

Abstract
Background
Obesity is increasingly prevalent disease worldwide and bariatric surgery is the most effective treatment for the most severe cases. The Roux-en-Y gastric bypass is still the most used technique all over the world and the laparoscopic approach has been preferred by surgeons with different approaches, propositions and techniques in performing the procedure.
Aim
To report the surgical aspects of the systematization and results of the simplified laparoscopic gastric bypass (Brazilian technique).
Methods
Were included all patients undergoing this procedure from January 2001 to July 2014; were described and analyzed aspects of this technique, the systematization and complications associated with the procedure.
Results
A total of 12,000 patients (72% women) were included, with a mean age of 43 years (14-76) and a mean BMI of 44.5 (35-90 kg/m2). Mean total operative time was 72 minutes (36-270) and the mean hospital stay was 36 hours. There were 303 cases of gastrojejunostomy stenosis (2.5%), 370 patients had gastrointestinal bleeding (3%) with only one lap revision due to a enteroanastomosis bleeding and six revisions related to intestinal obstruction caused by impacted clots in the jejunojenunostomy. Blood transfusion was needed in 32 patients (0.3%); Petersen hernia was diagnosed in 18 (0.15%) and digestive fistula in 54 (0.45%), which led to reoperation in 43 of them (67%). The overall mortality was 0.1% (fistula with sepsis=8, pulmonary thromboembolism=3; intestinal obstruction associated with sepsis=1).
Conclusion
The simplified laparoscopic gastric bypass is a feasible and safe option with low complication rate and easy reproducibility for education and training in bariatric surgery.
Keywords: Bariatric surgery, Gastric bypass, Obesity
Abstract
Racional
A obesidade é doença de prevalência crescente no mundo todo e a cirurgia bariátrica é o tratamento mais eficaz para os graus mais severos. O bypass gástrico em Y-de-Roux ainda é a opção técnica mais utilizada no mundo e a via de acesso laparoscópica tornou-se rapidamente a opção preferencial dos cirurgiões, com diversas variações e proposições técnicas na execução do procedimento.
Objetivo
Relatar os aspectos técnicos da sistematização cirúrgica e resultados do bypass gástrico laparoscópico simplificado (bypass brasileiro).
Métodos
Foram incluídos todos os pacientes submetidos a este procedimento entre janeiro de 2001 a julho de 2014. Foram descritos e analisados aspectos da sistematização técnica simplificada e as complicações associadas ao procedimento.
Resultados
No período, 12.000 pacientes (72% de mulheres) foram incluídos, com média de idade de 43 anos (14-76) e com IMC médio de 44,5 (35-90 kg/m2). O tempo operatório total médio foi de 72 minutos (36-270) e a permanência hospitalar média foi de 36 horas. Ocorreram 303 casos de estenose na gastroenteroanastomose (2,5%), 370 pacientes tiveram hemorragia digestiva (3%) com necessidade de reoperação de apenas um deles por sangramento da enteroanastomose e seis pacientes foram reoperados por obstrução na enteroanastomose causada por impactação de coágulos. Transfusão sanguínea foi necessária em 32 pacientes (0,3%); hérnia de Petersen foi diagnosticada em 18 (0,15%) e fístula digestiva em 54 (0,45%), o que levou à reoperação em 43 deles (67%). A mortalidade global foi de 0,1% (fístula com sepse=8; tromboembolismo pulmonar=3; obstrução intestinal com sepse associada=1).
Conclusão
O bypass gástrico laparoscópico simplificado é opção técnica factível e segura, com baixo índice de complicações e com fácil reprodutibilidade para ensino em cirurgia bariátrica.
INTRODUCTION
The prevalence of obesity in the United States almost doubled in the past 20 years and today reaches more than a third of Americans. While the number of overweight and obesity is stable around 65%, the percentage of morbidly obese is increasing yearly24,32. In Brazil, obesity and overweight has reached more than half of the population, and in recent years have shown increasing incidence and prevalence in the adult population as in childhood and youth15.
Long-term studies have shown a clear relationship between obesity and mortality28,9 and, in cases in its most severe degrees, reduce the life expectancy of these individuals up to 20 years; also interferes with quality of life due to the association with severe comorbidities such as hypertension, diabetes mellitus type 2, sleep apnea, dyslipidemia and orthopedic disorders8. The bariatric surgery, in turn, has proven to be the most effective and long lasting treatment for morbid obesity and its comorbidities, reducing the morbidity and mortality of these patients, with much better results when compared to clinical approaches28,27.
The Roux-en-Y gastric bypass (RYGB), despite the recent growth in the indication of sleeve gastrectomy, is still the most worldwide performed procedure2 and considered by many as the gold standard technique. Since its original description in 1967 by Mason and Ito21 - initially with a horizontal pouch, wide gastroenterostomy and Billroth II reconstruction -, the RYGB has been undergoing a series of changes and technical improvements over time, resulting in the modern concept of vertical pouch, reconstruction in Roux-en-Y and calibrated anastomosis22,11,30,17,6,7,4. The biggest breakthrough, however, occurred with the adoption of laparoscopic access, which provided significant reduction in morbidity associated with it20.
