

Abstract
Objective
Students referred to school administration for alcohol policies violations currently receive a wide variety of interventions. This study examined predictors of response to two interventions delivered to mandated college students (N = 598) using a stepped care approach incorporating a peer-delivered 15-minute BA session (BA; Step 1) and a 60–90 minute brief motivational intervention delivered by trained interventionists (BMI; Step 2).
Method
Analyses were completed in two stages. First, three types of variables (screening variables, alcohol-related cognitions, mandated student profile) were examined in a logistic regression model as putative predictors of lower-risk drinking (defined as 3 or fewer heavy episodic drinking [HED] episodes and/or 4 or fewer alcohol-related consequences in the past month) six weeks following the BA session. Second, we used generalized estimating equations to examine putative moderators of BMI effects on HED and peak blood alcohol content (pBAC) compared to assessment-only control (AO) over the 3, 6, and 9 month follow-ups.
Results
Participants reporting lower scores on the Alcohol Use Disorders Identification Test (AUDIT), more benefits to changing alcohol use, and those who fit the ‘Bad Incident’ profile at baseline were more likely to report lower risk drinking 6 weeks after the BA session. Moderation analyses revealed that ‘Bad Incident’ students who received the BMI reported more HED at 9-month follow up than those who received AO.
Conclusion
Current alcohol use as well as personal reaction to the referral event may have clinical utility in identifying which mandated students benefit from treatments of varying content and intensity.
Keywords: alcohol, brief advice, brief motivational intervention, peers
Thousands of college students receive campus alcohol violations and mandatory alcohol interventions each year (Bernat, Lenk, Nelson, Winters, & Toomey, 2014). However, the mandated student population is a heterogeneous one, for which a “one size fits all” intervention approach may not be appropriate (Borsari, 2012; Merrill, Carey, Lust, Kalichman, & Carey, 2014). A stepped care approach may be an efficient way to address the needs of this population, as it provides a lower dose/minimal intervention initially and a more intensive intervention for those who do not respond to the lower dose intervention (Sobell & Sobell, 2000). Two promising candidates for inclusion in stepped care approaches for reducing alcohol use and consequences in college students are brief advice (BA; Fleming et al., 2010; Helmkamp et al., 2003; Kulesza, Apperson, Larimer, & Copeland, 2010; Schaus, Sole, McCoy, Mullett, & O’Brien, 2009) and brief motivational interventions (BMI; Carey, Scott-Sheldon, Carey, & DeMartini, 2007; Fachini, Aliane, Martinez, & Furtado, 2012; Larimer & Cronce, 2007). Additionally, research suggests the use of peer counselors (fellow undergraduate students who deliver evidence-based interventions) may be one way to enhance and reduce the costs of intervention approaches (Larimer et al., 2001; Mastroleo, Mallett, Ray, & Turrisi, 2008). Thus, the combination of a stepped care approach with a peer counselor delivery component has the potential to meet a number of individual student needs.
A stepped care trial conducted with mandated students (Borsari et al., 2012) first provided a BA session delivered by a peer counselor; six weeks later, students who exhibited risky drinking (defined as 4 or more heavy episodic drinking [HED] episodes and/or 5 or more alcohol-related consequences) were randomized to a second intervention (BMI) or assessment only (AO). At 9-month follow-up, students who had received a BMI significantly reduced the number of alcohol-related problems compared to students in the AO group. However, neither the BMI nor AO participants demonstrated reductions in alcohol use (HED, peak blood alcohol content [pBAC]). These findings suggest that implementing stepped care with mandated students can be effective in reducing alcohol-related harms. That said, it is important to efficiently and empirically identify individuals who will require more intensive intervention following a peer-led BA, as well as the characteristics of students who are more or less responsive to a professionally-led BMI. This enhanced knowledge is vital for the efficient allocation of peer and professional intervention efforts and resources on campus.
Although predictors of response to sequentially-administered BA and BMI have yet to be examined, predictors of response to BA and moderators of response to BMI administered in stand-alone interventions have emerged in the literature. For example, one trial found BA and BMI equally efficacious in reducing alcohol use but not problems, and these outcomes were mediated by both descriptive norms and coping skills (Kulesza, McVay, Larimer, & Copeland, 2013). Research with mandated students found that women reduced drinking more following a BMI than a computer-delivered intervention, whereas men reduced alcohol use following either intervention (Carey, Henson, Carey, & Maisto, 2009). Students with higher numbers of alcohol-related problems at baseline were more responsive to a BMI with written feedback than to written feedback alone (Mun, White, & Morgan, 2009). Characteristics of the referral incident have also been found to predict outcomes. Specifically, BMI is more effective than written feedback alone for students who experienced severe incidents requiring police or medical attention (Mun et al., 2009), but less effective than computer delivered interventions for individuals who did not view the referral incident as aversive (Mastroleo, Murphy, Colby, Monti, & Barnett, 2011).
To our knowledge, no study has examined predictors of drinking response to two interventions delivered sequentially with mandated college students using a stepped care approach. There are several commonly assessed variables that have been associated with heavy alcohol use in college students. We examined three different types of variables. First, we wanted to examine whether four commonly obtained screening variables would inform response to the BA or BMI. Specifically, current risky drinking was of interest as there has been mixed prior results as to whether heavier drinkers are more responsive or not to a BMI (Mun et al., 2009; Murphy et al., 2001). As previously discussed, gender has been associated with differential response to BMIs. As early onset of alcohol use has been consistently related to alcohol use and abuse in adults (DeWit, Adlaf, Offord, Ogborne, 2000; Grant & Dawson, 1997; Morean, Corbin, & Fromme, 2012), students with an earlier age of first drink (AFD) may be less likely to reduce their drinking following a BA and/or BMI intervention. Sensation seeking (SS) is a personality trait with a biological basis that expresses itself as a need for physiological arousal (Quinn, Stappenbeck, & Fromme, 2011; Stephenson, Hoyle, Palmgreen, & Slater, 2003) and has been linked directly (Studies 1 and 2; Woicik, Stewart, Pihl, & Conrod, 2009) and indirectly to alcohol use in mandated (Pearson & Hustad, 2014) and incoming (Hustad, Pearson, Neighbors, & Borsari, 2014) college students.
Alcohol-related cognitions are also commonly assessed in mandated college students. Perhaps the most commonly assessed cognitions are alcohol-related expectancies and descriptive norms. Alcohol-related expectancies are beliefs about the cognitive, affective or behavioral effects of alcohol use and can be both positive (e.g., “drinking allows me to relax around others”) and negative (e.g., “when I drink, I often say things that I regret later”). However, recent reviews reveal inconsistent findings regarding expectancy interventions and drinking and alcohol-related outcomes (Cronce & Larimer, 2011; Labbe & Maisto, 2011; Scott-Sheldon, Terry, Carey, Garey, & Carey, 2012). Descriptive norms refer to the perception of other’s quantity and frequency of drinking, and are based largely on observations of how people consume alcohol in discrete drinking situations (Perkins, 2003). Descriptive norms have been linked to college alcohol use (see Borsari & Carey, 2001, 2003) and have been used commonly in interventions addressing college student drinking (Lewis & Neighbors, 2006; Miller et al., 2012). We were also particularly interested two other cognitions related to alcohol use. Reasons for limited drinking (RFLD; Greenfield, Guydish, & Temple, 1989) in college students have been found to be negatively related to binge drinking and alcohol related consequences (Collins, Koutsky, Morsheimer, & MacLean, 2001; Epler, Sher, & Piasecki, 2009; Palfai & Ralston, 2011) and positively related to interest in receiving alcohol-focused treatment (Epler, Sher, Loomis, & O’Malley, 2009). Finally, the participants’ perceptions of the costs and benefits of change may make mandated students more receptive to intervention. This may be especially true regarding a BMI that incorporates motivational interviewing (MI; Miller & Rollnick, 2012), a style “designed to strengthen personal motivation and commitment to a specific goal by eliciting and exploring the person’s own reasons for change” (p. 29).
