

Abstract
Background
Positive psychology interventions have been found to enhance well-being and decrease clinical symptomatology. However, it is still unknown how flourishing can also be increased. Although multicomponent interventions seem to be necessary for this purpose, different formats can be used. A cost-effective approach could be a positive psychology-based self-help book with tailored email support to reach large target groups and to prevent dropout.
Objective
This study will evaluate the efficacy of a comprehensive multicomponent self-help intervention with or without email support on well-being and flourishing, and will seek to determine the working mechanisms underlying the intervention.
Methods
In this 3-armed, parallel, randomized controlled trial, 396 participants with low or moderate levels of well-being and without clinical symptomatology will be randomly assigned to (1) a self-help book condition with weekly email support, (2) a self-help book condition without email support but with a weekly information email, or (3) a waiting list control condition. Online measurements will be assessed at baseline, at post-test (3 months after baseline), and at 6 and 12 months after baseline.
Results
The primary outcomes are well-being and flourishing (ie, high levels of well-being). Secondary outcomes are the well-being components included in the intervention: positive emotion, use of strengths, optimism, self-compassion, resilience, and positive relations. Other measures include depressive and anxiety symptoms, personality traits, direct medical and non-medical costs, life-events, and client satisfaction.
Conclusions
This study will add knowledge to the efficacy and cost-effectiveness of a multicomponent positive psychology intervention. We will also explore who can benefit most from this intervention. If the intervention is found to be effective, our results will be especially relevant for public mental health services, governments, and primary care.
Trial Registration
The Netherlands Trial Register NTR4297; http://www.trialregister.nl/trialreg/admin/rctview.asp?TC=4297 (Archived by WebCite at http://webcitation.org/6Uwb5SUUM).
Keywords: well-being, flourishing, mental-health promotion, positive psychology, self-help, email support
Introduction
Background
Since the introduction of positive psychology in 1998 [1], the proportion of published studies on this topic has grown rapidly each year compared to the entire field of psychological research [2]. Researchers have argued that the study of positive psychology is more capacious than the field of psychopathology because its primary focus is not on dysfunction but on well-being and optimal functioning [3]. Recent evidence indicates that positive mental health and mental illness are related but different continua [4-6]. This so-called two-continua model implies that individuals can experience positive outcomes such as life-satisfaction, meaning, and personal growth when mentally ill, and that the absence of mental illness does not automatically imply high levels of positive mental health [7,8]. As a consequence, researchers have underscored the importance of enhancing positive mental health in addition to preventing and treating mental illness, in clinical populations as well as in the general population [3,9].
A central aim in positive psychology is to increase the amount of flourishing worldwide [1,10]. Flourishing is defined as the presence of high levels of the affective or “feeling good” dimension of well-being (ie, hedonic well-being) in combination with high levels of the psychological functioning or “living well” dimension of well-being (ie, eudaimonic well-being) [4,9,11]. Compared to “languishers” (ie, people at the lowest levels of hedonic and eudaimonic well-being) and individuals with depression, research has shown that flourishers experience the least emotional distress and psychosocial impairment, have hardly any lost work days, and are most likely to survive [4,8]. Keyes and colleagues [12] have found initial support for the hypothesis that an increase in well-being protects against the development of mental illness. More specifically, they found that the risk for having a mental disorder was equally lowest for individuals who were flourishing in 1995 and in 2005, and for individuals who were flourishing in 2005 but not in 1995 [12]. The same study also indicates that it is possible to enhance the amount of flourishing [12]. However, there seems to be significant room for improvement because epidemiological studies using the same operationalization of flourishing have found that there were only 17% flourishers in the United States [4], 20% flourishers in South Africa [13], and 37% flourishers in The Netherlands [14]. Some researchers theorize that even small improvements in the level of well-being in the general population could generate large preventive effects on the amount of psychopathology [9,15]. Yet, little is known about how the amount of flourishing can be increased. The present study will evaluate a theory- and research- based positive psychology intervention (PPI) on efficacy, specific working mechanisms, and cost-effectiveness for enhancing well-being and flourishing in the general population.
Positive Psychology Interventions
A large number of theories have been used to develop interventions and exercises within the positive psychology movement, as can be found in the Key Competence Happiness Database [16]. Two meta-analyses have shown that PPIs significantly enhance well-being and alleviate depression in the short term, although effect sizes were relatively small [17,18]. These small effect sizes might be a result of the nature and intensity of the included interventions, which were mostly single-component interventions (ie, one or more individual exercises targeting one component of well-being). Examples are “the three good things exercise” or “savoring” targeting positive emotion, and “using one’s strengths in new ways” to increase flow. However, since well-being is a multifaceted construct [10,19] it might be more efficacious to promote well-being and flourishing with a multicomponent intervention that contains a variety of evidence-based individual exercises targeting 2 or more theoretically relevant hedonic and eudaimonic well-being components. For example, the well-being theory of Seligman [10] states that the components of positive emotion, engagement, relationships, meaning, and accomplishment (PERMA) are all necessary for flourishing. Also, multicomponent interventions are higher intensity, target more resources of well-being in an individual, and are often of longer duration than single-component interventions, which may increase their efficacy.
In the last decade, some multicomponent PPIs have been investigated, including different face-to-face interventions. Examples are (1) Positive Psychotherapy, a structured 14-session program developed for individual or group therapy in clinical settings based on Seligman’s well-being theory [10,20,21], (2) Well-being therapy, an individual psychotherapeutic strategy of 8-12 sessions that is based on Ryff’s model of psychological well-being [19] and therefore contains strategies and therapeutic techniques to influence the components self-acceptance, environmental mastery, positive relations with others, personal growth, autonomy, and purpose in life [22], and (3) the Working for Wellness Program, a structured 6-week group-based program for employees with a strong focus on strengths, flow, and social relationships [23]. The efficacy of these multicomponent PPIs on mental illness and positive mental health have been demonstrated in a wide variety of studies—including randomized controlled trials (RCTs)—although most of these studies used small samples [20,22,23]. However, the need for trained therapists in these intensive face-to-face PPIs is a disadvantage that may limit their feasibility, cost-effectiveness and dissemination.
Positive psychology exercises have the advantage of being relatively small and easy-to-implement in daily life, and are therefore well-suited for self-administered interventions. Recently, some Web-based multicomponent PPIs have been developed to increase the reach of PPIs. For example, Schueller and Parks [24] selected 6 exercises from the Positive Psychotherapy intervention (active-constructive responding, gratitude visit, life summary, three good things, savoring, and strengths) and randomly assigned participants to a 6-week program containing all 6 exercises, 4 of the exercises, or 2 of the exercises. The 2- and 4-exercise programs resulted in significantly larger effects on depressive symptomatology than the control group and the 6-exercise program, although participants in the latter program practiced the exercises on significantly more days than participants in the 2- or 4-exercise programs [24]. Another, more comprehensive intervention is Psyfit. This intervention contains 6 modules, each with 4 lessons, about goal setting, positive emotion, positive relations, mindfulness, optimism, and mastery [25]. An RCT showed significant but small effects on well-being and depressive symptomatology, although most participants completed less than 4 lessons of 1 or more modules [25]. While these and other Web-based multicomponent PPIs have shown that they can reach many individuals, their cost-efficacy seem to be limited by low adherence rates [24-27], which could be due to the lack of human contact and coaching [27,28].
