

Abstract
The present study examined pausing patterns in spontaneous speech as a measure of the effect of deep brain stimulation (DBS) of the subthalamic nucleus (STN) on parkinsonian speech. Pauses reflect various aspects of speech and language processes, including motor initiation and linguistic planning. Relatively little attention has been given to pauses in determining the effect of STN-DBS. An examination of pausing may be helpful to understanding how this form of therapy affects these behaviors. Seven individuals with Parkinson’s disease who received surgery for bilateral STN-DBS participated. Spontaneous speech samples were elicited in both the ON and OFF STN-DBS condition. Findings indicated that long pauses (250–3000 ms) in spontaneous speech were significantly shorter and more frequent in the STN-DBS ON condition. Furthermore, the proportion of nonlinguistic boundary pauses was significantly greater with stimulation. The findings support previous studies suggesting that speech motor control and lexical retrieval may be affected by STN-DBS.
Keywords: deep brain stimulation (DBS), subthalamic nucleus (STN), parkinsonian speech, pauses
Introduction
Despite numerous studies demonstrating the beneficial effects of high frequency electrical deep brain stimulation (DBS) of the subthalamic nucleus (STN) on limb movements (Krystkowiak et al., 2003; Kumar et al., 1998; Limousin et al., 1995), the impact of STN-DBS on speech production is still controversial (Gentil et al., 2000; Gentil et al., 2003; Gentil, Chauvin, Pinto, Pollak, & Benabid, 2001; Gentil, Garcia-Ruiz, Pollak, & Benabid, 1999; Krack et al. 2003; Romito et al., 2002; Romito et al., 2003) and even less is known about its effect on language. Several studies reported that STN-DBS improved dynamic and static movements of articulatory organs as well as phonatory and laryngeal function (Gentil et al., 1999; Gentil et al., 2000; Gentil et al, 2001; Gentil et al., 2003; Pinto, Gentil, Fraix, Benabid, & Pollak, 2003; Sidtis et al., 2010). However, other studies provided evidence that STN-DBS has an adverse effect on speech function, reporting dysarthria as one of the most common side effect of STN-DBS (Krack et al. 2003; Romito et al. 2002; Romito et al. 2003). As for its effect on language, only a few studies have conducted comprehensive and detailed research regarding this topic, which have yielded conflicting results (Whelan et al., 2003; Zanini et al., 2003).
Most studies examining the effect of STN-DBS in PD have focused on prosodic components including pitch, rate, and syllable duration, as parkinsonian speech is often disordered at the suprasegmental level. Pausing is one of the suprasegmental components that characterize parkinsonian speech. Some studies have found that individuals with PD produced more pauses than normal controls (Hammen, Yorkston, & Becukelman, 1989; Torp & Hammen, 2000), other studies have revealed that fewer pauses were produced in individuals with PD than normal controls (Skodda & Schlegel, 2005), and still others found large individual differences (Metter & Hanson, 1986). The inconsistent results may be attributed to small sample sizes, a range of disease severity, the different speech tasks used, and/or variations in the definition of pause.
Pauses are defined as “periods of silence” (O’Connell & Kowal, 1983, p. 221). Some studies have used the term “empty pause” or “silent pause” to be distinguished from the term filled pauses. Filled pauses refer to vocal hesitations such as “uh” or “um,” which are different from the pauses that are the focus of this study.1
Pauses are known to reflect various levels of speech-language processes. A certain group of pauses has been associated with motor speech processes. For example, speaker with motor speech planning difficulties may produce abnormal pauses within sounds, syllables, or words (Duffy, 2005; Ogar, Slama, Dronkers, Amici, & Gorno-Tempini, 2005). Other pauses are likely to serve a linguistic function. For instance, speakers may pause to search for a lexical item, or to plan for a linguistic unit, such as a phrase or sentence (Ferreira, 1991; Goldman-Eisler, 1961, 1972; Krauss, 1998; Niemi & Koivuselka-Sallinen, 1987; Zeches & Yorkston, 1995).
As individuals with PD show motor speech (Coates & Bakheit, 1997; Duffy, 2005; Hartelius & Svensson, 1994) and/or linguistic disturbances (Auriacombe et al., 1993; Grossman, 1999; Signorini & Volpato, 2006), pauses may provide a useful tool to understand their deficits. For example, abnormal pausing patterns in PD may reflect difficulty in starting and stopping speech movements, one of the motor functions of the basal ganglia (BG). The BG are crucial for movement control, especially in the initiation, monitoring, and termination of voluntary movement gestures (Graybiel, 1990; Jin & Costa, 2010; Banichi & Compton, 2011). Pause data in this population may be helpful in clarifying the role of the BG in the control of speech movements. Furthermore, pauses may signal subtle motor speech or linguistic changes due to STN-DBS, which might have been ignored in previous studies focused on examining segments and other suprasegmental features.
