

Dear Editor:
The acidic pH of the stratum corneum (SC) is important to the protective functions of the skin, including permeability barrier homeostasis1,2, SC integrity and cohesion1,2, antimicrobial defense2,3, and primary cytokine activation. The pH of the SC increases in inflamed skin4 such as in atopic dermatitis (AD). Therefore, the reversal of pH abnormality may be a possible preventive or therapeutic strategy for these problems5. Acidification of the SC improves permeability barrier homeostasis by increasing the activity of the two key ceramide-generating enzymes such as β-glucocerebrosidase and acidic sphingomyelinase6, and reinforces SC integrity and cohesion by decreasing the activity of serine proteases. Many alternative treatment modalities have been suggested for refractory AD. In Japan, bathing in acidic hot spring water is one of the treatment options for refractory AD. Acidic water has been known to have an antibacterial effect against Staphylococcus aureus, which densely colonize in the eczematous skin of AD7. We conducted a clinical study in patients with refractory AD by using acidic water bathing. We compared the efficacy of acidic water bathing to that of wet-wrap dressing which has already been shown to be highly effective for severe or refractory AD3,8.
The experiment was performed after obtaining approval from the Institutional Review Board (2011-49) of Wonju Severance Christian Hospital, Yonsei University Wonju College of Medicine. Eighteen patients with AD were recruited. Their eczema area and severity index (EASI) scores ranged from 11.4 to 59.6 (mean±standard deviation, 26.9±12.7). All patients had refractory AD that required long-term maintainence with cyclosporine to control their atopic eczema. Eight patients (positive control group) were treated with wet-wrap dressing and ten patients (treatment group) were treated with acidic water bathing (Table 1). The mean EASI scores of the wet-wrap dressing group and the acidic water bathing group were 28.69 and 25.36, respectively. No statistical difference was observed (p-value=0.67).
Table 1. Summary of atopic dermatitis patients.
| Group* | Case number | Sex | Age (yr) | EASI | ΔEASI (%) | |
|---|---|---|---|---|---|---|
| Pre-treat | Post-treat | |||||
| Wet-wrap dressing (control group) | ||||||
| 1 | F | 9 | 46.5 | 26.4 | 43.2 | |
| 2 | F | 4 | 36.9 | 30.0 | 18.7 | |
| 3 | M | 28 | 35.5 | 20.7 | 40.0 | |
| 4 | M | 9 | 15.8 | 16.0 | 0.0 | |
| 5 | M | 20 | 37.6 | 21.4 | 43.1 | |
| 6 | F | 17 | 17.6 | 12.1 | 31.3 | |
| 7 | M | 16 | 18.5 | 10.7 | 42.2 | |
| 8 | M | 30 | 21.1 | 14.8 | 66.7 | |
| 16.6±8.6 | 28.7±10.9 | 19.0±14.7 | 31.1±15.7 | |||
| Acidic water bathing (treated group) | ||||||
| 1 | M | 23 | 26.9 | 14.4 | 46.5 | |
| 2 | F | 38 | 23.8 | 20.7 | 13.0 | |
| 3 | M | 27 | 14.8 | 3.3 | 77.7 | |
| 4 | M | 35 | 59.6 | 53.7 | 9.9 | |
| 5 | M | 39 | 33.9 | 19.6 | 42.2 | |
| 6 | M | 29 | 23.3 | 13.0 | 44.2 | |
| 7 | F | 14 | 11.4 | 8.5 | 25.4 | |
| 8 | M | 17 | 22.9 | 14.0 | 38.9 | |
| 9 | F | 13 | 12.2 | 9.6 | 21.3 | |
| 10 | M | 17 | 24.8 | 20.6 | 16.9 | |
| 26.6±8.9 | 26.9±15.1 | 19.9±12.4 | 33.6±20.6 | |||
Values are presented as data only or mean±standard deviation. *Among the 18 patients, 8 patients were applied with wet-wrap dressing and 10 patients were applied with acidic water bathing. EASI: eczema area and severity index, F: female, M: male.
