

Abstract
Background:
HIV/AIDS is one of the diseases which not only makes threats to physical health, but also, due to the negative attitudes of people and the social stigma, affects the emotional and social health of patients. The aim of this study was to identify the psychological, social, and family problems of people living with HIV/AIDS (PLWHA) in Iran.
Methods:
In this qualitative study, we used purposive sampling to enroll PLWHA, their families, and physicians and consultants in two cities of Kermanshah and Tehran. Each group of PLWHA, their families, physicians, and consultants participated in two focus group discussions (FGDs), and a total of eight FGDs were conducted. Six interviews were held with all key people, individually.
Results:
Based on the views and opinions of various groups involved in the study, the main problems of PLWHA were: Ostracism, depression, anxiety, a tendency to get revenge and lack of fear to infect others, frustration, social isolation, relationship problems, and fear due to the social stigma. Their psychological problems included: Marriage problems, family conflict, lack of family support, economic hardships inhibiting marriage, and social rejection of patient's families. Their family problems were: Unemployment, the need for housing, basic needs, homelessness, and lack of social support associations.
Conclusions:
It seems that the identification and focusing on psychological, social, and family problems of affected people not only is an important factor for disease prevention and control, but also enables patients to have a better response to complications caused by HIV/AIDS.
Keywords: HIV/AIDS, Iran, psychological needs, qualitative study, social needs
INTRODUCTION
Nowadays, HIV/AIDS is one of the most serious problems in many parts of the world which has a high priority for health managers and decision-makers. Despite enormous efforts to prevent and control the HIV/AIDS epidemic, the number of cases and deaths from the disease continue to grow in such a way that AIDS has been known as the fourth main cause of death around the world.[1] According to the World Health Organization, approximately 35 million people worldwide are infected with HIV/AIDS and it seems that the disease will be recognized as the primary cause of death in the world by 2020.[2] In Iran, like many parts of the world, HIV prevalence is rising and the number of detected cases is only a part of the total cases. Recent estimates of the number of cases diagnosed with HIV in 2011 show that about 93,250 people in the country are suffering from HIV/AIDS and it is estimated that this number will raise to 126,300 patients by 2015.[3] Due to adverse social consequences arising from the dominant social believes and social stigma, HIV/AIDS is among the diseases which not only affects the physical aspects, but also the social and psychological conditions of patients.[4] In addition to the physiological effects of the disease, people living with HIV/AIDS (PLWHA) may encounter numerous problems such as discrimination, losing social status and role, changes in the patterns of relationships (intimacy), losing jobs and financial resources, and facing problems to provide required medicines.[5,6] Many of these problems are also common among other people who suffering from other chronic diseases, but the stress associated with social and family problems arising from the diseases such as social stigma and exclusion especially by support groups is very intensely and uniquely threatening people with HIV/AIDS.[6] Community and social network members may fear to be infected with HIV disease and they are frightened to take care of HIV/AIDS patients. This can cause the ground to withdraw more patients from the support needed and make them deprived from the benefits of social support.[7] Failure to notice and concentrate on patients’ problems may lead to lower levels of accountability and increase infected persons’ pessimism toward society, and thus cause the spread of the virus in broader levels.[8] In a study in Tehran, after the diagnosis of HIV/AIDS diseases among people, job loss increased from 5% to 52%.[9] In another study in 2008 which was conducted among 2000 adolescents and young adults aged 10–24 years, who were living in urban areas in seven cities, 35.6% of participants agreed to have HIV/AIDS-infected classmates or colleagues, 45% said that PLWHA were great shame to their families, and 45.1% believed that the infected people were guilty.[10] Accordingly, although some success has been obtained in treating the disease and increasing life expectancy among patients, there is a long road ahead to overcome problems and improve their quality of life. The first step is to reach a deep understanding of the challenges and psychological and social problems which are facing infected patients. This study aimed to identify psychological, social, and family problems of PLWHA and their families.
METHODS
This is a qualitative study which aimed to identify and determine the views of officials and key people, physicians and consultants, and PLWHA and their families about psychological, social, and family problems of PLWHA. It was conducted in two cities of Kermanshah and Tehran in 2012.
