

Dear Sirs,
Moyamoya disease is characterized by a progressive narrowing or occlusion of the terminal portion of the internal carotid arteries and the proximal part of the anterior and middle cerebral arteries, with a concomitant development of abnormal collateral vessels [1]. Common clinical presentations in childhood are ischemic stroke or transient ischemic attack, headache and convulsion [1].
Involuntary movements in patients with moyamoya disease are uncommon, occur in only 3 to 6% of patients [2], and mostly in children. These involuntary movements include chorea, hemidystonia, hemichoreoathetosis, and paroxysmal dyskinesia [2], and are attributed to ischemic changes in the basal ganglia-thalamocortical circuits.
Here, we report on a 17-year-old female patient who had an involuntary choreiform movement in her right hand that was associated with moyamoya disease. This symptom, along with hyperventilation, developed immediately after eating hot noodles. The symptom was usually aggravated under stressful conditions such as student assessments and regressed when at rest. The patient had no familial history of chorea or other movement disorders, and she denied the use of any drugs. There was no family history of neurological diseases.
On examination, the patient presented with choreic movements involving the right arm. The involuntary movement was a jerky and irregular athetoid movement (Supplementary Video in the online-only Data Supplement). In addition, there was mild slowness with a decremental response observed in the both arms. Neither rigidity nor a rest tremor was observed. The choreoathetoid movement was not present during sleep. The patient’s mental status was normal, and the cranial, motor and sensory nerve examinations showed no other abnormality.
The routine laboratory tests, including a complete blood count, fasting glucose and glycosylated hemoglobin A1c, liver enzymes, blood urea nitrogen, creatinine, electrolytes, the erythrocyte sedimentation rate, thyroid functions, serum ceruloplasmin, urine and serum copper, vitamin B1, vitamin B6, and niacin were within the normal limits. The antinuclear antibody and antiphospholipid antibody tests were negative. Genetic tests for Huntington’s disease and spinocerebellar ataxia type 17 were normal. Magnetic resonance imaging (MRI) of the brain showed a low signal intensity on the right parieto-occipital area and multiple flow-voids in both basal ganglia on T2-, T1-, and fluid attenuation inversion recovery-weighted images (Figure 1A, B, and C). Contrast-enhanced MRI showed diffuse leptomeningeal enhancement along the cortical sulci and a strong enhancement of perforating arteries in the basal ganglia and deep white matter (“ivy sign”) (Figure 1D and E). Magnetic resonance cerebral angiography demonstrated severe stenosis of both internal carotid arteries at the supraclinoid portion with numerous collateral vessels (Figure 1F). A 99mTc-hexamethylpropylene amieoxime brain single photon emission computed tomography showed decreased perfusions in the right temporo-occipital cortex, bilateral fronto-temporal areas, and in both basal ganglia (Figure 1G). Digital subtraction cerebral angiography confirmed the moyamoya disease Suzuki grade IV (Figure 1H, I, and J).
Figure 1.
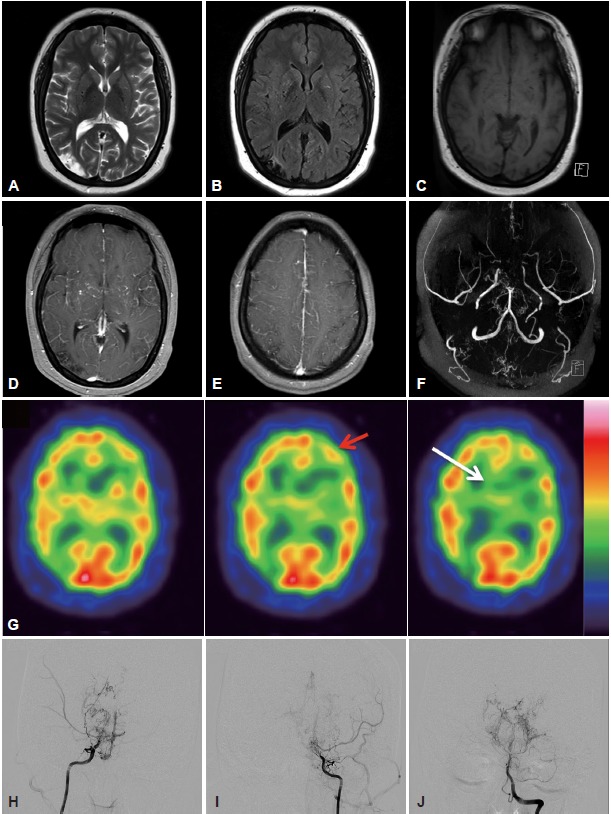
A, B, and C: Magnetic resonance imaging (MRI) of the brain showed a low signal intensity on the right parieto-occipital area and multiple flow-voids in both basal ganglia on T2-, T1-, and fluid attenuation inversion recovery-weighted images. D and E: Contrast-enhanced MRI showed diffuse leptomeningeal enhancement along the cortical sulci and strong enhancement of perforating arteries in the basal ganglia and deep white matter (“ivy sign”). F: Magnetic resonance cerebral angiography revealed a severe stenosis of both internal carotid arteries at the supraclinoid portion with numerous collateral vessels. G: A 99mTc-hexamethylpropylene amieoxime brain single photon emission computed tomography showed decreased perfusions in the right temporo-occipital cortex and bilateral frontal areas (red arrow) and in both basal ganglia (white arrow). H, I, and J: Digital subtraction cerebral angiography confirmed the moyamoya disease (Suzuki grade IV).
