

Abstract
We present the case of a 50-year-old woman, who is a bilateral Syme's amputee and subsequently underwent patellofemoral arthroplasty (PFA) for osteoarthritis primarily involving the patellofemoral (PF) joint. History and physical examination were suggestive of severe PF arthritis without patellar instability of the right knee. The diagnosis was confirmed by roentgenogram and a PFA was performed. A slightly modified rehabilitation program was implemented and the patient was followed until 6 years after surgery. In comparison to the preoperative scores, the Oxford, the Western Ontario and McMaster Universities (WOMAC), the Knee Society, and the Hospital for Special Surgery Knee Scores improved significantly (p < 0.05) at the time of final follow-up. PF problems specific to below-knee amputees, factors to be considered before performing PFA, and the drawbacks of other treatment modalities in these patients have been discussed.
Keywords: Below-knee amputee, Patellofemoral osteoarthritis, Patellofemoral arthroplasty, Patellar tendon bearing prosthesis, Patella alta
1. Introduction
The prevalence of arthritis in the patellofemoral (PF) joint is high, especially in women.1 In fact, 24% of women who have symptoms from arthritis in the knee have an isolated involvement of the PF compartment.2 However, disagreement prevails regarding the prevalence of PF osteoarthritis (OA) in the lower limb amputees.3, 4
Patellofemoral arthroplasty (PFA) is a rescue procedure for isolated PF osteoarthritis5 and it can be effective in 80–85% of cases.6 Interestingly, for the first time in the literature we present a case of bilateral Syme's amputee who underwent PFA for severe PF OA of the right knee.
2. Case report
Our case is a 50-year-old woman who underwent bilateral Syme's amputation 50 years ago when she was a 17-day-old infant for burns caused by accidental fall of a hot lamp during phototherapy. Her final prosthesis was a combined patellar tendon bearing (PTB) and end-bearing below-knee prosthesis consisting of a push fit laminate socket with pelite liner, exoskeletal shank, and a solid ankle cushion heel (SACH) foot. Until 44, she enjoyed uninterrupted standing and walking for an hour, shopping, and line dancing.
However, during the last 6 years, she had increasing anterior knee pain (right more than left) that worsened with ambulation. Pain was extreme especially when she was using the stairs and trying to stand from sitting position. The pain also kept her awake at night frequently. There was no history suggestive of patella subluxation or dislocation. Her body mass index (BMI) was 32.
Examination of the right knee showed severe tenderness and crepitus of the PF joint. There was no medial or lateral tibiofemoral (TF) joint line tenderness. The knee range of motion (ROM) was 0–130° and the knee was stable and normally aligned. The Oxford score, the Western Ontario and McMaster Universities (WOMAC) score, the hospital for special surgery knee score (HSS), and the knee society score (KSS) were recorded before surgery (Table 1)
Table 1.
Comparison of preoperative and 6 years follow up clinical scores.
| Clinical score | Normal range of score | Before surgery | At final follow up | p value |
|---|---|---|---|---|
| Oxford knee score | 0 (worst)–48 (best) | 14 | 29 | 0.0038 |
| WOMAC score | 0 (best)–100 (worst) | 82 | 51 | 0.0001 |
| HSS score | 0 (worst)–100 (best) | 51 | 83 | 0.0001 |
| KSS (knee score) | 0 (worst)–100 (best) | 50 | 65 | 0.0449 |
| KSS (function score) | 0 (worst)–100 (best) | 10 | 60 | 0.0001 |
Roentgenogram of the right knee showed well-preserved (Kellgren–Lawrence grade 1) medial and lateral TF joint spaces in the anteroposterior view and a normally placed patella with osteophytes involving the PF joint in the lateral view (Fig. 1). Skyline view revealed mild lateral subluxation of the patella with severe osteoarthritis (Kellgren–Lawrence grade 4) of the lateral half of the PF joint (Fig. 1). Clinical and roentgenogram evaluation of the left knee suggested early osteoarthritis of the PF joint (Kellgren–Lawrence grade 2).
Fig. 1.

Anteroposterior, lateral, and skyline views of the right knee roentgenogram showing severe PF osteoarthritis.
Conservative treatments, such as physiotherapy and analgesic medications, met with only limited success and the patient was forced to decrease her level of activities and resorted to short distance ambulation (less that one block). Considering the age and the limited involvement of the right knee disease, with the patient's consent, a PFA was performed without any complication.
The operation was performed under a spinal anesthesia with a proximal-thigh tourniquet applied. A midline skin incision followed by a medial parapatellar approach was used. An oval dome patella (Depuy Orthopaedics Inc., Warsaw, IN, USA) and Depuy GCK P.F.J Trochlear implant were used with Depuy Smartset GHV gentamicin bone cement.
