

Abstract
Background
Since 2009, the Hemorrhagic Fever with Renal Syndrome (HFRS) Targeted Expanded Program on Immunization (EPI) has been carried out in the 16–60 age population in Yichun City of Jiangxi Province. However, the annual reported incidences of HFRS in Yichun City Increased significantly from 2009 to 2013.
Material/Methods
The information on HFRS reported cases were obtained from the China Information System for Disease Control and Prevention (CISDCP), and demographic data was collected from the Basic Information System. Hantavirus-specific antigen and antibody of rodent specimens were tested by enzyme-linked immunosorbent assay (ELISA) or immune fluorescent assay.
Results
The annual HFRS incidences among all age subgroups presented growth tendencies in non-EPI targeted regions and EPI targeted regions, except for the EPI target population. The annual incidences of EPI target population were stable at around 10 per 100,000 population from 2008 to 2013. HFRS annual incidence was significantly related to rat virus index among all age subgroups in non-EPI targeted regions and >60 age subgroup in EPI targeted regions.
Conclusions
HFRS vaccine implement has had a notable effect in HFRS prevention and control.
MeSH Keywords: Ecology, Hantaan virus, Viral Vaccines
Background
Hemorrhagic fever with renal syndrome, caused by Hantaviruses (family Bunyaviridae) is an acute interstitial nephropathy characterized by high fever and varying degrees of renal insufficiency and hemorrhage [1]. HFRS includes diseases such as Korean hemorrhagic fever, epidemic hemorrhagic fever, and nephropathia epidemica. Hantaviruses is widely distributed in eastern Asia, particularly in China, Russia, and Korea [2–5]. Rodents are the natural reservoir for Hantaviruses. Known carriers include the striped field mouse (Apodemus agrarius), which is the reservoir for both Saaremaa and Hantaviruses [6]. Symptoms of HFRS usually develop within 1 to 2 weeks after exposure to infectious material, but in rare cases, they may take up to 8 weeks to develop [7]. Initial symptoms begin suddenly and include intense headaches, back and abdominal pain, fever, chills, nausea, and blurred vision [8,9].
China is the most severe endemic area in the world, with 30,000 to 50,000 cases reported annually, accounting for more than 90% of the total number of cases globally [3,10]. In 1989 the HFRS was classified as a Class B notifiable communicable disease in China. With the aim to reduce HFRS incidence, the Chinese government has implemented the HFRS-targeted Expanded Program on Immunization in several highest incidence provinces from 2008. According to the China CDC report, Jiangxi Province is one of the Chinese provinces with the highest HFRS incidence in the last 10 years, and almost 70% of HFRS cases were reported in Yichun City. Yichun City has implemented the HFRS-targeted EPI since 2009 and free vaccine was provided to the 4 highest incidence counties: Gaoan, Shanggao, Yifeng, and Fengxin. But the reported incidences of HFRS in both Jiangxi Province and Yichun City increased from 2009 to 2013 (Figure 1).
Figure 1.
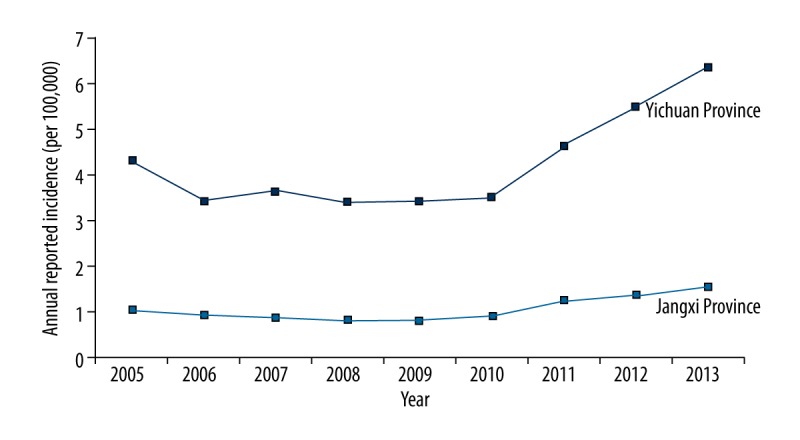
HFRS annual reported incidence of Jiangxi province and Yichun City from 2005 to 2013.