With these considerations in mind, we are currently conducting a study that aims to examine the effect of STN-DBS on pausing in Parkinsonian speech, examining a range of speech tasks. This paper reports results from this study, focusing on pausing patterns in spontaneous speech.
Methods
Participants
The participants were seven right-handed male subjects with idiopathic PD who had electrodes implanted in the STN bilaterally. The indications for STN-DBS therapy were advanced, medically refractory PD with marked clinical swings between medication doses (i.e., ON/OFF effects) as well as levodopa-induced dyskinesias. Speech evaluations in either the ON and OFF STN-DBS condition were performed at least 12 hrs following the last dose of levodopa, which was taken the evening before the study. ON and OFF studies were performed on different days separated by at least one week. The stimulation frequency was 185 Hz and the pulse width was 60 µs in all cases. None of the subjects had confounding neurologic, psychiatric, or medical disorders. The participants, all of whom had been clinically evaluated by a speech-language pathologist, showed mild hypokinetic dysarthria. In another study using speech samples obtained from these subjects, the mean intelligibility accuracy obtained from listeners’ ratings was over 90% (Sidtis et al., under review). All subjects provided informed consent to participate in the protocol approved by the institutional review board at the Nathan Kline Institute (Table 1).
TABLE 1.
Clinical and Demographic Characteristics of the STN-DBS Participants
| ID | Age (yr) |
Education (yr) |
PD (yr) |
DBS (mo) |
Levodopa (mg/day) |
UPDRSIII OFF |
UPDRS III ON |
|---|---|---|---|---|---|---|---|
| 103 | 54 | 14 | 14 | 44 | 250 | 51.0 | 25.0 |
| 104 | 57 | 16 | 16 | 27 | 400 | 57.0 | 55.5 |
| 106 | 59 | 15 | 10 | 09 | 600 | 27.5 | 19.0 |
| 107 | 62 | 18 | 15 | 02 | 600 | 26.0 | 23.0 |
| 109 | 49 | 16 | 09 | 04 | 300 | 23.5 | 21.5 |
| 110 | 62 | 11 | 11 | 56 | 600 | 52.5 | 31.0 |
| 111 | 56 | 11 | 11 | 37 | 400 | 11.5 | 4.0 |
| Mean | 57 | 14.4 | 12.3 | 25.6 | 450 | 35.6 | 25.6 |
All subjects were right-handed males and all but one subject were native speakers of English (106 was a native speaker of Italian who immigrated to the US as an adolescent). Age, education, and the duration of PD (PD) are in years. The duration of STN-DBS (DBS) is in months. Levodopa refers to the daily dose in mg. The Unified Parkinson’s Disease Rating Scale III (motor ratings) (UPDRS; Fahn et al., 1987) are off-medication and with STN-DBS on and off. Subject 104 had maximum scores on the rigidity items on the UPDRS III, which were not responsive to STN-DBS.
Procedure
Data Collection
Spontaneous speech samples were collected from the participants using a discourse task. The discourse task included a monologue of the speaker talking about his/her job, hobby, and/or family for 60 seconds. The task was performed both in the STN-DBS ON and in the OFF conditions. Speech samples were recorded using a Marantz digital recorder (PMD660) with an Audio-technica cardioid microphone (AT3035). Four of the STN-DBS subjects were tested in the STN-DBS OFF condition first. The two conditions are typically evaluated one week apart. The OFF condition was tested at least 2 hours after turning off the stimulators. For both the STN-DBS ON and OFF evaluations, subjects were tested at least 12 hours after their last dose of levodopa.
Data Analysis
Identification of Pauses
Acoustic analysis was performed using PRAAT version 5.0.46 (Boersma & Weenink, 2009). Pauses were identified by a period of silence during speech production in the acoustic waveform. Figure 1 presents an example of a pause identified on an acoustic waveform using PRAAT. To be considered as a pause in the spontaneous speech samples, the silence has to be greater than 100 ms, and the maximum duration of silence to be considered as a pause was 3000 ms.
Figure 1.