Self-Help Book With Email Support
Another, possibly cost-effective approach could be to intertwine the advantages of the aforementioned formats by using an accessible self-help book in combination with email support to reach and stimulate large groups of individuals at minimal costs. Meta-analyses have shown that the use of self-help books—also called bibliotherapy—with or without support are effective in the treatment of depression [29,30] and the treatment of alcohol problems [31]. Also, research on guided self-help in the form of email support in combination with face-to-face therapy or online therapy has shown promising results [32,33]. Besides, there are some indications that tailored email support is more effective than no support or automated email support [32,34]. More important, promising findings have been found for the use of positive psychology-based self-help books without any support [35-37] or with email support [38]. For example, Parks and Szanto [37] compared a PPI group of students who received the book “The How of Happiness” [39] to a group of students who received a cognitive behavioral self-help book to cope with depression and a control group. Results showed that both intervention groups were equally effective in reducing depressive symptoms at post-test compared to the control group, and that significant increases in life-satisfaction were found only for the PPI compared to the control condition at the 6-month follow-up. Another study used a multicomponent self-help book based on acceptance and commitment therapy in a sample with mild to moderate depressive symptomatology [38]. One intervention group received the book with extensive and tailored email support on progress and process, while another group received the book with minimal email support on progress. Results revealed significant increases in well-being and mindfulness and significant decreases in depressive, anxiety, and fatigue symptomatology for both intervention groups at 3-months follow-up compared to a waiting list control group [38]. In this study, we will use a version of the extensive email support similar to that used in the latter study [38]. That is, participants will be guided through the self-help book by tailored email feedback from trained counselors, but we will compare it to receiving an information email instead of minimal email support.
This Study
This study will examine a comprehensive multicomponent positive psychology-based self-help book with email support. The self-help book is entitled, “This is your life” (TL) [40] and targets 6 key components in positive psychology: positive emotion, use of strengths, optimism, self-compassion, resilience, and positive relations. We will compare a condition wherein participants receive the book with weekly asynchronous and tailored email support (TL-E) to a condition wherein participants receive the book with a weekly email with information (TL-I). Both groups will be compared to a waiting list control condition (WL). Our research aim is to evaluate the efficacy of the multicomponent self-help book with or without email support in terms of well-being and flourishing in an RCT (NTR4297) and to evaluate which of the included well-being components in the self-help book contribute to its efficacy. We expect that TL-E will be equivalent or superior to TL-I and superior to WL at post-test and 6 months follow-up, and that the effects will be sustained at 12 months follow-up.
This study will add to current knowledge in 3 ways. First, it will be conducted in a sample with low or moderate levels of well-being without moderate or severe clinical symptomatology, which is a potential “happiness-seekers” group [41] that has not previously been studied in PPIs [17,18,27]. Second, this study will gain insight into the working mechanisms underlying the intervention by evaluating which of the included well-being components in the self-help book (ie, positive emotion, use of strengths, optimism, self-compassion, resilience, and positive relations) contribute to its efficacy and by examining individual differences in demographic characteristics, number of life events, personality traits, and adherence rates. Third, this study will examine if the innovative format used in this study (ie, self-help book with relatively inexpensive email support) is a cost-effective approach for enhancing well-being and flourishing compared to a waiting list control group, since little is known about the cost-effectiveness of PPIs [26].
Methods
Study Design
This study is a parallel RCT with 3 groups: a group receiving the self-help book with weekly asynchronous and tailored email support (TL-E); a group receiving the self-help book without email support but with a weekly information email (TL-I); and a waiting list control group (WL). Outcomes will be assessed at baseline (T0), post-test (around 3 months after baseline; T1), and at 6 (T2) and 12 months (T3) after baseline. All measurements will be self-reported and gathered via email with a link to a personal questionnaire built with Qualtrics software [42]. The design and procedures of this study were approved by the Ethics Committee of the University of Twente in The Netherlands (no. 13212).
Participants
Participants will be recruited from the general population in The Netherlands using newspaper advertisements. The recruitment messages will be positively framed: (1) “Get the best out of yourself and improve your resilience and well-being with a free self-help course”, and (2) “Become happy and stay happy? Improve your resilience and well-being with a free self-help course”.
Interested participants will be directed to a website with extensive information about the study and an application form. After applying, participants will be sent a personal link to a screening questionnaire on their specified email address. Participants who open the personal link will be asked to give online informed consent. If no informed consent is given, participants will be diverted to the information website and will not be able to participate in the study. If informed consent is given, participants will fill out the screening questionnaire before the start of the study. Figure 1 shows the intended flow-chart of participants.
Figure 1.
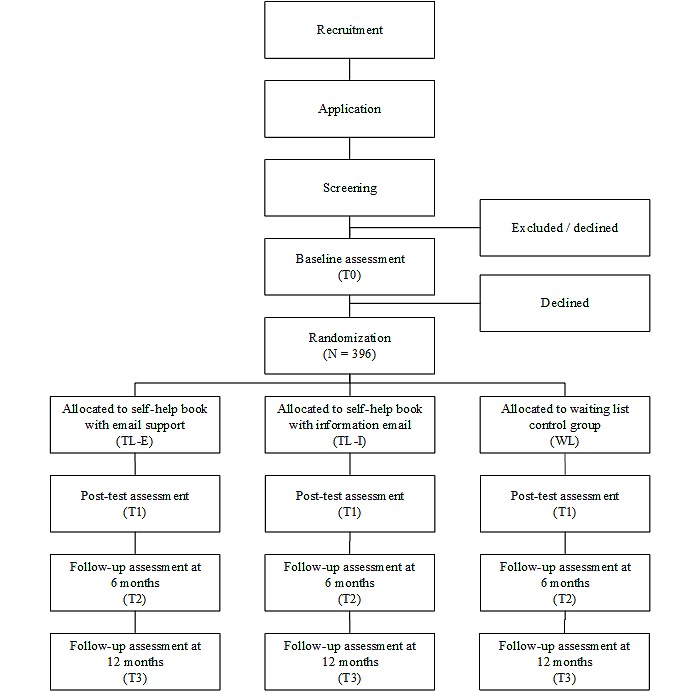
Design of the study and intended flow-chart of participants.
Adults aged 18 or above with low or moderate levels of well-being without moderate or severe clinical symptomatology are eligible for this study because previous studies have shown that these individuals might search for happiness [41] and could boost their mental health by elevating the level of well-being [7,8]. Other inclusion criteria are a sufficient internet connection, a valid email address, and a willingness to invest an average of 4 hours per week for 8-12 weeks. In the screening questionnaire, the Mental Health Continuum Short Form (MHC-SF) will be used to assess the level of well-being and the Hospital Anxiety and Depression Scale (HADS) will be used to assess the level of clinical symptomatology. Participants will be excluded from the study if they score 4 or 5 (range 0-5) on at least 1 of the 3 emotional well-being items in combination with a score of 4 or 5 (range 0-5) on at least 6 of the 11 social and psychological well-being items of the MHC-SF, which is operationalized as flourishing (ie, high levels of well-being) [13,43]. Participants will also be excluded if they score 10 or higher (range 0-21) on the depression scale and/or on the anxiety scale of the HADS, which indicates individuals with moderate or severe clinical symptomatology [44]. Participants who will be excluded from the study will be notified by email because, (1) they are already flourishing, or (2) they probably have at least moderate depression or anxiety symptoms. The latter group will receive their specific scores and their meaning on the HADS and will be advised to talk to their general practitioner when symptoms persist or increase. After screening, the remaining participants receive a personal email link to the baseline questionnaire.
Randomization
Randomization will be conducted after all eligible participants complete the baseline questionnaire, with 396 participants being randomly assigned to 1 of the 3 groups (allocation ratio, 1:1:1). Randomization will be stratified by gender and educational level (ie, low, medium, high) using a computerized random number generator created with Excel. This is an automated process with no interference from the investigators.