In order to evaluate the effect of the EPI program, this paper analyzed the reported HFRS case data of Yichun City, including 4 EPI targeted regions and 6 non-EPI targeted regions, and conducted an ecological study by comparing the reported incidence changes among the non-vaccinated regions and vaccinated regions.
Material and Methods
Data resource and collection
The information, including sex, date of onset, birthdate, and residential address of HFRS reported cases from 2005 to 2013 were obtained from the CISDCP, which is a web-based surveillance system to report and monitor infectious diseases and has been applied in the Chinese Center for Disease Control and Prevention since 2004 [11]. Each case was confirmed by laboratory testing or diagnosed by clinical symptoms according to the Diagnostic Criteria for Epidemic Hemorrhagic Fever. Demographic data was collected from the Basic Information System, a subsystem of the CISDCP.
Rodents surveillance
Rodent hantavirus surveillance was carried out in spring and autumn-winter seasons by night trapping method every year. Snap traps were set up in the field and in residential areas to estimate the proportion of different species of reservoir rodents and the intensity of rodents. Direct and indirect immune fluorescent assay were conducted to detect hantavirus-specific antigen from rodent lungs. Enzyme-linked immunosorbent assay was conducted to detect Hantavirus-specific antibody from rodent serum. Rodent density, positive number (PA), positive rate (PR), and index of rat with virus (IRV) were calculated.
Data analysis
According to EPI request, the age range of the human target population was 16 to 60 years [8], so we categorized reported cases and resident population into 3 groups: “early age” (<16 years of age), “targeted age” (16–60 years of age), and “old age” (>60 years of age) groups. The demographic characteristics between EPI and non-EPI targeted regions were compared by χ2 and t test by STATA 11.0 software (StataCorp, College Station, TX). The description of annual HFRS incidences was conducted by Microsoft Excel 2010 and the correlation coefficient between annual HFRS incidences and rat virus index was calculated by STATA 11.0 software.
Results
Demographic characteristics of HFRS cases
A total of 3529 HFRS cases were reported from 2005 to 2013. Based on EPI request, all HFRS human cases in Yichun City from 2005 to 2013 were divided into 2 region groups: non-EPI targeted regions and EPI targeted regions. As Table 1 shows, there were no significant differences between non-EPI and EPI targeted regions on age and sex distributions in each year from 2005 to 2013.
Table 1.
Demographic characteristics between EPI targeted regions and non-EPI targeted regions.
| Year | Non-EPI targeted regions | EPI targeted regions | P1 | P2 | ||
|---|---|---|---|---|---|---|
| Age (χ̄±S) | Sex (female/male) | Age (χ̄±S) | Sex (female/male) | |||
| 2005 | 41.06±13.82 | 38/11 | 37.02±17.06 | 133/61 | >0.05 | >0.05 |
| 2006 | 43.58±14.97 | 25/9 | 39.79±16.67 | 110/44 | >0.05 | >0.05 |
| 2007 | 39.36±16.40 | 23/13 | 41.87±15.57 | 114/52 | >0.05 | >0.05 |
| 2008 | 41.91±14.60 | 41/19 | 40.87±14.70 | 84/47 | >0.05 | >0.05 |
| 2009 | 43.83±18.11 | 34/18 | 42.01±16.30 | 100/35 | >0.05 | >0.05 |
| 2010 | 37.92±16.82 | 35/16 | 40.30±16.23 | 95/44 | >0.05 | >0.05 |
| 2011 | 42.37±17.58 | 56/30 | 41.45±17.82 | 113/53 | >0.05 | >0.05 |
| 2012 | 44.49±17.35 | 108/36 | 41.84±19.16 | 119/39 | >0.05 | >0.05 |
| 2013 | 43.24± 19.96 | 110/55 | 41.63±20.20 | 122/60 | >0.05 | >0.05 |
P1 – t test of age between EPI and non-EPI targeted regions; P1 – χ2 test of sex between EPI and non-EPI targeted regions.
Age distribution of HFRS cases
As Table 2 shows, the HFRS reported cases numbers of each age subgroup increased continuously in both EPI and non-EPI targeted regions from 2008 to 2013. The proportions of EPI targeted age (16–60 years of age) subgroups decreased continuously, but the proportions of older adults (>60 years of age) were increasing rapidly in both EPI and non-EPI targeted regions from 2008 to 2013 (Figure 2).
