

Abstract
A 71-year-old woman with a right adrenal mass detected by computed tomography was referred to our institution. Before 33 months, she had undergone a radical heminephrectomy for an 11-cm renal cell carcinoma (RCC) in the left moiety of a horseshoe kidney. The adrenal tumor was diagnosed as the metastasis of RCC. The tumor was subsequently removed in a laparoscopic adrenalectomy by a retroperitoneal approach. Pathologic examination revealed the mass to be the adrenal metastasis of RCC. To our knowledge, this is the initial report of a laparoscopic adrenalectomy for the adrenal metastasis of renal cell carcinoma arising from a horseshoe kidney.
Keywords: Adrenal metastasis, Renal cell carcinoma, Horseshe kidney, Laparoscopic adrenalectomy
Introduction
A horseshoe kidney is one of the most common disorders of the genitourinary system and originates during the fourth to sixth week of fetal life. Its incidence is estimated to be approximately 0.25% of the total population and more men are afflicted than women.1 No genetic determinant is known, although, it has been reported in identical twins and in siblings within the same family. Many types of malignant tumors arising from horseshoe kidneys have been reported, the most frequently observed of which are renal cell carcinomas (RCCs).2 In the literature, although the therapy or the operation for RCC in horseshoe kidneys has been mentioned,2 there is little information concerning metastasis from RCC. We encountered a patient with an adrenal metastasis of renal cell carcinoma in a horseshoe kidney and treated it with laparoscopic adrenalectomy. Herein, we report this rare case along with a discussion of the literature.
Case presentation
A 69-year-old woman was referred to our institution for a left renal mass, which was found incidentally by a computed tomography (CT) scan for low-grade fever at another hospital. The CT images revealed a solid tumor measuring approximately 11 cm in diameter at the left renal lesion, which was well defined and heterogeneously enhanced in a horseshoe kidney (Fig. 1A). The tumor was limited to the kidney, without any metastasis or lymphadenopathy. The patient was successfully treated with open heminephrectomy after isthmus division through a midline abdominal incision. The pathologic study of the specimen confirmed a 10-cm organ-confined clear cell carcinoma (pT2), grade 2, with negative margins. There were no complications during the perioperative periods.
Figure 1.

(A) Computed tomography demonstrates an 11-cm solid enhancing tumor in the left moiety of a horseshoe kidney (left). (B) Computed tomography images of right adrenal tumor (a black arrow) which showed dynamic contrast enhancement pattern (right).
However, 33 months later, the follow-up CT scan showed a 3-cm mass in the right adrenal gland with no calcification, which was well enhanced (Fig. 1B). A magnetic resonance imaging scan was performed to accurately locate the mass and determine its resectability. The patient's laboratory tests, including endocrinologic function, and metabolic evaluations were all within normal limits. The patent was diagnosed with a tumor that was an adrenal metastasis from the primary renal cell carcinoma and which could be removed. A laparoscopic retroperitoneal adrenalectomy was used to treat this patient.
After the induction of general anesthesia, the patient was placed in the jack-knife position with the ipsilateral side elevated. A 2-cm incision was made on the right posterior axillary line, and subsequently, a balloon trocar was inserted to dilate the retroperitoneal space. After creating the working space in the retroperitoneal cavity, a 12-mm open trocar port was placed. An 11-mm trocar was inserted under the direct vision on the middle axillary line, and 2 identical working ports were placed on the anterior side. The lateroconal fascia was widely dissected to expand the retroperitoneal space. A significantly tortuous aorta was observed close to the lumber quadrate muscle. The ablation of fatty tissue was performed to determine the positional relationship in the cavity. The inferior vena cava and the right side of the horseshoe kidney were not identified at that point. Although the dissection of fatty tissue along the aorta progressed, the adrenal tumor was found near the aorta (Fig. 2). The adrenal gland with the tumor was fully exposed by the dissection of the surrounding tissue with adequate hemostasis. Finally, the adrenal central vein was verified and triple-clipped and cut. The specimen was placed in the endoscopic pouch and retrieved through the trocar port. The operative time was 173 minutes with minimal blood loss. There were no complications during the perioperative period. The patient was discharged on the eighth postoperative day.
Figure 2.
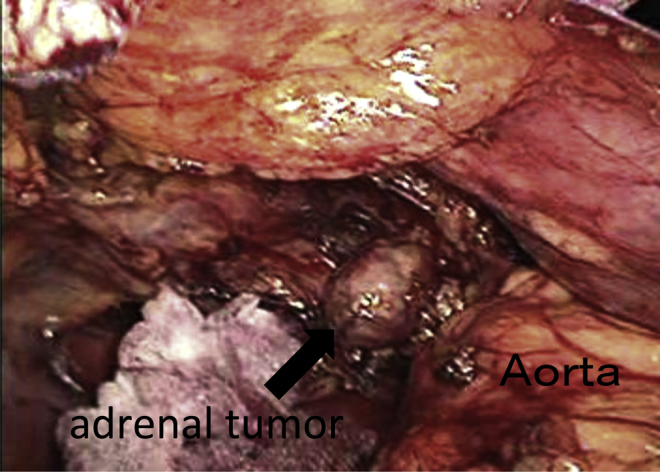
Retroperitoneal cavity while a laparoscopic adrenalectomy was performed. The adrenal tumor was found nearby the significantly tortuous aorta.
