

Abstract
Background
Young children raised in institutions are exposed to extreme psychosocial deprivation that is associated with elevated risk for psychopathology and other adverse developmental outcomes. The prevalence of attention deficit hyperactivity disorder (ADHD) is particularly high in previously institutionalized children, yet the mechanisms underlying this association are poorly understood. We investigated whether deficits in executive functioning (EF) explain the link between institutionalization and ADHD.
Method
A sample of 136 children (aged 6–30 months) was recruited from institutions in Bucharest, Romania, and 72 never institutionalized community children matched for age and gender were recruited through general practitioners’ offices. At 8 years of age, children’s performance on a number of EF components (working memory, response inhibition and planning) was evaluated. Teachers completed the Health and Behavior Questionnaire, which assesses two core features of ADHD, inattention and impulsivity.
Results
Children with history of institutionalization had higher inattention and impulsivity than community controls, and exhibited worse performance on working memory, response inhibition and planning tasks. Lower performances on working memory and response inhibition, but not planning, partially mediated the association between early institutionalization and inattention and impulsivity symptom scales at age 8 years.
Conclusions
Institutionalization was associated with decreased EF performance and increased ADHD symptoms. Deficits in working memory and response inhibition were specific mechanisms leading to ADHD in previously institutionalized children. These findings suggest that interventions that foster the development of EF might reduce risk for psychiatric problems in children exposed to early deprivation.
Keywords: ADHD, children, early deprivation, executive functioning
Introduction
Institutionalization is a widespread phenomenon in low- and middle-income countries (UNICEF, 2010) that puts young children at risk for adverse development and health outcomes. The deleterious effects of institutionalization are evident in numerous developmental domains, both physical and psychosocial, and can be long-lasting (Rutter et al. 2010). Young children raised in institutions exhibit profound deficits in cognitive, emotional and social functioning (Rutter et al. 2010; Nelson et al. 2014). Elevations in psychopathology are particularly marked in previously institutionalized children (Rutter et al. 2001; Zeanah et al. 2009; Humphreys et al. 2015).
The Bucharest Early Intervention Project (BEIP) was designed to examine the effects of a foster care intervention among institutionalized children on subsequent brain and behavioral development (Zeanah et al. 2003; Nelson et al. 2014). In this study, exposure to institutionalization was associated with elevations in both internalizing and externalizing disorders, but only internalizing disorders were remediated through placement into foster care at 4½ years (Zeanah et al. 2009). By contrast, exposure to institutionalization was associated with an increased risk for externalizing disorders that was not improved by placement into foster care. Twenty-one percent of children raised in institutions met criteria for attention deficit hyperactivity disorder (ADHD) by age 4½ years, even if they later lived in a foster care family (Zeanah et al. 2009); at 12 years the rate of ADHD was 19.3% (Humphreys et al. 2015). High rates of ADHD have also been observed in other studies of children reared in institutions (Kreppner et al. 2001; Stevens et al. 2008) and they are markedly higher than in never institutionalized children, where the prevalence of ADHD is estimated to be between 3% and 10% (Kessler et al. 2006; Spencer et al. 2007). Indeed, symptoms of ADHD are so common among previously institutionalized children, that some have argued that they represent one type of deprivation-specific behavior patterns (Kreppner et al. 2001; Rutter et al. 2010). Yet the mechanisms that mediate the link between institutionalization and elevated risk for ADHD are poorly understood.
Executive Functioning (EF) deficits are strongly associated with ADHD symptoms (Barkley, 1997; Sergeant, 2000; Martinussen et al. 2005; Willcutt et al. 2005; Schoemaker et al. 2012). However, EF and ADHD are not synonymous and current research has emphasized the heterogeneity in cognitive function observed in the population of children diagnosed with ADHD (Fair et al. 2012). It has been widely hypothesized that this heterogeneity reflects as yet unidentified subpopulations of children with ADHD currently subsumed under the umbrella diagnosis (Willcutt et al. 2005; Halperin & Schulz, 2006), and it is possible that ADHD following exposure to childhood adversity is one of these subpopulations. In this case, we would expect that children with ADHD following institutionalization would not necessarily evidence the same EF deficits often observed in other populations of children with ADHD. EF generally refers to a set of higher-order functions that regulate cognition and behavior and can be broken into three to four interrelated yet distinct domains: inhibition, working memory, set-shifting and planning (Sonuga-Barke et al. 2002; Niendam et al. 2012). Institutionalization is also associated with deficits in multiple aspects of EF, in preschool and school-aged children, including working memory, set-shifting, and inhibitory control (Colvert et al. 2008; Bos et al. 2009; Pollak et al. 2010; Hostinar et al. 2012; Loman et al. 2013; McDermott et al. 2013; Merz et al. 2013). Similar to the pattern observed in ADHD, EF improvements have not been observed following early intervention (Bos et al. 2009). It is possible that the risk for ADHD conferred by institutionalization is explained by the effect of early institutional rearing on EF. We explore this hypothesis in the current report.
The possibility of an early neurodevelopmental mechanism linking environmental experience to ADHD (Taylor & Rogers, 2005; Stevens et al. 2008) is suggested by studies linking other types of early adverse environments other than institutionalization to ADHD (Biederman et al. 1995; McLaughlin et al. 2010b). Deficits in EF have also been observed in children exposed to various adverse conditions, such as maltreatment (Pears et al. 2010) and witnessing domestic violence (DePrince et al. 2009). Few studies have examined the underlying factors leading to psychopathology in previously institutionalized children. Those studies that have been conducted found links between atypical brain functioning and ADHD (McLaughlin et al. 2010a, 2014; Slopen et al. 2012). To our knowledge, there is only one previous study (i.e. Colvert et al. 2008) that explored the possible mediating role of EF in the link between institutionalization and psychopathology. However, this study is limited by a single task assessing inhibitory control. In the current study we extend this previous report by examining the role of EF as a mechanism linking institutionalization to ADHD symptoms using a more comprehensive assessment of EF.
The current investigation presents data from the BEIP sample at 8 years of age. Previous reports on these data showed that the children with history of institutional rearing had increased inattention and impulsivity symptoms (McLaughlin et al. 2014) and decreased performance on working memory (Bos et al. 2009) and inhibition (McDermott et al. 2013). Here, we expected to find links between the children’s EF abilities and their ADHD symptoms. Furthermore, we predicted that elevations in ADHD symptoms in the institutionalized children would be mediated by differences in EF abilities.