Interventions
This study will use the self-help book, “This is your life” [40] in both experimental conditions. This book is mainly based on the overarching and comprehensive well-being theory of Seligman [10] and Ryff’s theory of psychological well-being [19]. The book consists of 8 modules on 6 key components in positive psychology: positive emotion; discovering and using strengths; optimism and hope; self-compassion; resilience and post-traumatic growth; and positive relations (Table 1). Each module contains psycho-education derived from specific theories and empirical evidence in positive psychology and related research areas. Each module also contains a number of positive psychology exercises, ranging from 3-10 per module. Most of these exercises are evidence-based, such as the "three good things exercise" [17,18] and "imagine your best possible self" [45-47]. All modules are, in theory, effective independent strategies for enhancing well-being. Participants in the experimental groups will receive the self-help book by regular mail, accompanied by a time schedule for reading the book and practicing the recommended exercises (see Table 1). Participants will be instructed to read one module per week—except for module 2, which can be spread out over two weeks—in sequential order, and to practice the recommended exercises of that module. If the participant has more time, he or she can re-read the module and practice other exercises of that module. Participants will be encouraged to invest the most time in the exercises that feel most beneficial to them. Participants will have 8-12 weeks to complete the 8 modules of the book to take holidays and other circumstances into account. When participants in the TL-E group need more than 9 weeks to complete the book, in consultation with the counselor, they will not receive email support in the weeks they are not in the position to work on a module. Participants in the TL-I group will receive weekly information emails during the first 9 weeks and will be asked to read the emails in chronological order in the weeks they actually work on a module. On average, participants in the experimental groups will be expected to invest 4 hours per week during the intervention period.
Table 1.
Content of “This is your life” and recommended exercises for participants in the experimental conditions.
| Module | Recommended exercises | Theoretical background |
| 1. Positive emotions |
|
Fredrickson, 1998 [48]; Fredrickson, 2001 [49]; Fredrickson, 2009 [50] |
|
|
|
|
| 2. Discovering strengths |
|
Linley et al., 2010 [51]; Linley and Harrington, 2006 [52] |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
| 3. Use of strengths, flow |
|
Csikszentmihalyi, 2001 [53] |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
| 4. Optimism, hope |
|
Carver et al., 2010 [54]; Scheier and Carver, 1992 [55]; Seligman, 1990 [56] |
|
|
|
|
|
|
|
|
| 5. Self-compassion |
|
Gilbert, 2009 [57]; Neff, 2003 [58]; Neff and Germer, 2012 [59] |
|
|
|
|
|
|
|
|
| 6. Resilience |
|
Joseph, 2011 [60]; Joseph and Linley, 2006 [61]; Tedeschi and Calhoun, 2004 [62] |
|
|
|
|
|
|
|
|
|
|
|
|
| 7. Positive relations (I) |
|
Gable et al., 2004 [63]; Reis and Gable, 2003 [64]; Reis et al., 2010 [65]; Rosenberg, 2009 [66] |
|
|
|
|
|
|
|
|
|
|
|
|
| 8. Positive relations (II) |
|
Bloom, 2011 [67]; Otake et al., 2006 [68] |
|
|
|
|
|
|
|
|
Email Support
The TL-E group will receive weekly email support from a personal counselor. These counselors will be 5 senior positive psychology students of the University of Twente who completed a course on email counseling in which they are trained to guide a fellow student on using the self-help book “This is your life”. Each of these will guide 25 participants and the remaining participants will be guided by the first author (MS). Participants will be randomly assigned to 1 of the 6 counselors in the same manner as the randomization procedure outlined above (eg, stratified by gender and educational level). Additional training will be given in a 1-day workshop and via weekly supervision by authors MS and EB and a clinical psychologist. In these meetings, random emails of the counselors will be discussed to increase treatment integrity, and counselors can ask specific questions to the supervisors. The personal counselors will introduce themselves in an initial email sent the day participants receive the self-help book. The participants will be asked to introduce themselves before the email sessions start. Participants will be instructed to send a weekly email on Sunday or Monday wherein they write about their experiences with the scheduled module. Every Wednesday, the personal counselors will answer the emails.
The main goal of the email support is to encourage the participants to read the scheduled modules and practice the recommended exercises. The email support will be more process-oriented than content focused, and will be flexible within the boundaries of the structured time schedule. The personal counselors will be instructed to provide tailored feedback on progress and process using positive reinforcement, paraphrasing, and motivational interviewing techniques (eg, “I read that you have invested quite some time in the recommended exercises of this week.”; “Could it be helpful for you to practice this exercise more regularly?”; “What have you discovered when you performed the exercises?”). Specifically, counselors will use positive reinforcement for signs of awareness, insights, improvement and change (eg, “This seems a valuable experience for you, how exactly did you achieve that?; “What will be a next sign of progress?”; “That seems like a helpful thought to me.”). When there are reasons to assume that a participant has serious complaints, the participant will be referred to a general practitioner or a health care specialist. In an attempt to reduce intervention dropout, reminders will be sent to participants who do not send an email to their counselor. The first 2 reminders will be sent by the personal counselor, followed by up to 3 additional reminders sent by the researcher (MS). If a participant has completed more than 3 modules of the book, he or she will only receive reminders from their personal counselor. A final email with overall feedback on the process of the participant will be sent to all participants who complete at least 3 modules. This final email will be sent when the participant has completed all modules (between 8 and 12 weeks), when the maximum of 3 reminders has been reached by the personal counselor, or when participants are in week 12 of the study without completing all modules.
Email With Information
The TL-I group will receive a weekly email from the investigator that contains additional information about the self-help book or the study. A frequently-asked-questions (FAQs) format will be used for this email (eg, “Q: How can I find the time to practice the recommended exercises?” “A: Select a good moment in your daytime routine, so that practicing the exercises can become a habit. For example, during lunch time, directly after work or half an hour before bed time.”). The information emails will be a work-in-progress during the study because FAQs by participants in the TL-E group will also be integrated into the information emails. Participants will be instructed to read the weekly emails and not to respond to the investigator.
Control group
Participants in the control group will be on a waiting list for the first 6 months of the study and will receive the self-help book after they complete the 6-month follow-up assessment. For the sake of comparison at the long-term follow-up, the control group will also receive the information emails in the same way provided in the TL-I group.
Measures
For a brief overview of all outcome measures and assessment times, see Table 2. Because one of our aims is to examine the working mechanisms underlying the intervention, which requires assessing all included positive psychology components, measures are selected on brevity and availability in the Dutch language.
Table 2.
Intended questionnaires and assessment times.
|
|
|
|
T0 | T1 | T2 | T3 |
| Questionnaire | Measurement | Screening | Pre-test | Post-test | Follow-upa | Follow-upb |
| MHC-SF | Well-being/ flourishing | X | X | X | X | X |
| FS | Social-psychological well-being |
|
X | X | X | X |
| HADS | Symptoms of depression and anxiety | X |
|
|
X | X |
| m-DES | Positive and negative emotions |
|
X | X | X | Xd |
| SUS | Use of strengths |
|
X | X | X | Xd |
| LOT-R | Optimism |
|
X | X | X | Xd |
| SCS-SF | Self-compassion |
|
X | X | X | Xd |
| BRS | Resilience |
|
X | X | X | Xd |
| SPR | Positive relations |
|
X | X | X | Xd |
| EPQ-RSS | Extraversion and neuroticism |
|
X |
|
|
|
| NEO-FFI | Conscientiousness |
|
X |
|
|
|
| MCQ | Direct medical consumption costs |
|
X | Xc | Xc | X |
| PCQ | Non-medical productivity costs |
|
X |
|
|
X |
| Brugha Life-events | Positive and negative life-events |
|
X | X | X | X |
| CSQ-8 | Client satisfaction |
|
|
Xd |
|
|
| Process evaluation | Invested time, adherence, positive changes |
|
|
Xd |
|
Xe |
|
|
Level of (continued) use |
|
|
|
|
X |
| Demographics | Gender, age, education, marital status, living situation, ethnicity, daily activities | X |
|
|
|
|
a 6 months after T0.
b 12 months after T0.
c Only medical health care costs are assessed, not medication costs.
d Only assessed in the experimental groups, not the control group.
e Only assessed in the control group, not the experimental groups.
