

Abstract
Background
A giant cutaneous horn (GCH) is a morphologic description of conical lesion with a dense, hyperkeratotic protrusion of more than 1 cm in height that resembles an animal horn but without its bony core. These can occur in association with benign, premalignant or malignant cutaneous diseases which can be determined by excision and histopathologic review of the base.
A PubMed search (performed June 2015) revealed 54 cases of giant cutaneous horns in world literature. The most common site affected was the scalp followed by lip and leg. The commonest histological diagnosis found was squamous cell carcinoma followed by verruca vulgaris and trichilemmal horns.
Main observation
We present an 85-year-old Filipino female with a one year history of a rapidly growing skin lesion on her upper chest. This was excised fully and histological review of the base demonstrated a keratoacanthoma.
Conclusions
This is the first known occurrence of a giant cutaneous horn on the chest. While giant cutaneous horns are more commonly associated with malignant lesions, differential diagnosis includes benign lesions such as keratoacanthomas. This differential can be considered in a rapidly growing lesion. Excision and histopathologic review of the base of a cutaneous horn are essential to guide potential further therapy.
Keywords: chest, cutaneous horn, keratoacanthoma, keratosis, skin cancer
Introduction
A cutaneous horn is a clinical description of conical lesion that resembles a horn of an animal but without its bony core. These are made of cohesive keratinized material. Cutaneous horns can occur in association with benign or malignant cutaneous diseases, which can be confirmed by excision and histopathological review of the base. Giant cutaneous horns (GCH) greater than 1 cm in height are said to be rare as they are often removed early.[1] A recent PubMed search (June 2015) revealed 54 cases in world literature. This paper reports the 55th case of GCH and an example of a non-malignant association. This is the first reported case from the Philippines and the first case of GCH on the anterior chest wall.
Case Report
An 85-year-old Filipino female presented to the dermatology clinic with a one year history of a rapidly growing skin lesion on her upper chest. She sought medical attention because she was no longer able to conceal the lesion as it was protruding forward against her clothing. She complained that it was cosmetically disfiguring and caused her a lot of embarrassment. In addition, it was becoming more pruritic adding to her discomfort. There was no history of ulceration or bleeding. She had no past medical history of note; but in her younger years, she worked as a farmer and was constantly exposed to the sun.
Physical examination revealed a hyperkeratotic conical mass arising from the sternal area with the base measuring 6.5 cm in widest diameter vertically and 4.0 cm horizontally, and projecting 4 cm long anteriorly, then tapering to less than 1 cm wide at the tip [Fig. 1]. There was no cervical or axillary lymphadenopathy. Systemic examination was normal. Routine blood investigations were within normal limits.
Figure 1.

Giant cutaneous horn on the upper chest.
A clinical diagnosis of giant cutaneous horn (GCH) was made and she was referred to a general surgeon who performed total excision with primary closure under general anaesthesia. The lesion was sent for histopathological examination.
Histological review of the excised mass [Fig. 2] showed a broad cup-shaped invagination of the epidermis with an eosinophilic and parakeratotic plug. The adjacent epithelium surrounding the keratogenous plug showed acanthosis and was predominantly composed of cells with eosinophilic "glassy" cytoplasm. The dermis beneath the epidermal tumour showed a variably dense inflammatory infiltrate composed of lymphocytes mostly, but also admixed with eosinophils, few plasma cells and occasionally neutrophils. Solar elastosis was also noted suggesting a history of sun exposure. These findings were in keeping with a completely excised keratoacanthoma.
Figure 2.
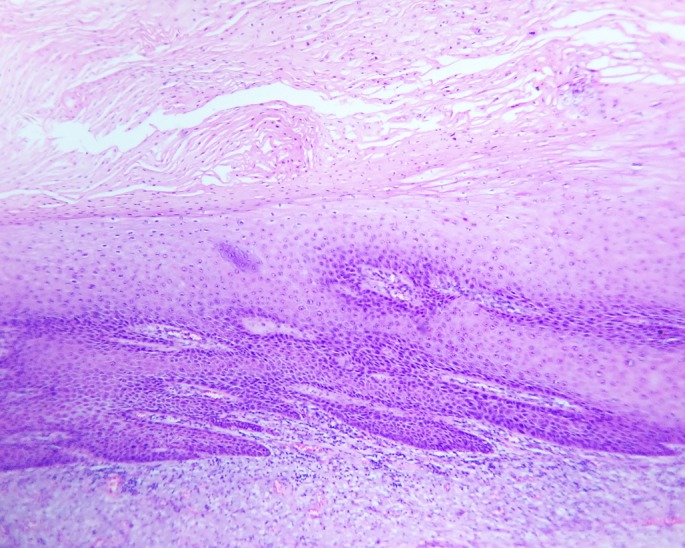
Histopathology showing hyperkeratosis and parakeratosis (H and E stain, ×100).
