

Abstract
Purpose:
The aim of this study was to assess knowledge and attitude of dentists in Bosnia and Herzegovina (BH) regarding signs and symptoms of child abuse and neglect (CAN), reporting procedure and level of education.
Methods:
Data were collected through a self-administrated structured questionnaire adopted and modified from previous studies. It was administrated to 300 dentists out of which a total number of 210 subjects were in final sample for statistical analyses. Response rate was seventy percent. Descriptive statistics, Chi-square and Kruskal-Wallis H test were used to analyze statistical differences in responses. The level of significance was set at p<0.05.
Results:
Dentists in BH are very rarely provided (80%) with training related to recognition and reporting of CAN. Sixty six percent of dentists had never suspected CAN in their practice. Only nine percent of dentists would report suspicious of CAN. Prevailing reasons for not reporting suspected case of CAN was lack of knowledge of the reporting procedure (43%), and combination of indicated answers that never had a case and lack of knowledge about the procedure (31%).
Conclusion:
Results of this study suggest that dentists need an effective education to increase their knowledge and awareness of all aspects of CAN.
Keywords: child abuse and neglect, dentist knowledge, Bosnia and Herzegovina
1. INTRODUCTION
Child abuse and neglect (CAN) has been defined by the World Health Organization (WHO) as, ‘‘Every kind of physical, sexual, emotional abuse, neglect or negligent treatment, commercial or other exploitation resulting in actual or potential harm to the child’s health, survival, development or dignity in the context of a relationship of responsibility, trust or power‘‘(1).
Abuse can be physical, sexual, psychological and economic; neglect can be physical, psychological, medical and educational while medical neglect is defined as intentional failure to provide necessary medical treatment and health protection (2).
American Academy of Pediatric Dentistry (AAPD) defined dental neglect, as willful failure of a parent or guardian to seek and follow through with whatever treatment is necessary to ensure a level of oral health essential for adequate chewing function and freedom from pain and infection (3).
International studies emphasize the role of dental practitioners in detecting CAN (4, 5, 6, 7). It has been reported that orofacial trauma is present in approximately 50 to 75 percent of all reported cases of physical child abuse (8, 9). Therefore, dental health care providers are most likely to be the first to recognize the evidence of physical abuse. Different nationwide studies reported very low percentage of dentists’ participation in reporting suspected cases of CAN (10, 11, 12, 13, 14).
WHO estimated that almost 53,000 children died worldwide in 2002 from homicide (1).
In the United States each year almost 2,000 infants and young children die from being abused or neglected by caretakers (4). The problem is more extent in low economic countries associated with low incomes, poverty, high rate of unemployment, increased level of stress and unstable political situation (9, 12). Bosnia and Herzegovina has all of the listed risk factors.
The purpose of this study was to assess knowledge and attitude of BH dentists regarding signs and symptoms of CAN, reporting procedure and level of education.
2. MATERIALS AND METHODS
Cross-sectional survey was carried out from March to June 2013. Data were collected through a self-administrated structured questionnaire offered to 300 dentists working in 7 different towns in BH. Final sample consisted of 210 dentists who agreed to participate in the study and returned questionnaire correctly filled. Response rate was 70 percent. The drop-out rate observed in present study was higher than anticipated during the design phase of the study but having in mind that the total number of dentists registered in public sector in BH was 997, the final sample of 210 participants can be considered as a representative for this survey (15, 16).
The questionnaire consisted of twenty-seven questions adopted and modified from previous studies (4,6,14). All questions about knowledge and attitudes were formulated as a statement using multiple- choice or true-false format.
Data were coded and entered into an SPSS package (Statistical Package for the Social Sciences, v. 13) and analyzed by using descriptive analysis for responses to each question. Question by question were tabulated and analyzed using frequencies and percentages from responses to each questions to compile prevalence data. Non-parametric statistical tests (The chi-square test and Kruskal Wallis H test) were used to analyze differences among respondents in respect of age, gender, professional experience, specialty, and workplace. The level of significance was set at p<0.05.
3. RESULTS
All subjects (n=210) indicated to treat paediatric patients on daily basis. Most of the subjects were female (70 %) the most frequent age was 30-49 years (67%) with working experience of less than 10 years in dental practice (48 %). Most of the respondents (62 %) indicated they were general practitioners (GP). The remaining of 38% was divided between pediatric dentists (18 %) and other specialties (20 %): orthodontics, oral surgeons and periodontologysts. Seventy percent of dentists were working in public practice and 30 % privately. Results about the level of educational training and self education regarding CAN and related items revealed very low level of education and any kind of training whereas 92.4 percent of subjects had no education or training, and 84.3 % hasn’t been provided so far with any kind of information about CAN. Knowledge of social issues related to CAN was evaluated in six questions were respondents indicated answers as: “yes”, “no” or “don’t know”. Distribution of answers of social indicators is given in Table 1. The answer “don’t know” was very frequent, indicating a lack of knowledge related to social indicators of CAN. Results regarding knowledge of the physical indications of CAN are given in Table 2.