Primary Outcome
Well-being is the primary outcome of this study, measured with the 14-item MHC-SF and the 8-item Flourishing Scale (FS). The items of the MHC-SF can be divided into 3 subscales: emotional well-being (3 items), social well-being (5 items), and psychological well-being (6 items). All items can be answered on a 6-point answer scale from 0 (never) to 5 (almost always). A mean score will be computed separately for the total scale and the 3 subscales. The MHC-SF has excellent psychometric properties [5,13]. The FS measures social-psychological well-being with 8 positively formulated items. Participants rate the items on a 7-point scale from 1 (strongly disagree) to 7 (strongly agree). Total summed scores can range from 8-56. The FS has demonstrated good internal consistency and construct validity [69].
Secondary Outcomes
The MHC-SF is also used to measure the amount of flourishing [13,43]. Flourishers score 4 or 5 on 1 or more items on the emotional well-being subscale in combination with a score of 4 or 5 on 6 of the 11 remaining items. Languishers are those with scores of 0 or 1 on these subscales, and individuals who are neither flourishing nor languishing are labelled as moderately mentally healthy.
Depressive and anxiety symptoms will be measured with the HADS [44]. Each subscale consists of 7 items, 14 items in total. Answer categories differ per item, but all items have 4 answer categories with scores ranging from 0-3. Item scores are summed into a total scale score for anxiety (range 0-21) and depression (range 0-21). The HADS is a widely validated instrument and can be used as a screening instrument in different populations [70,71]. A cut-off score of 10 and above on each subscale is generally used to identify individuals with at least mild depressive or anxiety symptomatology [44,70].
Positive and negative emotional states will be assessed with the modified Differential Emotions Scale (m-DES), which measures 8 groups of positive emotions and 8 groups of negative emotions on a 7-point scale (1 = not at all, 7 = very intense). Total mean scores will be computed. Although the DES is validated and widely used, the m-DES has not yet been validated [72].
The Strength Use Scale (SUS) is a 14-item scale to assess participants’ use of their strengths in a variety of settings [73]. Scores range from 1 (strongly disagree) to 7 (strongly agree) with a total summed score of 14 to 98. The SUS possesses high internal consistency and long-term stability [74].
Optimism will be assessed with the 10-item Life Orientation Test-Revised (LOT-R) [75,76]. Items are rated on a 5-point scale ranging from 0 (strongly disagree) to 4 (strongly agree) and indicate participants’ evaluation of positive expectations about the future. There are 4 filler items which are excluded from analysis. Scores on the 6 items are summed into a total optimism score ranging from 0-24. The LOT-R has shown predictive and discriminant validity [75].
Self-compassion will be assessed with the Self-Compassion Scale-Short Form (SCS-SF), which consists of 12 items. Participants rate the items on a 7-point scale ranging from 1 (rarely or never) to 7 (almost always) with a total summed score ranging from 12-84. The SCS-SF has proven to be a valid equivalent of the long-form version [77] developed by Neff [78].
The 6-item Brief Resilience Scale (BRS) [79] will be used to evaluate the level of resilience, which is the ability to bounce back and cope with stress or negative life-events. Items are rated on a 5-point scale from 1 (strongly disagree) to 5 (strongly agree) with total mean scores ranging from 1 to 5. The psychometric properties are good [79].
Although positive relations will be assessed with 1 item of Ryff’s scales of psychological well-being [19] in the MHC-SF, we will also measure the original Subscale of Positive Relations (SPR) as proposed by Ryff [19]. This subscale contains 9 items and a 6-point scale ranging from 1 (strongly disagree) to 6 (strongly agree) [80] and a total summed score that range of 9-54.
Tertiary Outcomes
The personality traits extraversion and neuroticism will be assessed with the Eysenck Personality Questionnaire-Revised Short Scale (EPQ-RSS) [81-83] and conscientiousness with the NEO Five Factor Inventory (NEO-FFI) [84]. These personality surveys are widely used and validated. Direct medical and non-medical costs will be measured with the Dutch Medical Consumption Questionnaire (MCQ) [85] and 5 items from the Productivity Cost Questionnaire (PCQ) [86]. Other variables that will be assessed are positive and negative life-events with a scale based on the Brugha Life-events section [87], and the socio-demographics of gender, age, educational, marital status, living situation, ethnicity, and daily activities.
Process Outcomes
The Client Satisfaction Questionnaire-short form (CSQ-8) [88,89] will be used to determine overall satisfaction. Additional questions will be asked about time spent with the intervention and self-help book modules, adherence to each module, and significant positive changes since they started with the intervention. The latter question is based on the Client Change Interview Protocol [90]. All email correspondence between participants and personal counselors will be retrieved and saved for content analysis.
Sample Size
Well-being is the primary outcome used for the power calculation. We expect to detect a significant effect on well-being between the experimental groups TL-E and TL-I compared to the WL group. Based on recent meta-analyses [17,18] and a previous comparable study [38], we expect to find a standardized effect size on well-being of 0.40 or larger. The targeted sample size is 99 participants per group (297 in total) to provide a statistical power of (1 - β) = 80% and a 5% significance level (two-tailed). To allow a study dropout rate of 25%, we need 132 participants in each condition and 396 participants in total for the trial.
Statistical Analyses
The Consolidated Standards of Reporting Trials (CONSORT) statement [91] will be used to report the results. Independent t tests and Chi-square statistics (X2) will be used to examine baseline differences between the study groups. Non-significant socio-demographic differences at baseline will indicate successful randomization. Internal consistency of the constructs will be determined using Cronbach’s alpha. To examine the efficacy of the intervention, intention-to-treat analyses will be conducted by including all participants in the analyses who have been randomized. The Expectation Maximization (EM) method will be used to impute all missing data on the continuous measures of T1, T2 and T3. This method imputes the data by maximum likelihood estimation using the observed data in an iterative process [92]. The intention-to-treat analysis will be compared with a completers-only analysis.
To examine significant differences between the 3 groups, we will perform repeated measures ANOVA in a 3 (group) x 3 (time) design with well-being (MHC-SF and FS) as the primary dependent variable and positive/negative emotions (mDES), the use of strengths (SUS), optimism (LOT-R), self-compassion (SCS-SF), resilience (BRS), and positive relations with others (SPR) as the secondary dependent variables. Significant time x group interactions will be tested with Tukey’ post hoc tests. Within-group effects (Cohen’s d) will be calculated by subtracting the mean post-test or follow-up score from the mean baseline score and dividing the difference by the pooled standard deviation. Between-group effects (Cohen’s d) will be calculated by subtracting the mean post-test or follow-up score of the experimental group from the mean post-test or follow-up score of the control group, and dividing the difference by the pooled standard deviation [93]. These effect sizes are used to gain insight into the relevance of the significant effects. To examine changes in the amount of flourishers, languishers, and moderately mentally healthy (MHC-SF), descriptive statistics will be used. Changes in categories will be tested with X2-statistics.
Mediator and moderator analyses will be performed as described by Hayes [94,95]. Mediator analyses will be conducted to investigate which of the specific components of the intervention—positive emotion, use of strengths, optimism, self-compassion, resilience, and positive relations—contribute to its efficacy and mediate overall well-being. Moderator analyses will be conducted to examine which specific subgroups will improve most (or least) on well-being and flourishing from participation in one of the experimental groups. The independent variables of gender, educational level, life-events, personality traits, level of adherence to the intervention, and participation satisfaction will be entered as moderators in regression analyses.
A cost-effectiveness analysis will be conducted from a societal perspective. For each condition, the mean annual health care costs (MCQ), costs due to productivity losses (PCQ), and intervention costs will be calculated on an annual per capita basis for the reference year 2014. All costs will be expressed in Euro (€). The incremental cost-effectiveness ratio (ICER) will be calculated using a bootstrap approach. Then, a cost-effectiveness acceptability curve will demonstrate the probability of the cost-effectiveness of TL-E and TL-I compared to WL, for a range of willingness-to-pay (WTP) ceilings. All tests will be two-sided and will use alphas of 0.05. All data-analyses will be performed with SPSS version 21.0 or higher.
Results
The data collection will be completed in June 2015.