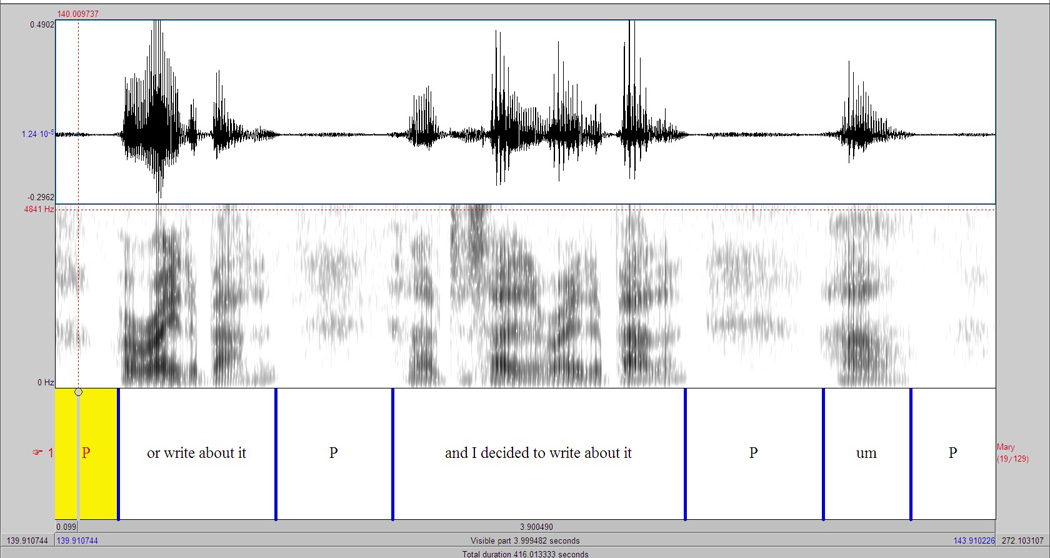
An example of identification of a pause using PRAAT. The top row indicates acoustic waveform, the second row shows a spectrogram, and the bottom row presents the transcription of the speech sample, where “P” indicates a pause.
Identified pauses were categorized as short (100–250 msec) and long pauses (250–-3000 msec). This was based on the observation that pauses tend to be functionally different with respect to their length: Short pauses are more likely to serve motor function and long pauses are more likely to serve linguistic functions (Green et al., 2004). The most commonly accepted criterion to distinguish motoric from cognitive-linguistic pauses is 250 ms (Boomer, 1965; Goldman-Eisler, 1968; Guo et al., 2008; Hieke et al., 1983; Oliveira, 2000; Thurber & Tager-Flusberg, 1993). This criterion was also supported by our pause duration data indicating bimodal distribution in speech samples, with bifurcation occurring around 250 msec (Figure 2). The selection of 3000 msec as a maximum cutoff point was meant to exclude phenomena other than pauses (e.g., blocks). In the present paper, the findings from long pauses are reported.
Figure 2.
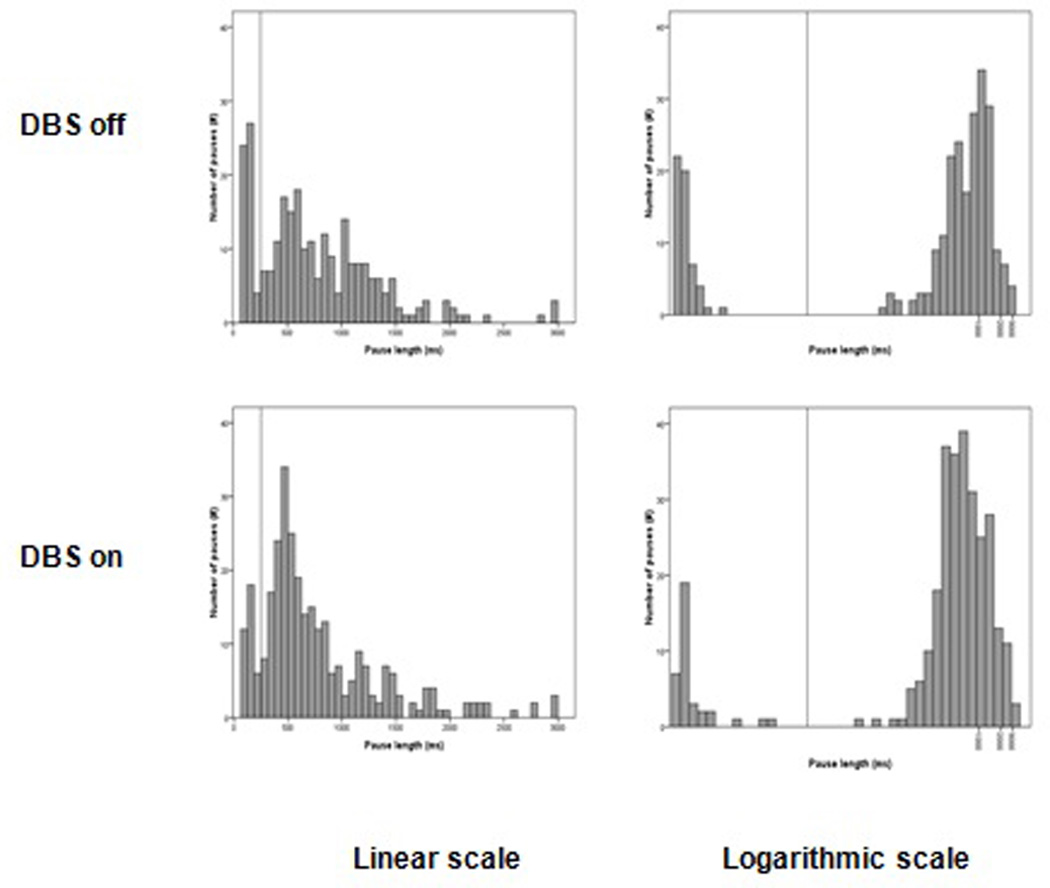
Distribution of pause length in discourse samples of PD STN-DBS participants during STN-DBS OFF and ON condition. To clearly view the distribution, charts were depicted in linear (left column) and logarithmic scale (right column). Vertical line in each chart indicates 250ms, where the bifurcation of distribution occurs.
Pauses were analyzed in terms of duration and frequency. Additionally, long pauses were measured with respect to their location within speech samples. As long pauses were considered to reflect linguistic processes, it was assumed that location of these pauses would occur at the boundaries of linguistic units. Therefore, long pauses were categorized as boundary and nonboundary pauses, reflecting pauses placed at the linguistic boundary or not located at linguistic boundary, respectively (Table 2).
TABLE 2.
Details of Boundary and Nonboundary Pauses within Discourse Samples
| Location | Subcategory | Description |
|---|---|---|
| Boundary pauses | Main clause | Pauses located before sentences that can stand alone including simple sentences (e.g.,/I have a daughter), coordinate clauses (e.g., I have a daughter/and my sister has a son), and subject-implied coordinate clauses (e.g., I have a daughter/and a son). |
| Subordinate clause | Pauses located before sentences that cannot stand by itself including adjective, adverbial, and noun clauses (e.g., She called me/when I was at work.) | |