Patients in the acidic water bathing group were instructed to take a 40-minute warm bath with a pH of 3.0 twice daily for 2 days, pat with a towel, and thoroughly apply moisturizers immediately after getting out of the bath. The acidic water was made by dissolving citric acid (Fuso Chemical Co., Qingdao, China) in tap water until the bath water had a pH of 3.0.
The wet-wrap dressing group took a 5-minute tepid bath or shower, applied moisturizer (Cellbrick; Barummedi, Seoul, Korea) thoroughly on the whole body after patting gently, and wore clinging wet dressings soaked with warm and clean water with a raincoat over the dressings. For the first and/or second treatment, 1:3 diluted topical 0.05% desonide lotion (Desowen; Galderma Pharma SA, Lausanne, Switzerland) and moisturizer were used. For the third and fourth treatments, only moisturizer was used. After 40 minutes, the patients took off the wet dressings and applied moisturizer again.
Both patient groups were told not to use any additional medications other than the moisturizers and corticosteroids used in the treatment. Every patient filled in a questionnaire and was given an EASI score on the first visit. To evaluate epidermal permeability barrier function, basal transepidermal water loss (TEWL) and SC hydration (SCH) were measured with a Tewameter (Courage & Khazaka, Cologne, Germany), and a Corneometer (Courage & Khazaka) from lesion-free and lesional sites at the patients' forearms before and after each treatment. Skin evaluation was performed 12 hours after the last treatment. On the third day, 12 hours after the end of 4 sessions of treatments, the patients were asked about their satisfaction and any side effects.
Improvement of EASI score, referred to as Δ EASI, was compared between the acidic water bathing group and the wet-wrap dressing group. The Δ EASI of the group treated with acidic water bathing was over 30%. There was no difference compared to the group treated with wet-wrap dressing (Fig. 1). The effect of acidic water bathing on epidermal permeability barrier function was assessed by comparing Δ TEWL and Δ SC hydration measured from the lesion-free skin and lesional skin of the patients in each group. No significant differences were found in non-lesional skin or lesional skin between the two groups (Fig. 2). The satisfaction of patients in the acid water bathing group was nearly the same as that of patients in the wet-wrap dressing group. No side effects were reported except for an initial, rapidly subsiding, and mild tingling sensation in two patients in the acidic water bathing group. Recently, the efficacy of SC acidification in the treatment of developmentally impaired skin has been studied. Hyper-acidification was revealed to normalize the impaired barrier function of neonatal and aged human and rodent skin in which SC acidification was impaired. Maintenance of SC acidity by topical acidic application was demonstrated to prevent the emergence of AD9 and even the occurrence of respiratory allergic inflammation10. In Japan, bathing in acidic hot springs (around pH 2.5) located near a dormant volcano is known to be effective for severe or refractory AD. However, Korea has no hot water springs. To mimic the effects of these hot springs for patients with AD, we used artificially acidified water, which costs a small amount. Improvements of the eczema lesions measured by EASI scores and the permeability barrier function measured by TEWL and SC hydration were not significantly different between patients with AD treated with acidic water bathing and those treated with wet-wrap dressing, the latter being an already widely accepted treatment for refractory AD. Patient satisfaction with the two treatments was similar, and side effects were negligible.
Fig. 1. The improvement in eczema area and severity index (EASI) score indicated by Δ EASI (%) in the patient group treated with acidic water bathing was not significantly different from that seen in the wet-wrap dressing group. Results are shown as the mean±standard error of the mean.
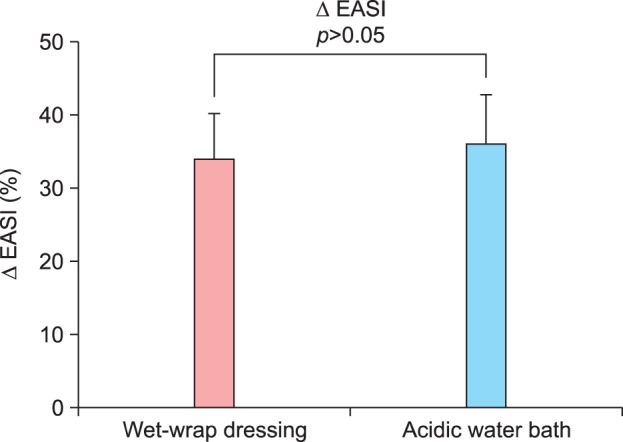
Fig. 2. Improvement in skin barrier function indicated by Δ TEWL (%) and Δ SCH (%) in the acidic water bathing group was comparable to that in the wet-wrap dressing group. There were no differences between the two groups in either lesion-free or lesional skin. Results are shown as the mean±standard error of the mean. TEWL: transepidermal water loss, SCH: stratum corneum hydration.