The pathologic examination of the specimen demonstrated that the tumor was formed from many atypical clear cells that were composed of swelling nuclei in the clear cytoplasm. The adrenal mass was diagnosed as metastatic renal cell carcinoma with features similar to the primary renal tumor (Fig. 3).
Figure 3.
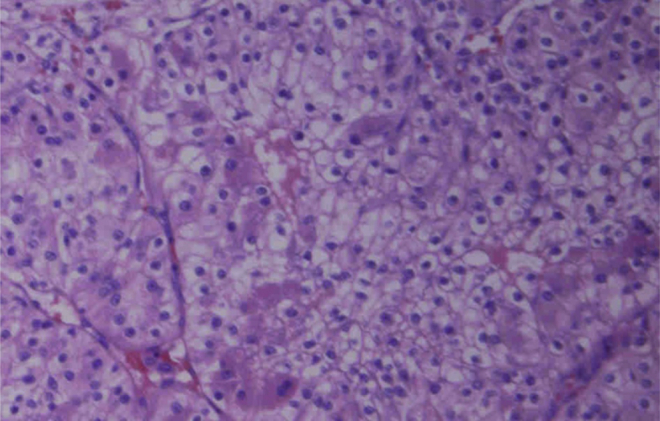
Microscopic specimen of the right adrenal gland. Pathologic examination revealed that the tumor was formed of many atypical clear cells that were composed of swelling nuclei in the clear cytoplasm (hematoxylin and eosin; ×40).
The patient has been in good condition but has experienced recurrence on the lung and the other adrenal gland. She rejected all the treatment for the metastatic disease, but is now still alive with no therapy.
Discussion
RCC is the most common tumor associated with horseshoe kidneys, but in these patients, it occurs no more often than in the general population.2 In patients with horseshoe kidneys, prognosis is unaffected by the anomaly and is dependent on tumor pathology and the stage at diagnosis, as is the case for patients with normal kidneys.1, 2 RCC can metastasize to almost any organ, including the lungs, liver, kidneys, bones, and brain. Adrenal metastases from RCC are not uncommon, with autopsy studies showing an incidence of 6% to 23%.3, 4 However, in nephrectomized patients, the incidence of solitary adrenal metastasis to the ipsilateral gland and the contralateral gland is 3% to 0.7%, respectively.5 Surgical removal is the only known effective treatment in patients with solitary adrenal metastasis, with 29% to 35% of patients subsequently surviving 5 years or more.5 Laparoscopic adrenalectomy for malignancy is still controversial; however, it can be performed with acceptable outcomes in carefully selected patients with small, organ-confined, solitary metastasis. Therefore, aggressive treatment, such as excision of such lesions, is thought to be effective. The anatomic position of the adrenal gland in the horseshoe kidney is definitely different from the normal pattern. Therefore, it is thought to be difficult to perform an adrenalectomy for the metastasis. Additionally, it has been supposed that in the manner, the working space does not extend into the peritoneal space to adhesion during the previous surgery. The most difficult point of this operation is that the landmarks in the retroperitoneal space, such as the kidney, vena cava, and gonadal vein could not be accurately located. However, once the adrenal gland was detected, the subsequent procedures to the resection were not complicated. Thus, this operation was relatively safe and effective.
Conclusion
We have experienced adrenal metastasis of renal cell carcinoma in a horseshoe kidney. To our knowledge, this is the first report of a laparoscopic adrenalectomy for such a case.
Consent
Written informed consent for the publication of this case report and the accompanying images was obtained from the patient. A copy of the written consent is available for review by the Editor-in-Chief of this journal on request.
Conflict of interest
None of the authors has any conflict of interest to disclosure.
Funding source
No external funding was secured for this study.
Footnotes
Available online 17 May 2014
This is an open access article under the CC BY-NC-ND license (http://creativecommons.org/licenses/by-nc-nd/3.0/).
References
- 1.Bauer S.B. Anomalies of the upper urinary tract. In: Wein A.J., Kavousi L.R., Novik A.C., Partin A.W., Peters C.A., editors. Campbell-Walsh Urology. ed. 9. Saunders; Philadelphia: 2007. pp. 3269–3334. [Google Scholar]
- 2.Rubio B.J., Regalado P.R., Sanchez M.F. Incidence of tumoural pathology in horseshoe kidneys. Eur Urol. 1998;33:175–179. doi: 10.1159/000019551. [DOI] [PubMed] [Google Scholar]
- 3.Lau W.K., Zincke H., Blute M.L. Contralateral adrenal metastasis of renal cell carcinoma: treatment, outcome, and a review. BJU Int. 2003;91:775–779. doi: 10.1046/j.1464-410x.2003.04237.x. [DOI] [PubMed] [Google Scholar]
- 4.Kessler O.J., Mukamel E., Servadio C. Metachronous renal cell carcinoma metastasis to the contralateral adrenal gland. J Urol. 1998;51:539–543. doi: 10.1016/s0090-4295(97)00698-5. [DOI] [PubMed] [Google Scholar]
- 5.Plawner J. Results of surgical treatment of kidney cancer with solitary metastasis to contralateral adrenal. Urology. 1991;37:233–236. doi: 10.1016/0090-4295(91)80291-e. [DOI] [PubMed] [Google Scholar]