| Prepositional phrase | Pauses located before prepositional phrases (e.g., We had a woman/from a state agency.) | |
| Infinitive/participial Phrase | Pauses located before participial (e.g., I started/making conversation) or infinitive phrases (e.g., I went there/to look around.) | |
| Fragment | Pauses located before a word or word string failed to be included in above mentioned syntactic boundaries, but acting like a independent phrase, or a sentence (e.g.,/Yes). | |
| Filled pauses located at boundary location | Pauses located before filled pauses followed by above mentioned syntactic boundaries (e.g., She called me/um when I was at work.). | |
| Nonboundary pauses | Lexical | Pauses located before content words including nouns, verbs, adjectives, and adverbs (e.g., I/transfer them to DVD). |
| Repetition | Pauses located before syllable, word, or phrase repetitions (e.g., I took group to/to to to to Europe) | |
| Revision | Pause located before word or phrase revision (e.g., My younger brother works at uh retail/retailing). | |
| Block/prolongation | Pauses located before block or prolongation. | |
| Within unit | Pauses located before within a unit that does not apply to any of above-mentioned nonboundary categories (e.g., I transfer/them to DVD) | |
| Filled pauses located at nonboundary location | Pauses located before filled pauses followed by above mentioned nonsyntactic boundaries (e.g. I also like/uh astronomy in general) |
In the discourse samples, long pauses located at syntactic boundaries were called boundary pauses. Boundary pauses included ones located before main clauses, subordinate clauses, prepositional phrases, infinitive/participial phrases, and sentence fragments (Crystal, 2003; Zeches & Yorkston, 1995). Pauses placed within these clauses and phrases were considered as nonboundary pauses. Nonboundary pauses were subcategorized into lexical, repetition, revision, block/prolongation, and within unit.
In addition, silent pauses placed before filled pauses (uh, um) were categorized as boundary or nonboundary pauses depending on the location of the filled pause. Similar to silent pauses, which were the focus of the present study, filled pauses have been observed to mark the boundaries of linguistic units and also been shown to co-occur with silent pauses (Swerts et al., 1996). Thus, in the present study, silent pauses placed before filled pauses, which were located before above-mentioned syntactic boundaries, were considered as boundary pauses. Likewise, silent pauses occurring before filled pauses appearing before above-mentioned nonboundaries were considered as nonboundary pauses. Details of the subcategorization of boundary and nonboundary pauses were presented in Table 2.