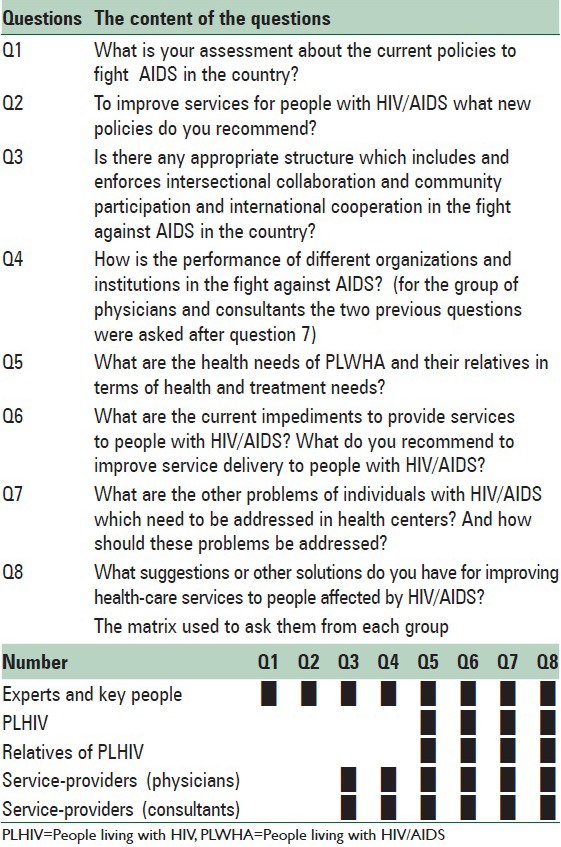
In order to obtain information about rich experiences of the participants, purposive sampling was used; it was tried to enroll participants who had experiences related to the main subject of research and who had experienced different jobs and responsibilities. Inclusion criteria were different based on the nature of the different groups. Inclusion criteria for PLHWA were: History of HIV infection for more than 2 years, history of at least 6 months of referring to one of the service centers, being over 18 years of age, and being literate. Inclusion criteria for the family and relatives of PLWHA included: Continuous living with someone who is infected with HIV/AIDS as his/her spouse, parent, brother or sister, child, or as the guardian of a HIV-positive person, being over 18 years of age, and being literate. Inclusion criteria for service providers were: History of at least 1 year of working experience in one of the service centers which provide services for PLWHA, working as physician or consultant. Two focus group discussions (FGDs) were held for every group of PLWHA, their families, and physicians and consultants, and consequently a total of eight FGDs were performed; the key people were also interviewed in six individual interviews. The data of this study included the opinions and views of the participants and they were collected through asking some questions in semi-structured deep interviews and FGDs. If required, probe questions were used to deepen the responses [Table 1].
Table 1.
Guide questions used for each study groups in the study in 2012
In the case of participants’ approval, each session was recorded by electronic recorder devices. In addition, the nonverbal features and signs were also recorded by the main researcher and the note-taker. All the recorded discussions and interviews were then transcribed and typed.
In order to observe the ethical issues in the study, the researcher asked for participants’ approval to record their voices; in the case of disapproval, the voices were not recorded. They were assured that the content of their discussions would not be disclosed to anybody and would just be kept by the researchers and would be eliminated at the end of the research analysis. Participants in the study were free to decide whether to take part in the study or not and they were allowed to quit the study at any time. To observe ethical considerations, a code was used instead of each participant's name and the code was used while typing and analyzing the content.
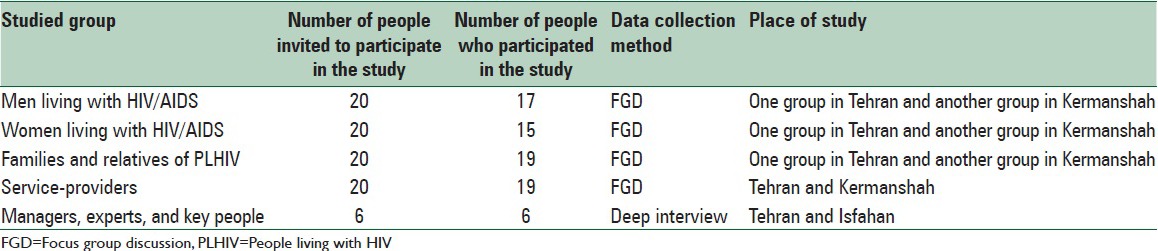
To conduct this study, the study population was divided into five groups. These groups included: (1) Men with HIV/AIDS; (2) women with HIV/AIDS; (3) families and relatives of PLWHA; (4) service providers, including physicians and consultants; (5) managers and experts and key people. Totally, 86 people were invited for the study, and 76 of them were participated [Table 2].
Table 2.