It is also possible that a combination of factors, rather than a single variable, is associated with lower risk drinking in response to BA and/or BMI. Work from our research group (Barnett et al., 2008) derived three distinct profiles of mandated students based on their typical rates of alcohol use and problems, drinking on the day of the referral event, and personal responsibility and aversiveness of the incident. These profiles were: (1) ‘Bad Incident’ which was characterized by low scores for heavy drinking and problems, and high levels of referral event drinking, responsibility, and aversiveness; (2) ‘So What?’, which was characterized by high heavy drinking and alcohol-related problems, moderate incident drinking and responsibility, and low aversiveness; and (3) ‘Why Me?’, which was characterized by a pattern of relatively low heavy drinking and alcohol-related problems, very little incident drinking, and low responsibility and aversiveness. Perhaps such a multi-faceted and empirically-derived mandated student profile may be the most informative way to predict response to a BA and/or BMI.
Current Study
The purpose of this study was to evaluate whether a peer-delivered BA or professionally delivered BMI was more or less effective with certain individuals. To do so, we examined differential response to BA and BMI in a clinical trial with high fidelity to the two interventions, low attrition rates, and high participant satisfaction (Borsari et al., 2012). Two sets of analyses were conducted to examine the utility of three different types of variables in predicting response to two interventions (BA and BMI). First, we first examined which screening variables (risky drinking, gender, age of first drink, sensation seeking), alcohol-related cognitions (alcohol expectancies, perceived descriptive norms, reasons for limited drinking, costs and benefits of change), and mandated student profile (‘Bad Incident’, ‘So What’, and ‘Why Me?’) predicted lower risk drinking following a BA session. In the context of the stepped care trial, lower risk drinking was defined as 3 or fewer heavy drinking episodes and 4 or fewer alcohol-related consequences in the past month. Second, we conducted moderation analyses to identify the certain conditions under which BMI may be more effective than AO in reducing alcohol use over 3, 6 and 9 month follow-ups. The non-significant differential effects across the BMI and AO conditions in alcohol use provide a compelling rationale for moderation analyses incorporating a subset of the screening variables, alcohol-related cognitions, and mandated student profile. Placed in the larger context, this study will improve our understanding of which students may be more responsive to two commonly delivered interventions of different length and complexity.
Method
Design
This study implemented stepped care with undergraduate students age 18 years and older who violated campus alcohol policy at a four-year college in the Northeast US (Borsari et al., 2012). There were two steps of intervention. All participants received Step 1, a peer-delivered BA session. Mandated students who reported continued risky alcohol use six weeks after the BA session were randomized by computer to (a) Step 2, a 60–90 minute BMI or (b) assessment only control (AO). Participants then completed 3, 6 and 9 month follow-ups via internet (Figure 1).
Figure 1.
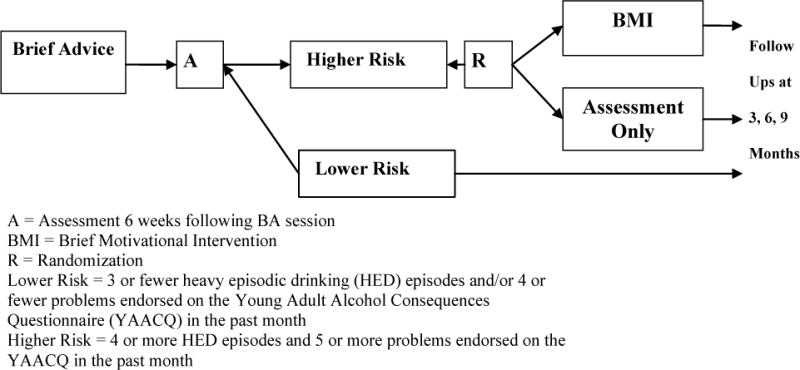
Randomized Clinical Trial Implementing Stepped Care for Mandated College Students
Participants
Prospective participants (N = 982) had been referred to the student health office (SHO) for mandatory counseling following adjudication by campus judicial affairs staff. Of these students, 598 (61%) agreed to participate in the research study and provided informed consent. Students who declined to participate (n = 384) in the project received treatment as usual from the SHO, consisting of a 15–30 minute individual discussion of their referral incident and alcohol use. The majority of those who refused to participate (70%) cited time constraints as their reason (the baseline assessment and intervention took 20–30 minutes longer than treatment as usual). Participants received $15 for the baseline assessment, $40 for the 6-week assessment, and $25, $35 and $60 for the 3, 6 and 9-month assessments, respectively. The University Institutional Review Board of the study site approved all procedures.
Interventions
Step 1: Brief Advice (BA)
The manualized BA was administered by a trained SHO peer (i.e., fellow undergraduate college student) counselor and lasted approximately 15 minutes. The peer counselor facilitated discussion of the events leading to the referral incident, the reactions of friends and family, and any changes the student had made to his or her drinking as a result. The peer counselor also provided a 12-page booklet containing educational information (from Cunningham, Wild, Bondy, & Lin, 2001). The BA session was mostly didactic, but the peer counselors did solicit personal information from participants often using open-ended questions. Throughout the session, participants were given the opportunity to ask questions or discuss their personal alcohol use with the peer counselor.
Assignment to Step 2
Consistent with a stepped care strategy, the tailoring variables in this project were heavy episodic drinking (HED) episodes and alcohol-related problems.1 The decision rule was that higher risk students (reporting 4 or more HED episodes and/or 5 or more alcohol-related consequences in the past month) were randomized to receive AO or Step 2 (BMI). Participants reporting lower risk drinking (3 or fewer HED episodes and/or 4 or fewer alcohol-related consequences in the past month) were provided no additional intervention.
Step 2: Brief Motivational Intervention (BMI)
Adapted from previous interventions with college students (Dimeff, Baer, Kivlahan, & Marlatt, 1999), this manualized BMI has resulted in significant reductions in alcohol use and problems with mandated and non-mandated students in other trials (Borsari & Carey, 2000, 2005; Carey et al., 2009; Hustad, Mastroleo, et al., 2014). The BMIs were delivered by 11 interventionists who were PhD students or postdoctoral fellows. At the beginning of the BMI, the participant was given a personalized feedback report of his/her responses to the baseline and six-week follow-up, including normative quantity/frequency of drinking, BAC and tolerance, alcohol-related consequences, influence of setting on drinking, and alcohol expectancies. Throughout the BMI, which lasted approximately 45–60 minutes, interventionists followed the four principles of Motivational Interviewing (MI): express empathy, develop discrepancy, roll with resistance, and support self-efficacy for change (see Miller & Rollnick, 2002).