The number of boundary and nonboundary pauses for each speech sample was counted. The percentages of nonboundary pauses out of total number of pauses, possible number of nonboundaries, and total words were calculated.
Statistical Analysis
Pairwise t-tests were conducted to examine the difference between STN-DBS conditions (ON and OFF). In the present study, an alpha level of 0.05 was adopted to determine statistical significance.
Results
A pairwise t-test revealed that there was a significant difference in mean duration of long pauses between the STN-DBS OFF and ON conditions [t(206) = 7.719; p < 0.001]. The mean duration of long pauses was significantly shorter in the STN-DBS ON (M = 742.2, SD = 427.5) than in the STN-DBS OFF condition (M = 919.9, SD = 514). There was also a significant difference in the number of long pauses between STN-DBS conditions [t(6) = −3.2333; p = 0.018]. A greater number of pauses was found in the STN-DBS ON (M = 37.1, SD = 18.3) than in the STN-DBS OFF condition (M = 29.7, SD = 13.9).
The location of long pauses was also found to be affected by stimulation. Percentages of nonboundary pauses compared to the total number pauses [t(6) = −3.001; p = 0.024], to total number of possible nonboundary locations [t(6) = −3.655; p = 0.011], and to total words [t(6) = −3.739; p = 0.010] were all greater in STN-DBS ON than in STN-DBS OFF condition (Figure 3)
Figure 3.

Percentage of non-boundary pauses in the STN-DBS On and OFF conditions as a function of total number of pauses, possible non-boundary locations, and words.
Discussion
This paper reports results of a study examining the effect of STN-DBS on pausing in parkinsonian speech in spontaneous speech. Long pauses, defined as silent intervals longer than 250 ms, were analyzed in spontaneous speech samples obtained from individuals with PD in STN-DBS ON and OFF conditions. The findings revealed that long pauses were significantly shorter in STN-DBS ON, but occurred more frequently in STN-DBS ON compared to the OFF condition. Long pauses were also significantly more often placed in nonlinguistic boundary locations.
These results are all consistent with a model of the BG’s role in motor program initiation, monitoring and termination (Banichi & Compton, 2011; Graybiel, 1990; Jin & Costa, 2010). The findings that long pauses are shorter, more frequent, and more randomly placed with respect to linguistic structure in the STN-DBS ON condition suggest that the stimulation in the STN alters the execution pattern of the motor program. It is unclear whether this change is detrimental or beneficial to speech fluency. If we assume that the observed pattern of pauses is a result of stimulation adversely affecting initiation of speech movements, our results appear to be in accordance with the previous study which reported a case of an individual with PD who developed speech initiation difficulties after STN-DBS implantation (Moretti et al., 2003).
In a different vein, the increased number of nonlinguistic boundary pauses in STN-DBS ON condition also may suggest disruption of lexical retrieval. Long pauses located within linguistic units (i.e., in nonlinguistic boundaries) are thought to reflect lexical retrieval processes (Krauss, 1998; Zeches & Yorkston, 1995). Our findings may suggest that stimulation in the STN-DBS subjects may be adversely affecting the lexical retrieval process, which would be consistent with the findings showing reduced verbal fluency in the STN-DBS ON condition (Alegret et al., 2001; De Gaspari et al. 2006; Dujardin, Defebvre, Krystkowiak, Blond, & Destée, 2001). At this point, caution is required on this point and additional work needs to be done on possible subtypes of nonboundary pauses as well as on different speech production modes.
These finding—more pauses, shorter pauses, pausing more broadly distributed in the discourse—are compatible with each other. As previously noted, long pauses are likely to serve linguistic functions (Green et al., 2004). That is, speakers pause to retrieve a word or plan a linguistic unit, such as phrases or sentences (Harley, 2001). Long pauses that are placed within linguistic units, that is, in nonlinguistic boundaries, have been considered as reflecting lexical retrieval and/or failure to plan a linguistic unit (Krauss, 1998; Zeches & Yorkston, 1995). The increased number of long pauses may reflect difficulty in lexical retrieval and/or linguistic planning, but further analysis of long and short pauses is necessary to establish the relative effects of STN-DBS on motor and linguistic planning and on lexical retrieval.