Study groups and number of participants in the each interview techniques in the study in 2012
Open code software was used to analyze data using qualitative content analysis. We used content analysis to categorize the problems based on participants’ point of views. The goal of content analysis is understanding the phenomenon under study through categorization of meaning units.[11] This method compared with other methods such as ethnography, grounded theory, phenomenology, and historical research focuses on the content or contextual meaning of the text[11] and examines language intensely, beyond the words for the purpose of classifying large amounts of text into an efficient number of categories that represent similar meanings.[12]
First, all the interviews were transcribed into texts; the texts were reread several times, and initial codes were identified. During the process of coding, all data were examined line by line, and it was tried as much as possible to report the findings as stated by the respondents. Then, the codes which were semantically similar were classified into identical categories. At the next stage, the identified classes were classified under more comprehensive categories; it was performed to merge classes to reduce the number of categories. To ensure accuracy and reliability of newly coded data, the previously coded interviews were reviewed again.
To guarantee the trustworthiness of the analyzed data, the four strategies of credibility, dependency, conformability, and transferability were applied. In order to ensure credibility, the participants enrolled in the study were selected from among those who had the experience of the subject, that is, HIV. Dependency was achieved by taking the ideas of the research team members into account while reviewing, theme extracting, and analyzing the transcripts. Reviews by researchers and co-authors had led to improved dependency. To enhance conformability of the research, the reports and transcripts were given to several researchers and experts to collect their views and ideas. In addition, to enhance the transferability of the findings, a rich description was provided for the data.
RESULTS
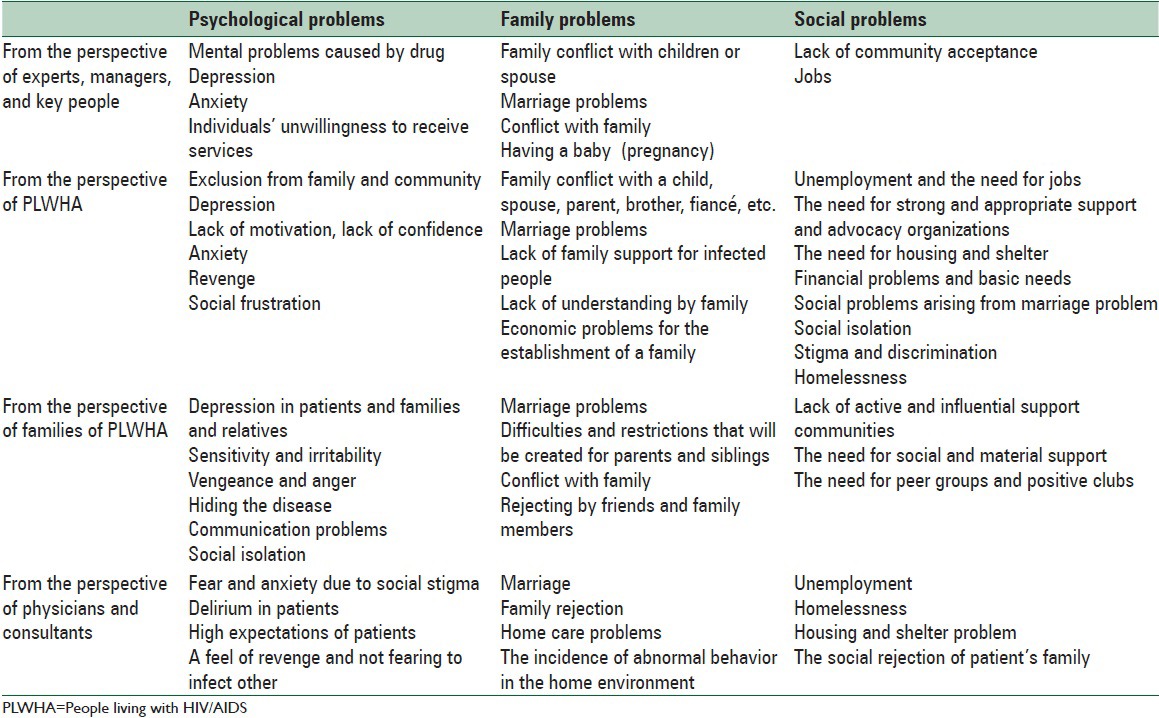
In this study, the problems of PLWHA were classified in three categories of psychological, social, and family problems. Participants’ comments on these topics were collected and categorized under one of the categories. Table 3 summarizes the findings.
Table 3.