Discussion
This study will investigate the short- and long-term efficacy of a multicomponent PPI (ie, self-help book with tailored email support) on well-being and flourishing. Mediator and moderator analyses will be conducted to explore which theoretically relevant hedonic well-being and eudaimonic well-being components included in the self-help book appear to contribute to its efficacy, and who will benefit most from the intervention. The study will be conducted in The Netherlands in a sample with low or moderate levels of well-being without moderate or severe clinical symptomatology. The results from this study will contribute to the knowledge of evidence-based PPIs, in particular multicomponent PPIs, and will be valuable for public mental health services and governments who are increasingly interested in enhancing well-being in the general population [96,97].
There could be several limitations that need to be considered in advance. First, our results might not be generalizable to the general Dutch population, since we will use a self-selected sample and apply exclusion criteria on the level of well-being and clinical symptomatology. It is not unlikely that our open recruitment with advertisement in national newspapers will attract mostly highly-educated women. However, we will use a randomization procedure stratified by gender and education, which will create equal distribution of these characteristics to each group and therefore not harm the internal validity of our study. Second, non-adherence to the intervention and drop out from assessments (incomplete data) could occur. Both types of attrition are closely related and may bias our results [98]. Reasons for non-adherence and dropout could be related to individual characteristics (ie, low-educated individuals might find the intervention and/or assessments too difficult), characteristics of the intervention (ie, individuals in the experimental conditions receive the self-help book after baseline and are unaware of the content of the book and type of exercises when they apply for the study), and characteristics of the study (ie, participants will be given instructions and a time schedule) [98]. To gain insight on adherence in our study, participants will be asked about time spent on each module, and the personal counselors will gather reasons for non-adherence mentioned in the email correspondence. Although we expect to find higher adherence rates for individuals in the TL-E condition than has previously been found for Web-based multicomponent PPIs [24,25,27], it could be lower than in face-to-face multicomponent PPIs [20,22,23]. However, our study can only draw conclusions about the comparison of the self-help book with email support to the self-help book without email support. Differences in adherence and efficacy between face-to-face support, email support, and no support warrant attention in future research. Furthermore, to prevent low power due to drop out, we have taken into account an attrition rate of 25% in our power analysis. We will also conduct dropout analysis to identify any selectiveness or characteristics of attrition that may be relevant for real-life implementation of the intervention. Third, the use of senior positive psychology students for the email support can be a risk for the professionalism of our intervention because these students are unexperienced psychologists. We will try to reduce this risk by providing extensive supervision from experienced psychologists and by only selecting students who are thoroughly trained in email support and who have practiced the self-help book. On the other hand, the guidance is primarily process-oriented and advanced clinical counseling skills are therefore not considered necessary. The benefit of using students as counselors is that the intervention costs will be very low. If proven effective, it could be even more effective when implemented in a mental health service with experienced and professional counselors, although this could be disadvantageous for its cost-effectivity. Nevertheless, this needs to be tested in future research.
Our study will be the first to investigate the efficacy and working mechanisms of a theory- and research- based multicomponent PPI in the form of a self-help book with email support to enhance well-being and flourishing in the general population. Our study will add to the existing knowledge in that we (1) focus on well-being and flourishing instead of mental illness, (2) use a multicomponent intervention instead of a single-component intervention, (3), integrate some advantages of face-to-face multicomponent PPIs with web-based multicomponent PPIs by using a self-help book with asynchronous and tailored email support, (4) examine the intervention in a population with low or moderate levels of well-being without moderate or severe clinical symptomatology instead of a population with at least moderate clinical symptomatology without any criteria on the well-being dimension of the two-continua model of mental health, and (5) measure and analyze each specific well-being component that is included in the self-help book: positive emotion, use of strengths, optimism, self-compassion, resilience, and positive relations. Taken together, our results will contribute to a new field of multicomponent PPIs for enhancing well-being and flourishing in the general population and highlight a new target population for mental health promotion. If proven effective, our results can be specifically of interest for public mental health and primary care because these health care fields are expanding, while specialist mental health care is diminishing, at least in The Netherlands.
Abbreviations
- ANOVA
analysis of variance
- BRS
Brief Resilience Scale
- CONSORT
Consolidated Standards for Reporting Trials
- CSQ-8
Client Satisfaction Questionnaire-short form
- EM
expectation maximization
- EPQ-RSS
Eysenck Personality Questionnaire–Revised Short Scale
- FS
Flourishing Scale
- HADS
Hospital Anxiety and Depression Scale
- ICER
incremental cost-effectiveness ratio
- LOT-R
Life Orientation Test-Revised
- MCQ
Medical Consumption Questionnaire
- m-DES
modified Differential Emotions Scale
- MHC-SF
Mental Health Continuum-Short Form
- NEO-FFI
NEO Five Factor Inventory
- PCQ
Productivity Cost Questionnaire
- PERMA
positive emotion, engagement, relationships, meaning and accomplishment
- PPI
positive psychology intervention
- RCT
randomized controlled trial
- SCS-SF
Self-Compassion Scale-Short Form
- SPR
Subscale of Positive Relations
- SPSS
Statistical Package for the Social Sciences
- SUS
Strengths Use Scale
- TL
“This is your life”
- TL-E
“This is your life” with email support
- TL-I
“This is your life” with an information email
- WL
waiting list control condition
- WTP
willingness-to-pay
Footnotes
Conflicts of Interest: None declared.
References
- 1.Seligman MEP, Csikszentmihalyi M. Positive psychology. An introduction. Am Psychol. 2000 Jan;55(1):5–14. doi: 10.1037//0003-066x.55.1.5. [DOI] [PubMed] [Google Scholar]
- 2.Rusk RD, Waters LE. Tracing the size, reach, impact, and breadth of positive psychology. J Posit Psychol. 2013 May;8(3):207–221. doi: 10.1080/17439760.2013.777766. [DOI] [Google Scholar]
- 3.Kobau R, Seligman MEP, Peterson C, Diener E, Zack MM, Chapman D, Thompson W. Mental health promotion in public health: perspectives and strategies from positive psychology. Am J Public Health. 2011 Aug;101(8):e1–9. doi: 10.2105/AJPH.2010.300083.AJPH.2010.300083 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Keyes CLM. The mental health continuum: from languishing to flourishing in life. J Health Soc Behav. 2002 Jun;43(2):207–22. [PubMed] [Google Scholar]
- 5.Lamers SMA, Westerhof GJ, Bohlmeijer ET, ten Klooster PM, Keyes CLM. Evaluating the psychometric properties of the Mental Health Continuum-Short Form (MHC-SF) J Clin Psychol. 2011 Jan;67(1):99–110. doi: 10.1002/jclp.20741. [DOI] [PubMed] [Google Scholar]
- 6.Westerhof GJ, Keyes CLM. Mental Illness and Mental Health: The Two Continua Model Across the Lifespan. J Adult Dev. 2010 Jun;17(2):110–119. doi: 10.1007/s10804-009-9082-y. http://europepmc.org/abstract/MED/20502508 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Keyes CLM. Promoting and protecting mental health as flourishing: a complementary strategy for improving national mental health. Am Psychol. 2007;62(2):95–108. doi: 10.1037/0003-066X.62.2.95.2007-01685-003 [DOI] [PubMed] [Google Scholar]
- 8.Keyes CLM, Simoes EJ. To flourish or not: positive mental health and all-cause mortality. Am J Public Health. 2012 Nov;102(11):2164–72. doi: 10.2105/AJPH.2012.300918. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Huppert FA. Psychological well-being: Evidence regarding its causes and consequences. Appl Psychol Health Well Being. 2009;1(2):137–164. doi: 10.1111/j.1758-0854.2009.01008.x. [DOI] [Google Scholar]
- 10.Seligman MEP. Flourish: A New Understanding of Happiness, Well-Being - And How to Achieve Them. London: Nicholas Brealey Publishing; 2011. [Google Scholar]
- 11.Huppert FA, So TT. Flourishing Across Europe: Application of a New Conceptual Framework for Defining Well-Being. Soc Indic Res. 2013 Feb;110(3):837–861. doi: 10.1007/s11205-011-9966-7. http://europepmc.org/abstract/MED/23329863 .9966 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Keyes CLM, Dhingra SS, Simoes EJ. Change in level of positive mental health as a predictor of future risk of mental illness. Am J Public Health. 2010 Dec;100(12):2366–71. doi: 10.2105/AJPH.2010.192245.AJPH.2010.192245 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Keyes CLM, Wissing M, Potgieter JP, Temane M, Kruger A, van Rooy S. Evaluation of the mental health continuum-short form (MHC-SF) in setswana-speaking South Africans. Clin Psychol Psychother. 2008;15(3):181–92. doi: 10.1002/cpp.572. [DOI] [PubMed] [Google Scholar]
- 14.Schotanus-Dijkstra M, Pieterse ME, Drossaert CHC, Westerhof GJ, de Graaf R, ten Have M, Walburg JA, Bohlmeijer ET. What Factors are Associated with Flourishing? Results from a Large Representative National Sample. J Happiness Stud. 2015 Jun 11; doi: 10.1007/s10902-015-9647-3. [DOI] [Google Scholar]
- 15.Rose G, Khaw K, Marmot M. Rose's strategy of preventive medicine: the complete original text. Oxford: Oxford University Press; 2008. [Google Scholar]
- 16.Key Competence Happiness. [2014-12-19]. http://www.keycompetencehappiness.com/en .
