

Abstract
Distal femoral varus osteotomy is a well-established procedure for the treatment of lateral compartment cartilage lesions and degenerative disease, correcting limb alignment and decreasing the progression of the pathology. Surgical techniques can be performed with a lateral opening-wedge or medial closing-wedge correction of the deformity. Fixation methods for lateral opening-wedge osteotomies are widely available, and there are various types of implants that can be used for fixation. However, there are currently only a few options of implants for fixation of a medial closing-wedge osteotomy on the market. This report describes a medial, supracondylar, V-shaped, closing-wedge distal femoral osteotomy using a locked anterolateral proximal tibial locking plate that fits anatomically to the medial side of the distal femur. This is a great option as a stable implant for a medial closing-wedge distal femoral osteotomy.
Osteotomies around the knee were commonly used for the treatment of unicompartmental arthritis in the early 1970s and 1980s1, 2, 3; however, as arthroplasties became popular and showed good long-term results, the number of osteotomies for the treatment of knee arthritis decreased over the next few decades in the United States. They are still frequently performed in Europe, Asia, and South America.
Distal femoral varus osteotomy (DFVO) is a well-established procedure for the treatment of lateral compartment cartilage lesions and degenerative disease.4, 5, 6, 7, 8, 9 Its objective is to change the mechanical alignment to neutral in cartilage repair procedures or to overcorrect the axis in cases of degenerative lateral compartment osteoarthritis.10
Surgical techniques such as lateral opening-wedge or medial closing-wedge correction of the deformity can also be used. A medial closing-wedge DFVO can be stabilized with either a cast or internal fixation by a blade plate.2, 6, 7, 11, 12 Osteotomies may be combined with cartilage repair procedures for neutral axial alignment of the limb. In this case, achieving the desirable degree of correction is a very difficult task, and there are few options for stabilization of the osteotomy. One of the options is to use a medial distal femoral locking plate to secure the desired correction, but these systems are not often commercially available for the medial side of the femur. We describe the use of an anterolateral proximal tibial locking plate for fixation of a supracondylar, V-shaped, medial DFVO (Video 1).
Surgical Technique
Medial closing-wedge distal femoral osteotomy is recommended for patients with valgus malalignment meeting the following criteria: cartilage lesions (femoral and/or tibial lateral compartment cartilage lesions of the knee, femoral and/or tibial localized degenerative disease, or femorotibial lateral compartment osteoarthritis); intact medial compartment cartilage and medial meniscus; age younger than 60 years; and desire to stay active (perform exercises) or play sports (Table 1). Absolute contraindications to distal femoral osteotomy are tricompartmental osteoarthritis, patellofemoral pain, and osteoarthritis or meniscal deficiency in the compartment intended for weight bearing. Relative contraindications are smoking and knee range of motion less than 90°.
Table 1.
Indications and Contraindications of Distal Femoral Varus Osteotomy
| Indications |
| Cartilage lesions |
| Femoral and/or tibial lateral compartment cartilage lesions of knee |
| Femoral and/or tibial localized degenerative disease |
| Femorotibial lateral compartment osteoarthritis |
| Intact medial compartment cartilage and medial meniscus |
| Age <60 yr |
| Desire to stay active (perform exercises) or play sports |
| Contraindications |
| Absolute |
| Tricompartmental osteoarthritis |
| Patellofemoral pain |
| Osteoarthritis or meniscal deficiency in compartment intended for weight bearing |
| Relative |
| Smoking |
| Knee range of motion <90° |
The study was approved by the hospital scientific committee, and all patients consented to participate this study. The type of implant used in this study was an anterolateral tibial plateau locking plate. The plates were obtained from 2 different manufacturers that supply implants to our hospital: 3.5-mm AxSOS proximal tibial locking plate (Stryker, Kalamazoo, MI) and 3.5- or 4.5-mm LCP proximal tibial locking plate (Synthes, West Chester, PA) (Fig 1). Right tibial implants were used in the right distal femur, and left tibial implants were used in the left distal femur.
Fig 1.

(A) Anteroposterior and (B) lateral views of Stryker 3.5-mm AxSOS proximal tibial locking plate. (C) Synthes anterolateral 4.5-mm LCP proximal tibial locking plate.