Measures
Alcohol use
Both tailoring variables for the decision rules and outcome variables were obtained using the Alcohol and Drug Use Measure (Borsari & Carey, 2000, 2005). The tailoring variable for response to the BA session was number of HED episodes obtained using a gender-specific question that asked participants to report the number of times they consumed 5 or more drinks for males (4+ for females) in the past month. The maximum number of drinks consumed during the past month and the amount of time spent drinking during this episode to calculate the students’ estimated peak BAC (pBAC), using the Matthews & Miller (1979) equation and an average metabolism rate of 0.017 g/dL per hour. pBAC and HED were used as an outcome variables in the moderation analyses.
Alcohol-related consequences
Alcohol-related consequences were used as a tailoring variable and were assessed by the 48-item Young Adult Alcohol Consequences Questionnaire (YAACQ; Read, Kahler, Strong, & Colder, 2006). Dichotomous items (yes/no) were summed for a total number of alcohol-related consequences experienced in the past month. The YAACQ demonstrated high internal consistency in this sample (α = .94 at six week assessment).
Screening variables
Risky drinking at baseline was assessed by the Alcohol Use Disorders Identification Test (AUDIT; Saunders, Aasland, Babor, De La Fuente, & Grant, 1993). The AUDIT is a 10-item questionnaire assesses quantity and frequency of alcohol use as well as concerns of others regarding one’s drinking, and scores on the AUDIT can range from 0 to 40 (higher scored indicate riskier drinking). The AUDIT is commonly used as a screening tool with mandated college students (e.g., DeMartini & Carey, 2012) and exhibited good internal consistency with this sample (α = 0.75). We also assessed gender and recorded age of first drink by asking the student when he/she first started drinking, not counting small tastes or sips of alcohol (e.g., Grant & Dawson, 1997). Sensation seeking was measured by the Brief Sensation Seeking Scale-4 (BSSS-4; Stephenson et al., 2003), a 4-item true/false measure derived from the 80-item BSSS (Hoyle, Stephenson, Palmgreen, Pugzles Lorch, & Donohew, 2002), which determines the extent to which the participant engages in or would like to engage in activities that provide novel or intense sensations or experiences. The BSSS-4 demonstrated good internal consistency in this study at baseline (α = .80) and 6-week assessment (α = .79).
Alcohol-related cognitions
Alcohol expectancies were assessed using the Brief Comprehensive Effects of Alcohol Scale (Ham, Stewart, Norton, & Hope, 2005), a 15-item measure assesses valuations (i.e., the extent to which a student believes a certain effect to be ‘good’ or ‘bad’) of both positive (e.g., “I would act sociable”) and negative (e.g., “I would feel dizzy”) alcohol expectancies. Students reported valuations of these expectancy outcomes using a 5-point scale (1 = Bad to 5 = Good) and computed mean positive (α = .82) and negative (α = .83) valuations for each participant. This measure has also been used with mandated students (Borsari, O’Leary Tevyaw, Barnett, Kahler, & Monti, 2007). Descriptive norms were assessed using the Drinking Norms Rating Form (Baer, Stacy, & Larimer, 1991), a 3-item measure recorded the participants’ estimates of their own weekly alcohol consumption, as well as that of close friends and the typical student at the college. In this study, we created difference scores of personal alcohol consumption minus perceived norms for close friend and the typical student. The Reasons for Limited Drinking Scale (RLD; Greenfield et al., 1989) is a 19-item measure that assesses four reasons for regulating alcohol use: self-control (e.g., concern about alcohol-related problems), upbringing (e.g., religion discourages drinking), self-reform (e.g., seeing negative consequences in others) and performance (e.g., cognitive or motor impairments). Participants answer the items on a 4 point scale ranging from (0) not applicable to (3) very important. This measure demonstrated good reliability in this sample at baseline (α = .87) and 6-week assessment (α = 89). Finally, the students’ perceptions of the costs and benefits of change was measured using the Alcohol and Drug Consequences Questionnaire (ADCQ; Cunningham, Sobell, Gavin, Sobell, & Breslin, 1997), a 29-item measure that assesses the costs and benefits of changing personal alcohol use. There are two scales, costs (14 items) and benefits (15 items). Participants are asked to rate each item (e.g., “I will have difficulty relaxing”) on a scale ranging from not important (1) to extremely important (5); items may also be determined as not applicable (0). Excellent internal consistency was evident for both costs (baseline α = .92; 6-week α = .93) and benefits (baseline α = .91; 6-week α = .93) scales. In this study, we used the difference (benefits minus costs) to represent a single measure of whether the participant saw more benefit (positive sum) or costs (negative sum) to reducing their alcohol use.
Mandated student profile
Using methods identical to previous work (Barnett et al., 2008), we used baseline data to conduct a cluster analysis (Johnson & Wichern, 1998) to classify mandated students on the basis of five standardized variables (number of HED episodes and the number of alcohol-related problems in past month, number of drinks consumed on the day of the referral incident, and perceived responsibility and aversiveness of the referral incident). Differences among the profiles were examined using ANOVA and Scheffe pairwise comparisons and approximated those developed in Barnett et al. (2008) in several ways. First, the ‘Bad Incident’ (n = 116) profile reported lowest past month alcohol use and problems, moderate number of drinks during the incident, and highest incident responsibility and aversiveness. The ‘Bad Incident’ profile also reported a large proportion of higher-risk referrals such as vandalism and being drunk in public (21%) as well as being medically evaluated for intoxication or sent to an emergency room (both 2%). Second, participants assigned to the ‘So What?’ profile (n = 169) reported the highest past month drinking and problems, highest drinks on the night of the incident, highest level of responsibility for the incident, yet lower aversiveness. Most of the referrals for ‘So What?’ students tended to be of alcohol possession (90%) and higher-risk referrals such as vandalism and drunk in public (8%). Finally, the ‘Why Me?’ (n = 242) profile reported low rates of past-month drinking and problems, lowest number of drinks on the night of the incident, and low levels of responsibility aversiveness. The majority of their offenses were possession (75%) or being in the presence (21%) of alcohol.
Data Analysis
For our first analysis, we conducted a multivariate logistic regression model predicting the odds of reporting lower risk drinking after the BA session (i.e., reporting fewer than 3 HED episodes and/or a score of 4 or less on the YAACQ). Putative predictors were screening variables (gender, AUDIT scores, age of first drink, sensation seeking), alcohol-related cognitions (descriptive norms, alcohol expectancies, reasons for limiting drinking, and costs and benefits of change) and the mandated student profile (‘Bad Incident’, ‘So What?’, ‘Why Me?’). The proposed predictors, assessed at baseline, were additionally examined with means, standard deviations, and frequencies.
Our second analysis examined moderation of BMI’s effect on alcohol use (HED and pBAC). These moderation analyses were conducted only with the students who met risky drinking criteria at 6 weeks and who completed at least one 3, 6 and 9 month follow-up (i.e., non-BA responders; approximate ns: BMI = 184, AO = 180) and incorporated the same variables as in our first analysis, with three exceptions. Specifically, we did not examine AUDIT scores, descriptive norms and expectancies as moderators, as these were explicitly addressed in the context of the BMI and are therefore more appropriately conceptualized as mediators of BMI effects (Apodaca & Longabaugh, 2009; Borsari & Carey, 2000, 2005). Furthermore, moderator variables were measured at the six-week follow up (prior to the Step 2 BMI), with the exception of gender, age at first drink, and mandated student profile (which were assessed at baseline). Moderator analyses were conducted using Generalized Estimating Equations (GEE; Liang & Zeger, 1986) using models described by Aiken and West (1991) that included the independent and moderator variable effects as well as a multiplicative term for their interaction. If moderation effects were detected, BMI and AO effects were examined at specified time points (3, 6 and 9 months). GEE models covaried the time 1 (6-week assessment occurring before the BMI session) value of the dependent variable, and were conducted using Gaussian distributional assumptions and an autoregressive (AR1) correlation structure. All analyses were conducted in SPSS v. 20.0.