Method
Sample
Participants were children from the BEIP, a longitudinal study of the effects of institutionalization and the only randomized controlled trial of foster care for children raised in institutional settings (Zeanah et al. 2003; Nelson et al. 2014). A total of 136 children living in institutions in Bucharest, Romania were recruited during infancy (age range 6–31 months, mean age = 22 months). Following recruitment and baseline testing the children were randomly assigned to a care as usual group (CAUG, N = 68) or a foster care group (FCG, N = 68). Children in the CAUG received care as usual, meaning that they remained in institutional care longer, and children in the FCG were placed in a network of foster families selected and trained by study investigators living in Bucharest. Seventy-two never institutionalized (NIG) children raised by their families in the community also were recruited to serve as controls. Details on study design and participants have been described previously (see Zeanah et al. 2003). Study procedures were approved by the local commissions on child protection in Bucharest and approved by an ethics committee comprising appointees from government and Bucharest University academic departments. The study was approved and overseen by the institutional review boards of the home institutions of the three principal investigators. A complete description of procedures employed to ensure ethical integrity has been published previously (Zeanah et al. 2012).
The current study presents data from the sample of children who completed neuropsychological testing at a follow-up assessment when they were 8 years of age. A total of 29 previously institutionalized children (17 from CAUG, 12 from FCG) were lost to follow-up (the main reasons for attrition were lost contact and refusal to participate). The control group was supplemented by the addition of age-matched children recruited from two local schools. Of the 205 children who agreed to participate at the 8-year assessment, we were able to obtain teacher ratings of psychopathology for 195 of them, and 157 children completed the neuropsychological testing. A total of 146 children (43 from CAUG, 47 from FCG, 56 from NIG) had data on both the EF and ADHD measures (see flowchart of participants in Fig. 1). Mean age at testing was 8.56 years (S.D. = 0.40). Descriptive data on demographic variables for the institutionalized and non-institutionalized children are presented in Table 1 and show equal gender distributions but significant differences in age of testing and ethnicity in the two groups.
Fig. 1.
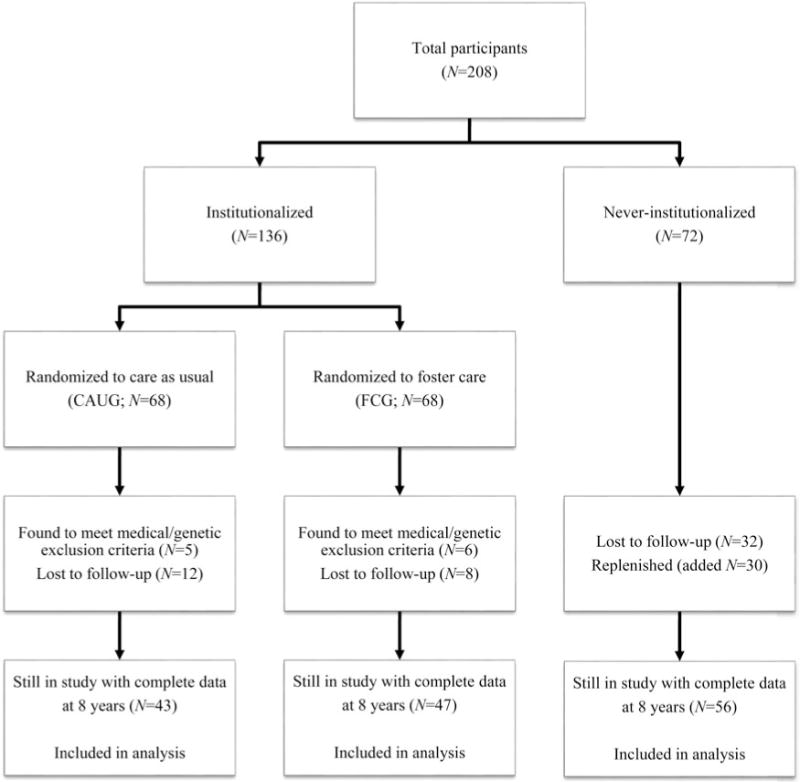
Flow chart of participants.
Table 1.
Descriptive statistics on demographic information
| EIG (N = 90) | NIG (N = 56) | Group difference | |
|---|---|---|---|
| Age at testing, years (S.D.) | 8.63 | 8.44 | t = 2.90; p = 0.004 |
| Gender | |||
| Male | 43 | 26 | N.S. |
| Female | 47 | 30 | |
| Ethnicity | |||
| Romanian | 46 | 50 | χ2(2) = 24.73, p < 0.001 |
| Roma | 33 | 4 | |
| Other/unknown | 11 | 2 |
EIG, Ever institutionalized group; NIG, never institutionalized group; N.S., not significant.
Consistent with our previous reports, we did not observe an intervention effect of foster care on symptoms of ADHD (t94 = 1.13, p = 0.26 for inattention; t93 = −0.07, p = 0.94 for impulsivity) or any of the EF indices (their corresponding p values ranged from 0.38 to 0.80) in this sample. Accordingly, for the remainder of this paper we consider two groups, children who were ever institutionalized (EIG, N = 90) and children who were never institutionalized (NIG, N = 56).
Measures
ADHD
Symptoms of ADHD were assessed through teacher report using the Health and Behavior Questionnaire (HBQ; Essex et al. 2002), which has been previously used in research on institutionalized children (Wiik et al. 2011). The HBQ has been used extensively with children of preschool age to adolescence, and has demonstrated good reliability and convergent and discriminant validity (Essex et al. 2002; Lemery-Chalfant et al. 2007). Symptoms are rated on a 3-point Likert scale: 0 (‘never or not true’), 1 (‘sometimes true’) or 2 (‘often or very true’), with higher scores indicating elevated levels of symptomatology. ADHD symptoms of inattention (six items) and impulsivity (nine items) are assessed.
EF
We measured EF using the Cambridge Automated Neuropsychological Test Battery (CANTAB; http://www.cantab.com), behavioral tasks that have been widely used with typically developing children, at-risk children, children with ADHD, and adults (Nigg, 2001; Fried et al. 2015). The CANTAB has been validated extensively on samples of school-age children and has been found to discriminate well between clinical and standard populations (Luciana & Nelson, 2002). As detailed below, four CANTAB subtests (each typically lasting between 5 and 10 min) were administered to assess working memory and planning skills. Additionally, we used a version of the Flanker task (Eriksen & Schultz, 1979) to assess response inhibition.
Delayed Matching to Sample (DMS) is a short-term memory task in which the child is presented with a stimulus pattern and then needs to select a matching pattern from a series of four patterns shown below the stimulus. Trials are either simultaneous (both the stimulus and the four choices are shown on the screen at the same time), with a 0-s delay (the stimulus disappears just before the choices are presented), or with a delays of 4000 or 12 000 ms. The main outcome variables are the number of correct trials and latency of response for each type of trial.
The Paired Associates Learning (PAL) subtest assesses spatial working memory and new learning. Six to eight boxes are presented sequentially on the screen, with some or all containing a different pattern. The patterns are then shown again in the middle of the screen, one at a time and in a randomized order, and the child has to touch the box that contained the pattern. The difficulty increases with the number of patterns contained in the boxes. Outcome variables include stages completed at first trial, total stages completed, and memory score (i.e. number of patterns correctly located after the first trial summed across the stages completed).
