

Abstract
Background:
Epidermoid and dermoid cyst comprise <1% of spinal tumors and may be congenital (hamartoma) or acquired (iatrogenic) in origin. Epidermoid cysts within the neuraxis are rare benign neoplasms that are most commonly located in the intracranial region.
Case Description:
Here, we report the a case of an acquired intradural extramedullary epidermoid cyst involving the thoracic region in an adult female who had no associated history of an accompanying congenital spinal deformity.
Conclusion:
Early diagnosis and immediate surgical intervention reduce patient morbidity. Near complete or subtotal excision of the cyst wall is warranted to prevent inadvertent injury to the spinal cord thus minimizing neurological morbidity.
Keywords: Acquired, congenital, epidermoid cysts, spinal tumors
BACKGROUND
Epidermoid cysts within the neuraxis are rare benign neoplasms that are commonly located intracranially. They account for <1% of all intraspinal tumors.[1,8] The “pearly spinal tumors” with smooth, glistening, white capsules are mostly intradural and extramedullary in location and may be congenital or acquired in origin. Here, we report an acquired thoracic epidermoid spinal tumor without any congenital spinal deformity.[2,7]
CASE DESCRIPTION
A 20-year-old female presented with a progressive thoracic myelopathy (numbness/difficulty in walking) of 5–6 months duration; she previously underwent some type of thoracic surgery (e.g., thoracic spine scar). Her neurological examination showed loss of motor function at the 3/5 levels in both legs accompanied by numbness in both legs. The thoracic magnetic resonance imaging (MRI) showed a well-defined intradural extramedullary mass on the right side of the spinal canal markedly compressing the cord extending from the D7/D8 to the D8/D9 levels (measuring approximately 3 cm × 1.7 cm × 1.5 cm). The tumor was isointense to hypointense on T1-weighted images, and hyperintense on T2-weighted studies [Figure 1]. At surgery, the soft grayish/white soft tumor and cyst and wall were fully resected, and the internal white fluid containing hair follicles were all removed [Figures 2 and 3]. Histopathology was consistent with an epidermoid cyst without malignancy (e.g., squamous-lined cyst with keratin debris) [Figure 4]. Postoperatively, the patient was neurologically intact and remained stable 6 months later.
Figure 1.

(a) Magnetic resonance imaging dorsolumbar spine showing well-defined intradural extramedullary mass lesion on the right side of the spinal canal extending from the D7/D8 to D8/D9 levels. (b) Magnetic resonance imaging showing isointense to hypointense mass lesion with signal intensity nearly comparable to the cord (e.g., isointense) on T1-weighted images (c) Magnetic resonance imaging showing hyperintense signal intensity of the lesion on T2-weighted images with associated mass effects
Figure 2.
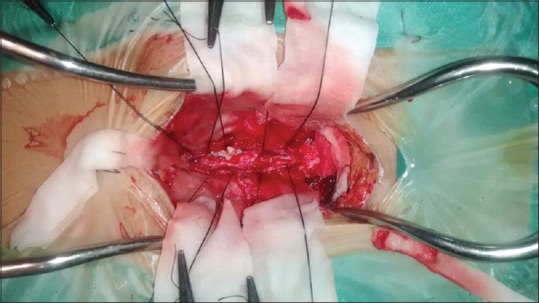
Intraoperative photograph showing grayish white soft tissue tumor containing hair follicles
Figure 3.
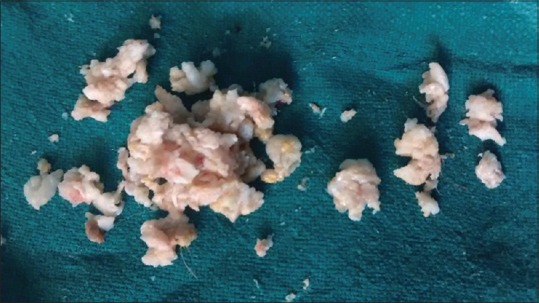
Intraoperative photograph showing excised tumor tissue
Figure 4.
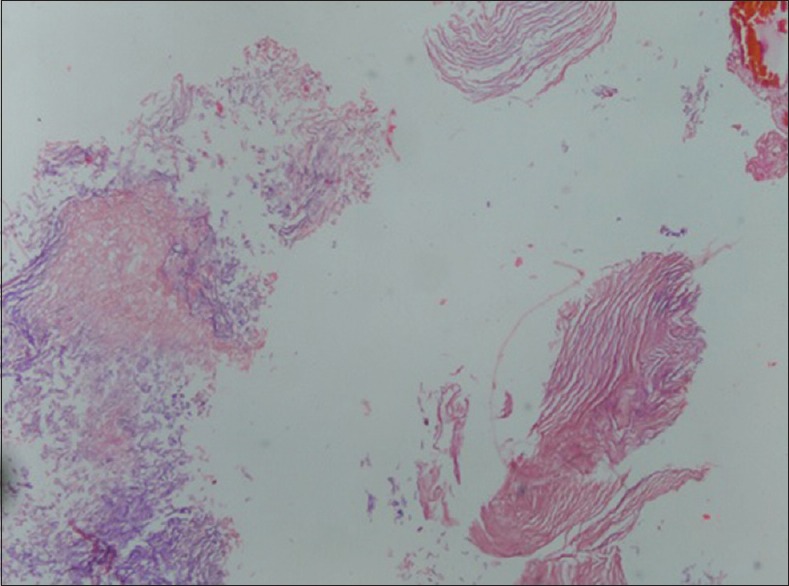
Microphotograph (H and E, ×100) showing predominantly laminated keratin, anucleated squames
DISCUSSION
Frequency spinal epidermoid tumors
In adults, epidermoids more commonly affect the cranium versus the spine (ratio 6:1).[4] Epidermoid and dermoid cyst comprise <1% of spinal tumors and may be congenital (hamartoma) or acquired (iatrogenic) in origin.[6]
Location of spinal epidermoid tumors
Spinal dermoids can be extradural, intradural extramedullary, or intramedullary. The most common site of occurrence of these tumors is the lumbosacral region (60%), followed by the thoracic (10%), and cervical regions (5%).