- 17.Bolier L, Haverman M, Westerhof GJ, Riper H, Smit F, Bohlmeijer E. Positive psychology interventions: a meta-analysis of randomized controlled studies. BMC Public Health. 2013;13:119. doi: 10.1186/1471-2458-13-119. http://www.biomedcentral.com/1471-2458/13/119 .1471-2458-13-119 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Sin NL, Lyubomirsky S. Enhancing well-being and alleviating depressive symptoms with positive psychology interventions: a practice-friendly meta-analysis. J Clin Psychol. 2009 May;65(5):467–87. doi: 10.1002/jclp.20593. [DOI] [PubMed] [Google Scholar]
- 19.Ryff CD. Happiness is everything, or is it? Explorations on the meaning of psychological well-being. J Pers Soc Psychol. 1989;57(6):1069–1081. doi: 10.1037/0022-3514.57.6.1069. [DOI] [Google Scholar]
- 20.Rashid T. Positive psychotherapy: A strength-based approach. J Posit Psychol. 2014 Jun 09;10(1):25–40. doi: 10.1080/17439760.2014.920411. [DOI] [Google Scholar]
- 21.Seligman MEP, Rashid T, Parks AC. Positive psychotherapy. Am Psychol. 2006 Nov;61(8):774–88. doi: 10.1037/0003-066X.61.8.774.2006-21079-029 [DOI] [PubMed] [Google Scholar]
- 22.Fava GA, Tomba E. Increasing psychological well-being and resilience by psychotherapeutic methods. J Pers. 2009 Dec;77(6):1903–34. doi: 10.1111/j.1467-6494.2009.00604.x.JOPY604 [DOI] [PubMed] [Google Scholar]
- 23.Page KM, Vella-Brodrick DA. The Working for Wellness Program: RCT of an Employee Well-Being Intervention. J Happiness Stud. 2013 Jun 11;14(3):1007–1031. doi: 10.1007/s10902-012-9366-y. [DOI] [Google Scholar]
- 24.Schueller SM, Parks AC. Disseminating self-help: positive psychology exercises in an online trial. J Med Internet Res. 2012 Jun;14(3):e63. doi: 10.2196/jmir.1850. http://www.jmir.org/2012/3/e63/ v14i3e63 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Bolier L, Haverman M, Kramer J, Westerhof GJ, Riper H, Walburg JA, Boon B, Bohlmeijer E. An Internet-based intervention to promote mental fitness for mildly depressed adults: randomized controlled trial. J Med Internet Res. 2013;15(9):e200. doi: 10.2196/jmir.2603. http://www.jmir.org/2013/9/e200/ v15i9e200 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Bolier L, Majo C, Smit F, Westerhof GJ, Haverman M, Walburg JA, Riper H, Bohlmeijer E. Cost-effectiveness of online positive psychology: Randomized controlled trial. J Posit Psychol. 2014 Apr 23;9(5):460–471. doi: 10.1080/17439760.2014.910829. [DOI] [Google Scholar]
- 27.Mitchell J, Vella-Brodrick D, Klein B. Positive Psychology and the Internet: A Mental Health Opportunity. E J Appl Psychol. 2010 Dec 30;6(2) doi: 10.7790/ejap.v6i2.230. [DOI] [Google Scholar]
- 28.Riper H, Andersson G, Christensen H, Cuijpers P, Lange A, Eysenbach G. Theme issue on e-mental health: a growing field in internet research. J Med Internet Res. 2010;12(5):e74. doi: 10.2196/jmir.1713. http://www.jmir.org/2010/5/e74/ v12i5e74 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Cuijpers P. Bibliotherapy in unipolar depression: a meta-analysis. J Behav Ther Exp Psychiatry. 1997 Jun;28(2):139–47. doi: 10.1016/s0005-7916(97)00005-0.S0005-7916(97)00005-0 [DOI] [PubMed] [Google Scholar]
- 30.Gregory RJ, Canning SS, Lee TW, Wise JC. Cognitive Bibliotherapy for Depression: A Meta-Analysis. Prof Psychol Res Pr. 2004;35(3):275–280. doi: 10.1037/0735-7028.35.3.275. [DOI] [Google Scholar]
- 31.Apodaca TR, Miller WR. A meta-analysis of the effectiveness of bibliotherapy for alcohol problems. J Clin Psychol. 2003 Mar;59(3):289–304. doi: 10.1002/jclp.10130. [DOI] [PubMed] [Google Scholar]
- 32.Barak A, Klein B, Proudfoot JG. Defining internet-supported therapeutic interventions. Ann Behav Med. 2009 Aug;38(1):4–17. doi: 10.1007/s12160-009-9130-7. [DOI] [PubMed] [Google Scholar]
- 33.Cuijpers P, Donker T, van Straten A, Li J, Andersson G. Is guided self-help as effective as face-to-face psychotherapy for depression and anxiety disorders? A systematic review and meta-analysis of comparative outcome studies. Psychol Med. 2010 Dec;40(12):1943–57. doi: 10.1017/S0033291710000772.S0033291710000772 [DOI] [PubMed] [Google Scholar]
- 34.Carter W, Fergus K, Ahmad S, McLeod D, Stephen J. Defining the Role of the Online Therapeutic Facilitator: Principles and Guidelines Developed for Couplelinks, an Online Support Program for Couples Affected by Breast Cancer. JMIR Cancer. 2015 Apr 14;1(1):e4. doi: 10.2196/cancer.3887. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Fordyce MW. Development of a program to increase personal happiness. J Couns Psychol. 1977;24(6):511–521. doi: 10.1037/0022-0167.24.6.511. [DOI] [Google Scholar]
- 36.Fordyce MW. A program to increase happiness: Further studies. J Couns Psychol. 1983;30(4):483–498. doi: 10.1037/0022-0167.30.4.483. [DOI] [Google Scholar]
- 37.Parks AC, Szanto RK. Assessing the efficacy and effectiveness of a Positive Psychology-based self-help book. Ter Psicol. 2013 Apr;31(1):141–149. doi: 10.4067/S0718-48082013000100013. [DOI] [Google Scholar]
- 38.Fledderus M, Bohlmeijer ET, Pieterse ME, Schreurs KMG. Acceptance and commitment therapy as guided self-help for psychological distress and positive mental health: a randomized controlled trial. Psychol Med. 2012 Mar;42(3):485–95. doi: 10.1017/S0033291711001206.S0033291711001206 [DOI] [PubMed] [Google Scholar]
- 39.Lyubomirsky S. The How of Happiness: A Practical Guide to Getting The Life You Want. London: Piatkus Books; 2008. [Google Scholar]
- 40.Bohlmeijer E, Hulsbergen M. Dit is jouw leven. Ervaar de effecten van de positive psychologie (This is your life. Experience the effects of positive psychology) Amsterdam: Uitgeverij Boom; 2013. [Google Scholar]
- 41.Parks AC, Della Porta MD, Pierce RS, Zilca R, Lyubomirsky S. Pursuing happiness in everyday life: the characteristics and behaviors of online happiness seekers. Emotion. 2012 Dec;12(6):1222–34. doi: 10.1037/a0028587.2012-13960-001 [DOI] [PubMed] [Google Scholar]
- 42.Qualtrics software of the Qualtrics Research Suite, 2014. [2014-12-19]. Provo: UT http://www.qualtrics.com/
- 43.Keyes CLM. Mental health in adolescence: is America's youth flourishing? Am J Orthopsychiatry. 2006 Jul;76(3):395–402. doi: 10.1037/0002-9432.76.3.395.2006-11985-014 [DOI] [PubMed] [Google Scholar]