Spatial Working Memory (SWM) tests the ability to retain spatial information across a delay and to manipulate remembered items in working memory. A number of 3–8 colored boxes are shown on the screen and the subject is invited, by process of elimination, to find a blue token in each of these boxes and use it to fill up an empty column on the right of the screen. Variables of interest are between errors (i.e. number of times across trials in which the subject revisits a box in which a token has previously been found), within errors (i.e. number of times within a search in which the subject revisits an empty box), and strategy (i.e. presence/absence of organized patterns of search).
The Stockings of Cambridge (SOC) task is a planning task derived from the Tower of London test (Shallice, 1982). The child views a set of three hanging stockings on the top of the screen that contain colored circles in a given order and another set of stockings on the lower half of the screen containing the same circles but positioned differently across the stockings. The child is instructed to move the circles in the lower display to copy the upper model using as few moves as possible. The difficulty of the trials increases gradually from two-move problems to more complex models that require five moves to solve. Key outcomes are number of trials solved in minimum moves, mean number of moves for each level of difficulty, and initial and subsequent thinking times.
The Flanker task assesses the children’s capacity to respond to target stimuli in the context of other distracting stimuli. A series of five arrows (pointing to the left or right) are presented to the child on a computer screen. The child is instructed to focus solely on the central arrow, which always appears flanked by two more arrows on either side, and to press as quickly and as accurately as possible the left button on a pad when the target points to the left, and the right button when the arrow is directed to the right. The two pairs of distracting arrows between which the target arrow is situated point to either the same direction as the target (congruent trials, <<<<< and >>>>>) or the opposite (incongruent trials, >><>> and <<><<). We collected both response accuracy and reaction time (RT) during congruent and incongruent trials. Differences in RT between incongruent and congruent trials (known as the Flanker effect) are thought to reflect response inhibition (Fan et al. 2002).
Procedure
All children were accompanied to the laboratory by their main caregiver to complete the procedures. Informed consent was obtained from the caregiver and written approvals to participate were collected from the local authority representatives prior to the start of the study for the institutionalized and foster care children whose legal guardians were not their biological parents. The child was invited to one of the study rooms to complete the CANTAB in the presence of a researcher who provided standard instructions. In a separate session, the child was asked to complete the Flanker task along with other procedures; however, due to logistical reasons, a total of 47 children (16 from CAUG, 10 from FCG, 21 from NIG) completed both the CANTAB and the Flanker tasks during the same visit. Finally, the research team contacted the primary school teachers and asked them to complete the teacher version of the HBQ.
Statistical analysis
We investigated whether impaired EF task performance associated with exposure to institutionalization was responsible for the elevated rates of inattention and impulsivity among previously institutionalized children relative to community controls using standard tests of statistical mediation. To provide evidence for mediation, four criteria must be met (Baron & Kenny, 1986; MacKinnon et al. 2002). First, an association between the exposure and outcome of interest must be established. Here, we examined differences in symptoms of ADHD using univariate analysis of variance (ANOVA) with group (EIG and NIG) as a between-subjects factor. Because previous research suggests that EF may be differentially associated with subtypes of ADHD (Martel et al. 2007; Brocki et al. 2010), we examined symptoms of inattention and impulsivity as separate outcomes.
Second, the exposure must be associated with the putative mediator. We examined group differences in EF using univariate ANOVAs with group as a between-subjects factor. We examined performance on working memory (DMS, PAL, SWM), response inhibition (Flanker), and planning (SOC) tasks. Third, the mediator must be associated with the outcome. Here, we examined the association between EF and ADHD symptoms using linear regression.
The final critical test of mediation involves the degree of attenuation in the association between the exposure and outcome in a model that includes the mediator. If this association is attenuated significantly, a significant indirect effect of the exposure on the outcome through the mediator exists, establishing evidence for mediation (Baron & Kenny, 1986; MacKinnon et al. 2002). Here, we tested the significance of the mediator using a bootstrapping approach that provides bias corrected confidence intervals and allows multiple mediators (i.e. measures of EF) to be examined in one model (Preacher & Hayes, 2008). Confidence intervals that do not include zero indicate significant mediation. Age and gender were included as covariates in all analyses, and statistical significance was evaluated at the 0.05 level, using two-sided tests.
Results
Institutionalization and ADHD symptomatology
Mean scores of inattention and impulsivity were examined between the two groups using ANOVA and are presented in Table 2. Children with history of institutionalization had significantly higher inattention (F1,193 = 49.01, p < 0.001), and impulsivity (F1,192 = 32.87, p < 0.001), than the community controls (Table 2).
Table 2.
Teacher reports of ADHD symptoms in the EIG and NIG children
| EIG (N = 96)
|
NIG (N = 99)
|
Group difference
|
||||
|---|---|---|---|---|---|---|
| Mean | S.D. | Mean | S.D. | F | p value | |
| Inattention | 5.42 | 3.35 | 2.31 | 2.83 | 49.01* | <0.001 |
| Impulsivity | 7.61 | 5.29 | 3.73 | 4.09 | 32.87* | <0.001 |
ADHD, Attention deficit hyperactivity disorder; EIG, ever institutionalized group; NIG, never institutionalized group.
Significant at the 0.05 level, two-sided test; analyses control for age and gender.
Institutionalization and executive functioning
ANOVA was conducted to examine whether the two groups differed on the variables of interest from each of the five tasks. Results are presented in Table 3 and show that children in the EIG performed significantly more poorly than NIG children on multiple dimensions of executive functioning as measured by our CANTAB battery and the Flanker task. Children exposed to institutional rearing had significantly lower accuracy on the longest delay trials of the DMS task (F1,143 = 10.89, p = 0.001), a lower number of PAL stages completed on first trial (F1,155 = 7.78, p = 0.006), lower PAL first trial memory scores (F1,155 = 10.90, p = 0.001), lower SWM strategy scores (F1,155 = 10.73, p = 0.001), higher number of SWM between errors (F1,155 = 17.40, p < 0.001), lower response inhibition in the Flanker task (F1,148 = 10.05, p = 0.002), and fewer problems solved in minimum moves on the SOC task (F1,155 = 6.36, p = 0.013).
Table 3.
EF abilities in the EIG and NIG children
| EIG (N=90)
|
NIG (N=57)
|
Group difference
|
||||
|---|---|---|---|---|---|---|
| Mean | S.D. | Mean | S.D. | F | p value | |
| DMSa | ||||||
| Percent accuracy 4000 ms | 57.39 | 23.76 | 62.81 | 19.06 | 2.09 | 0.15 |
| Percent accuracy 12 000 ms | 51.82 | 25.49 | 65.97 | 24.77 | 10.89* | 0.001 |
| PAL | ||||||
| Stages completed on 1st trial | 4.89 | 1.23 | 5.44 | 1.10 | 7.78* | 0.006 |
| First trial memory score | 16.32 | 4.65 | 18.70 | 3.76 | 10.90* | 0.001 |
| SWM | ||||||
| Strategy score | 39.45 | 2.54 | 37.63 | 4.43 | 10.73* | 0.001 |
| Between errors total | 67.36 | 12.85 | 57.67 | 15.83 | 17.40* | <0.001 |
| Flanker | ||||||
| RT incongruent – RT congruent | 0.05 | 0.06 | 0.09 | 0.09 | 10.05* | 0.002 |
| SOC | ||||||
| Problems solved in minimum moves | 5.55 | 2.02 | 6.35 | 1.72 | 6.36* | 0.013 |
EF, Executive functioning; EIG, ever institutionalized group; NIG, never institutionalized group; DMS, Delayed Matching to Sample; PAL, Paired Associates Learning; SWM, Spatial Working Memory; RT, reaction time; SOC, Stockings of Cambridge;
Significant at the 0.05 level, two-sided test; analyses control for age and gender.