The present clinical experiments in humans showed that acidic water bathing was as effective for severe or refractory AD as was wet-wrap dressing. However, we could not select subjects by age because of the limited number of enrolled patients. Furthermore, a blind study could not be performed. We surmise that acidic water bathing can be an alternative and safe therapeutic modality for severe or refractory AD.
ACKNOWLEDGMENT
This study was supported by a grant from the Korean Health Technology R&D Project, Ministry of Health & Welfare, Republic of Korea (Grant No.: HN10C0033).
References
- 1.Fluhr JW, Kao J, Jain M, Ahn SK, Feingold KR, Elias PM. Generation of free fatty acids from phospholipids regulates stratum corneum acidification and integrity. J Invest Dermatol. 2001;117:44–51. doi: 10.1046/j.0022-202x.2001.01399.x. [DOI] [PubMed] [Google Scholar]
- 2.Hachem JP, Crumrine D, Fluhr J, Brown BE, Feingold KR, Elias PM. pH directly regulates epidermal permeability barrier homeostasis, and stratum corneum integrity/cohesion. J Invest Dermatol. 2003;121:345–353. doi: 10.1046/j.1523-1747.2003.12365.x. [DOI] [PubMed] [Google Scholar]
- 3.Devillers AC, de Waard-van der Spek FB, Mulder PG, Oranje AP. Treatment of refractory atopic dermatitis using 'wet-wrap' dressings and diluted corticosteroids: results of standardized treatment in both children and adults. Dermatology. 2002;204:50–55. doi: 10.1159/000051810. [DOI] [PubMed] [Google Scholar]
- 4.Fluhr JW, Elias PM. Stratum corneum pH: formation and function of the "acid mantle". Exog Dermatol. 2002;1:163–175. [Google Scholar]
- 5.Hachem JP, Roelandt T, Schürer N, Pu X, Fluhr J, Giddelo C, et al. Acute acidification of stratum corneum membrane domains using polyhydroxyl acids improves lipid processing and inhibits degradation of corneodesmosomes. J Invest Dermatol. 2010;130:500–510. doi: 10.1038/jid.2009.249. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Holleran WM, Takagi Y, Uchida Y. Epidermal sphingolipids: metabolism, function, and roles in skin disorders. FEBS Lett. 2006;580:5456–5466. doi: 10.1016/j.febslet.2006.08.039. [DOI] [PubMed] [Google Scholar]
- 7.Akiyama H, Yamasaki O, Tada J, Kubota K, Arata J. Antimicrobial effects of acidic hot-spring water on Staphylococcus aureus strains isolated from atopic dermatitis patients. J Dermatol Sci. 2000;24:112–118. doi: 10.1016/s0923-1811(00)00091-8. [DOI] [PubMed] [Google Scholar]
- 8.Devillers AC, Oranje AP. Efficacy and safety of 'wet-wrap' dressings as an intervention treatment in children with severe and/or refractory atopic dermatitis: a critical review of the literature. Br J Dermatol. 2006;154:579–585. doi: 10.1111/j.1365-2133.2006.07157.x. [DOI] [PubMed] [Google Scholar]
- 9.Hatano Y, Man MQ, Uchida Y, Crumrine D, Scharschmidt TC, Kim EG, et al. Maintenance of an acidic stratum corneum prevents emergence of murine atopic dermatitis. J Invest Dermatol. 2009;129:1824–1835. doi: 10.1038/jid.2008.444. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Lee HJ, Yoon NY, Lee NR, Jung M, Kim DH, Choi EH. Topical acidic cream prevents the development of atopic dermatitis- and asthma-like lesions in murine model. Exp Dermatol. 2014;23:736–741. doi: 10.1111/exd.12525. [DOI] [PubMed] [Google Scholar]