

To the Editor: Ma2 antibody-mediated encephalitis is a rare type of paraneoplastic neurological syndrome (PNS) present with various clinical symptoms. Lung or testicular germ-cell malignancies are the most commonly associated tumors.[1] Here, we reported a patient with a Ma2 antibody-mediated encephalitis related to ileal lymphoma.
A 62-year-old male with a history of hypertension and diabetes mellitus presented with 6 months of mental and behavior change. He had memory loss and visual hallucinations since September 2013. The patient gained 12.5 kg of bodyweight increase due to increased appetite and was diagnosed as bulimia nervosa at a local hospital. He also stated dizziness, unstable walking and diplopia with ptosis of bilateral eyelids. He felt sleepy and drowsy during daytime but sleepless at night. He also experienced urinary incontinence occasionally. On admission, the patient was alert. The mini-mental state examination was 18/30, indicating moderate impairment of memory. The patient had vertical gaze paresis, unable to look upward and downward with horizontal nystagmus. His muscle power and muscle tone were normal with diminished tendon reflexes. He had unstable gait and could not walk in a straight line.
Brain magnetic resonance imaging showed abnormality in medial temporal lobe and diencephale [Figure 1]. A lumbar puncture yielded clear cerebrospinal fluid (CSF) with normal open pressure. CSF exhibited a white blood cell count of 38 × 106/L, a protein level of 0.73 g/L, normal level of glucose and chloride and no detectable oligoclonal bands. The cytological analysis yielded no malignant cells. Paraneoplastic antibody testing (EUROIMMUN AG, Germany) revealed that anti-Ma2 antibodies were positive in both CSF and serum. The patient developed hypothermal episodes with bradycadia and decreased the level of consciousness which was remitted after intravenous immunoglobulin (IVIg) treatment. Positron-emission tomography revealed hypermetabolism in the right hippocampus and left parahippocampal gyrus while hypermetabolism in ileal lesions indicated malignant lesion. After the resection of his terminal ileum and the right superior colon, pathological examination confirmed the diagnosis of submucosal follicular lymphoma. The patient received chemotherapy for lymphoma but deceased 1-month later due to septic shock with leucopenia.
Figure 1.
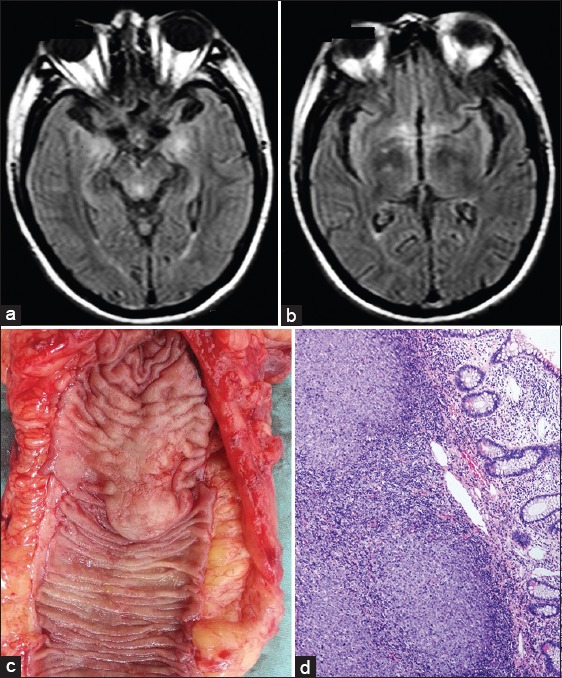
Neuroimaging and pathological findings of the patient. Brain magnetic resonance imaging fluid-attenuated inversion recovery sequences showed abnormity in medial temporal lobe (a) and diencephale (b). Resected tissue of terminal ileum demonstrated a focal mass (c). Pathological findings of submucosal follicular lymphoma (d), H E staining, ×200.
Anti-Ma2 encephalitis differs from typical paraneoplastic limbic encephalitis for most patients developed combination of the limbic system, diencephalon or brainstem encephalitis. Hypothalamus and pituitary gland could even be involved.[2] It was reported in young patients with testicular cancer or tumors of lung and breast.[3] We described the clinical and pathological findings in a patient with Ma2 antibody-mediated brain stem/limbic encephalitis associated with submucosal follicular lymphoma of the ileum. It broadens the spectrum of tumor associated with this rare PNS. The clinical manifestation and neuroimaging of this patient suggested a combined limbic, diencephalic and brainstem lesions. In fact, only 26% of the patients had classical limbic encephalitis in the literature. Excessive daytime sleepiness, as presented, in this case, affected 32% of the patients, sometimes with narcolepsy cataplexy.[1] After receiving oncological treatment and immunotherapy, including steroids, IVIg and plasma exchange, some patients have neurological improvement. But nearly half of the patients deteriorated after treatment.
Anti-Ma2-associated encephalitis has a unique clinical presentation and should not be overlooked considering its remarkable involvement of the limbic system, diencephalon and brainstem. This disorder should be suspected in patients with subacute involvement of one or more of these three brain regions and CSF abnormalities suggesting an inflammatory process.
Footnotes
Edited by: Li-Min Chen
Source of Support: Nil.
Conflict of Interest: None declared.
REFERENCES
- 1.Dalmau J, Graus F, Villarejo A, Posner JB, Blumenthal D, Thiessen B, et al. Clinical analysis of anti-Ma2-associated encephalitis. Brain. 2004;127:1831–44. doi: 10.1093/brain/awh203. [DOI] [PubMed] [Google Scholar]
- 2.Bergner CG, Lang C, Spreer A, Bähr M, Mohr A, Simons M. Teaching NeuroImages: Ma2 encephalitis presenting as acute panhypopituitarism in a young man. Neurology. 2013;81:e146–7. doi: 10.1212/01.wnl.0000435307.33389.f7. [DOI] [PubMed] [Google Scholar]
- 3.Hoffmann LA, Jarius S, Pellkofer HL, Schueller M, Krumbholz M, Koenig F, et al. Anti-Ma and anti-Ta associated paraneoplastic neurological syndromes: 22 newly diagnosed patients and review of previous cases. J Neurol Neurosurg Psychiatry. 2008;79:767–73. doi: 10.1136/jnnp.2007.118588. [DOI] [PubMed] [Google Scholar]