DMS statistics are reported only on those subjects who had scores which were greater than expected by chance in the 0-ms delay trials.
ADHD and EF
Associations between inattention and impulsivity and the EF indices are reported in Table 4 (see Appendix Table A1 for correlational associations amongst all variables of interest). Inattention was significantly associated with several aspects of working memory performance. These included the number of PAL stages completed on first trial, PAL first trial memory score, SWM strategy score, and SWM between errors. Inattention was also marginally negatively associated with accuracy in the longest delay trials of the DMS, another index of working memory. Likewise, inattention was associated with response inhibition measured in the Flanker task. Last, a marginal association was observed between inattention and planning as assessed by SOC problems solved in minimum moves. All associations were in the expected direction: elevated levels of inattention symptoms associated with decreased EF performance.
Table 4.
Associations between ADHD symptoms and EF indices at 8 yearsa
| Inattention
|
Impulsivity
|
|||
|---|---|---|---|---|
| β | p | β | p | |
| Working memory | ||||
| DMS % accuracy 12 000 msb | −0.17 | 0.059 | −0.16 | 0.07 |
| PAL stages completed on 1st trial | −0.24 | 0.004 | −0.11 | 0.16 |
| PAL first trial memory score | −0.39 | <0.001 | −0.25 | 0.002 |
| SWM strategy score | 0.18 | 0.037 | 0.21 | 0.013 |
| SWM between errors total | 0.30 | <0.001 | 0.20 | 0.016 |
| Response inhibition | ||||
| Flanker RT incongruent – RT congruent | −0.21 | 0.012 | −0.24 | 0.004 |
| Planning | ||||
| SOC problems solved in minimum moves | −0.15 | 0.079 | −0.19 | 0.018 |
ADHD, Attention deficit hyperactivity disorder; EF, executive functioning; DMS, Delayed Matching to Sample; PAL, Paired Associates Learning; SWM, Spatial Working Memory; RT, reaction time; SOC, Stockings of Cambridge.
Analyses control for age and gender.
DMS statistics are reported only on those subjects who had scores which were greater than expected by chance in the 0-ms delay trials.
Similar to our findings with inattention symptoms, we observed significant associations between impulsivity and PAL first trial memory score, SWM strategy score, SWM between errors and a marginally significant association between impulsivity and accuracy in the longest delay trials of the DMS. Impulsivity was also associated with response inhibition in the Flanker task and the number of SOC problems solved in minimum moves. No association was observed between impulsivity and PAL stages completed on first trial.
Mediation analysis
In order to assess whether indices of EF explain the relations between early deprivation and later ADHD symptomatology, we conducted two multiple mediation analyses separately for inattention and impulsivity. We separately tested mediation for working memory, response inhibition and planning by entering the measures of these constructs that were associated with both institutionalization and the outcome (i.e. inattention and impulsivity).
The total effect of early institutionalization in predicting inattention was significant (B = −1.80, p < 0.001) and was attenuated by 15.6% with the inclusion of the working memory indices in the model (i.e. DMS percent accuracy 12 000 ms., PAL stages completed on first trial, PAL first trial memory score, SWM strategy score, and SWM between errors total, B = −1.52, p < 0.001; Fig. 2). The indirect effect of institutionalization on inattention was significant [95% confidence interval (CI) −0.56 to −0.06]. By contrast, the indirect effects of institutionalization on inattention when the inhibition or planning indices were added to the model were not statistically significant (95% CIs −0.28 to 0.00; −0.19 to 0.03 respectively).
Fig. 2.
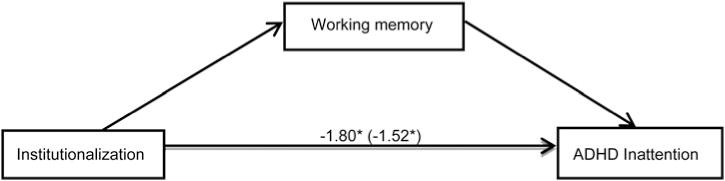
Model of the association between institutionalization and symptoms of inattention at 8 years as mediated by indices of working memorya. ADHD, attention-deficit/hyperactivity disorder. [aUnstandardized coefficients are shown for the direct and indirect (in parentheses, with mediators included) regression models; *p < 0.001.]
Similarly, the total effect of institutionalization in predicting impulsivity was significant (B = −2.23, p < 0.001) and was attenuated by 16.6% with the inclusion of working memory indices in the model (B = −1.86, p < 0.001). The indirect effect of institutionalization was statistically significant (95% CI −0.80 to −0.04). Likewise, the total effect of institutionalization on impulsivity was significant (B = −2.24, p < 0.001) and was attenuated by 9% with the inclusion of the Flanker index of response inhibition (B = −2.04, p < 0.001; Fig. 3). The indirect effect of institutionalization on impulsivity through response inhibition was significant (95% CI −0.52 to −0.03). By contrast, the indirect effect of institutionalization in the prediction of impulsivity when the planning index was added to the model was not statistically significant (95% CI −0.40 to 0.01). Together, these findings suggest that inattention and impulsivity associated with exposure to institutionalization are partially explained by deficits in working memory and response inhibition, but not planning abilities.
Fig. 3.
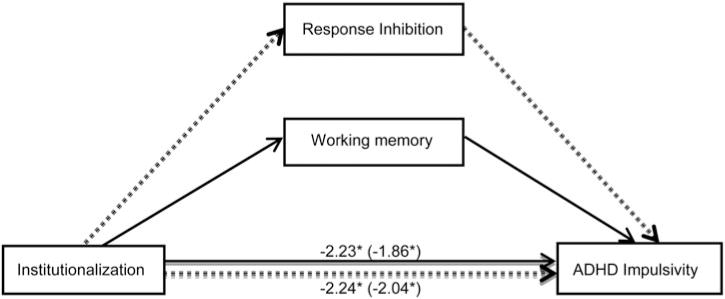
Models of the associations between institutionalization and symptoms of impulsivity at 8 years as mediated by indices of working memory (solid lines) and response inhibition (dotted lines)a. ADHD, Attention deficit hyperactivity disorder. [aUnstandardized coefficients are shown for the direct and indirect (in parentheses, with mediators included) regression models; *p < 0.001.]