Results
Sample
Participants were 67% male, 96% Caucasian, and 68% freshman with a mean age of 18.68 (SD = 0.78). They were cited for possession of alcohol (78.18%), being in the presence of alcohol (12.14%), alcohol-related behavior (9.30%), and alcohol-related medical complications (0.38%). All 598 students who agreed to participate completed a 45-minute baseline assessment immediately prior to receiving the Step 1 BA. Of those 598 students, 582 successfully completed the 6-week follow up web assessment (95%), and 102 were designated low risk and 462 were designated high risk. Fifty-seven students were assigned to the BMI or AO during the summer months (see Borsari et al., 2014), and the remaining 405 participants were assigned to BMI (n = 211) or AO (n = 194).
Predictors of Lower Risk Drinking Following a BA Session
As can be seen in Table 1, participants with higher baseline AUDIT scores were less likely to report lower risk drinking (OR = 0.831; 95% CI: 0.76–0.91) six weeks following the BA session, and participants reporting more benefits than costs to changing their alcohol use (OR = 1.022; 95% CI: 1.006–1.039) were more likely to report lower risk drinking following a BA session. In addition, compared to the ‘Bad Incident’ profile, mandated students assigned to the ‘So What?’ and ‘Why Me?’ profiles were less likely to report lower risk drinking following a BA session (OR = 0.188; 95% CI: 0.050–0.07 and OR = 0.251; 95% CI: 0.12–0.51, respectively). All remaining predictors were non-significant.
Table 1.
Logistic regression predicting lower-risk drinking six weeks after brief advice session
| Predictors | B (se) | p | Odds Ratio | 95% CI |
|---|---|---|---|---|
| Screening Variables | ||||
| AUDIT | −0.185 (.045) | <0.001 | 0.831 | (0.760, 0.908) |
| Gender | −0.512 (.289) | 0.077 | 0.599 | (0.340, 1.056) |
| Age of first drink | −0.076 (.086) | 0.376 | 0.927 | (0.783, 1.097) |
| Sensation seeking | −0.006 (.040) | 0.874 | 0.994 | (0.920, 1.074) |
| Alcohol-Related Cognitions | ||||
| Costs and Benefits of Change | 0.022 (.008) | 0.007 | 1.022 | (1.006, 1.039) |
| Reasons for Limiting Drinking | 0.005 (.013) | 0.685 | 1.005 | (0.980, 1.032) |
| Expectancies | ||||
| Positive | 0.002 (.023) | 0.935 | 1.002 | (0.957, 1.049) |
| Negative | 0.022 (.026) | 0.396 | 1.022 | (0.972, 1.076) |
| Descriptive Norms | ||||
| Close friend | −0.018 (.014) | 0.183 | 0.982 | (0.956, 1.009) |
| Average student | 0.006 (.011) | 0.615 | 1.006 | (0.983, 1.029) |
| Mandated Student Profile | ||||
| Student profile – Bad Incident? 1 | — | — | — | — |
| Student profile – So What? | −1.674 (.673) | 0.013 | 0.188 | (0.050, 0.701) |
| Student profile – Why Me? | −1.384 (.358) | <0.001 | 0.251 | (0.124, 0.505) |
Notes. N = 570. AUDIT = Alcohol Use Disorders Identification Test. Positive Costs and Benefits of Change sum indicative of perceiving more benefits of change.
Bad Incident student profile is the reference group.
Moderators of BMI Effects
Moderator analyses showed that gender, age of first drink, sensation seeking, costs and benefits of change, and reasons for limited drinking did not significantly moderate the impact of BMI relative to AO over time on HED and pBAC (all ps > .05). However, GEE results showed a moderation effect for mandated student profile. Students that belonged to the ‘Bad Incident’ profile had the greatest increase in HED when assigned to BMI (B = 1.63 [.77], p = .04). Figure 2 demonstrates the difference in HED between the BMI and AO groups by mandated student profile at 9 month follow-up. For covariate effects across all models, the 6-week value of the outcome variable was positively associated with greater alcohol use (Brange= .47–1.22; ps < .001).
Figure 2.
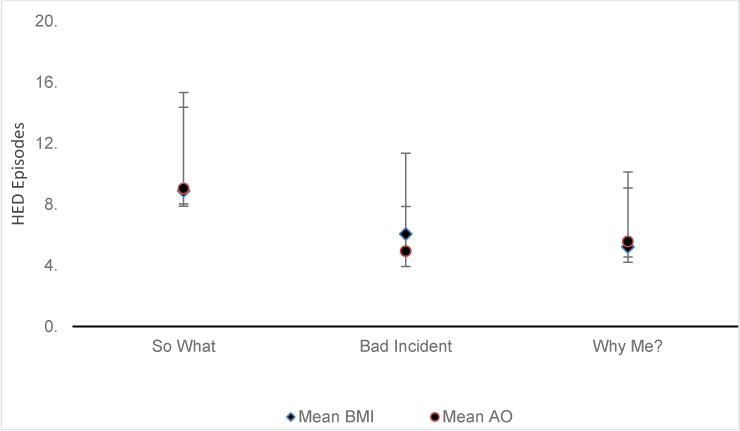
Difference between Brief Motivational Intervention (BMI) and Assessment Only (AO) groups on 9-month heavy episodic drinking (HED) episodes by mandated student profile.
Discussion
To our knowledge, this study represents the first attempt to systematically identify which mandated students may respond best to sequentially-administered BA and/or BMI. As has been posited previously (Barnett et al., 2008; Borsari & O’Leary Tevyaw, 2005), the lower-risk drinking exhibited by approximately 20% of the participants six weeks after a BA session indicates that all mandated students do not require an intensive BMI to reduce their alcohol-related problems. Thus, these findings can assist school administrations in strategically allocating their clinical resources by careful consideration of which mandated students respond to BA and/or BMI.
Regarding response to the BA session, students with lower AUDIT scores and perceiving more benefits than costs to reducing their drinking were less likely to be eligible for a more intensive Step 2 BMI when they were assessed six weeks later. These findings intuitively indicate that BA may be particularly useful for those who are drinking less and already see the benefits of reducing alcohol use. Furthermore, the lack of descriptive norms and expectancies in predicting lower risk drinking following the BA session suggests that these constructs may be best conceptualized as mediators of intervention effects. This would be consistent with recent research showing that mandated students who had higher close friend norms were less likely to reduce their drinking regardless of alcohol sanctions than students who perceived lower close friend norms (Merrill, Carey, Reid, & Carey, 2014). Therefore, these alcohol cognitions may need to be explicitly addressed in the context of the intervention in order to be linked to outcome. Regarding moderation of BMI effects on alcohol use, none of the screening or alcohol-related cognitions significantly moderated BMI effects on HED or pBAC over the 9 month follow-up.