The first case series of RYGB performed laparoscopically was published in 1994 by Wittgrove & Clark31, after two years of development of the technical model in experimental animals. The gastroenterostomy was performed with a circular stapler and enteroenterostomy entirely done with cutting linear staplers. At this time, few surgeons had experience and conditions for practicing the same technique, which meant, that most of them begin trying to operate laparoscopically exactly as in laparotomy12.
The first group of patients undergoing laparoscopic RYGB by Gastro-Obese-Center team in early 2001, occurred exactly this way. The technical steps of the operation were adapted by laparotomy to laparoscopy. Long gastric pouches with restriction ring placement, firstly performing the intestinal step and then the retrocolic and retrogastric gastroenterostomy. Operations were long, about 3-4 h and difficult to reproduce. Given the technical difficulties in the former cases, was chosen for develop systematization that could offer safety, but based on a simple and reproducible model that could serve, among other purposes, as a method of teaching and training. Furthermore, aimed to establish a new technical standard, already developed within the principles of laparoscopic surgery since the beginning. Based on this, a technique was devised which later became known as "simplified RYGB" or "Brazilian technique", currently broadcast worldwide.
The aim of this paper is to report the technical aspects of surgical systematization and results of the simplified laparoscopic RYGB.
METHODS
All patients undergoing laparoscopic RYGB from January 2001 to July 2014 were included. All, also, had formal and internationally recognized indication for bariatric surgery (body mass index - BMI equal to or greater than 40 kg/m2 or BMI equal or greater than 35 kg/m2 with comorbidities).
Preoperative preparation
After the initial consultation guidance, where they discussed the reasons for surgery - the most widely used techniques, the expected results, the importance of a multidisciplinary approach and the particularities of each patient - they were referred to complementary examinations and evaluations with endocrinologist, cardiologist, nutritionist, physiotherapist and psychologist. If there was a need, the psychologist asked the opinion of the psychiatrist. The tests included upper endoscopy with biopsy for histological study and research of Helicobacter pylori, total abdominal ultrasonography, pulmonary function tests and general laboratory tests. After that, the results were evaluated, the patient properly prepared and the operation scheduled. In conjunction with the anesthetic evaluation, was filled the informed consent form for admission, surgery and anesthesia.
Surgical technique
Position the patient and the surgical team
The operation was performed with the patient in the supine position with legs open and with 45 degrees inclined position. The fixation of the patient on the operating table was made by placing one belt on abdominal area and another below the level of the thighs. The surgeon stood between the legs, with the 1st assistant, who handled the camera and the auxiliary clamp, and the scrub on the right. Was not used bladder catheterization. Antibiotic prophylaxis was routinely used. Prevention of thromboembolism was made with use of graduated compression stockings, intermittent pneumatic boots, enoxaparin and compression, which was started before surgery and continued for 10 days after discharge. Disposable orogastric tube - Fouchet 32 Fr -, was routinely placed.
Pneumoperitoneum and placement of the trocars
The pneumoperitoneum was performed with direct puncture with a Veress needle in the left upper quadrant, near the costal margin at the level of the midclavicular line (Palmer's point). The initial pressure was set at 16 mmHg, and maintained till the expected pressure (from 15 to 16 mmHg) was reached. The operation was initiated by the placement of the 10 mm permanent trocars for introduction of 30 degrees optics/camera placed at mesogastrium between 12-15 cm below the xiphoid process and 3 cm to the left of the midline, considered as number 1 trocar. The number 2, of 5 mm, was placed near the xiphoid process for the use of liver retractor which was usually a stick/probe attached to the surgical field with the aid of Backaus forceps and surgical dressing. The number 3, disposable of 12 mm, was to be used by the surgeon's left hand, placed on the right side of the patient in an intermediate position between the previous two, 3-5 cm lateral to the midline. The number 4, also permanent of 5 mm, was placed along the left costal margin in the anterior axillary line to the 1st assistant. The last trocar, number 5, disposable of 12 mm, was placed adjacent to the left costal margin in the hemi-clavicular line to surgeon's right hand manipulation. The pneumoperitoneum was maintained by trocar number 5 (Figure 1).
Figure 1.