Specificity of associations
In order to ascertain that deficits in EF represent a mechanism which specifically explains symptoms of ADHD as opposed to other forms of psychopathology in previously institutionalized children, we ran additional analyses with the outcome scales of internalizing (e.g. anxiety and depression) and externalizing (i.e. oppositional/defiant and conduct) symptoms of the HBQ. Institutionalization was indeed associated with elevations in both of these scale scores on the HBQ (details not presented but available upon request). However, disruptions in EF did not mediate the association of institutionalization with any form of psychopathology other than ADHD, which supports our hypothesis that EF deficits are a pathway linked specifically to ADHD symptoms.
Discussion
The purpose of the current study was to test whether deficits in EF were a mechanism linking early psychosocial deprivation to ADHD symptoms at age 8 years. The association between early institutionalization and ADHD symptoms was partially explained by deficits in working memory (for both inattention and impulsivity) and response inhibition (for impulsivity only), but was not accounted for by planning ability. These findings build on previous reports describing the pathways through which institutionalization influences mental health outcomes in children and extends previous research by highlighting the importance of working memory and inhibition as neurodevelopmental mechanisms involved in the association of institutional rearing with ADHD symptoms.
The association between institutionalization and symptoms of ADHD observed here are consistent with results from a number of other studies (e.g. Kreppner et al. 2001; Stevens et al. 2008; Wiik et al. 2011), as well as our own work in the BEIP when the children were assessed at earlier ages (Zeanah et al. 2009). Elevated ADHD symptomatology associated with early institutionalization is likely to result from deficits in neurodevelopmental processes. Consistent with this hypothesis, poorer performance on EF tasks has been observed in prior studies of previously institutionalized children (e.g. Colvert et al. 2008; Pollak et al. 2010; Merz & McCall, 2011; Hostinar et al. 2012; Merz et al. 2013). The novelty of the current investigation is that it is the first to demonstrate that one mechanism linking early institutionalization to ADHD is disruption in working memory and response inhibition. To best of our knowledge, only one report (i.e. Colvert et al. 2008) has tested mediation and suggested that inhibition might play a mediating role in this link, but the analyses showed only a trend that failed to attain statistical significance. Here, we found that response inhibition served as a significant mediator of the association between institutionalization and impulsivity, a specific cluster of ADHD symptomatology.
Previous investigations in the BEIP and other samples of children adopted from Eastern Europe have identified several neurobiological factors that partially or fully mediate the association between institutionalization and the incidence of ADHD. In our own sample, delayed cortical maturation manifesting in atypical EEG frequency band signals and reduced cortical thickness in multiple brain regions has been found to partially mediate the link from early deprivation to ADHD at 4½ and 8 years (McLaughlin et al. 2010a, 2014). In contrast to those findings, the current paper explores the mediating pathway of specific cognitive functions, namely working memory, response inhibition, and planning. Our findings point to specific cognitive functions that link institutionalization to ADHD, but not common to other forms of externalizing psychopathology or to internalizing psychopathology. We also find specificity in the specific domains of EF that are involved in this association. Two findings are notable. First, children raised in institutions exhibited deficits in working memory only during the most difficult trials of the DMS task that required holding a stimulus in mind for the longest period of time. Although previously institutionalized children performed reasonably well at maintaining a stimulus in working memory for short periods of time, maintaining this representation over time was more challenging for them; this pattern suggests that more complex aspects of working memory – such as updating or manipulating information – may be most impacted by institutional rearing. Second, our finding that the association between institutional rearing and ADHD was mediated specifically by working memory and inhibition, but not by planning, highlights that while many aspects of cognitive and neural function and neural structure are impacted by institutionalization, they may not all contribute equally to risk for ADHD. Indeed, it is by identifying specific pathways of risk, as we do here, that we are most likely to develop interventions to remediate the effects of institutional rearing on specific mental health outcomes, including ADHD. Our findings suggest that although children exposed to institutional rearing exhibit deficits in multiple forms of EF, the association with ADHD symptoms is explained primarily by deficits in working memory and response inhibition. Given the sample size, and the fact that our main effect differs subtly from previous findings, because we controlled for age and gender in the analysis, it is possible that planning does play a role in ADHD following institutionalization, albeit, one which was too small for us to observe here. The non-significant mediating effect of planning needs to be replicated in future investigations before firm conclusions are drawn.
These findings are consistent with previous work that demonstrates that performance on the SWM sub-test, but not the planning subtest of the CANTAB predicts symptom severity in adolescents with ADHD (Coghill et al. 2014). One possible explanation for this observation is that working memory might represent a more basic aspect of EF that scaffolds the development of more complex cognitive functions and that, when disrupted, has more severe downstream effects on cognition and behavior, including symptoms of inattention and impulsivity.
Similarly, our finding that symptoms of impulsivity emerge partly as a result of poor response inhibition in children who experienced psychosocial neglect early in life is consistent with the finding that good response inhibition functions as an index of resilience following exposure to environmental adversities (Nigg et al. 2007; McDermott et al. 2013). The fact that we do not see the same association with inattention may be related to the selective importance of response inhibition in predicting symptoms of motor impulsivity and hyperactivity (Barkley, 2001). Finally, within this study, the neuropsychological profile of children who have ADHD following exposure to institutionalization is very similar to the profiles of children who receive a diagnosis of ADHD having been raised in more typical environments. Thus it is possible that exposure to institutionalization increases risk for ADHD via its impact on the same neural structures and functions that underlie dysfunction in ADHD more generally.
The results in the current study should be interpreted in view of several limitations. First, our findings are based on EF and ADHD data collected at the same point in development, this first point that EF was assessed in the study. This suggests that our findings could also reflect earlier-onset ADHD predicting disruptions in EF, rather than the reverse. However, ADHD symptoms at age 4½ years were assessed in the BEIP using a parent-reported interview, and we observed no associations between earlier ADHD symptoms and EF at age 8 years. This provides further support for our interpretations of these associations at age 8 years. Because the BEIP is a longitudinal study, we hope in the future to make use of our repeated measures design to examine how EF predicts changes over time in ADHD. Second, psychopathology was only assessed using teacher questionnaires; previous studies have made use of psychiatric interviews and/or parental reports in obtaining child psychopathology data. However, ADHD behaviors frequently manifest in the school setting, and teacher reports provide a standardized method of reporting ADHD symptoms as compared to caregiver reports in this sample, given variation in the length and quality of caregiver relationships among children with and without exposure to institutional rearing. Teachers also have a unique perspective in having substantial amounts of time in which to observe children at a particular developmental period and to evaluate individual differences. Nevertheless, it is possible that symptoms observed at school are only part of the problematic behaviors shown in other environments, and that other informants and/or the use of diagnoses might reflect more adequately the manifestations of the problem. Finally, we were not able to account for the possible influence of other factors (e.g. prenatal, genetic risks, or medical illnesses during the gestational or early infancy periods, and socioeconomic status) that might have played a direct or interactive role in the link between early deprivation and ADHD and which should be examined in future studies.