Perhaps the most compelling finding is the differential response of the ‘Bad Incident’ profile to the BA and BMI. Namely, students in the ‘Bad Incident’ group were more likely to respond to the BA session (38% reported lower risk drinking) than those in the ‘Why Me?’ and ‘So What?’ groups (6% and 4%, respectively). Considered in the context of research indicating that a significant subset of mandated students reduce their alcohol use on their own prior to intervention or that they require very little additional intervention (Carey et al., 2009; Hustad et al., 2011; Morgan, White, & Mun, 2008), these findings suggest that a peer-led brief advice session may be an appropriate intervention for a considerable number of mandated students who are light drinkers and/or have significantly reduced their use as a result of the referral incident. Indeed, there has also been increased understanding of what aspects of the referral incident can contribute to these reductions. For example, in a 6 month prospective study of over 2200 college students, Wray, Simons and Dvorak (2011) found that students who were light drinkers did not change their drinking following an infraction. The authors posited that as these students were already drinking lightly, the infraction did not result in a reconsideration and change of personal alcohol use. For the heavy drinkers, however, those most likely to reduce their alcohol use following an alcohol infraction reported higher sensitivity to punishment, indicating that the referral incident was viewed as aversive and led to subsequent changes in drinking behaviors. Likewise, Qi et al. (2014) found high levels of incident aversiveness and personal responsibility were linked with higher readiness to change drinking following the incident, while Mastroleo et al. (2011) found that students who reported low levels of aversiveness to the referral incident reported higher levels of alcohol use following a booster session addressing their alcohol use. This research, combined with the findings of this study, suggest a multi-faceted profile can have clinical utility in identifying which mandated students could benefit from more intensive treatment.
The students in the ‘Bad Incident’ group who received a BA and then a more intensive BMI demonstrated increased heavy episodic drinking compared to those assigned to the assessment-only group at the 9 month follow-up. In contrast, there were no moderation effects evident in the other two profiles that were less likely to respond to the BA. This response by ‘Bad Incident” (and lighter drinkers) to a personalized BMI contradicts results from a recent integrated data analysis (IDA) of 24 independent trials administering BMIs to over 6,000 college students, 18% of which were mandated students (Ray et al., 2014). Findings indicated that BMI efficacy at longer term-follow-ups (6–12 months) is linked to an interaction between the number of topics addressed during a BMI and the degree to which the feedback was personalized to reflect the student’s own situation. Specifically, reductions in alcohol use are greater following BMIs that either (a) provide highly personalized information on a large number of topics or (b) provide more generic information on a fewer number of topics. In this study, ‘Bad Incident’ students increased their alcohol use following a professionally-delivered BMI with a large number of highly personalized feedback topics (including comparison to national and campus norms, self-reported consequences at baseline as well as 6-week assessment).
We can only speculate why there were increases in heavy episodic drinking in this subset of ‘Bad Incident’ students. Although there were no significant changes in alcohol use over the 9-month follow-up by participants in the BMI and AO groups, supplemental analyses indicated that the ‘Bad Incident’ students reported significantly lower rates of drinking and alcohol-related problems at the 6-week assessment than students in the other two profiles. Therefore, delivering a BMI to individuals who were slightly above the drinking cutoffs implemented in the stepped care design may have resulted in reactance to the intervention. Although examination of satisfaction ratings of the BMI revealed no significant differences among the three profiles, the personalized feedback in the BMI may have affirmed maintaining the status quo (i.e., not changing alcohol use) rather than facilitating motivation to change. In this context, and following a BA session, perhaps ‘Bad Incident’ students may have found the personalized feedback as irrelevant or unconvincing – especially if significant reductions had occurred following the incident. Such a reaction to the BMI may be akin to the iatrogenic effects observed when conducting a decisional balance exercise with an individual already motivated to reduce drinking (Miller & Rose, 2013).
Regarding clinical implications of these findings, the variables that predicted lower risk drinking following the peer-led BA or moderated the effects of a professionally delivered BMI may be useful in identifying students that may be more receptive to the interventions provided. That said, one could argue that the significance of AUDIT scores, proposes a simpler and more intuitive rule of thumb – provide the heavier drinkers with a BMI. Yet, simply using alcohol consumption and related problems as a referral strategy might not be as clinically useful as other constructs. In addition, the moderators of treatment response can be a focus of the BMI sessions and perhaps be more relevant and of intrinsic interest to the student than focusing solely on drinking and consequences assessed by the AUDIT or other measures. Efforts to balance the personalization as well as number and content of feedback topics will be informed by previously mentioned work by Ray and colleagues (2014) and other research reporting that college students’ (especially heavier drinkers) least favorite feedback topics were personal drinking profile and didactic information about alcohol (Miller & Leffingwell, 2013).
This study should be considered in the context of some limitations. First, the cutoffs determining lower risk drinking were developed by the authors, limiting the generalizability of these findings to future applications of stepped care with mandated students using more (or less) stringent decision rules for assignment to more intensive interventions. The lack of response of the ‘Bad Incident’ students to the more intensive BMI may have been an artifact of using solely alcohol use and problems as tailoring variables. Perhaps using an empirically derived and multi-faceted profile may be more efficient (e.g., target those individuals reporting low averseness/responsibility for incident in addition to risky alcohol use). Second, the lack of a non-BA comparison group precludes our ability to state how much the BA contributed to the lower risk drinking observed, and it is possible that some participants who were below the cutoff at Step 2 had not been above it at baseline. Third, the sample was predominately White and was recruited from a small college in the Northeast. Therefore, findings may not generalize to schools with different demographic characteristics and/or campuses with different alcohol policies and enforcement strategies. Fourth, although there is little evidence of significant under- or over-reporting of alcohol use in mandated students (Borsari & Muellerleile, 2009), self-report was not confirmed by collaterals.
Study findings also suggest promising directions for future research. First, variability in the direction of results by outcome (i.e., alcohol) underscores the complexity of evaluating the response to sequentially delivered interventions of different length and content as required in stepped care. Therefore, a task for future studies will first be to gain greater clarity in determining who best responds to what intervention when, in mandated students as well as other populations. Second, an analysis of what actually is occurring in the BA and BMI sessions may be enlightening to understand the changes (or lack thereof) following intervention. Coding therapist and client language, and linking these interactions to subsequent behavior change, may be one way to better understand the mechanisms of change. Although there have been recent efforts to code BMIs with mandated college students (Apodaca et al., 2014; Mastroleo, Magill, Barnett, & Borsari, 2014), several research questions remain. For example, process coding the peer-delivered BA sessions would be compelling, as efficacy studies have shown that the same peer-delivered BMI utilized in this study significantly reduced alcohol consumption and negative consequences with volunteer (Larimer et al., 2001; Mastroleo, Turrisi, Carney, Ray, & Larimer, 2010) and mandated (Mastroleo et al., 2014) students. Although effective in reducing drinking with college students, the use of peers as intervention agents has gained surprisingly little attention in the literature. Furthermore, the manner in which peer counselors interact and are accepted by the students with whom they work is unknown. Fromme and Corbin (2004) reported that professional counselors consistently had better ratings of intervention delivery than peer counselors, however the intervention was a multi-component group intervention, not BMI. In the current study, a peer-led BA session did not lead to reductions in risky drinking for a considerable number of mandated students in the ‘So What’ and ‘Why Me?’ profiles. Comparison of in-session processes by student profiles may reveal in-session differences and shed light on the observed effects, differences that were not captured by comparison of session satisfaction ratings or other self-report measures.