Positioning of the five trocars to perform the simplified RYGB
Gastric pouch construction
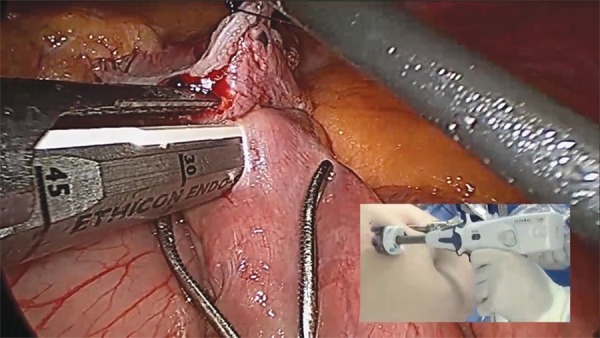
The preparation to create the gastric pouch was initiated with the dissection of the esophagogastric angle and the opening of the left gastrophrenic ligament with Ultracision®, so as to expose the lateral aspect of the left diaphragmatic pillar. Then, the exeresis of the fat pad of the esogastric junction (Belsey fat) was done. The lesser curvature dissection was performed, also with Ultracision®, with ligation of the second gastric vessel, getting access to the posterior gastric wall. In cases of use of restriction ring, dissection was initiated in the third vessel of the lesser curvature resulting in longer pouch to allow proper placement of the ring. The first firing of the linear cutting stapler was performed through trocar number 3 in the horizontal direction loaded with a 45 mm blue cartridge (Figure 2A). Then was initiated the dissection of retrogastric space until complete visualization of the left diaphragmatic crus, performing from there the vertical stapling through trocar number 5 in cranial direction, also with blue cartridges of 45 mm, finishing the gastric pouch and keeping safe distance from the esophagus of at least 0.5 cm from gastric tissue to esophagogastric angle (Figure 2B). Both the staple line of the bypassed stomach, as the gastric pouch (Figure 3) were submitted to continuous and transfixing suture reinforcement with absorbable sutures (3-0 Caprofyl®)
Figure 2.

A) Horizontal stapling - starting point in doing the gastric pouch; B) last vertical gastric stapling in making the pouch showing the technical detail with perfect visualization of the tip of the stapler near the esogastric angle and keeping safe distance to the esophagus
Figure 3.
Transfixing suture for continuous reinforcement of the staple line in the excluded stomach with absorbable sutures
Gastroenterostomy
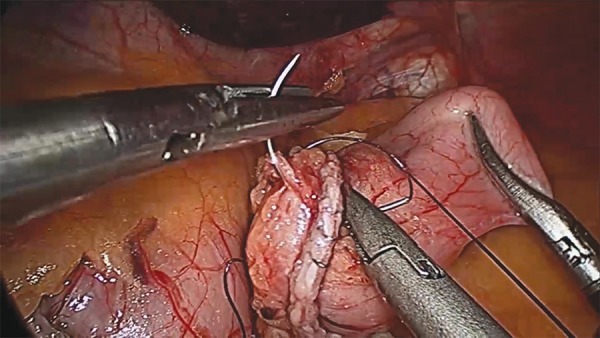
Aiming the ascent of the loop to the supramesocolic area for anastomosis, the greater omentum was mobilized to the upper abdomen and opened in its middle portion in the longitudinal direction, starting close to the colon in cranial direction. This maneuver allows easy access to duodenojejunal angle and initial segment of the jejunum, to define the length of biliopancreatic loop. Keeping the proximal part of the jejunum always to the right side of the surgeon, the loop was moved to the upper abdomen without division, similarly to the isoperistaltic Billroth II reconstruction. In this way, the surgeon can set the length of preference for biliopancreatic loop and the realization of gastroenterostomy. After doing two small holes with Ultracision® - one on the loop and the other on the posterior surface of the gastric pouch - and the stapler with white 45 mm cartridge, was performed gastroenterostomy with extension of only 15 mm using only the final portion of the stapler (Figure 4). The aperture was sutured with absorbable continuously seromuscular thread (Caprofyl® 3-0) having a 32 Fouchet Fr probe for calibration. Finished the suture, the probe was removed allowing the biggest adjustment to the final caliber of the anastomosis. Separate seromuscular sutures with nonabsorbable sutures (Ethibond® 2-0) were performed in three of the anastomotic angles: medial, lateral and internal.
Figure 4.
Stapler positioned to perform the gastroenterostomy calibrated with 15 mm probe
Petersen space closure
With superior traction of the mesocolon - close to the medial part of the transverse colon toward to the liver -, the Petersen space was closed with nonabsorbable continuous suture (Ethibond® 2-0), starting in the distal angle between the mesocolon and mesentery of the alimentary loop and going up to the edge of the transverse colon and jejunum (Figure 5). In this surgical step was taken great care to prevent bleeding or hematoma in mesentery.
Figure 5.