Table 2.
The number of reported HFRS cases in Yichun from 2005 to 2013.
| Year | Yichun city | EPI targeted regions | Non-EPI targeted regions | ||||||
|---|---|---|---|---|---|---|---|---|---|
| <16 | 16–60 | >60 | <16 | 16–60 | >60 | <16 | 16–60 | >60 | |
| 2005 | 29 | 193 | 21 | 27 | 150 | 17 | 2 | 43 | 4 |
| 2006 | 15 | 153 | 20 | 13 | 124 | 17 | 2 | 29 | 3 |
| 2007 | 17 | 161 | 24 | 14 | 133 | 19 | 3 | 28 | 5 |
| 2008 | 9 | 165 | 17 | 6 | 113 | 12 | 3 | 52 | 5 |
| 2009 | 11 | 154 | 22 | 9 | 113 | 13 | 2 | 41 | 9 |
| 2010 | 24 | 146 | 20 | 15 | 109 | 15 | 9 | 37 | 5 |
| 2011 | 29 | 182 | 41 | 20 | 118 | 28 | 9 | 64 | 13 |
| 2012 | 31 | 210 | 61 | 20 | 108 | 30 | 11 | 102 | 31 |
| 2013 | 47 | 225 | 75 | 25 | 117 | 40 | 22 | 108 | 35 |
Figure 2.

Reported cases proportions of 3 age subgroups in EPI and non-EPI targeted regions from 2005 to 2013.
Annual incidence of HFRS
Because age compositions of populations in EPI and non-EPI targeted regions were similar (data not shown), the calculation of HFRS reported incidence was not adjusted in this research. Because the EPI project was first implemented in high incidence areas, the incidences of each age subgroups in EPI targeted regions were higher than corresponding age subgroups in non-EPI targeted regions. As Table 3 and Figure 3 show, the annual incidences among all age subgroups presented growth tendencies in non-EPI targeted regions. In EPI targeted regions, the annual incidences among the early age and old age subgroups showed similar increasing tendency, but the annual incidences of EPI target population were stable, at around 10 per 100,000 population from 2008 to 2013. Because HFRS-targeted EPI was implemented in Yichun City from 2009, relative ratio with fixed base from 2008 to 2013 was calculated to reveal the development and increase velocities of HFRS annual incidence in EPI targeted (16–60 years of age) subgroups among EPI and non-EPI targeted regions (Table 4). Development and increase velocities of annual incidence among EPI targeted population maintained at a level of 100% and a level less than 15% relative to 2008. But among non-EPI targeted population, development velocities reached around 200% in 2012 and 2013, and increase velocities reached around 100% in 2012 and 2013. Semi-log plot directly reflected this relative growth rate among EPI and non-EPI targeted population from 2008 to 2013 (Figure 4).
Table 3.
HFRS annual incidence of 3 age subgroups from 2005 to 2013.
| Areas | Age | HFRS annual incidence (per 100,000 population) | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| 2005 | 2006 | 2007 | 2008 | 2009 | 2010 | 2011 | 2012 | 2013 | ||
| EPI targeted regions | <16 | 4.83 | 2.36 | 2.58 | 1.13 | 1.72 | 2.91 | 3.92 | 4.12 | 5.19 |
| 16–60 | 14.2 | 11.5 | 12.12 | 10.11 | 9.98 | 9.50 | 11.51 | 10.29 | 11.16 | |
| >60 | 10.18 | 10.11 | 11.19 | 6.9 | 7.27 | 8.08 | 14.67 | 14.38 | 18.79 | |
| Non-EPI targeted regions | <16 | 0.29 | 0.17 | 0.25 | 0.26 | 0.17 | 0.81 | 0.80 | 1.21 | 2.04 |
| 16–60 | 1.65 | 1.37 | 1.31 | 2.37 | 1.84 | 1.63 | 2.93 | 4.64 | 4.91 | |
| >60 | 1.16 | 0.86 | 1.43 | 1.41 | 2.47 | 1.32 | 3.26 | 7.28 | 8.08 | |
Figure 3.

HFRS annual incidence City from 2005–2013 in Yichun City.
Table 4.