In summary, intervention outcomes vary according to individual characteristics. Placed in a larger context of the literature, a refinement of the stepped care decision rules is expected to enable practitioners and researchers to increase the efficiency and response following an intervention. Ideally, these results can further guide efforts to systematically combine these approaches in ways that enhance the efficiency of intervention timing, delivery, and content of intervention based on personal characteristics (e.g. AUDIT scores, perceived benefit to change alcohol use, ‘Bad Incident’ profile, and HED frequency). Placed in a larger context, the findings of the study inform the larger stepped care literature that seeks to develop a menu of efficacious yet relatively low-intensity approaches that can be widely implemented (e.g., McKellar, Austin, & Moos, 2012)
Public Health Significance Statement: Public Health Relevance Statement.
This study indicates that for mandated college students, the personal reaction to the referral event may have clinical utility in identifying which individuals benefit from treatments of varying content and intensity. In the context of stepped care, the findings provide support for the sequential delivery of two efficacious yet relatively low-intensity approaches that can be widely implemented with this at-risk population.
Acknowledgments
Brian Borsari’s contribution to this manuscript was supported by National Institute on Alcohol Abuse and Alcoholism Grants R01-AA015518 and R01-AA017874. Molly Magill’s contribution was supported by NIAAA grant K23 AA018126. Nadine Mastroleo’s contribution to this manuscript was supported by NIAAA grant T32 AA07459. John Hustad’s contribution was supported by the National Center for Research Resources and the National Center for Advancing Translational Sciences, National Institutes of Health (NIH), through grant UL1RR033184 and KL2RR033180. The authors also wish to thank Donna Darmody, Dr. John J. King, and Dr. Kathleen McMahon for their support of the project, as well as recognize all of the interventionists’ efforts. Colleen Peterson, MS was also invaluable in data management and other technical aspects of this work. The contents of this manuscript do not represent the views of the National Institute on Alcohol Abuse and Alcoholism, the Department of Veterans Affairs or the United States Government.
Footnotes
We developed a decision rule that incorporated both (a) heavy episodic drinking and (b) alcohol related problems. Regarding heavy episodic drinking, 44% of college students reported heavy episodic drinking 1–2 times per week (Wechsler et al., 2002), a level we felt would be appropriate for Step 2 (BMI). Using a distribution of the YAACQ in a non-mandated sample (Kahler, Strong, & Read, 2005), we estimated that only about 25% of the sample would report 5 or more consequences in the past month on the YAACQ and therefore appropriate for Step 2 (see Borsari et al., 2012 for more detail regarding the development of the decision rule).
References
- Aiken LS, West SG. Multiple Regression: Testing and Interpreting Interactions. Newbury Park, CA: Sage Publications; 1991. [Google Scholar]
- Apodaca TR, Borsari B, Jackson KM, Magill M, Longabaugh R, Mastroleo NR, Barnett NP. Sustain Talk Predicts Poorer Outcomes among Mandated College Student Drinkers Receiving a Brief Motivational Intervention. Psychology of Addictive Behaviors. 2014;28:631–636. doi: 10.1037/a0037296. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Apodaca TR, Longabaugh R. Mechanisms of change in motivational interviewing: A review and preliminary evaluation of the evidence. Addiction. 2009;104(5):705–715. doi: 10.1111/j.1360-0443.2009.02527.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Baer JS, Stacy A, Larimer ME. Biases in the perception of drinking norms among college students. Journal of Studies on Alcohol. 1991;52(6):580–586. doi: 10.15288/jsa.1991.52.580. [DOI] [PubMed] [Google Scholar]
- Barnett NP, Borsari B, Hustad JTP, Tevyaw TO, Colby SM, Kahler CW, Monti PM. Profiles of college students mandated to alcohol intervention. Journal of Studies on Alcohol and Drugs. 2008;69(5):684–694. doi: 10.15288/jsad.2008.69.684. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bernat DH, Lenk KM, Nelson TF, Winters KC, Toomey TL. College Law Enforcement and Security Department Responses to Alcohol-Related Incidents: A National Study. Alcoholism: Clinical and Experimental Research. 2014;38:2253–2259. doi: 10.1111/acer.12490. [DOI] [PubMed] [Google Scholar]
- Borsari B. Stepped care in the college setting. In: Correia C, Barnett N, Murphy J, editors. College Student Alcohol Abuse: A Guide to Assessment, Intervention, and Prevention. New York: Wiley; 2012. pp. 195–217. [Google Scholar]
- Borsari B, Carey KB. Effects of a brief motivational intervention with college student drinkers. Journal of Consulting and Clinical Psychology. 2000;68(4):728–733. doi: 10.1037//0022-006X.68.4.728. [DOI] [PubMed] [Google Scholar]
- Borsari B, Carey KB. Peer influences on college drinking: A review of the research. Journal of Substance Abuse. 2001;13(4):391–424. doi: 10.1016/S0899-3289(01)00098-0. [DOI] [PubMed] [Google Scholar]
- Borsari B, Carey KB. Descriptive and injunctive norms in college drinking: a meta-analytic integration. Journal of Studies on Alcohol. 2003;64(3):331–341. doi: 10.15288/jsa.2003.64.331. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Borsari B, Carey KB. Two brief alcohol interventions for mandated college students. Psychology of Addictive Behaviors. 2005;19(3):296–302. doi: 10.1037/0893-164X.19.3.296. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Borsari B, Hustad JTP, Mastroleo NR, Tevyaw TO, Barnett NP, Kahler CW, Monti PM. Addressing alcohol use and problems in mandated college students: A randomized clinical trial using stepped care. Journal of Consulting & Clinical Psychology. 2012;80(6):1062–1074. doi: 10.1037/A0029902. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Borsari B, Muellerleile P. Collateral reports in the college setting: A meta-analytic integration. Alcoholism: Clinical & Experimental Research. 2009;33(5):826–838. doi: 10.1111/j.1530-0277.2009.00902.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Borsari B, O’Leary Tevyaw T. Stepped care: A promising treatment strategy for mandated college students. Journal of Student Affairs Research and Practice. 2005;42:381–397. doi: 10.2202/1949-6605.1514. [DOI] [Google Scholar]
- Borsari B, O’Leary Tevyaw T, Barnett NP, Kahler CW, Monti PM. Stepped care for mandated college students: a pilot study. American Journal on Addictions. 2007;16(2):131–137. doi: 10.1080/10550490601184498. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Borsari B, Short EE, Mastroleo NR, Hustad JT, Tevyaw TO, Barnett NP, Monti PM. Phone-delivered brief motivational interventions for mandated college students delivered during the summer months. Journal of Substance Abuse Treatment. 2014;46(5):592–596. doi: 10.1016/j.jsat.2014.01.001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Carey KB, Henson JM, Carey MP, Maisto SA. Computer versus in-person intervention for students violating campus alcohol policy. Journal of Consulting and Clinical Psychology. 2009;77(1):74–87. doi: 10.1037/a0014281. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Carey KB, Scott-Sheldon LAJ, Carey MP, DeMartini KS. Individual-level interventions to reduce college student drinking: A meta-analytic review. Addictive Behaviors. 2007;32(11):2469–2494. doi: 10.1016/j.addbeh.2007.05.004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Collins RL, Koutsky JR, Morsheimer ET, MacLean MG. Binge drinking among underage college students: a test of a restraint-based conceptualization of risk for alcohol abuse. Psychology of Addictive Behaviors. 2001;15(4):333–340. doi: 10.1037/0893-164X.15.4.333. [DOI] [PubMed] [Google Scholar]