This study identified working memory and response inhibition as partial mediators of the association between institutional rearing and ADHD symptoms at 8 years of age in children who were exposed to severe psychosocial deprivation in orphanages in Romania. The current findings have the potential to inform developmental specialists on some of the early neurodevelopmental pathways to psychopathology so that intervention can be effectively targeted in order to reduce risks and promote adaptive developmental outcomes for children exposed to adverse early environments. Specifically, our findings suggest that interventions designed to improve working memory and inhibition (Klingberg et al. 2005; Johnstone et al. 2010) could have a beneficial effect on ADHD symptoms among children exposed to institutional rearing.
Acknowledgments
This research was supported by a grant from the John D. and Catherine T. MacArthur Foundation Research Network on Early Experience and Brain Development (Charles A. Nelson, Network Chair), the National Institutes of Health (to C.A.N.; 1R01MH091363-01), and research support from the Binder Foundation (to C.A.N.). These funders provided support for all data collection and analysis. We thank Elizabeth Furtado for overseeing the Bucharest Early Intervention Project and all the laboratory staff in Romania (Anca Radulescu, Nicoleta Corlan, Nadia Radu, Carmen Iuga and Iuliana Dobre) for collecting the data and maintaining contact with the families. We also thank the caregivers and children who participated in this project.
Appendix Table A1.
Pearson correlations among study variables
| Inattention | Impulsivity | DMS percent accuracy at 0 ms | DMS percent accuracy at 4000 ms | DMS percent accuracy at 12 000 ms | PAL stages completed on first trial | PAL first trial memory score | SWM strategy | SWM between errors | RT incongruent – RT congruent | SOC problems solved in minimum moves | |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Inattention | 1 | 0.75*** | −0.32*** | −0.16 | −0.20* | −0.25** | −0.35*** | 0.18* | 0.30*** | −0.22** | −0.17* |
| Impulsivity | 1 | −0.27*** | −0.09 | −0.20* | −0.13 | −0.28*** | 0.21** | 0.20* | −0.25** | −0.23** | |
| DMS percent accuracy at 0 ms | 1 | 0.16 | 0.03 | 0.11 | 0.19* | −0.04 | −0.09 | 0.05 | 0.12 | ||
| DMS percent accuracy at 4000 ms | 1 | 0.13 | 0.26*** | 0.31*** | 0.13 | −0.17* | 0.03 | 0.01 | |||
| DMS percent accuracy at 12 000 ms | 1 | 0.17* | 0.24** | 0.03 | −0.21** | 0.10 | 0.14 | ||||
| PAL stages completed on first trial | 1 | 0.79*** | −0.03 | −0.32*** | −0.02 | 0.19* | |||||
| PAL first trial memory score | 1 | −0.08 | −0.39*** | 0.12 | 0.28*** | ||||||
| SWM strategy | 1 | 0.42*** | −0.19* | −0.24** | |||||||
| SWM between errors | 1 | −0.20* | −0.41*** | ||||||||
| RT incongruent – RT congruent | 1 | 0.12 | |||||||||
| SOC problems solved in minimum moves | 1 |
DMS, Delayed Matching to Sample; PAL, Paired Associates Learning; SWM, Spatial Working Memory; RT, reaction time; SOC, Stockings of Cambridge.
Correlation is significant at the 0.05 level (two-tailed).
Correlation is significant at the 0.01 level (two-tailed).
Correlation is significant at the 0.001 level (two-tailed).
Footnotes
Declaration of Interest
None.
References
- Barkley RA. Behavioral inhibition, sustained attention, and executive function: constructing a unified theory of ADHD. Psychological Bulletin. 1997;121:65–94. doi: 10.1037/0033-2909.121.1.65. [DOI] [PubMed] [Google Scholar]
- Barkley RA. The inattentive type of ADHD as a distinct disorder: what remains to be done. Clinical Psychology: Science and Practice. 2001;8:489–493. [Google Scholar]
- Baron RM, Kenny DA. The moderator-mediator variable distinction in social psychological research: conceptual, strategic, and statistical considerations. Journal of Personality and Social Psychology. 1986;51:1173–1182. doi: 10.1037//0022-3514.51.6.1173. [DOI] [PubMed] [Google Scholar]
- Biederman J, Milberger S, Faraone SV, Kiely K, Guite J, Mick E, Ablon S, Warburton R, Reed E. Family-environment risk factors for attention-deficit hyperactivity disorder. A test of Rutter’s indicators of adversity. Archives of General Psychiatry. 1995;52:464–470. doi: 10.1001/archpsyc.1995.03950180050007. [DOI] [PubMed] [Google Scholar]
- Bos KJ, Fox N, Zeanah CH, Nelson CA. Effects of early psychosocial deprivation on the development of memory and executive function. Frontiers in Behavioral Neuroscience. 2009;3:16. doi: 10.3389/neuro.08.016.2009. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Brocki K, Eninger L, Thorell L, Bohlin G. Interrelations between executive function and symptoms of hyperactivity/impulsivity and inattention in preschoolers: a two year longitudinal study. Journal of Abnormal Child Psychology. 2010;38:163–171. doi: 10.1007/s10802-009-9354-9. [DOI] [PubMed] [Google Scholar]
- Coghill DR, Hayward D, Rhodes SM, Grimmer C, Matthews K. A longitudinal examination of neuropsychological and clinical functioning in boys with attention deficit hyperactivity disorder (ADHD): improvements in executive functioning do not explain clinical improvement. Psychological Medicine. 2014;44:1087–1099. doi: 10.1017/S0033291713001761. [DOI] [PubMed] [Google Scholar]
- Colvert E, Rutter M, Kreppner J, Beckett C, Castle J, Groothues C, Hawkins A, Stevens S, Sonuga-Barke EJ. Do theory of mind and executive function deficits underlie the adverse outcomes associated with profound early deprivation? Findings from the ERA study. Journal of Abnormal Child Psychology. 2008;36:1057–1068. doi: 10.1007/s10802-008-9232-x. [DOI] [PubMed] [Google Scholar]
- DePrince AP, Weinzierl KM, Combs MD. Executive function performance and trauma exposure in a community sample of children. Child Abuse and Neglect. 2009;33:353–361. doi: 10.1016/j.chiabu.2008.08.002. [DOI] [PubMed] [Google Scholar]
- Eriksen CW, Schultz DW. Information processing in visual search: a continuous flow conception and experimental results. Perception & Psychophysics. 1979;25:249–263. doi: 10.3758/bf03198804. [DOI] [PubMed] [Google Scholar]
- Essex MJ, Boyce WT, Goldstein LH, Armstrong JM, Kraemer HC, Kupfer DJ. The confluence of mental, physical, social, and academic difficulties in middle childhood. II. Developing the MacArthur health and behavior questionnaire. Journal of the American Academy of Child and Adolescent Psychiatry. 2002;41:588–603. doi: 10.1097/00004583-200205000-00017. [DOI] [PubMed] [Google Scholar]
