DOI] [PubMed] [Google Scholar]
- 5.Gürtler VM, Sommer WH, Meimarakis G, et al. A comparison between contrast-enhanced ultrasound imaging and multislice computed tomography in detecting and classifying endoleaks in the follow-up after endovascular aneurysm repair. J Vasc Surg. 2013;2:340–45. doi: 10.1016/j.jvs.2013.01.039. [DOI] [PubMed] [Google Scholar]
- 6.Machado P, Forsberg F. Toshiba Medical System. Medical Review Initial experience with a novel microvascular flow imaging technique. Available from: URL: http://www.toshibamedicalsystems.com (23 march 2015, date last accessed)
- 7.Wu L, Yen HH, Soon MS. Spoke-wheel sign of focal nodular hyperplasia revealed by superb micro-vascular ultrasound imaging. QJM. 2015;8:669–70. doi: 10.1093/qjmed/hcv016. [DOI] [PubMed] [Google Scholar]