- Cronce JM, Larimer ME. Individual-focused approaches to the prevention of college drinking. Alcohol, Research & Health. 2011;34:210–221. [PMC free article] [PubMed] [Google Scholar]
- Cunningham JA, Sobell LC, Gavin DR, Sobell MB, Breslin FC. Assessing motivation for change: Preliminary development and evaluation of a scale measuring the cost and benefits of changing alcohol or drug use. Psychology of Addictive Behaviors. 1997;11:107–114. doi: 10.1037/0893-164X.11.2.107. [DOI] [Google Scholar]
- Cunningham JA, Wild TC, Bondy SJ, Lin E. Impact of normative feedback on problem drinkers: A small-area population study. Journal of Studies on Alcohol. 2001;62(2):228–233. doi: 10.15288/jsa.2001.62.228. [DOI] [PubMed] [Google Scholar]
- Fromme K, Corbin W. Prevention of heavy drinking and associated negative consequences among mandated and voluntary college students. Journal of Consulting & Clinical Psychology. 2004;72(6):1038–1049. doi: 10.1037/0022-006X.72.6.1038. doi: 2004-21587-014 [pii] 10.1037/0022-006X.72.6.1038. [DOI] [PubMed] [Google Scholar]
- Grant BF, Dawson DA. Age at onset of alcohol use and its association with DSM-IV alcohol abuse and dependence: Results from the National longitudinal alcohol epidemiologic survey. Journal of Substance Abuse. 1997;9:103–110. doi: 10.1016/s0899-3289(97)90009-2. [DOI] [PubMed] [Google Scholar]
- Greenfield TK, Guydish J, Temple MT. Reasons students give for limiting drinking: a factor analysis with implications for research and practice. Journal of Studies on Alcohol and Drugs. 1989;50(2):108–115. doi: 10.15288/jsa.1989.50.108. [DOI] [PubMed] [Google Scholar]
- Ham LS, Stewart SH, Norton PJ, Hope DA. Psychometric assessment of the Comprehensive Effects of Alcohol Questionnaire: Comparing a brief version to the original full scale. Journal of Psychopathology and Behavioral Assessment. 2005;27(3):141–158. doi: 10.1007/s10862-005-0631-9. [DOI] [Google Scholar]
- Helmkamp JC, Hungerford DW, Williams JM, Manley WG, Furbee PM, Horn KA, Pollock DA. Screening and brief intervention for alcohol problems among college students treated in a university hospital emergency department. Journal of American College Health. 2003;52(1):7–16. doi: 10.1080/07448480309595718. [DOI] [PubMed] [Google Scholar]
- Hoyle RH, Stephenson MT, Palmgreen P, Pugzles Lorch E, Donohew RL. Reliability and validity of a brief measure of sensation seeking. Personality and Individual Differences. 2002;32(3):401–414. doi: 10.1016/s0191-8869(01)00032-0. [DOI] [Google Scholar]
- Hustad JTP, Eaton Short E, Borsari B, Barnett NP, O’Leary Tevyaw T, Kahler CW. College alcohol citations result in modest reductions in student drinking. Journal of Substance Abuse Treatment. 2011;40(3):281–286. doi: 10.1016/j.jsat.2010.11.005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hustad JTP, Mastroleo NR, Kong L, Urwin R, Zeman R, LaSalle L, Borsari B. The comparative effectiveness of individual and group motivational intervention for mandated college students. Psychology of Addictive Behaviors. 2014;28(1):74–84. doi: 10.1037/a0034899. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hustad JTP, Pearson MR, Neighbors C, Borsari B. The role of alcohol perceptions as mediators between personality and alcohol-related outcomes among incoming college student drinkers. Psychology of Addictive Behaviors. 2014;28(2):336–347. doi: 10.1037/a0033785. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Johnson RA, Wichern DW. Applied multivariate statistical analysis. 4th. Upper Saddle River, NJ: Prentice Hall; 1998. [Google Scholar]
- Kahler CW, Strong DR, Read JP. Toward efficient and comprehensive measurement of the alcohol problems continuum in college students: the brief young adult alcohol consequences questionnaire. Alcoholism: Clinical & Experimental Research. 2005;29(7):1180–1189. doi: 10.1097/01.ALC.0000171940.95813.A5. [DOI] [PubMed] [Google Scholar]
- Kulesza M, Apperson M, Larimer ME, Copeland AL. Brief alcohol intervention for college drinkers: how brief is? Addictive Behaviors. 2010;35(7):730–733. doi: 10.1016/j.addbeh.2010.03.011. [DOI] [PubMed] [Google Scholar]
- Kulesza M, McVay MA, Larimer ME, Copeland AL. A randomized clinical trial comparing the efficacy of two active conditions of a brief intervention for heavy college drinkers. Addictive Behaviors. 2013;38(4):2094–2101. doi: 10.1016/j.addbeh.2013.01.008. [DOI] [PubMed] [Google Scholar]
- Labbe AK, Maisto SA. Alcohol expectancy challenges for college students: A narrative review. Clinical Psychology Review. 2011;31(4):673–683. doi: 10.1016/j.cpr.2011.02.007. [DOI] [PubMed] [Google Scholar]
- Larimer ME, Cronce JM. Identification, prevention, and treatment revisited: individual-focused college drinking prevention strategies 1999–2006. Addictive Behaviors. 2007;32:2439–2468. doi: 10.1016/j.addbeh.2007.05.006. [DOI] [PubMed] [Google Scholar]
- Larimer ME, Turner AP, Anderson BK, Fader JS, Kilmer JR, Palmer RS, Cronce JM. Evaluating a brief alcohol intervention with fraternities. Journal of Studies on Alcohol. 2001;62(3):370. doi: 10.15288/jsa.2001.62.370. [DOI] [PubMed] [Google Scholar]
- Lewis MA, Neighbors C. Social Norms Approaches Using Descriptive Drinking Norms Education: A Review of the Research on Personalized Normative Feedback. Journal of American College Health. 2006;54(4):213–218. doi: 10.3200/jach.54.4.213-218. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Liang K, Zeger SL. Longitudinal data analysis using generalized linear models. Biometrika. 1986;73(1):13–22. doi: 10.1093/biomet/73.1.13. [DOI] [Google Scholar]
- Mastroleo NR, Magill M, Barnett NP, Borsari B. A pilot study of two supervision approaches for peer-led alcohol interventions with mandated college students. Journal of Studies on Alcohol and Drugs. 2014;75(3):458–466. doi: 10.15288/jsad.2014.75.458. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mastroleo NR, Mallett KA, Ray AE, Turrisi R. The Process of Delivering Peer-Based Alcohol Intervention Programs in College Settings. Journal of College Student Development. 2008;49(3):255–259. doi: 10.1353/csd.0.0010. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mastroleo NR, Murphy JG, Colby SM, Monti PM, Barnett NP. Incident-specific and individual-level moderators of brief intervention effects with mandated college students. Psychology of Addictive Behaviors. 2011;25(4):616–624. doi: 10.1037/a0024508. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mastroleo NR, Turrisi R, Carney JV, Ray AE, Larimer ME. Examination of posttraining supervision of peer counselors in a motivational enhancement intervention to reduce drinking in a sample of heavy-drinking college students. Journal of Substance Abuse Treatment. 2010;39(3):289–297. doi: 10.1016/j.jsat.2010.06.005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Matthews DB, Miller WR. Estimating blood alcohol concentration: Two computer programs and their applications in therapy and research. Addictive Behaviors. 1979;4(1):55–60. doi: 10.1016/0306-4603(79)90021-2. [DOI] [PubMed] [Google Scholar]