Table 1.
Knowledge of social indicators of child abuse and neglect (CAN) among dentists in Bosnia and Herzegovina. *Correct answers are indicated with asterix.
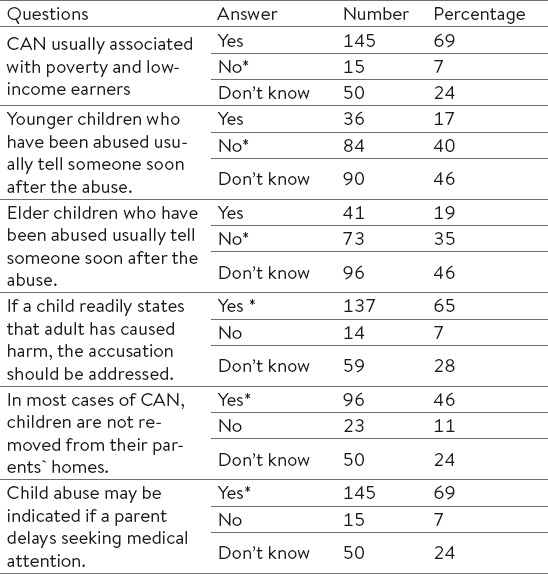
Table 2.
Knowledge of signs of physical abuse among dentists in Bosnia and Herzegovina. *Correct answers are indicated with asterix.

Respondents usually indicated correct answer, but “don’t know” as selected answer was prevalent in this section too.
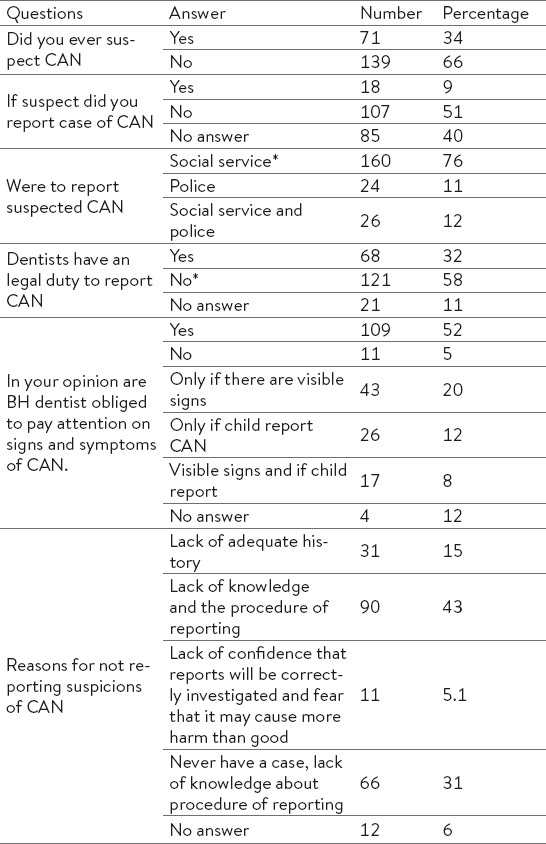
Majority of BH dentists have never suspected CAN (66 %), and only 9 percent of them if suspected, would reported. Results of knowledge and attitudes regarding legal and ethical responsibilities among BH dentists are given in Table 3. The most common reason for not reporting suspicions of CAN was lack of knowledge about the reporting procedure.
Table 3.
Knowledge and attitudes regarding legal and ethical responsibilities among dentists in Bosnia and Herzegovina.*Correct answers are indicated with asterix.
Statistical analyzes revealed significant differences in terms of social indicators, signs of physical abuse and knowledge of legal and reporting procedure. The chi-square test was used to analyze differences among respondents in respect of sex, specialty, and workplace. Kruskal Wallis H test was used to analyze differences in between age and years of working experience. More female dentists indicated that elder children would tell someone about the abuse (p=0.025). Dentists from public practice more frequently indicated that CAN was not related to poverty and low incomes (p=0.029), More GP than private practitioners considered that CAN was indicated if parent delayed seeking help and the difference between answers in this section was statistically significant (p=0.026). Statistically significant differences in respect of physical abuse were found between GPs and specialists where GPs more frequently indicated bite marks (p=0.004) and bruises on a neck (p=0.009) as possible signs of physical abuse.