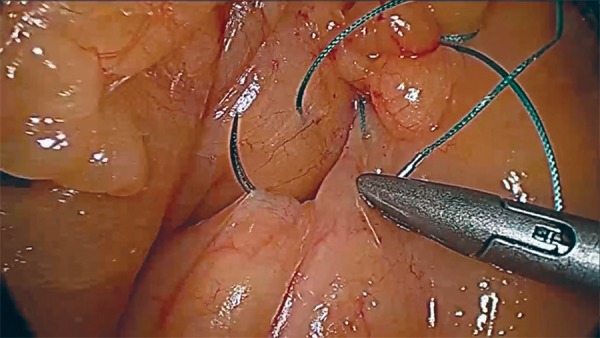
Continuous suture with nonabsorbable sutures to close the Petersen space
Enteroenterostomy
From the gastroenterostomy, in distal jejunum direction and according to the surgeon's preference, was measured the segment of jejunum to be anastomosed to the biliopancreatic loop on the afferent portion of the gastroenterostomy, thereby determining the length of the alimentary loop (Figure 6A).
Figure 6.

A) Definition of the length of the alimentary loop for enteroenterostomy with the biliopancreatic loop (AA=alimentary loop, AC=common loop; BP= biliopancreatic loop); B) section of the biliopancreatic loop near the gastroenterostomy for conversion technique in Roux-en-Y
The enteroenterostomy was performed in the anisoperistaltic way, with 45 mm white cartridge stapler. After reviewing the possibility of internal bleeding on the stapler line, the incision was sutured with absorbable sutures (3-0 Caprofyl®) with seromuscular continuous suture. The mesenteric defect was also closed with a continuous suture with nonabsorbable suture (2-0 Ethibond®).
After test with about 250 ml of saline solution stained with 10 ml of methylene blue introduced through Fouchet probe, it was possible to verify the integrity of the two anastomoses (which were connected as Billroth II). Then, the portion corresponding to biliopancreatic loop was sectioned along the gastroenterostomy to convert the initial format of double omega to Roux-en-Y technique (Figure 6B).
When indicated, one tubular silicone drain was exteriorized through the trocar number 4. The trocars, then, were removed under direct visualization and in case of bleeding the corresponding incision was sutured with Vicryl® 0 and the skin with absorbable sutures (3-0 Monocryl ), intradermal, in separate sutures.
RESULTS
During the study period 8,640 women (72%) and 3,360 men (28%) underwent laparoscopic RYGB totaling 12,000 patients. The average age was 43 years (14-76) and the mean BMI of 44.5 kg/m2 (35-90). The weight ranged from 86 kg (minimum) to 286 kg (maximum), with an average of 123 kg. Mean total operative time was 72 minutes, ranging from 36 minutes (minimum) and 270 minutes (maximum).
The mean hospital stay was 36 hours. There were 303 cases of gastroenterostomy stenosis (2.5%), and endoscopic balloon dilation was required in 214 patients (70%). Twelve had hematemesis postoperatively (0.1%) and 358 had rectal bleeding or melena (2.9%). There was need for reoperation for bleeding in one patient (bleeding in enteroenterostomy). Bleeding with impaction of clot causing obstruction of this anastomosis was responsible for six surgical interventions postoperatively. Of the total number of operated patients, 32 required blood transfusion (0.3%).
Petersen hernia was diagnosed in 18 patients (0.15%) and two cases of acute intestinal obstruction by herniation occurred in the mesenteric space. Fistula was observed in 54 patients (0.45%), which led to reoperation in 43 of them (67%). Twenty-seven patients presented collections at CT examination without diagnosis of fistula (0.22%). Of these, 17 required reoperation for drainage (63%).
The overall mortality was 0.1% (12 patients), fistula associated with progression to sepsis accounted for eight cases, three cases of pulmonary embolism and one patient died of sepsis associated with intestinal obstruction.
DISCUSSION
The RYGB was first described in 1967 as horizontal gastroplasty and a Billroth II gastroenterostomy, without concern for the size of the gastric pouch (reduction of 70-90%) and the size of gastroenterostomy which was usually between 20-30 mm21. Later adaptations in relation to the size of the gastric pouch with reduction of fundic segment and the caliber of the gastroenterostomy to about 12 mm, got better weight loss and control of dumping symptoms22.
Based on the principles of César Roux gastrectomy, the reconstruction of the RYGB started being made with Roux-en-Y technique since 1977, based on the proposition of Griffen11 in order to avoid the occurrence of bilious vomiting in the postoperative period. The gastroplasty produced reduction to approximately 90% of the gastric capacity, the gastroenterostomy was calibrated at 12 mm and the alimentary loop was of 30 cm in length.
The exclusive use of small curvature for the construction of the gastric pouch began in 1983 with Torres&Oca30, in order to reduce the risk of vascular lesions and spleen, and to facilitate the gastroenterostomy. The technique was based on gastric reduction (gastroplasty) of 95%, 4 cm gastric pouch at the small curvature, gastroenterostomy with a 1 cm circular stapler, 45 cm of biliopancreatic loop and extension of 90 cm.