Supracondylar V-shaped DFVO is performed as described by Aglietti et al.2 in their original article. The patient is placed in the supine position, and a tourniquet is usually used. A medial-side distal femoral approach is used for this technique with the knee flexed to 60°. A 15-cm skin incision is made starting 2 cm distal to the medial femoral epicondyle and extending 13 cm proximal on the medial side. The fascia is identified and is sectioned at the border of the vastus medialis muscle by the subvastus approach. The muscle is retracted anteriorly and laterally with a Hohmann retractor, and the periosteum is cut in the distal femoral shaft.
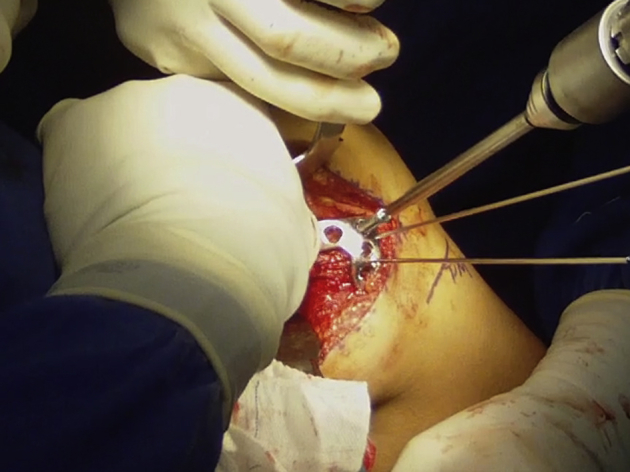
A 2.0-mm Kirschner wire (Stryker) is passed from medial to lateral on the medial epicondyle, parallel to the articular joint line, to guide the direction of the cut with a saw blade (Figs 2 and 3). A Hohmann retractor is positioned on the posterior part of the femur to protect the neurovascular structures.
Fig 2.
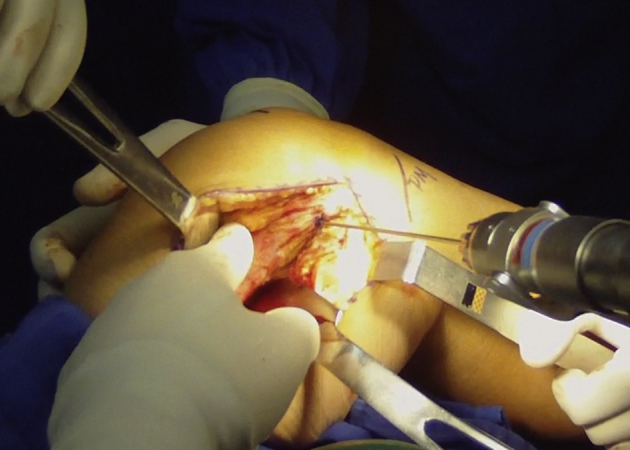
Medial view of the distal shaft of the femur and medial part of the knee. A 2.0-mm K-wire is being passed from medial to lateral on the medial epicondyle, parallel to the joint line.
Fig 3.
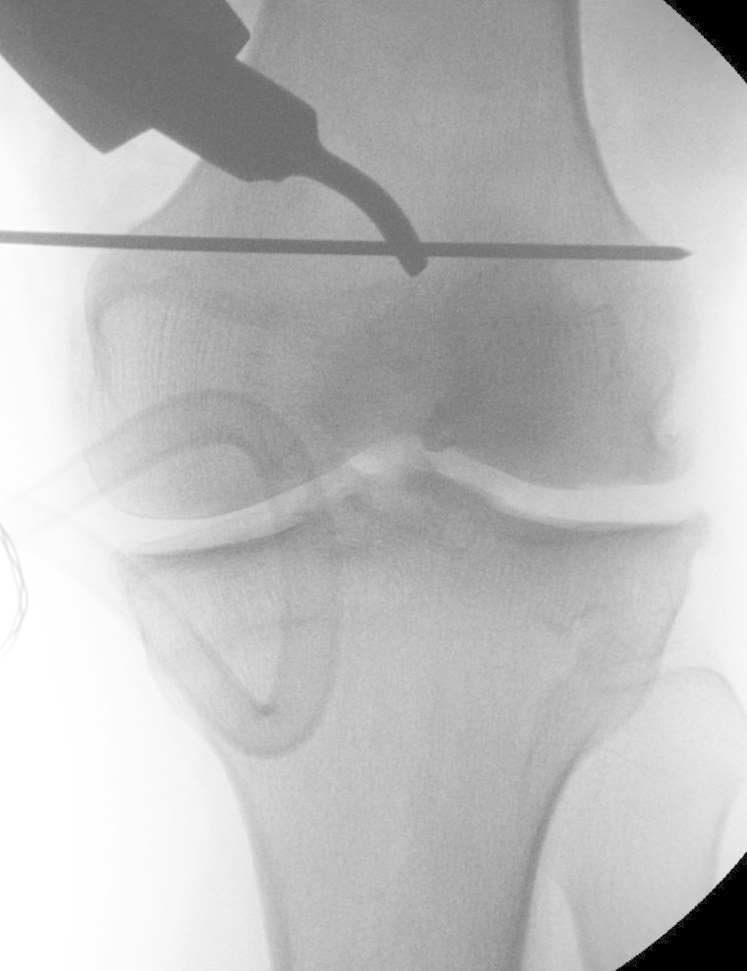
Fluoroscopic view of 2.0-mm K-wire from medial to lateral, parallel to joint line.