When the patient was in the recovery room, she was taught static quadriceps exercises. On postoperative day (POD) 1, she began physical therapy according to our institution's PFA rehabilitation protocol, which included quadriceps and gluteal isometric strengthening, active-assisted straight leg raises, and short-arc leg extension exercises. Vastus medialis oblique (VMO) exercise, which is very crucial for PFA patients, was started from day 1. On POD 2, the patient began weight bearing as tolerated with the aid of a Special walker manufactured by ARJO, Gloucester, UK (Fig. 2). Instead of the below-knee prosthesis, foam pads were used for weight bearing on both the legs (Fig. 2). The residual limb was constantly monitored for any signs of skin breakdown or infection, and skin monitoring was made a priority in patient education.
Fig. 2.

Patient weight bearing with special ARJO walker.
On day 3, she was able to perform level transfers with help. The following day, she was able to ambulate approximately 10 feet with ARJO walker and was able to do active straight leg raises. Continuous passive motion machine was used to achieve knee flexion, which gradually improved to 90° by day 6. At the time of discharge (POD 7), she was able to ambulate independently up to 20 feet with the aid of Zimmer walker frame. Skin staples were removed at 2 weeks and the wound healed uneventfully.
At the time of the final follow-up (6 years after surgery), she was able to walk 5–10 blocks unaided. Her knee ROM was 0–130° (Fig. 3) and she was able to negotiate stairs without much difficulty by holding the rails. Roentgenogram showed satisfactory implant and patellar position, with no signs suggestive of implant loosening (Fig. 4). Lastly, compared to the preoperative scores, there was a significant improvement (p < 0.05) in all the clinical scores (Table 1) recorded at the time of final follow-up.
Fig. 3.
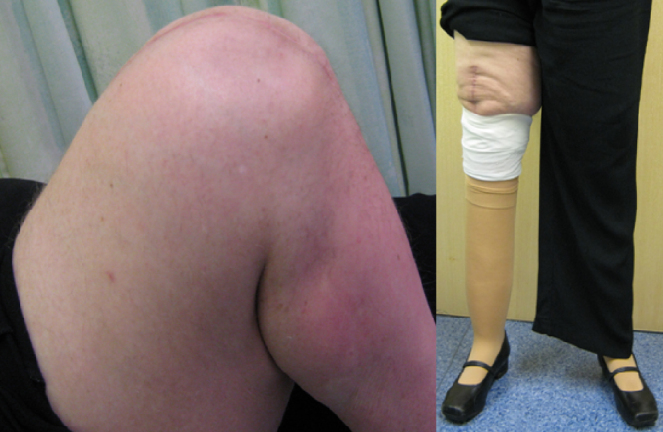
Knee ROM (up to 130°) and unaided walking at 6 years follow-up.
Fig. 4.

Roentgenogram showing anteroposterior, lateral, and skyline views of the right knee at 6 years follow-up.
3. Discussion
While there are few earlier case reports of total knee arthroplasty (TKA) performed in below-knee amputees,7, 8, 9 for the first time we report a case of bilateral Syme's amputee who underwent right knee PFA.
Controversy exists regarding the prevalence of PF OA in them.3, 4 Hungerford and Cockin4 found a marked increase in PF OA in the nonamputated leg. However, Burke et al.3 showed that only 1 in 42 had a radiological grade 2 or 3 PF OA in the nonamputated leg.
PFA is done as a bridging surgery to avoid TKA in midlife so that the patient can enjoy kinematics and ROM that more closely resembles a normal joint. Also subsequent revision to a primary TKA or addition of a unicompartmental TF arthroplasty is technically easier and more functional than a revision TKA.5
Patellectomy has been used for generations for debilitating PF OA. Patellectomy has experimentally been shown to reduce extension power by 25–60%. TF joint reaction forces have been shown to increase as much as 250%, suggesting a tendency for TF arthrosis after patellectomy. Variable pain relief, residual quadriceps weakness, and secondary instability, with failures as high as 45%, make this procedure undesirable in many practices. Not to mention the relatively poor outcomes after TKA in patients who had previously undergone patellectomy.10
Further, it is always said by the limb fitters that a stump would not last if exposed to full end-weight bearing, and so, a PTB socket is very useful in sharing the load.11 However, patellectomy has the drawback of losing a crucial weight-bearing area of the stump in below-knee amputees, who would otherwise be benefited by prosthesis with either PTB or PTB-suprapatellar-supracondylar (PTB-SCSP) socket.