The clinical presentations of pediatric moyamoya disease are associated with cerebral ischemia, which causes migraine-like headaches, epileptic seizures, and cerebral infarction [1]. The symptoms are characteristically induced by hyperventilation or breath holding, such as that during crying or playing an instrument [3]. These neurological events appear to have a vasoactive mechanism that is responsive to an acid-base imbalance, but not simply thrombogenic mechanisms [4]. In addition, some patients may experience an ischemic attack after eating hot and spicy noodles.
Chorea complicated by moyamoya disease as the first manifestation is extremely rare. In addition, the occurrence of chorea during a specific daily activity such as eating hot noodles is of particular interest. This case suggests that chorea relates directly to hyperventilation and the associated hypocarbia, which could result in profound vasoconstriction and vasospasm [4-6].
In the present patient, an ischemic lesion was found only in the right parieto-occipital area, which was on the ipsilateral side of the hemichorea. The occurrence of a right hemichorea in the present patient is difficult to explain. Some studies have reported ipsilateral ischemic lesions in moyamoya disease and chorea [6]. However, these studies did not provide any association between hemichorea and an ipsilateral ischemic lesion. We also cannot suggest any association between hemichorea and an ipsilateral parenchymal lesion. The patient’s symptom has not disappeared, but has been fluctuating. The chorea is usually aggravated in stressful conditions and is regressed when at rest. We speculate that the hypoperfusion of the left basal ganglia and frontal cortex is associated with a transient aggravation of the right hemichorea. An interruption of the basal ganglia-thalamocortical circuits could have caused the involuntary movements presented in the present patient.
Although hyperventilation-related hypoperfusionischemia is the main pathology for chorea in patients with moyamoya disease, to the best of our knowledge, the occurrence of chorea immediately after eating hot foods is rare. This case represents another example of chorea in moyamoya disease that is associated with vasospasm and ischemia.
Footnotes
Conflicts of Interest
The authors have no financial conflicts of interest.
Supplementary Materials
The online-only Data Supplement is available with this article at http://dx.doi.org/10.14802/jmd.15048.
The patient had choreic movements involving the right arm. There was mild slowness with a decremental response observed in the both arms. Neither rigidity nor a rest tremor was observed.(http://dx.doi.org/10.14802/jmd.15048.v001).
REFERENCES
- 1.Pandey P, Bell-Stephens T, Steinberg GK. Patients with moyamoya disease presenting with movement disorder. J Neurosurg Pediatr. 2010;6:559–566. doi: 10.3171/2010.9.PEDS10192. [DOI] [PubMed] [Google Scholar]
- 2.Baik JS, Lee MS. Movement disorders associated with moyamoya disease: a report of 4 new cases and a review of literatures. Mov Disord. 2010;25:1482–1486. doi: 10.1002/mds.23130. [DOI] [PubMed] [Google Scholar]
- 3.Fukui M, Kono S, Sueishi K, Ikezaki K. Moyamoya disease. Neuropathology. 2000;20 Suppl:S61–S64. doi: 10.1046/j.1440-1789.2000.00300.x. [DOI] [PubMed] [Google Scholar]
- 4.Mikulis DJ, Krolczyk G, Desal H, Logan W, Deveber G, Dirks P, et al. Preoperative and postoperative mapping of cerebrovascular reactivity in moyamoya disease by using blood oxygen level-dependent magnetic resonance imaging. J Neurosurg. 2005;103:347–355. doi: 10.3171/jns.2005.103.2.0347. [DOI] [PubMed] [Google Scholar]
- 5.Han SH, Kim YG, Cha SH, Chung SY. Moyamoya disease presenting with singing induced chorea. J Neurol Neurosurg Psychiatry. 2000;69:833–834. doi: 10.1136/jnnp.69.6.833. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Spengos K, Tsivgoulis G, Toulas P, Vemmos K, Vassilopoulos D, Spengos M. Hyperventilation-enhanced chorea as a transient ischaemic phenomenon in a patient with moyamoya disease. Eur Neurol. 2004;51:172–175. doi: 10.1159/000077665. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
The patient had choreic movements involving the right arm. There was mild slowness with a decremental response observed in the both arms. Neither rigidity nor a rest tremor was observed.(http://dx.doi.org/10.14802/jmd.15048.v001).