A chevron-type osteotomy is performed from medial to lateral, with the anterior arm having twice the length of the posterior arm (Fig 4). A saw blade is used for the anterior part of the osteotomy, and an osteotome is used for the posterior part to decrease the risk of injury to the neurovascular structures. The bone cut must be parallel to the K-wire and the articular joint line (Fig 5). Injury to the lateral femoral cortex can compromise sagittal stability. If this occurs, it must be addressed with the use of a small plate and screws or a staple.
Fig 4.

Medial approach to distal femur, showing Hohmann retractors positioned anterior and posterior to femur. The site of osteotomy is marked on the bone, with the anterior arm having twice the length of the posterior arm and with an angulation of 90° between these arms.
Fig 5.

(A) Incorrect direction of femoral saw blade cut for medial-side distal femoral varus osteotomy, oblique to K-wire (marked with a red X, meaning “wrong”). (B) Correct direction of saw blade for femoral cut, parallel to K-wire (marked with a green C, meaning “correct”).
An additional resection of 1 to 5 mm of the proximal part of the femur is performed with a saw blade to overlap the proximal part of the femur into the metaphysis of the distal part until the desired correction is achieved (Figs 6 and 7). Such impaction promotes bone apposition and rotational control of the osteotomy, improving stability (Fig 8).
Fig 6.
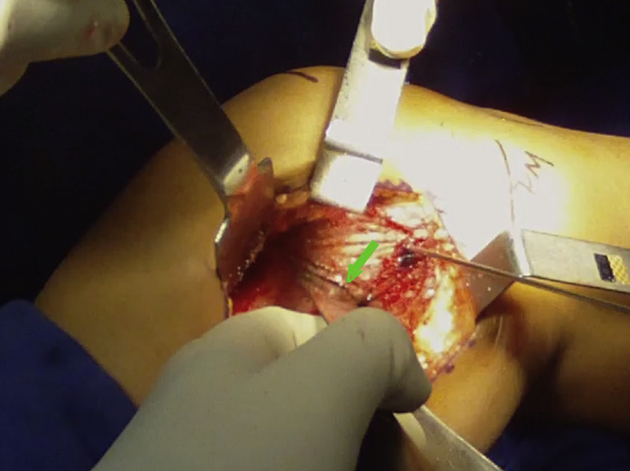
Additional resection of 1 to 5 mm of the proximal part of the femur is performed using a saw blade to overlap the proximal part of the femur into the metaphysis of the distal part until the desired correction is achieved. The arrow indicates the amount of bone resected.
Fig 7.
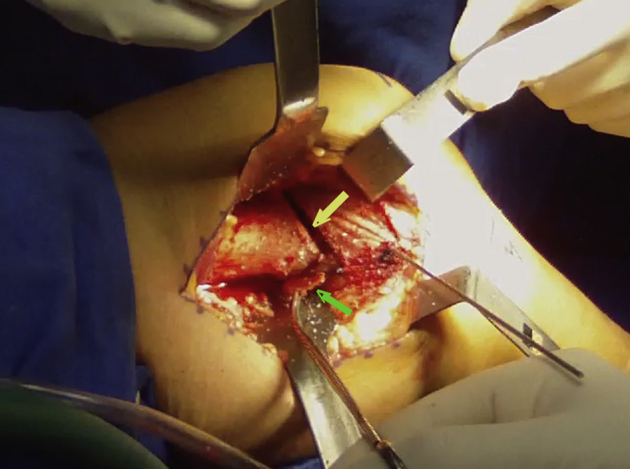
Removal of small wedge of bone from posterior part of osteotomy (green arrow). One should note the space left after removal of the wedge of bone at the anterior arm of the cut (yellow arrow).