The modern below-knee socket is shaped to take the body weight on nonsensitive areas, and relieve weight from sensitive areas. The PTB socket has an indentation at the site of the insensitive tough skin in the infrapatella area and the insensitive patella tendon.12 Weight is borne on the lower patellar ligament, the flare of the medial tibial condyle, and posteriorly under the flare of both tibial condyles.11
The PTB-SCSP socket has high medial and lateral sidewalls that extend above and over the femoral condyles. Also the socket extends along the anterior aspect so that the patella is enclosed within the socket. The PTB-SCSP socket applies force proximal to the patella during stance, in this way providing sensory feedback to limit genu recurvatum.13
Other treatment options for PF OA, such as tibial tubercle unloading osteotomies, have high complication rates and unpredictable results; the autogenous chondrocyte implantation or osteochondral transplants have inconsistent results in the PF joint because of the high shear stresses in this compartment.14, 15
Even though BMI of our patient remained a concern, many of the patients in Leadbetter's series have been overweight with a BMI >30 and the PFA literature does not single out the obese patient as a poor candidate for PFA. Specifically, no outcome studies have attributed an increase rate of PFA wear or prosthetic loosening to obesity. Conversely, such patients typically do not make good candidates for unloading osteotomy or cartilage restoration.16 Further, because of frequent comorbidities, these patients often experience more operative complications after TKA.17
Patella alta has been reported in patients with below-knee amputation using PTB prosthesis.18 In our case, the Insall-Salvati index was 1.18 and 1.39 in the right and left knee, respectively. An index over 1.2 indicates a patella alta, whereas an index below 0.8 indicates patella baja or infera.19 Our patient had a combined PTB and end-bearing prosthesis on both sides, which could probably explain the presence of normally placed patella in the operated side and a high riding patella in the other side, reflecting the possibility that the left patellar tendon would have transmitted relatively more load to the prosthesis compared to the right because of disparity in socket contouring. Another possibility is that because of the arthritic symptoms in the right knee, the patient would have strained the left knee more in recent years.
To be noted is that patella alta can adversely affect the outcome of PFA either by causing a patellar clunk while engaging in the trochlear implant during initial flexion from full extension or by increasing the lateral patellar instability. Patella alta should be considered as a contraindication to PFA unless this can be addressed intraoperatively by distalization of the tibial tuberosity or by choosing a trochlear implant, which extends proximal enough and thereby allowing the patella to engage in the trochlear implant during full extension of the knee with activated quadriceps (traction applied to duplicate this in surgery).5 Postoperative lateral view radiograph of the knee attests for ideal trochlear implant size and position and one can notice that the patella is engaged in the trochlear implant with the limb in full extension (Fig. 4).
The mild patellar subluxation and tilt seen in the preoperative skyline view (Fig. 1) is possibly because of the focal cartilage loss rather than static resultant force. Again, the mild patellar tilt seen in the postoperative skyline view (Fig. 4) could be because of the fact that the implanted patella plus trochlear component thickness is often re-established to normal, but this thickness is greater than the soft tissues that have seen in years because of PF bone and cartilage attrition.5 As the intraoperative tracking was satisfactory, a titrated lateral release was not performed. Also, the postoperative skyline radiograph (Fig. 4) shows the lateral coverage of the trochlear implant, which by design accommodates the patella. Postoperatively, there was no episode of subluxation or dislocation of patella observed by the patient. This further demonstrates the importance of early and full VMO activation for PFA patients.5
The surgeon should try to preserve the infrapatellar branch of the saphenous nerve and aim for healthy surgical scar as an anesthetic skin or a bad scar over the weight-bearing area may as well preclude the use of PTB prosthesis.11
The ARJO walker was used to assist standing from sitting position, level transfer, and ambulation in the early rehabilitation phase. This walker is much more stable and allows for controlled weight bearing in the stumps by means of elbow load distribution, which makes it an attractive option for such patients (Fig. 2). Postoperatively our patient was mobilized without the temporary prosthesis. Foam pads were used for weight bearing and ambulation (Fig. 2). Our patient was used to the foam pads even before the surgery, which made mobilization relatively easy. Rather than using a temporary prosthesis for immediate weight bearing postoperatively, a satisfactory outcome still is obtained by undergoing delayed limb fitting once the edema has settled and the wound healed.
4. Conclusion
PF problems specific to below-knee amputees and the factors to be considered while performing PFA in these patients have been discussed. Secondly, drawbacks of other treatment modalities for predominant PF arthritis, especially in below-knee amputees, have been highlighted. Thirdly, a slightly modified, safe, and successful rehabilitation program followed for our patient has been detailed. Lastly, this report shows that a successful outcome can be achieved by PFA, which is an ideal option and should be considered for isolated PF OA in below-knee amputees.
Conflicts of interest
The authors have none to declare.