The use of restriction ring was designed at the beginning of 1980's17, and became widely used only after 10 years6. The material used varied between the meshes of polypropylene, silicone ring and the aponeurosis fascia, always with the goal of reducing the incidence of migration and slip ring.
The RYGB performed with the design and technical principles known today, had its beginning in the operation proposed by Fobi and Capella - the first author indicated the technique as primary surgery for obesity treatment7 and the second initially as conversion of Mason gastroplasty procedure4 -, resulting pouch with triangular format in Fobi's or rectangular in Capella's proposals.
In Brazil, this procedure was initially widespread during the 90s, with gastric pouch of 5 cm in the small curvature, using restriction ring of 5.5 cm, retrocolic alimentary loop of 100 cm and bliopancreatic loop of 60 cm.
The laparoscopic procedure was proposed in 1994, with a gastric pouch of 15-20 ml, a gastroenterostomy retrogastric with circular stapler of 21 mm with the ogive placed through the mouth, and enetroentrostomy with linear stapling. Were not performed manual sutures and operating time varied a 3.5 to 7 hours31.
Gastroenterostomy and stenosis
The realization of gastroenterostomy is considered the most important step of RYGB, since its size seems to be a major factor in the loss of weight of the morbidly obese patient. Studies indicate that proper size, with less than 2 cm caliber, contributes to proper weight loss, while larger than 2 cm or suffering dilation over time anastomoses may result in failure in weight loss or even weight regain29,3. Moreover, gastroenterostomy is the most frequent site of more serious and severe complication of RYGB: digestive fistula.
In the present series, between 2001 and 2002, the gastroenterostomy was performed in uncalibrated manner, resulting in a final diameter greater than 2 cm. In the initial study, it has been found unsatisfactory weight loss of about 30% of patients. Furthermore, with the use of nonabsorbable suture (2-0 Ethibond®), was observed rate of stricture requiring endoscopic dilatation of almost 4%. To enhance the weight loss, over the followed two years (2003 and 2004), gastroenterostomy continued to be performed with the same nonabsorbable sutures, but now calibrated with 15 mm in diameter. The result was an improvement in weight loss, but the rate of stenosis requiring endoscopic dilation doubled, reaching 7.9%. The outcome of patients who passed dilatation, even using smaller balloon dilation of 2 cm, did not maintain the same standard of weight loss in comparison to the ones without dilation, compromising the operation result.
In a third phase, the gastroenterostomy began to be performed with absorbable suture (PDS 3-0) and calibrated to less than 15 mm. The rate of stenosis requiring dilatation decreased to 0.8%, and the weight loss results were satisfactory. Currently, it is performed with 15-20 mm of linear stapler extension, the incision closed with continuous seromuscular suture with absorbable sutures (3-0 Caprofyl®) and strengthening the three angles with nonabsorbable suture (2-0 Ethibond®) in order to decrease the tension on the anastomosis and collaborate with maintaining the caliber of gastroenterostomy in the long term.
Fistula
The occurrence of fistula in gastroenterostomy is great concern for the surgeon in the evolution of RYGB, since it is directly associated with increased morbidity and mortality. In addition, complications such as fistula appear to be directly related to the learning curve12,23.
In this series, the largest number of fistulas occurred during the first year, with a rate of 8.3%. In the second, there was a decrease to 4.6% and to 1.8% in the third. From the fourth year, the fistula rate has always remained below 2%, reducing year after year, until reaching the current rate of 0.28%. In the period in which it was used drainage as routine, it not only collaborated in the diagnosis - in the sense that the purulent discharge could be observed or allowed to perform testing with methylene blue - as well as collaborating in the treatment, since 35% of patients did not require reoperation, since they were in appropriate clinical conditions and with the fistula drained. Usually, fasting, nutritional support and antibiotic therapy resulted in healing of the fistula and improves these patients. As for the other 65%, surgical intervention was required, also made by laparoscopic access, in order to perform cleaning and adequate drainage of the cavity and sometimes by suturing the fistulous opening. In addition, it was performed routinely gastrostomy both for decompression and for establishing a route of early enteral feeding. They avoided the need for parenteral nutrition, resulting in lower risk of complications, less hospitalization time and reduced costs associated with treatment.
Mesenteric spaces and internal hernias
The reconstruction of the digestive transit with an antecolic/retrogastric pathway loop for food, leads the formation of two mesenteric spaces where internal hernias may occur18. The first is in the mesentery near the enteroenterostomy, represented by the junction of the mesenteries of the alimentary and biliopancreatic loops18. All patients had this mesenteric aperture sutured, and even that, there is in this series two cases of hernias in this space. The second is between the mesentery of the alimentary loop and the transverse mesocolon, known as space of Petersen18,13. Interestingly, the space described by the German surgeon Walther Petersen is the space in retrocolic opening formed by the transverse colon, the stomach (gastric pouch), alimentary loop and the retroperitonium26 and, by analogy, the concept was taken to laparoscopic surgery with antecolic reconstruction.