Categories of psychological, social, and family problems of PLWHA in view of different participants in the study
Psychological problems
The most common issues raised in relation to psychological health problems of PLWHA and affected people, which were stated by all groups participating in interviews, include the followings: Family and society exclusion, depression and anxiety, a feeling of revenge, no fearing to infect others, frustration, social isolation, relationship problems, and fear and anxiety caused by stigma. Some groups insisted certain issues, and their views were somehow distinct from other views. From the perspective of managers and key people, the most recent and important psychological problems of PLWHA were caused by the use of glass and people's reluctance to receive services. The group of physicians and consultants said that the most important psychological problems of patients are delirium and their high expectations. Below are the views of the different groups involved in the study about the psychological health problems of this group of patients.
Psychological problems from the perspective of experts, managers, and key people
According to one of the managers and experts, the latest and most important psychological problem of PLWHA are those caused by the use of glass: “The growing consumption of glass has caused new psychological problems among patients […] with the emergence of a new phenomenon like the spread of glass use among them […] we have faced new psychiatric or psychological events.” Depression and anxiety are also common in these patients. Fear of the disease and stigma leads to depression and anxiety and it is necessary to provide psychological support for patients to prevent rejection from society and its consequences: “They have to be accepted by their families, because if they would be isolated and ostracized, especially if they have underlying psychological problems, it is possible that they react unusually; for instance, because of poverty, sex-workers may take revenge on society, or act in a way that a normal person would not act. These are due to these emotional changes.” However, experts and key individuals including managers believed that PLWHA were reluctant to receive services.
Psychological problems from the perspective of people living with HIV/AIDS
From the perspective of infected people, the most important issues related to the disease was the exclusion from family life and population. According to the participants, people's education and awareness is very low so that after informing families about the disease of one of their family members, some reacted very badly or even rejected the patient. Some participants put emphasis on the constructive role of peer groups in counseling patients and encouraging them for a positive life. According to patients, they are facing problems such as depression, lack of motivation, and lack of confidence: “I think patients need much deeper psychologically supports […] patients have a very low confidence […] they have so much psychological problems [like] lack of confidence, lack of motivation.” One participant said: “I do not have any good motivation; {loud} what shall I hope? Who does care about me?” PLWHA are facing the problems of anxiety and panic disorders: “I am always in a bad mood. When I see somebody I say how lucky he is, even though he may be also positive. I am always thinking and I am always depressed. I have decided 10 times to kill myself.” Because of isolation from other people and due to related problems, they become indifferent about disease transmission and they will develop a strong feel of revenge on population: “{loud} what shall I hope? Who does care about me?” “There is no support for me to make me motivated to care about others. I don’t care who is going to be infected. When I am infected I cannot care about others. There is no difference between worse and the worst.” According to participants, most patients feel frustrated and have a feeling of loneliness: “Most of the time I just sit by myself talking to myself why? Why me? I cry two to three hours.”
Psychological problems from the perspective of families of people living with HIV/AIDS
According to the families of PLWHA, the disease leads to depression in patients and their families: “His disease affects me more, because I have got mental disorders and depression.” In addition, patients became sensitive and irritable: “Those who are HIV positive are very sensitive and they get very punctilious spirit.” They feel a sense of revenge and anger towards society: “For example, they say we are sick, why shall you stay healthy. I want to do something to make everybody infected.” Families of patients believed that these people tend to hide their illness, because the disease can cause communication problems, for example, it will prevent their marriage. In addition, family members are reluctant to disclose the illness to others and this will cause conflicts in the family. “His sister does not invite her spouse here, she is afraid to tell him that her brother is infected.” The disease leads to a situation in which other relatives of the patient avoid contact with family members: “I know that my family and mother are unwilling to socialize with me and my children.” Such problems lead to the social isolation of patients and their families: “My dad does not socialize with anyone; he does not hug children; he has been isolated; he does not work anymore.”
Psychological problems from the perspective of physicians and consultants
The group of physicians and consultants said that fear and anxiety caused by the stigma are the most important psychological problems of infected people. They believed the disease leads to psychological disorders in patients: “Some of our patients were hallucinating. When I spoke with one of them, he said I am the god of HIV.” In addition, patients’ expectations are very high, and some of them believe that the society is the cause of their illness. As a result, they develop a sense of revenge on other people and they do not fear to infect others: “Those who have high-risk behaviors such as injection say that we have experienced being in prison a lot and suffered many problems, so we do not care to be infected with HIV.”