Fig 8.

(A) Medial closing-wedge osteotomy with resection of 5 mm of proximal part of femur. (B) Overlap of proximal part of femur into metaphysis of distal part, correcting the deformity.
The plate can be bent in the middle to achieve anatomic correction of angulation (Fig 9). When the desired correction is achieved, the osteotomy is secured with a 3.5- or 4.5-mm anterolateral proximal tibial locking plate (3.5-mm AxSOS or 3.5- or 4.5-mm LCP) (Figs 10 and 11). Fluoroscopic imaging is used intraoperatively to evaluate the mechanical axis and ensure that it is appropriate (Fig 12).
Fig 9.

Bending of plate to achieve desired correction. Bending must be performed at the level of the osteotomy.
Fig 10.
Position of 4.5-mm anterolateral tibial locking plate (4.5-mm LCP proximal tibial locking plate). Fixation is achieved with two 1.0-mm K-wires and 2 locked screws in the distal part of the femoral osteotomy.
Fig 11.

Fluoroscopy is used to check the anteroposterior and lateral positioning of the plate after distal fixation with 2 screws. One should note that, on the lateral view, the most posterior hole in the distal part of the plate remains without a screw so as not to violate the intercondylar notch.
Fig 12.

(A) Assessment of mechanical alignment with bovie cord after complete fixation of osteotomy. (B) Fluoroscopic view of final construct and bovie cord showing the final alignment on the medial tibial eminence.
Three locked screws are used to secure the plate to the distal part of the femur, and 2 locked screws are placed in the proximal part (Table 2). Additional oblique screws can be used if additional stability is desired (Figs 13 and 14, Video 1).
Table 2.
Pearls, Pitfalls, and Complications of Medial Closing-Wedge Distal Femoral Osteotomy
| Pearls and pitfalls |
| The surgeon should try to obtain good exposure of the medial part of the distal femur from 2 cm distal to 10 to 15 cm proximal to the medial epicondyle. |
| A 2.0-mm K-wire is drilled from medial to lateral on the medial epicondyle, parallel to the articular joint line. |
| The saw blade should be parallel to the K-wire. The surgeon should not cut the bone with the saw blade perpendicular to the distal femur (oblique with the K-wire). Doing so will lead the saw blade into the intercondylar notch, and a fracture of the condyle may occur. |
| The anterior arm of the osteotomy has double the length of the posterior arm. |
| Violation of the lateral cortex of the femur requires an additional fixation on the lateral side. |
| The surgeon should remove 1 to 5 mm of bone from the proximal part of the femur. This will allow the distal part of the femur to overlap the proximal part until the desired correction is achieved. The surgeon should make sure that this small wedge of bone is removed all the way anteriorly and posteriorly; otherwise, it might break the lateral cortex when reducing the valgus deformity. |
| Usually, 3 locked screws distally and 2 locked screws proximally are sufficient for securing the locking plate to the distal femur, maintaining angular correction and stability. |
| The most posterior hole in the distal part of the locking plate remains without a screw so as not to violate the intercondylar notch. A short screw can be used to increase stability if desired. |
| Complications |
| Neurovascular injury |
| Nonunion (violation of lateral cortex) |
| Fracture of condyle |
| Deep infection |
| Failure to properly correct alignment |
| Hematoma |
| Compartment syndrome |
Fig 13.

(A) Anteroposterior radiograph showing 3.5-mm plate fixation with lock and cancellous screws. (B) Lateral radiograph showing positioning of plate anterior to Blumensaat line and proximal to trochlea. (C) Axial radiograph showing perfect anatomic position of plate in medial part of distal femur.
Fig 14.