Relative growth rate of HFRS annual incidence among EPI targeted population in Yichun City from 2008–2013.
| Relative ratio with fixed base | Regions | Year | |||||
|---|---|---|---|---|---|---|---|
| 2008 | 2009 | 2010 | 2011 | 2012 | 2013 | ||
| VD(%) | EPI targeted regions | Ref | 98.71 | 93.96 | 113.84 | 101.78 | 110.38 |
| Non-EPI targeted regions | Ref | 77.63 | 68.77 | 123.62 | 195.78 | 207.17 | |
| VI(%) | EPI targeted regions | Ref | −1.28 | −6.03 | 13.84 | 1.780 | 10.38 |
| Non-EPI targeted regions | Ref | −22.36 | −31.22 | 23.62 | 95.78 | 107.17 | |
VD – velocity of development; VI –velocity of increase.
Figure 4.
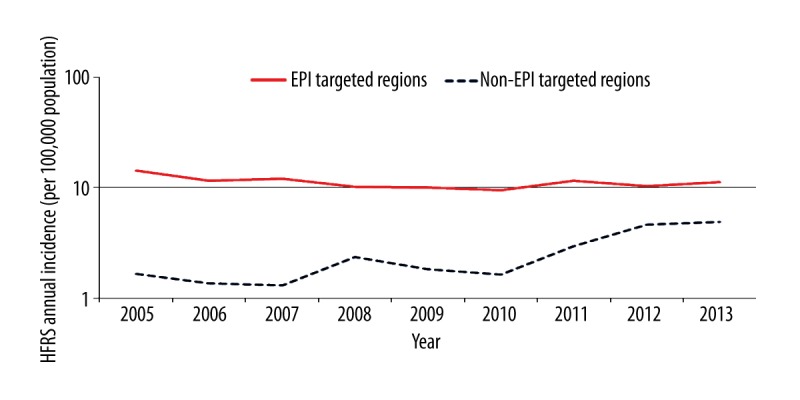
Semi-log plot of HFRS annual incidences of EPI targeted population in Yichun City from 2005 to 2013.
Correlation analysis of HFRS annual incidence and rodent Hantavirus epidemics in Yichun City from 2005 to 2013
From 2005 to 2013, a total 83400 traps were set out and 2102 rats were captured. All the specimens of captured rats were tested by the Virology Laboratory of Jiangxi Province Center for Disease Control and Prevention (CDC) (Table 5). The positive rat numbers and positive rates in 2011, 2012, and 2013 were significantly higher than in previous years. Correlation analysis showed HFRS annual incidence was related to rat virus index among all age subgroups in non-EPI targeted regions and old age subgroup in EPI targeted regions (r>0.06, p<0.05), except for the EPI targeted population and early age subgroups in EPI targeted regions (Table 6).
Table 5.
Data of Rodent Hantavirus surveillances in Yichun city from 2005 to 2013.
| Year | Mousetraps (N) | Rats (N) | Density (%) | NPA (N) | PA (%) | IRV |
|---|---|---|---|---|---|---|
| 2005 | 10600 | 307 | 2.90 | 0 | 0.00 | 0.000 |
| 2006 | 5700 | 219 | 3.84 | 0 | 0.00 | 0.000 |
| 2007 | 6800 | 231 | 3.40 | 4 | 1.73 | 0.024 |
| 2008 | 8000 | 210 | 2.63 | 1 | 0.48 | 0.011 |
| 2009 | 10400 | 232 | 2.23 | 0 | 0.00 | 0.000 |
| 2010 | 11100 | 226 | 2.04 | 1 | 0.44 | 0.009 |
| 2011 | 11600 | 210 | 1.81 | 9 | 4.28 | 0.027 |
| 2012 | 9600 | 254 | 2.65 | 8 | 3.15 | 0.029 |
| 2013 | 9600 | 213 | 2.22 | 7 | 3.29 | 0.027 |
PN – positive number; PA – positive rate; IRV – index of rat with virus. RVI=√(Density*PN).
Table 6.