- 44.Zigmond AS, Snaith RP. The hospital anxiety and depression scale. Acta Psychiatr Scand. 1983 Jun;67(6):361–70. doi: 10.1111/j.1600-0447.1983.tb09716.x. [DOI] [PubMed] [Google Scholar]
- 45.Meevissen YMC, Peters ML, Alberts HJEM. Become more optimistic by imagining a best possible self: effects of a two week intervention. J Behav Ther Exp Psychiatry. 2011 Sep;42(3):371–8. doi: 10.1016/j.jbtep.2011.02.012.S0005-7916(11)00035-8 [DOI] [PubMed] [Google Scholar]
- 46.Peters ML, Flink IK, Boersma K, Linton SJ. Manipulating optimism: Can imagining a best possible self be used to increase positive future expectancies? J Posit Psychol. 2010 May;5(3):204–211. doi: 10.1080/17439761003790963. [DOI] [Google Scholar]
- 47.Peters ML, Meevissen YMC, Hanssen MM. Specificity of the Best Possible Self intervention for increasing optimism: Comparison with a gratitude intervention. Ter Psicol. 2013 Apr;31(1):93–100. doi: 10.4067/S0718-48082013000100009. [DOI] [Google Scholar]
- 48.Fredrickson BL. What Good Are Positive Emotions? Rev Gen Psychol. 1998 Sep;2(3):300–319. doi: 10.1037/1089-2680.2.3.300. http://europepmc.org/abstract/MED/21850154 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.Fredrickson BL. The role of positive emotions in positive psychology. The broaden-and-build theory of positive emotions. Am Psychol. 2001 Mar;56(3):218–26. doi: 10.1037//0003-066x.56.3.218. http://europepmc.org/abstract/MED/11315248 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50.Fredrickson B. Positivity. Oxford: Oneworld Publications; 2009. [Google Scholar]
- 51.Linley A, Willars J, Biswas-Diener R. The Strengths Book: Be Confident, Be Successful, and Enjoy Better Relationships by Realising the Best of You. Coventry: CAPP Press; 2010. [Google Scholar]
- 52.Linley PA, Harrington S. Strengths coaching: A potential-guided approach to coaching psychology. Int Coach Psychol Rev. 2006 Apr;1(1):37–46. [Google Scholar]
- 53.Csikszentmihalyi M. Flow: The Psychology of Optimal Experience. New York: Harper Perennial Modern Classics; 2001. [Google Scholar]
- 54.Carver CS, Scheier MF, Segerstrom SC. Optimism. Clin Psychol Rev. 2010 Nov;30(7):879–89. doi: 10.1016/j.cpr.2010.01.006. http://europepmc.org/abstract/MED/20170998 .S0272-7358(10)00019-X [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55.Scheier MF, Carver CS. Effects of optimism on psychological and physical well-being: Theoretical overview and empirical update. Cogn Ther Res. 1992 Apr;16(2):201–228. doi: 10.1007/BF01173489. [DOI] [Google Scholar]
- 56.Seligman MEP. Learned Optimism: How to Change Your Mind and Your Life. New York: Vintage; 2006. [Google Scholar]
- 57.Gilbert P. The Compassionate Mind. How to use compassion to develop happiness, self-acceptance and well-being. London: Constable; 2010. [Google Scholar]
- 58.Neff KD. Self-compassion: An alternative conceptualization of a healthy atitude toward oneself. Self Identity. 2003 Apr;2(2):85–102. doi: 10.1080/15298860390129863. [DOI] [Google Scholar]
- 59.Neff KD, Germer CK. A pilot study and randomized controlled trial of the mindful self-compassion program. J Clin Psychol. 2013 Jan;69(1):28–44. doi: 10.1002/jclp.21923. [DOI] [PubMed] [Google Scholar]
- 60.Joseph S. What doesn’t kill us. The new psychology of post-traumatic growth. London: Piatkus; 2011. [Google Scholar]
- 61.Joseph S, Linley PA. Growth following adversity: theoretical perspectives and implications for clinical practice. Clin Psychol Rev. 2006 Dec;26(8):1041–53. doi: 10.1016/j.cpr.2005.12.006.S0272-7358(05)00169-8 [DOI] [PubMed] [Google Scholar]
- 62.Tedeschi RG, Calhoun LG. Posttraumatic Growth: Conceptual Foundations and Empirical Evidence. Psychological Inquiry. 2004 Jan;15(1):1–18. doi: 10.1207/s15327965pli1501_01. [DOI] [Google Scholar]
- 63.Gable SL, Reis HT, Impett EA, Asher ER. What do you do when things go right? The intrapersonal and interpersonal benefits of sharing positive events. J Pers Soc Psychol. 2004 Aug;87(2):228–45. doi: 10.1037/0022-3514.87.2.228.2004-16828-005 [DOI] [PubMed] [Google Scholar]
- 64.Reis HT, Gable SL. Toward a positive psychology of relationships. In: Keyes CLM, Haidt J, editors. Flourishing: Positive psychology and the life well-lived. Washington: APA; 2003. pp. 129–160. [Google Scholar]
- 65.Reis HT, Smith SM, Carmichael CL, Caprariello PA, Tsai FF, Rodrigues A, Maniaci MR. Are you happy for me? How sharing positive events with others provides personal and interpersonal benefits. J Pers Soc Psychol. 2010 Aug;99(2):311–29. doi: 10.1037/a0018344.2010-14719-008 [DOI] [PubMed] [Google Scholar]
- 66.Rosenberg MB. Nonviolent Communication: A Language of Life: Create Your Life, Your Relationships, and Your World in Harmony with Your Values. Encinitas: Puddledancer Press; 2003. [Google Scholar]
- 67.Bloom W. The Power of Modern Spirituality. How to live a life of compassion and personal fulfillment. London: Piatkus; 2011. [Google Scholar]
- 68.Otake K, Shimai S, Tanaka-Matsumi J, Otsui K, Fredrickson BL. Happy people become happier through kindness: A counting kindnesses intervention. J Happiness Stud. 2006 Sep;7(3):361–375. doi: 10.1007/s10902-005-3650-z. http://europepmc.org/abstract/MED/17356687 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 69.Diener E, Wirtz D, Tov W, Kim-Prieto C, Choi D, Oishi S, Biswas-Diener R. New Well-being Measures: Short Scales to Assess Flourishing and Positive and Negative Feelings. Soc Indic Res. 2009 May 28;97(2):143–156. doi: 10.1007/s11205-009-9493-y. [DOI] [Google Scholar]
- 70.Bjelland I, Dahl AA, Haug TT, Neckelmann D. The validity of the Hospital Anxiety and Depression Scale. An updated literature review. J Psychosom Res. 2002 Feb;52(2):69–77. doi: 10.1016/s0022-3999(01)00296-3.S0022399901002963 [DOI] [PubMed] [Google Scholar]
- 71.Spinhoven PH, Ormel J, Sloekers PPA, Kempen GIJM, Speckens AE, Van Hemert AM. A validation study of the Hospital Anxiety and Depression Scale (HADS) in different groups of Dutch subjects. Psychol Med. 1997 Mar;27(2):363–70. doi: 10.1017/s0033291796004382. [DOI] [PubMed] [Google Scholar]