Family problems
The most common issues related to family problems of PLWHA and affected people that were stated by all groups participating in the interview were as follow: Marriage problems, family conflict, depression, lack of family support, rejecting patients by family members, economic problems inhibiting marriage, and the social rejection of the patient's family. All groups expressed similar problems, and there was no disagreement in relation to family problems [Table 1].
Family problems from the perspective of experts, managers, and key people
In view of managers, marriage is one of the biggest problems of patients, because they do not have suitable conditions for marriage: “We have many, many problems for marriage; I think this is one of the major drawbacks of counseling centers […]. If there would be a possibility for communication we may introduce patients who are ready to marry and have the right conditions to other patients; it may lead to a good marriage with better outcomes; it may be beneficial for the patient. We can eliminate of at least one person as an outbreak in his area; it can be effective.” In addition to the above-mentioned findings, participants noted the following problems: Relationship problems between patients and his/her children, wife, or husband, family conflict, depression, and difficulties in pregnancy.
Family problems from the perspective of people living with HIV/AIDS
In view of participants, information and social awareness is very low, so that the families of some patients when are informed about the illness of their family members treat them very badly and even disavow the patient. Families’ ignorance about how to deal with patients caused family problems and conflict with child, wife, mother, brother, fiancée, and other family members: “One of my brothers clearly knows and understands how I became sick and he can understand that it was not my fault, I felt involuntarily in this hole; however, another one does not understand my condition, he says his daughter must not touch me, he prevents his children to visit our home. It separates us from each other.” One of the patients said: “My family completely cut their ties with me; when I was ill in hospital, I was isolated in a separate room.” Due to the unwillingness of other people to marry infected people, most patients are not able to marry: “I think most patients are facing marriage problem.” Sometimes the marriage problem is even passed to the families of PLWHA: “My oldest son is healthy; however I can[not] find anybody to marry him. I asked my niece to marry my son, her family rejected. Her father said that I can let my daughter go to that family to be infected.” Married people also face a variety of family problems: “My husband grudged a lot. I did not let him go; I loved him. He continued to grudge and did not use condoms. I had got pregnant; I suffered a lot to abort the child. Everyone helped me to abort the baby.” The economic problem is one of the other problems of married people: “HIV positives are financially under the pressure. I have married a HIV positive person who is financially poor; I cannot even introduce him to my kids […] we see each other out of home and he had done nothing for me.” Some of the problems of PLWHA were caused by the lack of family support for patients, so that sometimes even their emotional needs are not met: “We talked so much with my husband, but it did not have any effect. Now, although there is no sex, at least I am his wife, and I really need a hug and I need at least one hand to touch my head.” They suffer from lack of understanding their needs by their family members: “They do not understand us at all; they think we should behave as the same as healthy mothers. I need someone like myself to talk with her. I am close to my kids, but I cannot talk about my illness.” Problems in family relations sometimes extend to relationships between infected mothers and their children: “My son could not understand me […] he asks me for full support; he is expecting a healthy mother who is ready to support him fully. He has the right to live like everyone else does, but he really ignores me in a lot of places. He does not know that I’m sick and I need support; I need rest.”
Family problems from the perspective of families of people living with HIV/AIDS
Marriage problem is one of the most important problems stated by participants: “My son is 26–27 years old, and he has thousands of instincts, thousands of desires. How can I meet his desires? Legal marriage and concubine is too expensive; on the other hand, how can I go to a person [sex-worker] and tell her that my son has problems, come and sleep with him? How can I say this?” In addition, living with an infected person causes limitations and problems for other family members such as mother, father, brothers, and sisters: “I even thought to separate from my husband; he told me to choose one of us, me or your brother.” Sometimes, problems lead to separation and divorce: “We are not divorced now, but we’re living alone. She could not tolerate her child; she is mentally ill.”
Family problems from the perspective of physicians and consultants
Physicians and consultants put emphasis on marriage problems and family rejection. In addition to these two problems, the problems associated with home care were also noted by this group: “Many families refer to us and say that we cannot take care of patients, please give us a referral form so that we take the patient to hospital.” They believed that patients have some abnormal behaviors that cause different problems: “In their family, they have strange behaviors that frustrate the family; for instance, when one of them is shaving, he cuts his face and with a bloody hand touches everything and asks her mother for a towel.” The disease not only affects the patient, but also the family members as well and prevents the family to be accepted by the society: “The child wants to go to school; to get a discount, mother tells school director that the father of this baby is HIV infected; the director behaves badly and severely and rejects the child and does not register him […] some of the other mothers present at school ask the director not to register their children in a class were that boy is going to be registered.”