(A) Long-leg anteroposterior radiograph showing preoperative valgus deformity of the right knee in a patient with a lateral femoral condyle osteochondral lesion. (B) Postoperative long-leg radiograph with an anterolateral proximal tibial locking plate on the medial side of the distal femur, showing correction of the mechanical axis of the limb to neutral alignment.
A drain is then inserted, and the wound is closed in layers. A compressive dressing is applied, and the leg is placed in a hinged knee brace with toe-touch weight bearing for 2 weeks and partial weight bearing until 6 weeks after the procedure.
Discussion
Femoral osteotomies work well for realignment of the limb with a valgus deformity.13 The degree of correction may vary depending on the progression of disease at the time of treatment.
When a DFVO is combined with a cartilage repair procedure, the aim of the correction is neutral alignment of the limb. If there is mild degenerative disease in the compartment that is being treated, the mechanical axis should be a few degrees beyond neutral alignment, with overcorrection to the tibial eminence opposite the defect. If we are treating a patient with advanced degenerative disease, we may correct to neutral or overcorrect the axis to unload the degenerated compartment (Table 3).14, 15
Table 3.
Desired Correction With Distal Femoral Osteotomy for Malalignment in Cartilage Lesions
| Pathology | Aim of Alignment |
|---|---|
| Focal cartilage lesion treated | Neutral |
| Mild degenerative disease or cartilage lesion partially treated | Overcorrect to opposite tibial eminence |
| Osteoarthritis | Overcorrect to opposite compartment |
Lateral opening-wedge DFVO is a popular procedure with very consistent results5, 8, 16, 17, 18; however, it has the disadvantage that it requires more time for the bone to heal and often requires bone grafting to fill the gap at the osteotomy site. Moreover, because the plate is seated under the iliotibial band, it generally leads to irritation of the iliotibial band, making removal of the plate almost always necessary after bone consolidation.19
Medial closing-wedge DFVO is also a very well-established procedure for the treatment of the valgus knee; however, fixation on the medial side might be a problem if the surgeon does not want to take the anatomic axis to neutral using an AO 90° blade plate. Many authors who perform medial closing-wedge DFVO use a 90° blade plate for fixation of the osteotomy.3, 11, 20, 21, 22 There is a problem when the surgeon uses a 90° plate in cartilage repair procedures and wants to correct the mechanical axis to physiological neutral alignment (i.e. bringing the mechanical axis, but not anatomic axis, to 0°). In this scenario, it is extremely difficult to achieve the desired correction using the 90° blade plate.
Locking plates are widely used for intra-articular fractures, tibial osteotomies, and lateral femoral osteotomies. Locking plates have the advantage of increasing stability and reducing the period of partial weight bearing during recovery.4 Brinkman et al.23 compared axial and torsional stability using 5 different plates and osteotomy configurations in lateral and medial DFVO and concluded that lateral opening-wedge techniques were less stable and less stiff than medial techniques. Locking plates are often used in lateral and medial DFVO; however, there are only a few implants designed to be used on the medial side of the distal femur, and they are not always available in many countries. The only locking plate design for the medial distal femur is the Synthes TomoFix medial distal femoral plate, which is currently unavailable in Brazil and in many other countries.
An anterolateral proximal tibial locking plate fits perfectly into the medial cortex of the distal femur, making it a good option for fixation by medial closing-wedge DFVO. It has the advantage of allowing gradual corrections of the mechanical axis of the limb by bending the plate. This facilitates the surgical procedure and better achieves the planned correction (Fig 7). After the desired correction is achieved, the surgeon can perform temporary fixation with K-wires and then lock the plate with screws. The disadvantages of medial-side osteotomy are the proximity to the popliteal vessels, the fact that it is technically more demanding, and the lack of implant choices available on the market (Table 4).
Table 4.
Comparison of Advantages and Disadvantages of Lateral Opening-Wedge and Medial Closing-Wedge Osteotomies
| Femoral Varus Osteotomy | Advantages | Disadvantages |
|---|---|---|
| Lateral opening wedge | Potentially simpler | Irritation of iliotibial band |
| Several types of fixation | Longer time to heal | |
| Avoidance of neurovascular bundle | Need for bone graft | |
| Medial closing wedge | More aggressive weight bearing | Technically more demanding |
| No need for bone graft | Proximity to popliteal vessels | |
| Lack of implants available |
We conclude that the combination of V-shaped medial closing-wedge DFVO and a locking plate enhances the stability of the osteotomy and permits a shorter period of partial weight bearing and faster recovery, making it an excellent option for the treatment of a valgus knee. Anterolateral proximal tibial locking plates are an excellent choice of fixation for medial osteotomies because they fit anatomically into the medial side of the distal femur.
