

To the Editor: Coronary arterial involvement is rare in Takayasu's arteritis. We describe successful coronary artery stenting in a 17-year-old teenager with Takayasu's arteritis and acute inferior myocardial infarction due to occlusion of the right coronary artery.
The patient, a male student, 17-year-old, was admitted to our emergency room with persistent retrosternal pain accompanied by sweat 2 h. The patient had no history of hypertension or diabetes, and he neither drank alcohol nor smoked. There was no family history of coronary heart disease. On his physical examination, blood pressure of left arm was 140/70 mmHg and 100/70 mmHg for the right. Vascular murmur can be heard in the neck, supraclavicular and groin area. His initial electrocardiogram revealed II, III, avF ST-segment elevation 0.6–0.7 mV, laboratory test revealed a markedly elevated troponin I (>100 ng/ml), so we considered Takayasu's arteritis could not be excluded. We performed emergency percutaneous coronary interventional therapy. Coronary angiography revealed that the middle of the right coronary artery was totally occlusive [Figure 1a]. The proximal stenosis of left anterior descending branch was 50% and formed collateral circulation to the distal right coronary artery [Figure 1b]. Therefore, drug-eluting stent was implanted in the occlusion of right coronary artery [Figure 1c]. On the 2nd day of admission, his C-reactive protein level (20 mg/dl) and erythrocyte sedimentation rate (48.7 mm/h) were high. After 4th day of stenting, large vessel computed tomography (CT) was performed. CT angiography of the aorta showed that bilateral proximal subclavian arteries, internal carotid artery and renal artery had severe stenosis, celiac trunk had moderate stenosis. The superior mesenteric artery had severe stenosis.
Figure 1.
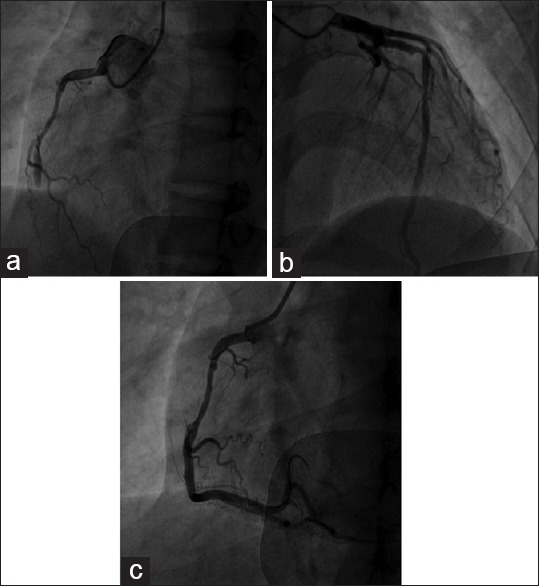
(a) Coronary angiography of right coronary artery; (b) Coronary angiography of left coronary artery; (c) Coronary stenting in right coronary artery.
Takayasu's arteritis is a rare chronic nonspecific inflammatory disease, its cause was unknown and predominantly affected the aorta and its main branches, including coronary arteries and pulmonary arteries. Coronary arterial involvement is rare in Takayasu's arteritis.[1,2] Coronary angiographic and pathologic studies together have revealed coronary artery lesions in 9–11% of cases.[3] We performed emergency coronary angiography successfully and implanted a drug-eluting stent in the occlusion of right coronary artery. It is important to select the appropriate operation time for the treatment of Takayasu arteritis with early detection and treatment, hormone drugs should be taken under the supervision of doctor.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Footnotes
Edited by: De Wang and Ya-Lin Bao
REFERENCES
- 1.Soeiro Ade M, Almeida MC, Torres TA, Franken M, Lima FG, Ganem F, et al. Clinical characteristics and long-term outcome of patients with acute coronary syndromes and Takayasu arteritis. Rev Port Cardiol. 2013;32:297–302. doi: 10.1016/j.repc.2012.06.020. [DOI] [PubMed] [Google Scholar]
- 2.Cipriano PR, Silverman JF, Perlroth MG, Griepp RB, Wexler L. Coronary arterial narrowing in Takayasu's aortitis. Am J Cardiol. 1977;39:744–50. doi: 10.1016/s0002-9149(77)80139-2. [DOI] [PubMed] [Google Scholar]
- 3.Sun T, Zhang H, Ma W, Yang L, Jiang X, Wu H, et al. Coronary artery involvement in takayasu arteritis in 45 Chinese patients. J Rheumatol. 2013;40:493–7. doi: 10.3899/jrheum.120813. [DOI] [PubMed] [Google Scholar]