- Fair DA, Bathula D, Nikolas MA, Nigg JT. Distinct neuropsychological subgroups in typically developing youth inform heterogeneity in children with ADHD. Proceedings of the National Academy of Sciences USA. 2012;109:6769–6774. doi: 10.1073/pnas.1115365109. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fan J, McCandliss BD, Sommer T, Raz A, Posner MI. Testing the efficiency and independence of attentional networks. Journal of Cognitive Neuroscience. 2002;14:340–347. doi: 10.1162/089892902317361886. [DOI] [PubMed] [Google Scholar]
- Fried R, Hirshfeld-Becker D, Petty C, Batchelder H, Biederman J. How informative is the CANTAB to assess executive functioning in children with ADHD? A controlled study. Journal of Attention Disorders. 2015;19:468–475. doi: 10.1177/1087054712457038. [DOI] [PubMed] [Google Scholar]
- Halperin JM, Schulz KP. Revisiting the role of the prefrontal cortex in the pathophysiology of attention-deficit/hyperactivity disorder. Psychological Bulletin. 2006;132:560–581. doi: 10.1037/0033-2909.132.4.560. [DOI] [PubMed] [Google Scholar]
- Hostinar CE, Stellern SA, Schaefer C, Carlson SM, Gunnar MR. Associations between early life adversity and executive function in children adopted internationally from orphanages. Proceedings of the National Academy of Sciences USA. 2012;109:17208–17212. doi: 10.1073/pnas.1121246109. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Humphreys KL, Gleason MM, Drury SS, Miron D, Nelson CA, Fox NA, Zeanah CH. Effects of institutional rearing and foster care on psychopathology at age 12 years in Romania: follow-up of an open, randomised controlled trial. Lancet Psychiatry. 2015;7:625–634. doi: 10.1016/S2215-0366(15)00095-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Johnstone SJ, Roodenrys S, Phillips E, Watt AJ, Mantz S. A pilot study of combined working memory and inhibition training for children with AD/HD. Attention Deficit Hyperactivity Disorders. 2010;2:31–42. doi: 10.1007/s12402-009-0017-z. [DOI] [PubMed] [Google Scholar]
- Kessler R, Adler L, Barkley R, Biederman J, Conners CK, Demler O, Faraone S, Greenhill L, Howes M, Secnik K, Spencer T, Ustun B, Walters E, Zaslavsky A. The prevalence and correlates of adult ADHD in the United States: results from the National Comorbidity Survey Replication. American Journal of Psychiatry. 2006;163:716–723. doi: 10.1176/appi.ajp.163.4.716. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Klingberg T, Fernell E, Olesen PJ, Johnson M, Gustafsson P, Dahlström K, Gillberg C, Forssberg H, Westerberg H. Computerized training of working memory in children with ADHD – a randomized, controlled trial. Journal of the American Academy of Child and Adolescent Psychiatry. 2005;44:177–186. doi: 10.1097/00004583-200502000-00010. [DOI] [PubMed] [Google Scholar]
- Kreppner JM, O’Connor TG, Rutter M, English & Romanian Adoptees (ERA) Study Team Can inattention/overactivity be an institutional deprivation syndrome? Journal of Abnormal Child Psychology. 2001;29:513–528. doi: 10.1023/a:1012229209190. [DOI] [PubMed] [Google Scholar]
- Lemery-Chalfant K, Schreiber JE, Schmidt NL, Van Hulle CA, Essex MJ, Goldsmith HH. Assessing internalizing, externalizing, and attention problems in young children: validation of the MacArthur HBQ. Journal of the American Academy of Child & Adolescent Psychiatry. 2007;46:1315–1323. doi: 10.1097/chi.0b013e3180f616c6. [DOI] [PubMed] [Google Scholar]
- Loman MM, Johnson AE, Westerlund A, Pollak SD, Nelson CA, Gunnar MR. The effect of early deprivation on executive attention in middle childhood. Journal of Child Psychology and Psychiatry. 2013;54:37–45. doi: 10.1111/j.1469-7610.2012.02602.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Luciana M, Nelson CA. Assessment of neuropsychological function in children through the Cambridge Neuropsychological Testing Automated Battery (CANTAB): normative performance in 4 to 12 year-olds. Developmental Neuropsychology. 2002;22:595–624. doi: 10.1207/S15326942DN2203_3. [DOI] [PubMed] [Google Scholar]
- MacKinnon DP, Lockwood CM, Hoffman JM, West SG, Sheets V. A comparison of methods to test mediation and other intervening variable effects. Psychological Methods. 2002;7:83–104. doi: 10.1037/1082-989x.7.1.83. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Martel M, Nikolas M, Nigg JT. Executive function in adolescents with ADHD. Journal of the American Academy of Child and Adolescent Psychiatry. 2007;46:1437–1444. doi: 10.1097/chi.0b013e31814cf953. [DOI] [PubMed] [Google Scholar]
- Martinussen R, Hayden J, Hogg-Johnson S, Tannock R. A meta-analysis of working memory impairments in children with ADHD. Journal of the American Academy of Child and Adolescent Psychiatry. 2005;44:377–384. doi: 10.1097/01.chi.0000153228.72591.73. [DOI] [PubMed] [Google Scholar]
- McDermott JM, Troller-Renfree S, Vanderwert R, Nelson CA, Zeanah CH, Fox NA. Psychosocial deprivation, executive functions and the emergence of socio-emotional behavior problems. Frontiers in Human Neuroscience. 2013;7:167. doi: 10.3389/fnhum.2013.00167. [DOI] [PMC free article] [PubMed] [Google Scholar]
- McLaughlin KA, Fox NA, Zeanah CH, Sheridan MA, Marshall P, Nelson CA. Delayed maturation in brain electrical activity partially explains the association between early environmental deprivation and symptoms of attention-deficit/hyperactivity disorder. Biological Psychiatry. 2010a;68:329–336. doi: 10.1016/j.biopsych.2010.04.005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- McLaughlin KA, Green JG, Gruber MJ, Sampson NA, Zaslavsky AM, Kessler RC. Childhood adversities and adult psychiatric disorders in the national comorbidity survey replication II: associations with persistence of DSM-IV disorders. Archives of General Psychiatry. 2010b;67:124–132. doi: 10.1001/archgenpsychiatry.2009.187. [DOI] [PMC free article] [PubMed] [Google Scholar]
- McLaughlin KA, Sheridan MA, Winter W, Fox NA, Zeanah CH, Nelson CA. Widespread reductions in cortical thickness following severe early-life deprivation: a neurodevelopmental pathway to attention-deficit/hyperactivity disorder. Biological Psychiatry. 2014;76:629–638. doi: 10.1016/j.biopsych.2013.08.016. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Merz EC, McCall RB. Parent ratings of executive functioning in children adopted from psychosocially depriving institutions. Journal of Child Psychology and Psychiatry. 2011;52:537–546. doi: 10.1111/j.1469-7610.2010.02335.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Merz EC, McCall RB, Groza V. Parent-reported executive functioning in post-institutionalized children: a follow-up study. Journal of Clinical Child & Adolescent Psychology. 2013;42:726–733. doi: 10.1080/15374416.2013.764826. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Nelson CA, Fox NA, Zeanah CH. Romania’s Abandoned Children: Deprivation, Brain Development, and the Struggle for Recovery. Harvard University Press; Cambridge, MA: 2014. [Google Scholar]