Social problems
The most common social problems that were expressed by all participants in the interview include: Unemployment and the need for jobs; the need for housing and shelter; basic needs and financial problems; homelessness; lack of active and impressive support communities; and the need for material and social support. Managers and key people believed that social rejection is one of the most important social problems; they also mentioned marriage problems, stigma, discrimination, and social exclusion as the other problems of PLWHA [Table 1].
Social problems from the perspective of experts, managers, and key people
According to experts, managers, and key people, a large amount of social problems are due to rejection by other people and society. They believed that the most important action is to inform and train people to accept them and to facilitate patients’ marriage which is a fundamental issue. In addition, infected people are facing employment problems: “Several steps must be taken to facilitate their employment. Nothing has been done yet to solve the problem. Employment and meeting their basic needs can solve their medical problems as well.”
Social problems from the perspective of people living with HIV/AIDS
According to patients, job and employment are very important problems. “My problem is a financial problem. My daughter is a university student. The Imdad Committee gives us a very little money, sometimes three to 37 thousand Toman. Subsidies are spent on gas bills, because it is too expensive.” Another person said: “{aloud} I’m unemployed; I need rest, what is going to happen to me?” According to PLWHA, support organizations must provide serious and appropriate supports. Moreover, the patients are facing housing and shelter problems: “I spent four days in one of my sisters’ home, and I have to spend four other days in another sister's home.” Approximately all people agreed upon the presence of financial difficulties and needs: “I saw a woman with CD4 below 50 working in other people's home as a servant…. The day I saw this lady she was totally pale.” Different diseases associated with HIV encompass a double burden upon this group: “They shouldn’t leave us alone by ourselves to die. Now, we are suffering at least from three kinds of disease […] we are dealing with hepatitis, HIV, TB, and maybe other diseases as well. How about the other diseases? At least one of them should be addressed.” Financial problems prevent infected people to seek treatment: “I do not seek services beyond those provided here because they are expensive. I do not ask for liver enzymes tests because they are expensive.” According to PLWHA, there is a direct relation between financial welfare and peace of mind and psychological relaxation: “Economic security is very important for HIV positive patients. There is direct link between your pocket and peace of mind and calmness.” Sometimes people even cannot afford the travel costs to attend vocational classes: “Sometime patients do not have enough money in their pockets to commute from a side of the city to the other side to attend vocational classes.” Family life and the problems hindering marriage are among the most common concerns of patients. According to PLWHA, neglecting marriage problem can lead to social problems: “Our problem is marriage. Those who are infected, exactly like me, are similar to moving bombs. We all have some needs. God has given us such a desire and we have to fulfill it.” Failure to meet these needs will lead to the transmission of the disease to other people: “Marriage is very important […] when they would not marry, and they wouldn’t have the chance to marry, they cannot take control of themselves. They start some relationship. They cannot abide and control themselves and the disease will be transmitted.”
As stated by the participants, stigma and discrimination are common problem of PLWHA; after a while, such problems lead to social isolation: “We are a community of socially vulnerable people. I do not have enough power and ability, and I have been so ignored that it is now too hard for me to compensate.” Sometimes discrimination and inappropriate behavior of other people will impose patients to become homeless: “Most of us have this problem and our families have rejected us when they have found that we are infected. A patient might be healthy for two years, but when he is rejected by his family, he uses drug to go to a camp and live there for instance for 20 days.”
Social problems from the perspective of families of people living with HIV/AIDS
Participants said that there is no active and well-organized support community: “There are several communities for everything [every disease] except for AIDS.” They believed patients and their families need material and social support. Besides, they said that the peer groups and positive clubs may be useful and helpful: “I wish there would be a place where they meet themselves, marry each other, because they have to live like other people.”
Social problems from the perspective of physicians and consultants
According to physicians and consultants, one of the most important problems raised by patients is employment. According to the physicians, providing jobs for these people can solve many of their problems, otherwise counseling alone may not be effective. Besides, it is necessary to extend the coverage of insurance supports so that it reduces the cost of drugs and tests. Homelessness and housing and shelter problems were also among the most important social problems stated by consultants: “We have some patients, there are some women, who have three to four children and they do not their own shelters.”