Footnotes
The authors report the following potential conflict of interest or source of funding: M.K.D. receives support from Depuy Synthes, Mundipharma, Smith & Nephew, Baxter, MDT, EMS, and the Fundação de Amparo a Pesquisa do Estado de São Paulo - São Paulo Research Foundation.
Supplementary Data
Detailed surgical technique for medial closing-wedge distal femoral osteotomy with proximal tibial locking plate. The patient is placed in the supine position on the operating table, and a medial-side approach is used in the left knee. Dissection of the soft tissue is performed by the subvastus approach, and the periosteum is incised. A V-shaped distal femoral osteotomy is performed, with the anterior arm having twice the length of the posterior arm. One to 5 mm of bone is resected, and limb alignment is corrected, closing the wedge of the osteotomy. A 3.5- or 4.5-mm anterolateral tibial locking plate (3.5-mm AxSOS or 3.5- or 4.5-mm LCP proximal tibia locking plate) is used for fixation.
{kind=link}
References
- 1.Maquet P. Valgus osteotomy for osteoarthritis of the knee. Clin Orthop Relat Res. 1976:143–148. [PubMed] [Google Scholar]
- 2.Aglietti P., Stringa G., Buzzi R., Pisaneschi A., Windsor R.E. Correction of valgus knee deformity with a supracondylar V osteotomy. Clin Orthop Relat Res. 1987:214–220. [PubMed] [Google Scholar]
- 3.McDermott A.G., Finklestein J.A., Farine I., Boynton E.L., MacIntosh D.L., Gross A. Distal femoral varus osteotomy for valgus deformity of the knee. J Bone Joint Surg Am. 1988;70:110–116. [PubMed] [Google Scholar]
- 4.Forkel P., Achtnich A., Metzlaff S., Zantop T., Petersen W. Midterm results following medial closed wedge distal femoral osteotomy stabilized with a locking internal fixation device. Knee Surg Sports Traumatol Arthrosc. 2015;23:2061–2067. doi: 10.1007/s00167-014-2953-1. [DOI] [PubMed] [Google Scholar]
- 5.Dewilde T.R., Dauw J., Vandenneucker H., Bellemans J. Opening wedge distal femoral varus osteotomy using the Puddu plate and calcium phosphate bone cement. Knee Surg Sports Traumatol Arthrosc. 2013;21:249–254. doi: 10.1007/s00167-012-2156-6. [DOI] [PubMed] [Google Scholar]
- 6.Thein R., Bronak S., Thein R., Haviv B. Distal femoral osteotomy for valgus arthritic knees. J Orthop Sci. 2012;17:745–749. doi: 10.1007/s00776-012-0273-1. [DOI] [PubMed] [Google Scholar]
- 7.Sternheim A., Garbedian S., Backstein D. Distal femoral varus osteotomy: Unloading the lateral compartment: Long-term follow-up of 45 medial closing wedge osteotomies. Orthopedics. 2011;34:e488–e490. doi: 10.3928/01477447-20110714-37. [DOI] [PubMed] [Google Scholar]
- 8.Puddu G., Cipolla M., Cerullo G., Franco V., Gianni E. Which osteotomy for a valgus knee? Int Orthop. 2010;34:239–247. doi: 10.1007/s00264-009-0820-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Omidi-Kashani F., Hasankhani I.G., Mazlumi M., Ebrahimzadeh M.H. Varus distal femoral osteotomy in young adults with valgus knee. J Orthop Surg Res. 2009;4:15. doi: 10.1186/1749-799X-4-15. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Cameron J.I., McCauley J.C., Kermanshahi A.Y., Bugbee W.D. Lateral opening-wedge distal femoral osteotomy: Pain relief, functional improvement, and survivorship at 5 years. Clin Orthop Relat Res. 2015;473:2009–2015. doi: 10.1007/s11999-014-4106-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Aglietti P., Menchetti P.P. Distal femoral varus osteotomy in the valgus osteoarthritic knee. Am J Knee Surg. 2000;13:89–95. [PubMed] [Google Scholar]