Majority of dentists working in public practice suspected CAN, and the difference between public and private practitioners was statistically significant. (p=0.002).
4. DISCUSSION
Large epidemiological study conducted to assess prevalence of CAN in Balkan countries among children aged 11, 13 and 16 in a representative sample of 42, 272 children and 26, 287 parents brought data for BH among other countries in region (13,14). Despite, high figures of prevalence of physical violence (50.99 percent), sexual victimization (13.61 percent) and feelings of neglect (48.04 percent) among examinees from BH medical and dental profession were not included in state programme or strategy dealing with education on recognizing and prevention of CAN and related issues. (13,14)
The present study is the first one conducted among dentists in Bosnia and Herzegovina regarding dental aspects of CAN. The findings of the present survey indicated that there was a lack of knowledge in many related to the subject of CAN. Having in mind that education is very important in this issue, and that this issue is very important for community, the lack of education and training courses is a serious problem for all authorities involved. Dental schools in many countries included the subject of CAN in their curricula, but results from many studies revealed that dentists or dental students still have not had enough knowledge about topic of CAN (17, 18). Findings of numerous studies emphasize the need for additional education and introduction of novels models of training related to recognition of CAN through long-life learning courses (4, 6, 10, 19, 20). According to results in our study, significant proportion of respondents are aware of their responsibility to pay attention to CAN, but lack of the knowledge of the reporting procedure was the most common reason for not reporting. Social and psychological barriers could be additional reason for under-reporting CAN. These findings are similar to those in other studies (4, 5, 6, 17, 18, 20).
Seventy percent of BH dentists associated poor oral health with physical neglect. Poor oral health could be considered as a dental neglect indicator. It is considered that untreated caries, periodontal disease, and other conditions can cause pain, infection and loss of function (2, 12, 20). The most frequent indicator of dental neglect is rampant early childhood caries (2, 21). Epidemiological findings of oral health status of children in BH, where decay, missing, filled index (DMFT) was more than 6, suggest that possible dental neglect could be considered (22, 23).
Baseline results about knowledge and attitudes of dentists in BH regarding CAN and related issues revealed urgent need for providing serious education for all dentists in BH. Dentists need extensive and effective education to increase their knowledge and their awareness of all aspects of CAN as well as to enhance the importance of their role in detecting and reporting suspected cases. In order to achieve this, dental schools, continuing education providers and all legal authorities could develop programs for training dentists in diagnosing, documenting and reporting suspected CAN cases.
Footnotes
CONFLICT OF INTEREST: NONE DECLARED.
REFERENCES
- 1.A World Health Organization and International Society for Prevention of Child Abuse and Neglect. Preventing child maltreatment: a guide to taking action and generating evidence. 2006. [Accessed: August, 08, 2014]. At: http://whqlibdoc.ho.int/publications/2006/9241594365_eng.pdf .
- 2.Arslanagic Muratbegovic A. Recognizing Child Abuse and Neglect in The Dental Office. Criminal Justice Issues. 2011;5-6:47–58. [Google Scholar]
- 3.American Academy of Pediatrics Committee on Early Childhood, Adoption, and Dependent Care. Oral and dental aspects of child abuse and neglect. Pediatrics. 1986;78(3):537–539. [PubMed] [Google Scholar]
- 4.Ramos-Gomez F, Rothman D, Blain S. Knowledge and attitudes among California dental care providers regarding child abuse and neglect. J Am Dent Assoc. 1989;129(3):340–348. doi: 10.14219/jada.archive.1998.0208. [DOI] [PubMed] [Google Scholar]