In conclusion, in this study STN-DBS had a significant effect on duration, frequency, and location of long pauses in the spontaneous speech of Parkinson subjects. These findings provide support for the impact of STN-DBS on motor speech control, reflecting operations of speech initiation and may well reflect a role in “higher order” processes of lexical retrieval and linguistic planning.
Acknowledgments
This work was supported by NIH R01 DC 007658, the Parkinson’s Disease Foundation, and the Bachmann-Strauss Foundation.
Footnotes
In the present study, the term “pause” will refer mainly “silent pause.” The term “filled pause” will be used when there is a need to differentiate between “silent pauses” and “filled pauses.”
Contributor Information
Ji Sook Ahn, Department of Communicative Sciences and Disorders, New York University, New York, NY Brain and Behavior Laboratory, Geriatrics Division, Nathan Kline Institute for Psychiatric Research, Orangeburg, NY.
Diana Van Lancker Sidtis, Department of Communicative Sciences and Disorders, New York University, New York, NY
John J. Sidtis, Brain and Behavior Laboratory, Geriatrics Division, Nathan Kline Institute for Psychiatric Research, Orangeburg, NY Department of Psychiatry, New York University School of Medicine, New York, NY.
References
- Alegret M, Junque C, Valldeoriola F, Vendrell P, Pilleri M, Rumia J, Tolosa E. Effects of bilateral subthalamic stimulation on cognitive function in Parkinson disease. Archives of Neurology. 2001;58:1223–1227. doi: 10.1001/archneur.58.8.1223. [DOI] [PubMed] [Google Scholar]
- Auriacombe S, Grossman M, Carvell S, Gollomp S, Stern MB, Hurtig HI. Verbal fluency deficits in Parkinson’s disease. Neuropsychology. 1993;7:182–192. [Google Scholar]
- Banichi MT, Compton RJ. Cognitive neuroscience. Belmont, CA: Wadsworth; 2011. [Google Scholar]
- Boersma P, Wenink D. Praat: Doing phonetics by computer [Computer program] [Retrieved January 7, 2009];Version 5.0.46. 2009 from http://www.praat.org/ [Google Scholar]
- Boomer DS. Hesitation and grammatical encoding. Language and Speech. 1965;8:148–158. doi: 10.1177/002383096500800302. [DOI] [PubMed] [Google Scholar]
- Coates C, Bakheit AM. The prevalence of verbal communication disability in patients with Parkinson’s disease. Disability and Rehabilitation. 1997;19:104–107. doi: 10.3109/09638289709166834. [DOI] [PubMed] [Google Scholar]
- Crystal D. The Cambridge encyclopedia of the English language. Cambridge, MA: Cambridge University Press; 2003. [Google Scholar]
- De Gaspari D, Siri C, Di Gioia M, Antonini A, Isella V, Pizzolato A, Pezzoli G. Clinical correlates and cognitive underpinnings of verbal fluency impairment after chronic subthalamic stimulation in Parkinson’s disease. Parkinsonism and Related Disorders. 2006;12:289–295. doi: 10.1016/j.parkreldis.2006.01.001. [DOI] [PubMed] [Google Scholar]
- Duffy J. Motor speech disorders: Substrates, differential diagnosis, and management. St. Louis, MO: Mosby; 2005. [Google Scholar]
- Dujardin K, Defebvre L, Krystkowiak P, Blond S, Destée A. Influence of chronic bilateral stimulation of the subthalamic nucleus on cognitive function in Parkinson’s disease. Journal of Neurology. 2001;248:603–611. doi: 10.1007/s004150170139. [DOI] [PubMed] [Google Scholar]
- Fahn S, Elton RL. Members of the UPDRS development committee. Unified Parkinson Rating Scale. In: Fahn S, Marsden CD, Calne DB, Goldstein M, editors. Recent Developments in Parkinson’s Disease. Vol. 2. New York: Macmillan Publishing; 1987. pp. 153–163. [Google Scholar]
- Ferreira F. Effects of length and syntactic complexity on initiation times for prepared utterances. Journal of Memory and Language. 1991;30:210–233. [Google Scholar]
- Gentil M, Chauvin P, Pinto S, Pollak P, Benabid AL. Effect of bilateral stimulation of the subthalamic nucleus on parkinsonian voice. Brain and Language. 2001;78:233–240. doi: 10.1006/brln.2001.2466. [DOI] [PubMed] [Google Scholar]