- 12.Makhmalbaf H., Moradi A., Ganji S. Distal femoral osteotomy in genovalgum: Internal fixation with blade plate versus casting. Arch Bone Jt Surg. 2014;2:246–249. [PMC free article] [PubMed] [Google Scholar]
- 13.Bagherifard A., Jabalameli M., Hadi H.A. The results of biplanar distal femoral osteotomy; a case series study. Arch Bone Jt Surg. 2015;3:35–38. [PMC free article] [PubMed] [Google Scholar]
- 14.Madelaine A, Lording T, Villa V, Lustig S, Servien E, Neyret P. The effect of lateral opening wedge distal femoral osteotomy on leg length. Knee Surg Sports Traumatol Arthrosc in press, available online 19 october, 2014. doi:10.1007/s00167-014-3387-5. [DOI] [PubMed]
- 15.Gupta V., Kamra G., Singh D., Pandey K., Arora S. Wedgeless ‘V’ shaped distal femoral osteotomy with internal fixation for genu valgum in adolescents and young adults. Acta Orthop Belg. 2014;80:234–240. [PubMed] [Google Scholar]
- 16.Hetsroni I., Lyman S., Pearle A.D., Marx R.G. The effect of lateral opening wedge distal femoral osteotomy on medial knee opening: Clinical and biomechanical factors. Knee Surg Sports Traumatol Arthrosc. 2014;22:1659–1665. doi: 10.1007/s00167-013-2405-3. [DOI] [PubMed] [Google Scholar]
- 17.Marin Morales L.A., Gomez Navalon L.A., Zorrilla Ribot P., Salido Valle J.A. Treatment of osteoarthritis of the knee with valgus deformity by means of varus osteotomy. Acta Orthop Belg. 2000;66:272–278. [PubMed] [Google Scholar]
- 18.Saithna A., Kundra R., Getgood A., Spalding T. Opening wedge distal femoral varus osteotomy for lateral compartment osteoarthritis in the valgus knee. Knee. 2014;21:172–175. doi: 10.1016/j.knee.2013.08.014. [DOI] [PubMed] [Google Scholar]
- 19.Haviv B., Bronak S., Thein R., Thein R. The results of corrective osteotomy for valgus arthritic knees. Knee Surg Sports Traumatol Arthrosc. 2013;21:49–56. doi: 10.1007/s00167-012-2180-6. [DOI] [PubMed] [Google Scholar]
- 20.Backstein D., Morag G., Hanna S., Safir O., Gross A. Long-term follow-up of distal femoral varus osteotomy of the knee. J Arthroplasty. 2007;22(suppl 1):2–6. doi: 10.1016/j.arth.2007.01.026. [DOI] [PubMed] [Google Scholar]
- 21.Berruto M., Bianchi M., Laura G. Surgical treatment of arthritic valgus knee: Femoral supracondylar osteotomy or knee replacement? Ital J Orthop Traumatol. 1993;19:33–41. [PubMed] [Google Scholar]
- 22.Kosashvili Y., Safir O., Gross A., Morag G., Lakstein D., Backstein D. Distal femoral varus osteotomy for lateral osteoarthritis of the knee: A minimum ten-year follow-up. Int Orthop. 2010;34:249–254. doi: 10.1007/s00264-009-0807-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Brinkman J.M., Hurschler C., Agneskirchner J.D., Freiling D., van Heerwaarden R.J. Axial and torsional stability of supracondylar femur osteotomies: Biomechanical comparison of the stability of five different plate and osteotomy configurations. Knee Surg Sports Traumatol Arthrosc. 2011;19:579–587. doi: 10.1007/s00167-010-1281-3. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Detailed surgical technique for medial closing-wedge distal femoral osteotomy with proximal tibial locking plate. The patient is placed in the supine position on the operating table, and a medial-side approach is used in the left knee. Dissection of the soft tissue is performed by the subvastus approach, and the periosteum is incised. A V-shaped distal femoral osteotomy is performed, with the anterior arm having twice the length of the posterior arm. One to 5 mm of bone is resected, and limb alignment is corrected, closing the wedge of the osteotomy. A 3.5- or 4.5-mm anterolateral tibial locking plate (3.5-mm AxSOS or 3.5- or 4.5-mm LCP proximal tibia locking plate) is used for fixation.