Correlativity analysis between HFRS annual incidences and rats virus index in Yichun City from 2005 to 2013.
| Statistical indicators | EPI targeted regions | Non-EPI targeted regions | ||||
|---|---|---|---|---|---|---|
| <16 | 16–60 | >60 | <16 | 16–60 | >60 | |
| r | 0.4245 | −0.1256 | 0.7576 | 0.6691 | 0.7071 | 0.6981 |
| p | 0.2548 | 0.7474 | 0.018 | 0.0488 | 0.0331 | 0.0365 |
Discussion
The annual report of China’s key infectious diseases surveillance from 2005 to 2013 showed that the number of HFRS reported cases in Jiangxi province stayed in the top 10 every year among 30 provinces in China, and the top city in Jiangxi province was Yichun, which accounted for more than 70%. This study analyzed the surveillance data of both HFRS human cases and rodent host from 2005 to 2013 to observe the epidemic changes and trends of HFRS. Since 2005, The HFRS prevalence trends in Jiangxi Province and Yichun City steadily declined until 2009, after which they were clearly increased in both Jiangxi Province and Yichun City [12], very similar to other Chinese provinces, as reported by He et al. [4].
The research work on HFRS vaccination started since 1970s, and 4 vaccines were produced, including 3 univalent vaccines (gerbil kidney cell vaccine, hamster kidney cell vaccine, and mouse brains vaccine) and 1 bivalent gerbil kidney cell vaccine. The safety, serology, and protection of these vaccines were all verified by many epidemiologic and serological studies, and the population 16–60 years old was confirmed the as target population. Considering that Yichun City is a mixed HFRS infected areas, bivalent gerbil kidney cell vaccine was selected and applied to targeted population in 4 high-risk counties from 2009. In order to investigate the variations of HFRS epidemiological characters, this study divided the surveillance data into 2 groups by region according to whether it was EPI or non-EPI targeted. Among those 2 groups, HFRS reported cases further divided into 3 subgroups: “early age”, “targeted age”, and “old age”.
This study found that age and sex distributions between non-EPI and EPI targeted regions were not significantly different each year from 2005 to 2013. The proportions of EPI targeted age (16–60 years) subgroups were decreasing continuously, and the proportions of older adults (>60 years) were increasing rapidly in both EPI and non-EPI targeted regions from 2008 to 2013. This findings were in conformity with results reveal by He et al., who described the age proportions of HFRS in 28 provinces in China between 2005 and 2010. They found the proportion of HFRS cases among targeted individuals showed a decrease and the proportion of the non-EPI-targeted age group increased significantly during the EPI years in both non-EPI and EPI targeted regions [4]. Because the proportions of HFRS cases among targeted ages were both decreasing in non-EPI and EPI targeted regions, we cannot ascribe this decrease to the effect of EPI implementation. This finding might be explained by population outflow. Nowadays in China, more and more young and middle-aged people are leaving home to seek jobs or education elsewhere. Older people became the main labor force in agriculture, which might increase the chances of hantavirus infection.
Even though the proportion of HFRS reported cases in the 16–60 age group were both decreasing in EPI and non-EPI targeted regions from 2008 to 2013, the annual incidence tendencies of this age population were obviously different. From 2009 to 2013, the annual incidences among early and old age population in both EPI and non-EPI targeted regions all showed upward tendencies and the annual incidences among EPI target age population in non-EPI targeted regions also increased but the annual incidences among EPI target age population in EPI targeted regions were relative stable. Through development velocity analysis, this research found the increase velocity of the annual incidences among EPI targeted age population in non-EPI was discernibly faster than in EPI targeted regions. In view of the similar geographical locale, population mobility, employment type, and living (hygiene) conditions in EPI and non-EPI targeted regions, this study considered that the annual incidences of EPI-targeted population in EPI implemented areas remained stable, and the overall incidence increase could have contributed to the effect of HFRS vaccination.
Previous study has reported that the rodent-vector is a key factor in HFRS epidemiology [4,13,14]. This study found the numbers of HFRS infection-positive rats and HFRS infection-positive rates in captured rats were significant increasing in 2011, 2012, and 2013 compared to previous years. The correlation analysis found HFRS annual incidence among the inoculated population was significantly more positive than the rat virus index, indicating active prevalence of hantaviruses in rodents might be the cause of increasing HFRS incidence in humans from 2011 to 2013.