References
- 1.Davies A.P., Vince A.S., Shepstone L., Donell S.T., Glasgow M.M. The radiologic prevalence of patellofemoral osteoarthritis. Clin Orthop. 2002;402:206–212. doi: 10.1097/00003086-200209000-00020. [DOI] [PubMed] [Google Scholar]
- 2.McAlindon T.E., Snow S., Cooper C., Dieppe P.A. Radiographic patterns of osteoarthritis of the knee joint in the community: the importance of the patellofemoral joint. Ann Rheum Dis. 1992;51:844–849. doi: 10.1136/ard.51.7.844. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Burke M.J., Roman V., Wright V. Bone and joint changes in lower limb amputees. Ann Rheum Dis. 1978;37:252–254. doi: 10.1136/ard.37.3.252. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Hungerford D., Cockin J. Abstract, British Orthopaedic Association Autumn Meeting. 1974. The fate of the retained lower limb joints in World War II amputees. [Google Scholar]
- 5.Farr J., II, Barrett D. Optimizing patellofemoral arthroplasty. Knee. 2008;15:339–347. doi: 10.1016/j.knee.2008.05.008. [DOI] [PubMed] [Google Scholar]
- 6.Lotke P.A., Lonner J.H., Nelson C.L. Patellofemoral arthroplasty: the third compartment. J Arthroplasty. 2005;20(4 suppl 2):4–6. doi: 10.1016/j.arth.2005.03.011. [DOI] [PubMed] [Google Scholar]
- 7.Crawford J.R., Coleman N. Total knee arthroplasty in a below-knee amputee. J Arthroplasty. 2003;18:662–665. doi: 10.1016/s0883-5403(03)00209-2. [DOI] [PubMed] [Google Scholar]
- 8.Pasquina P.F., Dahl E. Total knee replacement in an amputee patient: a case report. Arch Phys Med Rehabil. 2000;81:824–826. doi: 10.1016/s0003-9993(00)90118-7. [DOI] [PubMed] [Google Scholar]
- 9.Vanin N., Zeichen J., Brand J., Krettek C., Hankemeier S. Total knee replacement in a below-knee amputee: technical reference points and possible solutions. Unfallchirurg. 2008;111:633–636. doi: 10.1007/s00113-007-1366-8. [DOI] [PubMed] [Google Scholar]
- 10.Lonner J.H. Patellofemoral arthroplasty: current concepts. Univ Pa Orthop J. 2002;15:1–5. [Google Scholar]
- 11.Redhead R.G. Symposium: recent trends in limb fitting. Recent developments in prosthetics. Proc R Soc Med. 1966;59:3–5. doi: 10.1177/003591576605900102. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.James W.V. Principles of limb fitting and prostheses. Ann R Coll Surg Engl. 1991;73:158–162. [PMC free article] [PubMed] [Google Scholar]
- 13.Fergason J., Smith D.G. Socket considerations for the patient with a transtibial amputation. Clin Orthop. 1999;361:76–84. doi: 10.1097/00003086-199904000-00011. [DOI] [PubMed] [Google Scholar]
- 14.Brittberg M., Tallheden T., Sjogren-Jansson B., Lindahl A., Peterson L. Autogenous chondrocytes used for articular cartilage repair: an update. Clin Orthop. 2001;391(suppl):337–348. doi: 10.1097/00003086-200110001-00031. [DOI] [PubMed] [Google Scholar]
- 15.Hangody L., Rathonyi G.K., Duska Z., Vasarhelyi G., Fules P., Modis L. Autogenous osteochondral mosaicplasty, surgical technique. J Bone Joint Surg. 2004;86(suppl 1):65–72. [PubMed] [Google Scholar]
- 16.Leadbetter W.B. Patellofemoral arthroplasty in the treatment of patellofemoral arthritis: rationale and outcomes in younger patients. Orthop Clin North Am. 2008;39:363–380. doi: 10.1016/j.ocl.2008.04.001. [DOI] [PubMed] [Google Scholar]
- 17.Miric A., Lim M., Kahn B., Rozenthal T., Bombick D., Sculco T.P. Perioperative morbidity following total knee arthroplasty among obese patients. J Knee Surg. 2002;15:77–83. [PubMed] [Google Scholar]
- 18.Batra S., Kumar R., Lenka P. Bilateral recurrent dislocation of the patella associated with below knee amputation: a case report. BMC Musculoskelet Disord. 2005;17(6):9–11. doi: 10.1186/1471-2474-6-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Insall J., Salvati E. Patella position in the normal knee joint. Radiology. 1971;101:101–104. doi: 10.1148/101.1.101. [DOI] [PubMed] [Google Scholar]