In this study, the first three years with laparoscopic RYGB, the Petersen space was not closed routinely. Although the number of internal hernias has not been great, the complications that can result from bowel herniation through this space can be severe, often delayed in diagnosis and with the possibility of acute incarceration and subsequent strangulation of large intestinal segments13. The difficulty in diagnosis is due to the fact that these patients usually present atypical clinical features, without the features normally expected for obstructive acute abdomen, such as nausea, vomiting, abdominal distension, stop elimination of flatus and feces and typical radiological appearance with distension and hydro-aerial levels1,5. This atypical presentation is due to the fact that, at the beginning, sub-occlusion is more related to the biliopancreatic loop, with the maintenance of transit by the alimentary one1. As these patients, in general, are not evaluated in the emergency sector by bariatric surgeon, but by physician or surgeon general, the diagnosis may be confused or slowed down, allowing the risk of ischemic necrosis, which can lead to severe sepsis , large bowel resections and high mortality rates1.
Based on this, from the fourth year of experience in laparoscopic RYGB, was adopted the systematic closure of the space of Petersen by continuous suture with nonabsorbable suture (Ethibond® 2-0), which begins in the angle between the mesocolon and mesentery and continues until the end of the space, adjacent to the transverse colon. The longitudinal opening of the greater omentum, made in order to facilitate access to supramesocolic food loop, facilitates this closure, since the omentum is not going to be positioned in this space, which could technically difficult the suture. It is necessary that the suture be made to avoid bruising and bleeding, and not allowing small spaces between sutures, which can enable incarceration and strangulation of the herniated intestinal loop more easily.
Abdominal cavity drainage
Postoperative complications such as fistulas, seem to be more frequent during the beginning of the series (learning curve). With better technical training and experience occur naturally decrease in the rate of complications and mortality12,14. The routine use of drainage of the peritoneal cavity seems to bring more security to the surgeon early in his experience because he expects the drain facilitates, and even anticipate, the diagnose of complications such as bleeding and fistulas. In addition, the surgeon thinks that the drain can prevent reoperation. However, comparative study of the same surgical team in two periods, with and without routine drainage, showed that there seems to be no difference in the outcome of patients undergoing BGYR16.
It was noted that the systematic use of drainage could cause local pain and discomfort to the patient and provide a slight increase in hospitalization. Furthermore, it is known that abdominal drain may be possible source of infection, since even with closed and the negative pressure system may be retrograde contamination. Due to the low incidence of fistulas and bleeding in recent years in this series, five years ago it was decided to no longer use the routine abdominal drainage, reserving this practice only for selected cases. As a result, could be observed better comfort to patient with less pain and greater ease of movement and ambulation, and consequent shorter hospitalization and recovery.
Using restriction ring
Aiming to improve the outcome of weight loss for three years (2003-2005) the use of a constricting ring in gastric pouch was a routine. Originally consisted of a silicone tube with 3 mm thick and 6.5 cm in length, which was inside a nonabsorbable suture (Ethibond® 2) thread used to tie the ring. After this initial period, a specific model of ring that allowed better fit to the gastric pouch, from 5.5 to 7.2 cm in diameter, was used. The ring constraint was used in 2,347 patients during these three years producing both a favorable effect on the loss and weight maintenance over time; this experience was confirmed by others19. The large initial concern was with the erosion and migration of the ring to the gastric lumen, which over time was not confirmed, since this occurrence was less than 2%. Already the slippage of the ring to distal positions was much more frequent, and often resulted in signs and symptoms such as vomiting, epigastric pain, heartburn and important food intolerances that compromised the very quality of life of patients. However, even those patients with poorly adapted to RYGB ring, which pose serious food problems, avoided cogitate its withdrawal, for fear of regained weight. Some patients come to evolve into important nutritional deficits, with BMI below 20 kg/m2.
After three years of experience with RYGB ring, and analyzing risk and benefit, in 2006 was chosen to abandon of the use of restriction ring.
Training and reproducibility
From the beginning the simplified RYGB proved good applicability for teaching and training in bariatric surgery, even with the possibility of shortening the learning curve, reducing surgical time and improving outcomes. After being presented in a Congress of the Brazilian Society of Metabolic and Bariatric Surgery (SBCBM) was quickly adopted by several teams as a technique of choice. Also came to be used as a model in training courses for Brazil and other countries, getting known internationally as "Brazilian technique" for performing laparoscopic RYGB.
More recently, this same surgical systematization started to be performed by robotic platform (Da Vinci Surgical System, Intuitive Company, Sunnyvalle, CA), with the same security, the same technical facility and although the series yet is still small, with the same good results25.
CONCLUSION
The simplified laparoscopic RYGB is feasible and safe option technique with low complication rates and easy reproducibility and applicability in the teaching of bariatric surgery.