- Niendam TA, Laird AR, Ray KL, Dean YM, Glahn DC, Carter CS. Meta-analytic evidence for a superordinate cognitive control network subserving diverse executive functions. Cognitive, Affective and Behavioral Neuroscience. 2012;12:241–268. doi: 10.3758/s13415-011-0083-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Nigg JT. Is ADHD a disinhibitory disorder? Psychological Bulletin. 2001;127:571–598. doi: 10.1037/0033-2909.127.5.571. [DOI] [PubMed] [Google Scholar]
- Nigg JT, Nikolas M, Friderici K, Leeyoung P, Zucker RA. Genotype and neuropsychological response inhibition as resilience promoters for ADHD, ODD, and CD under conditions of psychosocial adversity. Development and Psychopathology. 2007;19:767–786. doi: 10.1017/S0954579407000387. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Pears KC, Fisher PA, Bruce J, Kim HK, Yoerger K. Early elementary school adjustment of maltreated children in foster care: the role of inhibitory control and caregiver involvement. Child Development. 2010;81:1550–1564. doi: 10.1111/j.1467-8624.2010.01491.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Pollak SD, Nelson CA, Schlaak MF, Roeber BJ, Wewerka SS, Wiik KL, Frenn KA, Loman MM, Gunnar MR. Neurodevelopmental effects of early deprivation in postinstitutionalized children. Child Development. 2010;81:224–236. doi: 10.1111/j.1467-8624.2009.01391.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Preacher KJ, Hayes AF. Asymptotic and resampling strategies for assessing and comparing indirect effects in multiple mediator models. Behavior Research Methods. 2008;40:879–891. doi: 10.3758/brm.40.3.879. [DOI] [PubMed] [Google Scholar]
- Rutter M, Kreppner JM, O’Connor TG, The English Romanian Adoptees (ERA) Study Team Specificity and heterogeneity in children’s responses to profound institutional privation. British Journal of Psychiatry. 2001;17:97–103. doi: 10.1192/bjp.179.2.97. [DOI] [PubMed] [Google Scholar]
- Rutter M, Sonuga-Barke E, Beckett C, Castle J, Kreppner J, Kumsta R, Schlotz W, Stevens S, Bell C, Gunnar M. Deprivation-specific psychological patterns: effects of institutional deprivation. Monographs of the Society for Research in Child Development. 2010;75:1–242. doi: 10.1111/j.1540-5834.2010.00550.x. [DOI] [PubMed] [Google Scholar]
- Schoemaker K, Bunte T, Wiebe SA, Espy KA, Dekovic M, Matthys W. Executive function deficits in preschool children with ADHD and DBD. Journal of Child Psychology and Psychiatry. 2012;53:111–119. doi: 10.1111/j.1469-7610.2011.02468.x. [DOI] [PubMed] [Google Scholar]
- Sergeant J. The cognitive-energetic model: an empirical approach to attention-deficit hyperactivity disorder. Neuroscience and Biobehavioral Reviews. 2000;24:7–12. doi: 10.1016/s0149-7634(99)00060-3. [DOI] [PubMed] [Google Scholar]
- Shallice T. Specific impairments in planning. Philosophical Transactions of the Royal Society of London. 1982;298:199–209. doi: 10.1098/rstb.1982.0082. [DOI] [PubMed] [Google Scholar]
- Slopen N, McLaughlin KA, Fox NA, Zeanah CH, Nelson CA. Alterations in neural processing and psychopathology in children raised in institutions. Archives of General Psychiatry. 2012;69:1022–1030. doi: 10.1001/archgenpsychiatry.2012.444. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sonuga-Barke E, Dalen L, Daley D, Remington B. Are planning, working memory, and inhibition associated with individual differences in preschool ADHD symptoms? Developmental Neuropsychology. 2002;21:255–272. doi: 10.1207/S15326942DN2103_3. [DOI] [PubMed] [Google Scholar]
- Spencer TJ, Biederman J, Mick E. Attention-deficit/hyperactivity disorder: diagnosis, lifespan, comorbidities, and neurobiology. Journal of Pediatric Psychology. 2007;32:631–642. doi: 10.1093/jpepsy/jsm005. [DOI] [PubMed] [Google Scholar]
- Stevens SE, Sonuga-Barke E, Kreppner JM, Beckett C, Castle J, Colvert E, Groothues C, Hawkins A, Rutter M. Inattention/overactivity following early severe institutional deprivation: presentation and associations in early adolescence. Journal of Abnormal Child Psychology. 2008;36:385–398. doi: 10.1007/s10802-007-9185-5. [DOI] [PubMed] [Google Scholar]
- Taylor E, Rogers JW. Practitioner review: early adversity and developmental disorders. Journal of Child Psychology and Psychiatry. 2005;46:451–467. doi: 10.1111/j.1469-7610.2004.00402.x. [DOI] [PubMed] [Google Scholar]
- UNICEF. At Home or in a Home? Formal care and adoption of children in Eastern Europe and Central Asia. UNICEF; Geneva, Swizerland: 2010. [Google Scholar]
- Wiik KL, Loman MM, Van Ryzin MJ, Armstrong JM, Essex MJ, Pollak SD, Gunnar MR. Behavioral and emotional symptoms of post-institutionalized children in middle childhood. Journal of Child Psychology and Psychiatry. 2011;52:56–63. doi: 10.1111/j.1469-7610.2010.02294.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Willcutt EG, Doyle AE, Nigg JT, Faraone SV, Pennington BF. Validity of the executive function theory of attention-deficit/hyperactivity disorder: a meta-analytic review. Biological Psychiatry. 2005;57:1336–1346. doi: 10.1016/j.biopsych.2005.02.006. [DOI] [PubMed] [Google Scholar]
- Zeanah CH, Egger HL, Smyke AT, Nelson CA, Fox NA, Marshall PJ, Guthrie D. Institutional rearing and psychiatric disorders in Romanian preschool children. American Journal of Psychiatry. 2009;166:777–785. doi: 10.1176/appi.ajp.2009.08091438. [DOI] [PubMed] [Google Scholar]
- Zeanah CH, Fox NA, Nelson CA. The Bucharest Early Intervention Project: case study in the ethics of mental health research. Journal of Nervous and Mental Disease. 2012;200:243–247. doi: 10.1097/NMD.0b013e318247d275. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Zeanah CH, Nelson CA, Fox NA, Smyke AT, Marshall P, Parker S, Koga S. Designing research to study the effects of institutionalization on brain and behavioral development: the Bucharest Early Intervention Project. Developmental Psychopathology. 2003;15:885–907. doi: 10.1017/s0954579403000452. [DOI] [PubMed] [Google Scholar]