Histopathology of epidermoid/dermoid tumor
The histopathology of dermoid and epidermoid cysts is usually based on their typical contents. Classically, they are lined by stratified squamous epithelium supported by an outer layer of collagenous tissue with a soft white material toward the interior of the cyst as a result of progressive desquamation of keratin from epithelial lining.[3]
Magnetic resonance imaging findings for epidermoid tumors
Preoperative MRI using fat-suppressed sequences for these lesions usually demonstrate homogenous intensity combined with heterogeneous intensity. Sometimes calcification is also seen in the walls with hair and cartilaginous tissue.[9]
Surgical recommendation: Early gross total excision
The mainstay of treatment for these lesions is gross total surgical excision. If there is adherence of the cyst wall to critical neural elements partial resection will suffice, resulting in a low recurrence rates (10% or less).[5] Certainly, early diagnosis with immediate surgical intervention reduces patient morbidity.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Footnotes
Contributor Information
Kulwant Singh, Email: neurosurgeryimsbhu@gmail.com.
Sharad Pandey, Email: drsharad23@yahoo.com.
Praveen Kumar Gupta, Email: dr.praveen1965@gmail.com.
Vivek Sharma, Email: luckin2010@gmail.com.
Deepa Santhosh, Email: dr.dee.san@gmail.com.
Amrita Ghosh, Email: amrita_lko@rediffmail.com.
REFERENCES
- 1.Amato VG, Assietti R, Arienta C. Intramedullary epidermoid cyst: Preoperative diagnosis and surgical management after MRI introduction. Case report and updating of the literature. J Neurosurg Sci. 2002;46:122–6. [PubMed] [Google Scholar]
- 2.Baba H, Wada M, Tanaka Y, Imura S, Tomita K. Intraspinal epidermoid after lumbar puncture. Int Orthop. 1994;18:116–8. doi: 10.1007/BF02484422. [DOI] [PubMed] [Google Scholar]
- 3.Ferrara P, Costa S, Rigante D, Mule A, D’Aleo C, Pulitanò S, et al. Intramedullary epidermoid cyst presenting with abnormal urological manifestations. Spinal Cord. 2003;41:645–8. doi: 10.1038/sj.sc.3101482. [DOI] [PubMed] [Google Scholar]
- 4.Kumar S, Gulati DR, Mann KS. Intraspinal dermoids. Neurochirurgia (Stuttg) 1977;20:105–8. doi: 10.1055/s-0028-1090362. [DOI] [PubMed] [Google Scholar]
- 5.Lunardi P, Missori P, Gagliardi FM, Fortuna A. Long-term results of the surgical treatment of spinal dermoid and epidermoid tumors. Neurosurgery. 1989;25:860–4. doi: 10.1097/00006123-198912000-00002. [DOI] [PubMed] [Google Scholar]
- 6.Pandey S, Sharma V, Shinde N, Ghosh A. Spinal intradural extramedullary mature cystic teratoma in an adult: A rare tumor with review of literature. Asian J Neurosurg. 2015;10:133–7. doi: 10.4103/1793-5482.161181. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Park JC, Chung CK, Kim HJ. Iatrogenic spinal epidermoid tumor. A complication of spinal puncture in an adult. Clin Neurol Neurosurg. 2003;105:281–5. doi: 10.1016/s0303-8467(03)00040-4. [DOI] [PubMed] [Google Scholar]
- 8.Roux A, Mercier C, Larbrisseau A, Dube LJ, Dupuis C, Del Carpio R. Intramedullary epidermoid cysts of the spinal cord. Case report. J Neurosurg. 1992;76:528–33. doi: 10.3171/jns.1992.76.3.0528. [DOI] [PubMed] [Google Scholar]
- 9.Scarrow AM, Levy EI, Gerszten PC, Kulich SM, Chu CT, Welch WC. Epidermoid cyst of the thoracic spine: Case history. Clin Neurol Neurosurg. 2001;103:220–2. doi: 10.1016/s0303-8467(01)00156-1. [DOI] [PubMed] [Google Scholar]