DISCUSSION
The findings of the present study were based on a qualitative approach and it provided us with a deep knowledge in the field of psychological, family, and social problems of PLWHA. Concerning the psychological problems, the major problems of PLWHA which were expressed by all the groups participating in the study were: Family and social exclusion: Depression and anxiety: A feel of revenge and not fearing to infect others; frustration; social isolation; relationship problems; and fear and anxiety caused by social stigma. However, there were some differences in opinions among the participants taking part in the study. From the perspective of managers and key people, the most recent and important psychological problems of PLWHA were caused by the use of glass and people's reluctance to receive services. The group of physicians and consultants said that the most important psychological problems of patients are delirium and their high expectations. There was no disagreement with reference to family problems and all groups agreed upon some problems, including marriage problems, family conflict, depression, lack of family support, rejecting patients by family members, economic problems inhibiting marriage, and the social rejection of the patient's family. The most common social problems of PLWHA that were expressed by all participants include: Unemployment and the need for jobs; the need for housing and shelter; basic needs and financial problems; homelessness; lack of active and impressive support communities; and the need for material and social support. The participants did not agree upon some issues. Managers and key people believed that social rejection is the most important social problems, while PLWHA put emphasis on stigma and discrimination.
Under the category of psychological problems, most PLWHA said that rejection by family and society is their most important psychological health problem. In fact, many people who are among the social network of PLWHA may feel that they are endangered by the disease and since they may become responsible to take care of the patients, they reject patients. This might be due to the lack of information about the nature of the disease and the way that the disease is transmitted; it not only has many adverse physical and psychological consequences for the patient, but also, as the findings of this study have also shown, can initiate a feel of revenge on the people and jeopardize public health. These findings are consistent with the results of studies by Lee et al. (2010) in Thailand, and Roberts-Pittman in United States.[6,13] From the perspective of managers and key people, the most recent and important psychological problems of PLWHA were caused by the use of glass and people's reluctance to receive services. Using glass may result in extreme irritability, inability to control anger, family and social violence, strong suspicion toward family members and those in close contact, and loss of responsibility and attention; it not only leads to permanent psychological disorders, but also increases the chance of disease transmission. According to physicians and consultants, the most important psychological problems of patients are delirium and their high expectations. It might be said that due to distrusting service providers for disclosing HIV infection, limited facilities, lack of access to facilities, inefficiency of staff in terms of moral and professional aspects, and also because of the side effects of drugs, patients might despair about the future; it is consistent with the results of other studies.[14]
Under the category of family problems, the most important issues raised by participants from different groups were lack of support and rejection from families; it is consistent with the results of Masoudi and Farhadi study (2005) which was conducted in Iran.[15] These findings are important because appropriate support from families enables them to have appropriate responses to the stress which is caused by illness and therefore they will have less psychological problems. It will increase their compliance to the treatment and prevents the transmission of infection to others. Because when a patient with AIDS is accepted by the family and community and when he is treated without any stigma and discrimination, the other susceptible individuals are more likely to be encouraged to ask for diagnosis and treatment; accordingly, more cases of HIV in the community will be identified and the disease will be controlled better. However, when families and society treat patients negatively, so that they would be isolated and excluded, the disease will spread in a clandestine mode of transmission and a major part of the infected population will remain hidden. As a result, the number of patients will increase.
Marriage problem was the other issue raised in the context of family and social problems. In fact, it can be said that, considering the average age of the patients who are largely in active young ages, there are not enough facilities for marriage. On the other hand, social stigma and negative attitudes of society toward the disease have led to more limitations and problems which hinder marriage. In fact, marriage problems and inability to form a family not only leads to mental health problems such as depression and isolation, but also can cause social damages. In other words, when the sexual needs of patients are not fulfilled via marriage and family formation, there may be an increase in high-risk behaviors. Considering the warnings about the risk of the third wave of HIV infection, which spreads through sex, health planners and policy-makers must design special solutions to deal with this problem.
Under the category of social problems, the most important problems stated by PLWHA who participated in this study were stigma, discrimination, and social exclusion. According to experts, managers, and key people, a large amount of social problems are due to rejection by other people and society. The present results are consistent with the results of many studies in this field.[16,17] Based on the literature, social stigma and discrimination associated with the disease have a significant relationship with poor physical and mental health, depression, and reduced quality of life for PLWHA. Due to the negative attitudes of society and the social stigma and discrimination, in many cases, these people are deprived of their most basic rights, such as employment, marriage, education, etc.