- Gentil M, Garcia-Ruiz P, Pollak P, Benabid AL. Effect of stimulation of the subthalamicnucleus on oral control of patients with parkinsonism. Journal of Neurology, Neurosurgery and Psychiatry. 1999;67:329–333. doi: 10.1136/jnnp.67.3.329. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gentil M, Garcia-Ruiz P, Pollak P, Benabid AL. Effect of bilateral deep-brain stimulation on oral control of patients with parkinsonism. European Neurology. 2000;44:147–152. doi: 10.1159/000008224. [DOI] [PubMed] [Google Scholar]
- Gentil M, Pinto S, Pollak P, Benabid AL. Effect of bilateral stimulation of the subthalamic nucleus on parkinsonian dysarthria. Brain and Language. 2003;85:190–196. doi: 10.1016/s0093-934x(02)00590-4. [DOI] [PubMed] [Google Scholar]
- Goldman-Eisler F. The distribution of pause duration in speech. Language and Speech. 1961;4:232–237. [Google Scholar]
- Goldman-Eisler F. Psycholinguistic: Experiments in spontaneous speech. London, New York: Academic Press; 1968. [Google Scholar]
- Goldman-Eisler F. Pauses, clauses, sentences. Language and Speech. 1972;15:103–113. doi: 10.1177/002383097201500201. [DOI] [PubMed] [Google Scholar]
- Graybiel AM. The basal ganglia and the initiation of movement. Revue neurologique. 1990;146:570–574. [PubMed] [Google Scholar]
- Green JR, Beukelman DR, Ball LJ. Algorithmic estimation of pauses in extended speech samples of dysarthric and typical speech. Journal of Medical Speech-Language Pathology. 2004;12:149–154. [PMC free article] [PubMed] [Google Scholar]
- Grossman M. Sentence processing in Parkinson’s disease. Brain and Cognition. 1999;40:387–413. doi: 10.1006/brcg.1999.1087. [DOI] [PubMed] [Google Scholar]
- Guo L, Tomblin JB, Samelson V. Speech disruptions in the narratives of—speaking children with specific language impairment. Journal of Speech Language and Hearing Research. 2008;51:722–738. doi: 10.1044/1092-4388(2008/051). [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hammen V, Yorkston K, Beukelman D. Pausal and speech duration characteristics as a function of speaking rate in normal and dysarthric individuals. In: Yorkston KM, Beukelman DR, editors. Recent advances in clinical dysarthria. Austin, TX: Pro-Ed; 1989. [Google Scholar]
- Harley T. The psychology of language: From data to theory. New York, NY: Taylor & Francis; 2001. [Google Scholar]
- Hartelius L, Svensson P. Speech and swallowing symptoms associated with Parkinson’s disease and multiple-sclerosis—a survey. Folia Phoniatrica et Logopaedica. 1994;46:9–17. doi: 10.1159/000266286. [DOI] [PubMed] [Google Scholar]
- Hieke AE, Kowal S, O'Connell DC. The trouble with “articulatory pauses". Language and Speech. 1983;26:203–214. [Google Scholar]
- Jin X, Costa RM. Start/stop emerge in nigrostriatal circuits during sequence learning. Nature. 2010;466:457–462. doi: 10.1038/nature09263. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Krauss RM. Why do we gesture when we speak? Current Directions in Psychological Science. 1998;7:54–59. [Google Scholar]
- Krack P, Batir A, Van Blercom N, Chabardes S, Fraix V, Ardouin C, Pollak P. Five-year follow-up of bilateral stimulation of the subthalamic nucleus in advanced Parkinson’s disease. New England Journal of Medicine. 2003;349:1925–1934. doi: 10.1056/NEJMoa035275. [DOI] [PubMed] [Google Scholar]
- Krystkowiak P, Blatt JL, Bourriez JL, Duhamel A, Perina M, Blond S, Defebvre L. Effects of subthalamic nucleus stimulation and levodopa treatment on gait abnormalities in Parkinson. Archives of Neurology. 2003;60:80–84. doi: 10.1001/archneur.60.1.80. [DOI] [PubMed] [Google Scholar]
- Kumar R, Lozano AM, Kim YJ, Hutchison WD, Sime E, Halket E, Lang E. Double-blind evaluation of subthalamic nucleus deep brain stimulation in advanced Parkinson’s disease. Neurology. 1998;51:850–855. doi: 10.1212/wnl.51.3.850. [DOI] [PubMed] [Google Scholar]
- Limousin P, Pollak P, Benazzouz A, Hoffmann D, Le Bas JF, Broussolle E, Perret JE, Benabid AL. Effect on parkinsonian signs and symptoms of bilateral subthalamic nucleus stimulation. Lancet. 1995;345:91–95. doi: 10.1016/s0140-6736(95)90062-4. [DOI] [PubMed] [Google Scholar]