Conclusions
The overall incidence of HFRS in Yichun City was increasing from 2008 to 2013, which may be caused by the more active hantavirus prevalence among rodents. The HFRS incidence among the older population was increasing rapidly, and more public health erffort should be focussed on them. HFRS vaccine implementation has had a notable effect in HFRS prevention and control, and it should be applied widely and continuously in the future.
Footnotes
Conflict of interest
None.
Source of support: This work was supported by grants from Jiangxi Provincial National Health and Family Planning Commission research project “Study on immune effect and high incidence investigation of HFRS in key areas of Jiangxi province” (20156078)
References
- 1.Hansen A, Cameron S, Liu Q, et al. Transmission of haemorrhagic fever with renal syndrome in china and the role of climate factors: a review. Int J Infect Dis. 2015;33:212–18. doi: 10.1016/j.ijid.2015.02.010. [DOI] [PubMed] [Google Scholar]
- 2.Macneil A, Nichol ST, Spiropoulou CF. Hantavirus pulmonary syndrome. Virus Res. 2011;162:138–47. doi: 10.1016/j.virusres.2011.09.017. [DOI] [PubMed] [Google Scholar]
- 3.Staff PNTD. Correction: Spatiotemporal transmission dynamics of hemorrhagic fever with renal syndrome in China, 2005–2012. PLoS Negl Trop Dis. 2015;9:e0003599. doi: 10.1371/journal.pntd.0003599. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.He X, Wang S, Huang X, Wang X. Changes in age distribution of hemorrhagic fever with renal syndrome: an implication of China’s expanded program of immunization. BMC Public Health. 2013;13:394. doi: 10.1186/1471-2458-13-394. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Yu PB, Tian HY, Ma CF, et al. Hantavirus infection in rodents and haemorrhagic fever with renal syndrome in Shaanxi province, China, 1984–2012. Epidemiol Infect. 2015;143:405–11. doi: 10.1017/S0950268814001009. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Xiao H, Tian HY, Cazelles B, et al. Atmospheric moisture variability and transmission of hemorrhagic fever with renal syndrome in Changsha City, Mainland China, 1991–2010. PLoS Negl Trop Dis. 2013;7:e2260. doi: 10.1371/journal.pntd.0002260. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Liu YX, Wang ZQ, Guo J, et al. Spatio-temporal evolution on geographic boundaries of HFRS endemic areas in Shandong Province, China. Biomed Environ Sci. 2013;26:972–78. doi: 10.3967/bes2013.032. [DOI] [PubMed] [Google Scholar]
- 8.Du H, Wang PZ, Li J, et al. Clinical characteristics and outcomes in critical patients with hemorrhagic fever with renal syndrome. BMC Infect Dis. 2014;14:191. doi: 10.1186/1471-2334-14-191. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Wu J, Wang DD, Li XL, et al. Increasing incidence of hemorrhagic fever with renal syndrome could be associated with livestock husbandry in Changchun, northeastern China. BMC Infect Dis. 2014;14:301. doi: 10.1186/1471-2334-14-301. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Liu X, Jiang B, Bi P, et al. Prevalence of haemorrhagic fever with renal syndrome in mainland China: analysis of National Surveillance Data, 2004–2009. Epidemiol Infect. 2012;140:851–57. doi: 10.1017/S0950268811001063. [DOI] [PubMed] [Google Scholar]
- 11.Xiong W, Lv JLi L. A survey of core and support activities of communicable disease surveillance systems at operating-level CDCs in China. BMC Public Health. 2010;10:704. doi: 10.1186/1471-2458-10-704. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Zhang S, Wang S, Yin W, et al. Epidemic characteristics of hemorrhagic fever with renal syndrome in China, 2006–2012. BMC Infect Dis. 2014;14:384. doi: 10.1186/1471-2334-14-384. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Li CP, Cui Z, Li SL, et al. Association between hemorrhagic fever with renal syndrome epidemic and climate factors in Heilongjiang Province, China. Am J Trop Med Hyg. 2013;89:1006–12. doi: 10.4269/ajtmh.12-0473. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Guan P, Huang D, He M, et al. Investigating the effects of climatic variables and reservoir on the incidence of hemorrhagic fever with renal syndrome in Huludao City, China: a 17-year data analysis based on structure equation model. BMC Infect Dis. 2009;9:109. doi: 10.1186/1471-2334-9-109. [DOI] [PMC free article] [PubMed] [Google Scholar]