At one year follow up, there was no recurrence of the lesion.
Discussion
A cutaneous horn is a conical lesion with a dense, hyperkeratotic protrusion that often resembles an animal horn but without its bony core. The first documentation of cutaneous horn was in the 1588 London exhibition of an elderly Welsh woman.[1] In 1953, Farris from Italy reported the first case of a giant cutaneous horn with adequate histology.[2]
A PubMed search (June 2015) and a review of the individual manuscripts revealed 54 cases of GCH. These voluminous lesions have been reported to occur at any age from seven months to 92 years.
Majority of the GCH lesions involve sun exposed areas of the head especially the scalp,[3,4] lip[5,6] and cheek.[7,8] Less commonly they affect the limbs[9] and rarely, they affect the torso[10] such as in our case.
The duration of growth or persistence of GCH has been reported from six weeks to seventy-five years. The largest horn was reported by Michal M et al (2002)[4] had a length of 25 cm.
GCH are often asymptomatic although patients report psychological distress with these disfiguring lesions.[4]
The most common histopathological findings at the base of GCH include squamous cell carcinoma[7,8] and verruca vulgaris.[9] Less common causes include trichilemmal horn especially when lesions involve the scalp,[3,4] verrucous carcinoma[6] and keratoacanthoma such as in our case. It has also been associated overlying longstanding lupus vulgaris.[10] A GCH often occurs in isolation. When these present in multiples, the histopathologic diagnosis is often verruca vulgaris.[9] Further studies might explain why a number of histological pathologies can develop cutaneous horns.
Cutaneous horns are treated by surgical excision requiring careful histological examination to exclude a focus of malignancy.[6,8] If malignancy is present, margins should be reassessed for complete excision otherwise a re-excision may be required.
Conclusion
While giant cutaneous horns are often associated with malignancies such as squamous cell carcinomas, benign causes such as keratoacanthomas should also be considered, although confirmation of diagnosis with excision and histopathologic review is still essential.
References
- Copcu E, Sivrioglu N, Culhaci N. Cutaneous horns: are these lesions as innocent as they seem to be? World J Surg Oncol. 2004;2:18. doi: 10.1186/1477-7819-2-18. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Farris G. Histological considerations on a case of a voluminous cutaneous horn. Minerva Dermatol. 1953;28:159–165. [PubMed] [Google Scholar]
- Wang X, Wang L, Gao T, Lian S. Recurrent trichilemmal carcinoma with a large cutaneous horn formation. Ann Saudi Med. 2012;1:1–2. doi: 10.5144/0256-4947.2012.01.7.1530. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Michal M, Bisceglia M, Di Mattia A, Requena L, Fanburg-Smith JC, Mukensnabl P, Hes O, Cada F. Gigantic cutaneous horns of the scalp: lesions with a gross similarity to the horns of animals: a report of four cases. Am J Surg Pathol. 2002;26:789–794. doi: 10.1097/00000478-200206000-00014. [DOI] [PubMed] [Google Scholar]
- Leelavathy B, Kemparaj T, Sathish S, Khadri SI. Squamous cell carcinoma arising from a giant cutaneous horn: a rare presentation. Indian J Dermatol. 2015;60:107. doi: 10.4103/0019-5154.147893. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kumar S, Bijalwan P, Saini SK. Carcinoma buccal mucosa underlying a giant cutaneous horn: a case report and review of the literature. Case Rep Oncol Med. 2014;2014:518372. doi: 10.1155/2014/518372. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kneitz H, Motschenbacher S, Wobser M, Goebeler M. Photoletter to the editor: Giant cutaneous horn associated with squamous cell carcinoma. J Dermatol Case Rep. 2015;9:27–28. doi: 10.3315/jdcr.2015.1196. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wang YR, Guo MF, Liu BY, He YF, Li LF. A giant cutaneous horn on the cheek. J Plast Reconstr Aesthet Surg. 2013;66:871–872. doi: 10.1016/j.bjps.2012.11.042. [DOI] [PubMed] [Google Scholar]
- Wang C, Wang W, Lei YJ, Wang JY, Dong XP, Wang J, Sheng RH, Pan ZA, Zhu WY, You LP, Peng HX, Xu XY. Multiple huge cutaneous horns overlying verrucae vulgaris induced by human papillomavirus type 2: a case report. Br J Dermatol. 2007;156:760–762. doi: 10.1111/j.1365-2133.2006.07734.x. [DOI] [PubMed] [Google Scholar]
- Wani A, Gupta V, Jan N. A Giant Cutaneous Horn in A Case of Lupus Vulgaris. J Turk Acad Dermatol. 2010;4:04101c. [Google Scholar]