Footnotes
Conflicts of interest: none
Financial source: none
REFERENCES
- 1.Agaba EA, Gentles CV, Shamseddeen H, Sasthakonar V, Kandel A, Gadelata D, Gellman L. Retrospective analysis of abdominal pain in postoperative laparoscopic Roux-em-Y gastric bypass patients: is a simple algorithm the answer? Surg Obes Rel Dis. 2008;4:587–593. doi: 10.1016/j.soard.2007.10.015. [DOI] [PubMed] [Google Scholar]
- 2.Banka G, Woodard G, Hernandez-Boussard T, Morton JM. Laparoscopic vs Open Gastric Bypass Surgery Differences in Patient Demographics, Safety, and Outcomes. Arch Surg. 2012;147:550–556. doi: 10.1001/archsurg.2012.195. [DOI] [PubMed] [Google Scholar]
- 3.Baretta GA, Alhinho HC, Matias JE, Marchesini JB, de Lima JH, Empinotti C, Campos JM. Argon Plasma Coagulation of Gastrojejunal Anastomosis for Weight Regain After Gastric Bypass. Obes Surg. 2014 Jul 09; doi: 10.1007/s11695-014-1363-2. [Epub ahead of print] [DOI] [PubMed] [Google Scholar]
- 4.Capella RF, Capella JF, Mandac H, Nath P. Vertical banded gastroplasty - gastric bypass: preliminary report. Obes Surg. 1991;1:389–395. doi: 10.1381/096089291765560782. [DOI] [PubMed] [Google Scholar]
- 5.Carucci LR, Turner MA, Shaylor SD. Internal hernia following Roux-em-Y gastric bypass surgery for morbid obesity: evaluation of radiographic findings at small-bowel examination. Radiology. 2009;251:762–770. doi: 10.1148/radiol.2513081544. [DOI] [PubMed] [Google Scholar]
- 6.Drew RL, Linner JH. Revisional surgery for severe obesity with fascia banded stoma Roux-en-Y gastric bypass. Obes Surg. 1992;2:349–354. doi: 10.1381/096089292765559945. [DOI] [PubMed] [Google Scholar]
- 7.Fobi MA. Why the operation I prefer is silastic ring vertical gastric bypass. Obes Surg. 1991;1:23–26. doi: 10.1381/096089291765560854. [DOI] [PubMed] [Google Scholar]
- 8.Fontaine KR, Redden DT, Wang C, Westfall AO, Allison DB. Years of life lost due to obesity. JAMA. 2003;289:187–193. doi: 10.1001/jama.289.2.187. [DOI] [PubMed] [Google Scholar]
- 9.Freedman DM, Ron E, Ballard-Barbash R, Doody MM, Linet MS. Body mass index and all-cause mortality in a nationwide US cohort. Int J Obes (Lond) 2006;30:822–829. doi: 10.1038/sj.ijo.0803193. [DOI] [PubMed] [Google Scholar]
- 10.Garrido AB. Cirurgia em obesos mórbidos - experiência pessoal. Arq Bras Endocrinol Metab. 2000;44(1):106–113. [Google Scholar]
- 11.Griffen WO, Jr, Young VL, Stevenson CC. A prospective comparison of gastric and jejunoileal bypass procedures for morbid obesity. Ann Surg. 1977;186(4):500–507. doi: 10.1097/00000658-197710000-00012. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Higa KD, Boone KB, Ho T. Complication of the laparoscopic Roux-en-Y gastric bypass: 1040 patients - What have we learned? Obes Surg. 2000;10:509–513. doi: 10.1381/096089200321593706. [DOI] [PubMed] [Google Scholar]
- 13.Higa KD, Ho T, Boone KB. Internal Hernias after laparoscopic Roux-em-Y gastric bypass: incidence, treatment and prevention. Obes Surg. 2003;13:350–354. doi: 10.1381/096089203765887642. [DOI] [PubMed] [Google Scholar]
- 14.Hollenbeak CS, Rogers AM, Barrus B, Wadiwala I, Cooney RN. Surgical volume impacts bariatric surgery mortality: A case for centers of excellence. Surgery. 2008;144:736–743. doi: 10.1016/j.surg.2008.05.013. [DOI] [PubMed] [Google Scholar]
- 15.Instituto Brasileiro de Geografia e Estatística - IBGE . Pesquisa de Orçamentos Familiares - 2008-2009 - Antropometria e estado nutricional de crianças, adolescentes e adultos no Brasil. Ministério do Planejamento; 2010. [Google Scholar]
- 16.Kavaturu S, Rogers AM, Haluck RS. Routine Drain Placement in Roux-en-Y Gastric Bypass: An Expanded Retrospective Comparative Study of 755 Patients and Review of the Literature. Obes Surg. 2012;22:177–181. doi: 10.1007/s11695-011-0560-5. [DOI] [PubMed] [Google Scholar]