- 5.John V, Messer LB, Arora R, Fung S, Hatzis E, Nguyen T, San A, Thomas K. Child abuse and dentistry: a study of knowledge and attitudes among dentists in Victoria, Australia. Aust Dent J. 1999;44(4):259–267. doi: 10.1111/j.1834-7819.1999.tb00230.x. [DOI] [PubMed] [Google Scholar]
- 6.Azevedo MS, Goettems ML, Brito A, Possebon AP, Domingues J, Demarco FF, Torriani DD. Child maltreatment: a survey of dentists in southern Brazil. Braz Oral Res. 2012;26(1):5–11. doi: 10.1590/s1806-83242012000100002. [DOI] [PubMed] [Google Scholar]
- 7.Al-Dabaan R, Newton JT, Asinakopoulou K. Knowledge, attitudes and experience of dentists living in Saudi Arabia toward child abuse and neglect. The Saudi Dental Journal. 2014;26:79–87. doi: 10.1016/j.sdentj.2014.03.008. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Al-Jundi SH, Zawaideh FI, Al-Rawi MH. Jordanian dental students’ knowledge and attitudes in regard to child physical abuse. J Dent Educ. 2010;74(10):1159–1165. [PubMed] [Google Scholar]
- 9.Jordan A, Welbury RR, Tiljak MK, Cukovic-Bagic I. Croatian dental students’ educational experiences and knowledge in regard to child abuse and neglect. J Dent Educ. 2012;76(11):1512–1519. [PubMed] [Google Scholar]
- 10.Bsoul SA, Flint DJ, Dove SB, Senn DR, Alder ME. Reporting of child abuse: a follow-up survey of Texas dentists. Pediatr Dent. 2003;25(6):541–545. [PubMed] [Google Scholar]
- 11.Bankole OO, Denloye OO, Adeyemi AT. Child abuse and dentistry: a study of knowledge and attitudes among Nigerian dentists. Afr J Med Sci. 2008;37(2):125–134. [PubMed] [Google Scholar]
- 12.Al-Habsi SA, Roberts GJ, Attari N, Parekh S. A survey of attitudes, knowledge and practice of dentists in London towards child protection. Are children receiving dental treatment at the Eastman Dental Hospital likely to be on the child protection register? Br Dent J. 2009;28;206(4):E7. doi: 10.1038/sj.bdj.2009.113. discussion 212-213. [DOI] [PubMed] [Google Scholar]
- 13.Periodic Report Summary 2–BECAN (Balkan epidemiological study on child abuse and neglect) [Accessed: October,21 2014]. At: http://cordis.europa.eu/result/rcn/58804_en.html .
- 14.Đuderija S. Prevencija nasilja nad djecom–perspektiva multidisciplinarnog institucionalnog tretiranja u Bosni i Hercegovini (prevention of child abuse- perspective of multidisciplinary institutionalized treatment approach in Bosnia and Herzegovina) Master thesis, University of Sarajevo. 2011 [Google Scholar]
- 15.Health statistics annual Federation of Bosnia and Herzegovina. 596 stomatologa. 2012. [Accessed: March, 04 2013]. At: http://www.zzjzfbih.ba/wp-content/uploads/2009/02/Zdravstveno-statisticki-godisnjak-FBiH-20121.pdf .
- 16.Analysis of population health. [Accessed: March, 04 2013]. At: http://www.phi.rs.ba/documents/publikacija_zdr_stanje_2012.pdf .
- 17.Thomas EJ, Straffon BA, Inglehart RM. Child Abuse and Neglect; Dental and Dental Hygiene Students’ Educational Experiences and Knowledge. J Dent Educ. 2006;70(5):558–565. [PubMed] [Google Scholar]
- 18.Owais AI, Qudeimat MA, Qodceih S. Dentists’ involvement in identification and reporting of child physical abuse. Jordan as a case study. Int J Paediatr Dent. 2009;19(4):291–296. doi: 10.1111/j.1365-263X.2009.00971.x. [DOI] [PubMed] [Google Scholar]
- 19.Mouden LD. Child abuse and dentistry: what you should know. J Mich Dent Assoc. 1994;76(5):22–27. [PubMed] [Google Scholar]
- 20.Cukovic-Bagic I. The role of the dentist in Recognition of Child Abuse. Acta Stomatol Croat. 2010;44(4):285–292. [Google Scholar]
- 21.Valencia-Rojas N, Lawrence HP, Goodman D. Prevalence of early childhood caries in a population of children with history of maltreatment. Journal of Public Health Dentistry. 2009;68(2):94–101. doi: 10.1111/j.1752-7325.2007.00077.x. [DOI] [PubMed] [Google Scholar]
- 22.Arslanagic Muratbegovic A, Markovic N, Zukanovic A, Selimovic-Dragas M, Kobaslija S, Juric H. Oral Health Related to Demographic Features in Bosnian Children Aged Six. Coll Antropol. 2010;34(3):1027–1033. [PubMed] [Google Scholar]
- 23.Markovic N, ArslanagićMuratbegovic A, Kobaslija S, Bajric E, Selimovic-Dragas M, Huseinbegovic A. Caries prevalence of children and adolescents in Bosnia and Herzegovina. Acta Medica Academica. 2013;42(2):108–116. doi: 10.5644/ama2006-124.79. [DOI] [PubMed] [Google Scholar]