- McKellar J, Austin J, Moos R. Building the first step: a review of low-intensity interventions for stepped care. Addict Sci Clin Pract. 2012;7(1):26. doi: 10.1186/1940-0640-7-26. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Merrill JE, Carey KB, Lust SA, Kalichman SC, Carey MP. Do students mandated to intervention for campus alcohol-related violations drink more than nonmandated students? Psychology of Addictive Behaviors. 2014;28(4):1265–1270. doi: 10.1037/a0037710. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Merrill JE, Carey KB, Reid AE, Carey MP. Drinking reductions following alcohol-related sanctions are associated with social norms among college students. Psychology of Addictive Behaviors. 2014;28(2):553–558. doi: 10.1037/a0034743. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Miller MB, Leffingwell TR. What do college student drinkers want to know? Student perceptions of alcohol-related feedback. Psychology of Addictive Behaviors. 2013;27(1):214–222. doi: 10.1037/a0031380. [DOI] [PubMed] [Google Scholar]
- Miller MB, Leffingwell TR, Claborn K, Meier E, Walters S, Neighbors C. Personalized Feedback Interventions for College Alcohol Misuse: An Update of Walters & Neighbors (2005) Psychology of Addictive Behaviors. 2012 doi: 10.1037/a0031174. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Miller WR, Rollnick S. Motivational interviewing: Preparing people for change. 2nd. Guilford Press; 2002. [Google Scholar]
- Miller WR, Rollnick S. Motivational Interviewing: Helping People Change. Guiford Press; 2012. [Google Scholar]
- Miller WR, Rose GS. Motivational Interviewing and Decisional Balance: Contrasting Responses to Client Ambivalence. Behavioural and Cognitive Psychotherapy. 2013:1–13. doi: 10.1017/S1352465813000878. [DOI] [PubMed] [Google Scholar]
- Morean ME, Corbin WR, Fromme K. Age of first use and delay to first intoxication in relation to trajectories of heavy drinking and alcohol-related problems during emerging adulthood. Alcoholism: Clinical & Experimental Research. 2012;36(11):1991–1999. doi: 10.1111/j.1530-0277.2012.01812.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Morgan TJ, White HR, Mun EY. Changes in drinking before a mandated brief intervention with college students. Journal of Studies on Alcohol and Drugs. 2008;69(2):286–290. doi: 10.1017/S1352465813000878. [DOI] [PubMed] [Google Scholar]
- Mun EY, White HR, Morgan TJ. Individual and situational factors that influence the efficacy of personalized feedback substance use interventions for mandated college students. Journal of Consulting & Clinical Psychology. 2009;77(1):88–102. doi: 10.1037/a0014679. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Murphy JG, Duchnick JJ, Vuchinich RE, Davison JW, Karg RS, Olson AM, Coffey TT. Relative efficacy of a brief motivational intervention for college student drinkers. Psychology of Addictive Behaviors. 2001;15(4):373. doi: 10.1037//0893-164X.15.4.373. [DOI] [PubMed] [Google Scholar]
- Palfai TP, Ralston TE. Life goals and alcohol use among first-year college students: the role of motives to limit drinking. Addictive Behaviors. 2011;36(11):1083–1086. doi: 10.1016/j.addbeh.2011.06.005. [DOI] [PubMed] [Google Scholar]
- Pearson MR, Hustad JT. Personality and alcohol-related outcomes among mandated college students: Descriptive norms, injunctive norms, and college-related alcohol beliefs as mediators. Addictive Behaviors. 2014;39(5):879–884. doi: 10.1016/j.addbeh.2014.01.008. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Perkins HW. The Social Norms Approach to Preventing School and College Age Substance Abuse. San Francisco: Jossey-Bass; 2003. [Google Scholar]
- Qi D, Pearson MR, Hustad JTP. Predictors of motivation to change in mandated college students following a referral incident. Psychology of Addictive Behaviors. 2014;28(2):524–531. doi: 10.1037/a0035910. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Quinn PD, Stappenbeck CA, Fromme K. Collegiate heavy drinking prospectively predicts change in sensation seeking and impulsivity. Journal of Abnormal Psychology. 2011;120(3):543. doi: 10.1037/a0023159. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ray AE, Kim SY, White HR, Larimer ME, Mun EY, Clarke N, Huh D. When Less Is More and More Is Less in Brief Motivational Interventions: Characteristics of Intervention Content and Their Associations With Drinking Outcomes. Psychology of Addictive Behaviors. 2014;28:1026–1040. doi: 10.1037/a0036593. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Read JP, Kahler CW, Strong DR, Colder CR. Development and preliminary validation of the young adult alcohol consequences questionnaire. Journal of Studies on Alcohol. 2006;67(1):169–177. doi: 10.15288/jsa.2006.67.169. [DOI] [PubMed] [Google Scholar]
- Saunders JB, Aasland OG, Babor TF, De La Fuente JR, Grant M. Development of the Alcohol Use Disorders Identification Test (AUDIT): WHO Collaborative Project on Early Detection of Persons with Harmful Alcohol Consumption–II. Addiction. 1993;88(6):791–804. doi: 10.1111/j.1360-0443.1993.tb02093.x. [DOI] [PubMed] [Google Scholar]
- Schaus JF, Sole ML, McCoy TP, Mullett N, O’Brien MC. Alcohol screening and brief intervention in a college student health center: a randomized controlled trial. Journal of Studies on Alcohol and Drugs, Supplement No. 2009;16:131–141. doi: 10.15288/jsads.2009.s16.131. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Scott-Sheldon LA, Terry DL, Carey KB, Garey L, Carey MP. Efficacy of expectancy challenge interventions to reduce college student drinking: A meta-analytic Review. Psychology of Addictive Behaviors. 2012 doi: 10.1037/a0027565. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sobell MB, Sobell LC. Stepped care as a heuristic approach to the treatment of alcohol problems. Journal of Consulting & Clinical Psychology. 2000;68(4):573–579. doi: 10.1037/0022-006X.68.4.573. [DOI] [PubMed] [Google Scholar]
- Stephenson MT, Hoyle RH, Palmgreen P, Slater MD. Brief measures of sensation seeking for screening and large-scale surveys. Drug and Alcohol Dependence. 2003;72(3):279–286. doi: 10.1016/j.drugalcdep.2003.08.003. [DOI] [PubMed] [Google Scholar]
- Wechsler H, Lee JE, Kuo M, Seibring M, Nelson TF, Lee H. Trends in college binge drinking during a period of increased prevention efforts. Findings from 4 Harvard School of Public Health College Alcohol Study surveys: 1993–2001. Journal of American College Health. 2002;50:203–217. doi: 10.1080/07448480209595713. [DOI] [PubMed] [Google Scholar]
- Woicik PA, Stewart SH, Pihl RO, Conrod PJ. The substance use risk profile scale: A scale measuring traits linked to reinforcement-specific substance use profiles. Addictive Behaviors. 2009;34(12):1042–1055. doi: 10.1016/j.addbeh.2009.07.001. [DOI] [PubMed] [Google Scholar]
- Wray TB, Simons JS, Dvorak RD. Alcohol-related infractions among college students: associations with subsequent drinking as a function of sensitivity to punishment. Psychology of Addictive Behaviors. 2011;25(2):352–357. doi: 10.1037/a0023614. [DOI] [PMC free article] [PubMed] [Google Scholar]