- Metter J, Hanson W. Clinical and acoustical variability in hypokinetic dysarthria. Journal of Communication Disorders. 1986;19:347–366. doi: 10.1016/0021-9924(86)90026-2. [DOI] [PubMed] [Google Scholar]
- Moretti R, Torre P, Antonello RM, Capus L, Gioulis M, Zambito Marsala S, Bava A. “Speech initiation hesitation” following subthalamic nucleus stimulation in a patient with Parkinson’s disease. European Neurology. 2003;49:251–253. doi: 10.1159/000070199. [DOI] [PubMed] [Google Scholar]
- Niemi J, Koivuselka-Sallinen Temporal delay and lexical retrieval in narratives: Aphasiological observations. Journal of Communication Disorders. 1987;20:171–186. doi: 10.1016/0021-9924(87)90008-6. [DOI] [PubMed] [Google Scholar]
- O'Connell DC, Kowal S. Pausology. In: Sedelow WA, Sedelow SY, editors. Computers in language research 2. Berlin, New York, Amsterdam: Mouton Publishers; 1983. [Google Scholar]
- Ogar J, Slama H, Dronkers N, Amici S, Gorno-Tempini M. Apraxia of speech: An overview. Neurocase. 2005;11:427–432. doi: 10.1080/13554790500263529. [DOI] [PubMed] [Google Scholar]
- Oliveira M. The role of pause occurrence and pause duration in the signaling of narrative structure. Advances in Natural Language Processing. 2002;2389:43–51. [Google Scholar]
- Pinto S, Gentil M, Fraix V, Benabid A, Pollak P. Effects of subthalamic nucleus stimulation on oral force control in Parkinson’s disease. Journal of Neurology. 2003;250:179–187. doi: 10.1007/s00415-003-0966-7. [DOI] [PubMed] [Google Scholar]
- Romito LM, Scerrati M, Contarino MF, Bentivoglio AR, Tonali P, Albanese A. Long-term follow up of subthalamic nucleus stimulation in Parkinson’s disease. Neurology. 2002;58:1546–1550. doi: 10.1212/wnl.58.10.1546. [DOI] [PubMed] [Google Scholar]
- Romito LM, Scerrati M, Contarino MF, Iacoangeli M, Bentivoglio AR, Albanese A. Bilateral high frequency subthalamic stimulation in Parkinson’s disease: long-term neurological follow-up. Journal of Neurosurgical Science. 2003;47:119–128. [PubMed] [Google Scholar]
- Sidtis D, Cameron K, Bonura L, Sidtis JJ. Speech intelligibility by listening in Parkinson speech with and without deep brain stimulation. Journal of Neurolinguistics. 2011;25(2):121–132. [Google Scholar]
- Signorini M, Volpato C. Action fluency in Parkinson’s disease: A follow-up study. Movement Disorder. 2006;21:467–472. doi: 10.1002/mds.20718. [DOI] [PubMed] [Google Scholar]
- Skodda S, Schlegel U. Speech rate and rhythm in Parkinson’s disease. Movement Disorders. 2005;23:985–992. doi: 10.1002/mds.21996. [DOI] [PubMed] [Google Scholar]
- Swerts M, Wichmann A, Beun RJ. Filled pauses as markers of discourse structure; Spoken Language, ICSLP 96. Fourth International Conference; 1996. [Google Scholar]
- Torp J, Hammen V. Perception of parkinsonian speech rate. Journal of Medical Speech-Language Pathology. 2000;8:323–329. [Google Scholar]
- Thurber C, Tager-Flusberg H. Pauses in the narratives produced by autistic, mentally retarded, and normal children as an index of cognitive demand. Journal of Autism and Developmental Disorders. 1993;23:309–322. doi: 10.1007/BF01046222. [DOI] [PubMed] [Google Scholar]
- Whelan BM, Murdoch BE, Theodoros DG, Hall B, Silburn P. Defining a role for the subthalamic nucleus within operative theoretical models of subcortical participation in language. Journal of Neurology, Neurosurgery, and Psychiatry. 2003;74:1543–1550. doi: 10.1136/jnnp.74.11.1543. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Zanini S, Melatini A, Capus L, Gioulis M, Vassallo A, Bava A. Language recovery following subthalamic nucleus stimulation in Parkinson’s disease. Cognitive Neuroscience and Neuropsychology. 2003;14:511–516. doi: 10.1097/00001756-200303030-00043. [DOI] [PubMed] [Google Scholar]
- Zeches JT, Yorkston KM. Pause structure in narratives of neurologically impaired and control subjects. Clinical Aphasiology. 1995;23:155–163. [Google Scholar]