- 72.Schaefer A, Nils F, Sanchez X, Philippot P. Assessing the effectiveness of a large database of emotion-eliciting films: A new tool for emotion researchers. Cogn Emot. 2010 Nov;24(7):1153–1172. doi: 10.1080/02699930903274322. [DOI] [Google Scholar]
- 73.Govindji R, Linley PA. Strength use, self-concordance and well-being: Implications for strengths coaching and coaching psychologists. International Coaching Psychology Review. 2007;2(2):143–153. [Google Scholar]
- 74.Wood AM, Linley PA, Maltby J, Kashdan TB, Hurling R. Using personal and psychological strengths leads to increases in well-being over time: A longitudinal study and the development of the strengths use questionnaire. Pers Individ Dif. 2011 Jan;50(1):15–19. doi: 10.1016/j.paid.2010.08.004. [DOI] [Google Scholar]
- 75.Scheier MF, Carver CS, Bridges MW. Distinguishing optimism from neuroticism (and trait anxiety, self-mastery, and self-esteem): a reevaluation of the Life Orientation Test. J Pers Soc Psychol. 1994 Dec;67(6):1063–78. doi: 10.1037//0022-3514.67.6.1063. [DOI] [PubMed] [Google Scholar]
- 76.Ten Klooster PM, Weekers AM, Eggelmeijer F, van Woerkom JM, Drossaert CHC, Taal E, Rasker JJ, Baneke JJ. Optimisme en/of pessimisme: factorstructuur van de Nederlandse Life Orientation Test-Revised. PSEG. 2010 Jun;38(2):89–100. doi: 10.1007/BF03089356. [DOI] [Google Scholar]
- 77.Raes F, Pommier E, Neff KD, Van Gucht D. Construction and factorial validation of a short form of the Self-Compassion Scale. Clin Psychol Psychother. 2011 Jun;18(3):250–5. doi: 10.1002/cpp.702. [DOI] [PubMed] [Google Scholar]
- 78.Neff KD. The development and validation of a scale to measure self-compassion. Self Identity. 2003 Jul;2(3):223–250. doi: 10.1080/15298860390209035. [DOI] [Google Scholar]
- 79.Smith BW, Dalen J, Wiggins K, Tooley E, Christopher P, Bernard J. The brief resilience scale: assessing the ability to bounce back. Int J Behav Med. 2008;15(3):194–200. doi: 10.1080/10705500802222972.901471909 [DOI] [PubMed] [Google Scholar]
- 80.Van Dierendonck D. Handleiding Positieve Geestelijke Gezondheids Schaal (PGGS). Versie 0.5 (Manual Positive Mental Health Scale, version 0.5) Amsterdam: Universiteit van Amsterdam; 2011. [Google Scholar]
- 81.Eysenck SBG, Eysenck HJ, Barrett P. A revised version of the psychoticism scale. Pers Individ Dif. 1985 Jan;6(1):21–29. doi: 10.1016/0191-8869(85)90026-1. [DOI] [Google Scholar]
- 82.Eysenck SBG, White O, Eysenck HJ. Personality and mental illness. Psychol Rep. 1976 Dec;39(3):1011–22. doi: 10.2466/pr0.1976.39.3.1011. [DOI] [PubMed] [Google Scholar]
- 83.Sanderman R, Arrindell WA, Ranchor AV, Eysenck HJ, Eysenck SBG. Het meten van persoonlijkheidskenmerken met de Eysenck Personality Questionnaire (EPQ) (Measuring personality traits with the Eysenck Personality Questionnaire) Groningen: Noordelijk Centrum voor Gezondheidsvraagstukken (RUG); 1995. [Google Scholar]
- 84.Costa PT, McCrae RR. Revised NEO Personality Inventory (NEO-PI-R) and the Five Factor Inventory (NEO-FFI). Professional Manual. Odessa, Florida: Psychological Assessment Resources Inc; 1992. [Google Scholar]
- 85.Bouwmans C, Hakkaart-van Roijen L, Koopmanschap M, Krol M, Severens H, Brouwer W. Medical Consumption Questionnaire. Productivity and Health Research Group. Rotterdam: Institute for Medical Technology Assessment, Erasmus Universiteit Rotterdam; 2013. [Google Scholar]
- 86.Bouwmans C, Hakkaart-van Roijen L, Koopmanschap M, Krol M, Severens H, Brouwer W. Productivity Cost Questionnaire. Productivity and Health Research Group. Rotterdam: Institute for Medical Technology Assessment, Erasmus Universiteit Rotterdam; 2013. [Google Scholar]
- 87.Brugha T, Bebbington P, Tennant C, Hurry J. The List of Threatening Experiences: a subset of 12 life event categories with considerable long-term contextual threat. Psychol Med. 1985 Feb;15(1):189–94. doi: 10.1017/s003329170002105x. [DOI] [PubMed] [Google Scholar]
- 88.Attkisson CC, Zwick R. The client satisfaction questionnaire. Psychometric properties and correlations with service utilization and psychotherapy outcome. Eval Program Plann. 1982;5(3):233–7. doi: 10.1016/0149-7189(82)90074-x. [DOI] [PubMed] [Google Scholar]
- 89.De Brey H. A cross-national validation of the client satisfaction questionnaire: the Dutch experience. Eval Program Plann. 1983;6(3-4):395–400. doi: 10.1016/0149-7189(83)90018-6. [DOI] [PubMed] [Google Scholar]
- 90.Client Change Interview Protocol. [2014-12-19]. http://experiential-researchers.org/instruments/elliott/changei.html .
- 91.Moher D, Hopewell S, Schulz KF, Montori V, Gøtzsche PC, Devereaux PJ, Elbourne D, Egger M, Altman DG. CONSORT 2010 explanation and elaboration: updated guidelines for reporting parallel group randomised trials. BMJ. 2010 Mar;340:c869. doi: 10.1136/bmj.c869. http://europepmc.org/abstract/MED/20332511 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 92.Dempster AP, Laird NM, Rubin DB. Maximum Likelihood from Incomplete Data via the EM Algorithm. J R Stat Soc Series B Stat Methodol (Suppl 1) 1977;39:1–38. doi: 10.2307/2984875. [DOI] [Google Scholar]
- 93.Cohen J. Statistical power analysis for the behavioral sciences. Hillsdale: Erlbaum; 1988. [Google Scholar]
- 94.Hayes AF. Beyond Baron and Kenny: Statistical Mediation Analysis in the New Millennium. Communication Monographs. 2009 Dec;76(4):408–420. doi: 10.1080/03637750903310360. [DOI] [Google Scholar]
- 95.Hayes AF PROCESS: A versatile computational tool for observed variable mediation, moderation, and conditional process modeling. [2014-12-19]. http://www.afhayes.com/public/process2012.pdf .
- 96.Foresight Mental Capital and Wellbeing Project . Final project report - Executive summary. London: The Government Office for Science; 2008. [Google Scholar]
- 97.Van Campen C, Bergsma A, Boelhouwer J, Boerefijn J, Bolier L. Sturen op geluk. Geluksbevordering door nationale overheden, gemeenten en publieke instellingen (Send happiness. Promoting happiness by national governments, municipalities and public services) Den Haag: Sociaal en Cultureel Planbureau; 2012. [Google Scholar]
- 98.Eysenbach G. The law of attrition. J Med Internet Res. 2005;7(1):e11. doi: 10.2196/jmir.7.1.e11. http://www.jmir.org/2005/1/e11/ v7e11 [DOI] [PMC free article] [PubMed] [Google Scholar]