- 17.Laws HL, Piantadosi S. Superior gastric reduce procedure for morbid obesity. Ann Surg. 1981;193(3):334–336. doi: 10.1097/00000658-198103000-00014. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Lockart ME, Tessler FN, Canon CL, Smith JK, Larrison MC, Fineberg NS, Roy BP, Clements RH. Internal hernia after gastric by-pass: sensitivity and specificity of seven CT signs with surgical correlation and controls. Radiology. 2007;188:745–750. doi: 10.2214/AJR.06.0541. [DOI] [PubMed] [Google Scholar]
- 19.Mali J, Jr, Herbella FAM, Valezi AC, Matsuo T, Menezes MA. Influence of the actual diameter of the gastric pouch outlet in weight loss after silicon ring Roux-em-Y gastric bypass: an endoscopic study. Obes Surg. 2010;20:1231–1235. doi: 10.1007/s11695-010-0189-9. [DOI] [PubMed] [Google Scholar]
- 20.Masoomi H1, Nguyen NT, Stamos MJ, Smith BR. Overview of outcomes of laparoscopic and open Roux-en-Y gastric bypass in the United States. Surg Technol Int. 2012;22:72–76. [PubMed] [Google Scholar]
- 21.Mason EE, Ito C. Gastric bypass. Ann Surg. 1969;170(3):329–336. doi: 10.1097/00000658-196909010-00003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Mason EE, Printen JK, Hartford CE, Boyd WC. Optimizing results of gastric bypass. Ann Surg. 1975;182(4):405–413. doi: 10.1097/00000658-197510000-00006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Nguyen NT, Rivers R, Wolfe BM. Factors Associated with Operative Outcomes in Laparoscopic Gastric Bypass. J Am Coll Surg. 2003;197:548–557. doi: 10.1016/S1072-7515(03)00648-3. [DOI] [PubMed] [Google Scholar]
- 24.Ogden CL, Carroll MD, Curtin LR, McDowell MA, Tabak CJ, Flegal KM. Prevalence of overweight and obesity in the United State, 1999-2004. JAMA. 2006;295:1549–1555. doi: 10.1001/jama.295.13.1549. [DOI] [PubMed] [Google Scholar]
- 25.Ramos AC, Domene CE, Volpe P, Pajecki D, D'Almeida LA, Ramos MG, Bastos EL, Kim KC. Early outcomes of the first Brazilian experience in totally robotic bariatric surgery. Arq Bras Cir Dig. 2013;26 Suppl 1:2–7. doi: 10.1590/s0102-67202013000600002. [DOI] [PubMed] [Google Scholar]
- 26.Rogers AM, Ionescu AM, Pauli EM, Meier AH, Shope TR, Haluck RS. When is a Petersen's Hernia not a Petersen's Hernia. J Am Coll Surg. 2008;207:121–124. doi: 10.1016/j.jamcollsurg.2008.01.019. [DOI] [PubMed] [Google Scholar]
- 27.Schauer PR, Bhatt DL, Kirwan JP, Wolski K, Brethauer SA, Navaneethan SD, Aminian A, Pothier CE, Kim ES, Nissen SE, Kashyap SR. Bariatric surgery versus intensive medical therapy for diabetes--3-year outcomes. N Engl J Med. 2014;370:2002–2013. doi: 10.1056/NEJMoa1401329. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Sjöström L, Narbro K, Sjöström CD, Karason K, Larsson B, Wedel H, Lystig T, Sullivan M, Bouchard C, Carlsson B, Bengtsson C, Dahlgren S, Gummesson A, Jacobson P, Karlsson J, Lindroos AK, Lönroth H, Näslund I, Olbers T, Stenlöf K, Torgerson J, Agren G, Effects of bariatric surgery on mortality in Swedish obese subjects. N Engl J Medicine. 2007;357(8):741–752. doi: 10.1056/NEJMoa066254. [DOI] [PubMed] [Google Scholar]
- 29.Smith C, Garren M, Gould J. Impacto f gastrojejunostomy diameter on long-term weight loss following laparoscopic gastric bypass: a follow-up study. Surg Endosc. 2011;25:2164–2167. doi: 10.1007/s00464-010-1516-x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Torres JC, Oca CF, Garrison RN. Gastric bypass: Roux-en-Y gastrojejunostomy from the lesser curvature. South Med J. 1983;76(10):1217–1221. [PubMed] [Google Scholar]
- 31.Wittgrove AC, Clark GW, Tremblay LJ. Laparoscopic gastric bypass, Roux-en-Y: preliminary report of five cases. Obes Surg. 1994;4:353–357. doi: 10.1381/096089294765558331. [DOI] [PubMed] [Google Scholar]
- 32.World Health Organization . Global Health Observatory Data Repository. Available in http://www.who.int/ [Google Scholar]