CONCLUSIONS
Stigma, discrimination, and social rejection by other people can lead to physical and mental problems; it can lead to the disclosure of HIV infection status, which in turn can increase the risk of developing the hidden cases of disease.[18]
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- 1.Mohraz M, Malek-Afzalip H, Goya MM, Sedaghat A, Namdari H, Dejman M, et al. Iran, Tehran: AIDS Research Center and UNAIDS; 2011. Integrated Model of HIV/AIDS in the Primary Health Care System. [Google Scholar]
- 2.UNAIDS. Global Report 2012: UNAIDS Report on the Global AIDS Epidemic. 2013. [Last accessed on 2014 Oct 05]. Available from: http://www.ebookpartnership.com .
- 3.Tehran: Ministry of Health and Medical Education; 2012. National Aids Committee Secretariat, Ministry of Health and Medical Education. Islamic Republic of Iran Progress Report, On Monitoring of the United Nations General Assembly Special Session on HIV and AIDS. [Google Scholar]
- 4.Charkheyan A. Tehran: University of Social Welfare and Rehabilitation; 2008. Relationship between social support and quality of life in HIV-infected people referred to Imam Khomeini Hospital in Tehran. [Google Scholar]
- 5.Hall VP. The relationship between social support and health in gay men with HIV/AIDS: An integrative review. J Assoc Nurses AIDS Care. 1999;10:74–86. doi: 10.1016/S1055-3290(05)60121-5. [DOI] [PubMed] [Google Scholar]
- 6.Roberts-Pittman B. Indiana, USA: Indiana State University; 2006. An Analysis of the Social Support Network of Gay Men Living with HIV. [Google Scholar]
- 7.Forouzan AS, Jorjoran Shushtari Z, Sajjadi H, Salimi Y, Dejman M. Social support network among people living with HIV/AIDS in Iran. AIDS Res Treat 2013. 2013:715381. doi: 10.1155/2013/715381. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Kalichman SC, DiMarco M, Austin J, Luke W, DiFonzo K. Stress, social support, and HIV-status disclosure to family and friends among HIV-positive men and women. J Behav Med. 2003;26:315–32. doi: 10.1023/a:1024252926930. [DOI] [PubMed] [Google Scholar]
- 9.UNAIDS. Republic of Iran Progress Report On Monitoring of the United Nations General Assembly Special Session on HIV and AIDS Tehran, 2014. [Last accessed on 2015 Aug 11]. Available from: http://www.unaids.org/sites/default/files/en/dataanalysis/knowyourresponse/countryprogressreports/2014countries/IRN_narrative_report_2014,_en.pdf .
- 10.Tehran, Iran: 2007. Ministry of Health and Medical Education Islamic Republic of Iran, First National AIDS controls program monitoring and evaluation 2004-2006. [Google Scholar]
- 11.Hsieh HF, Shannon SE. Three approaches to qualitative content analysis. Qual Health Res. 2005;15:1277–88. doi: 10.1177/1049732305276687. [DOI] [PubMed] [Google Scholar]
- 12.Weber RP. 2nd ed. USA: Sage; 1990. Basic Content Analysis. [Google Scholar]
- 13.Lee SJ, Jiraphongsa C, Iamsirithaworn S, Khumtong S, Rotheram-Borus MJ. Regional variations in HIV disclosure in Thailand: Implications for future interventions. Int J STD and AIDS. 2010;21:161–5. doi: 10.1258/ijsa.2009.009008. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Fallahi H, Akbar F, Faranak F, Masood Y, Farahnaz A. Benefit people with HIV of dental services and it's related factors. Payesh. 2008;7:59–65. [Google Scholar]
- 15.Masoodi M, Farhadi A. Levels of family social support to people of HIV positive/AIDS. J Lorestan Univ Med Sci. 2005;26:43–7. [Google Scholar]
- 16.Li L, Lee SJ, Thammawijaya P, Jiraphongsa C, Rotheram-Borus MJ. Stigma, social support, and depression among people living with HIV in Thailand. AIDS Care. 2009;21:1007–13. doi: 10.1080/09540120802614358. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Peltzer K, Ramlagan S. Perceived stigma among patients receiving antiretroviral therapy: A prospective study in KwaZulu-Natal, South Africa. AIDS Care. 2011;23:60–8. doi: 10.1080/09540121.2010.498864. [DOI] [PubMed] [Google Scholar]
- 18.Jorjoran Shushtari Z, Sajjadi H, Forouzan AS, Salimi Y, Dejman M. Disclosure of HIV Status and Social Support Among People Living With HIV. Iran Red Crescent Med J. 2014;16:e11856. doi: 10.5812/ircmj.11856. [DOI] [PMC free article] [PubMed] [Google Scholar]