

Abstract
An infrequently studied and potentially promising physiological marker for posttraumatic stress disorder (PTSD) is pupil response. This study tested the hypothesis that arousal-related pupil responses to threat would be differentially expressed in trauma-exposed individuals with or without PTSD. Eye-tracking technology was used to evaluate pupil response to threatening and neutral images selected from the International Affective Picture System. Forty trauma-exposed individuals were recruited for participation between 2010–2014. Sixteen of them met diagnostic criteria for PTSD. Individuals with PTSD showed significantly more pupil dilation to threat-relevant stimuli compared to the neutral figural elements, and to trauma-exposed controls. Arousal-related pupil dilation significantly predicted PTSD after time elapsed since trauma, cumulative violence exposure, and trait anxiety were statistically controlled. The logistic regression model correctly classified 95% of the sample. Pupil reactivity shows promise as a physiological marker for PTSD.
Keywords: risk, physiological marker, biological marker
Although many individuals report experiencing a traumatic event, only 6.8% develop post-traumatic stress disorder (PTSD) following trauma (Kessler et al., 2005). Variability in trauma response depends on various factors including genetic variations that confer susceptibility to trauma (Zoldaz & Diamond, 2013), and the potency of different trauma types. Indeed, individuals exposed to violent interpersonal trauma are more likely to experience PTSD than those exposed to adverse events such as natural disasters (Kessler et al., 2005). Thus, while there is a relationship between trauma exposure and PTSD, trauma exposure alone does not predict PTSD.
Research to identify physiological markers for PTSD has been inconclusive (Zoladz & Diamond, 2013). A less studied and promising marker for PTSD is arousal-related pupil response. Pupillometry allows continuous measurements of involuntary physiological reactions to stimuli (Granholm & Steinhauer, 2004). Yet, few reports have examined whether it could serve as diagnostic marker of PTSD. For instance, among trauma-exposed civilians, pupil dilation to threat words increased irrespective of PTSD status (Felmingham, Rennieb, Manorb & Bryant, 2011). Lexical stimuli have low salience, limited similarity to naturally occurring stressors, and may not induce sufficient arousal. Threat visual stimuli show greater promise (Armstrong, Bilsky, Zhao & Olatunji, 2013); however, there is limited research in this regard. In one study, Iraq war veterans with high PTSD symptom severity exhibited more pupil dilation in response to threatening than neutral visual images (Kimble, Fleming, Bandy, Kim, & Zambetti, 2012). However, applicability of these findings to clinical samples is limited since only two individuals met diagnostic PTSD criteria.
The primary aim of this study was to evaluate the association of PTSD and arousal-related pupil responses in trauma-exposed individuals with or without PTSD. Two correlates of PTSD that could influence pupil response were also statistically controlled: trait anxiety and cumulative violence exposure. Experimental stimuli included threatening images, representing themes of traumatic victimization. Given the thematic similarity between prior violent trauma-exposure and threatening image content, it is plausible that arousal-related pupil responses vary as a function of cumulative trauma-exposure. Therefore, pupil responses were expected to be independent predictors of PTSD after controlling for trait anxiety and cumulative violence exposure.
Methods
Participants
Participants (n = 40) were recruited between 2010–2014 via advertisements in a Northeastern urban community. Prospective participants were told the research aimed to learn how people cope with stress and trauma. Participants were screened by telephone using the Trauma Screen Questionnaire (Brewin et al., 2001), which assesses the occurrence in the past two weeks of ten symptoms related to traumatic experiences. Participants were enrolled so there were roughly equal numbers of persons likely to meet criteria for PTSD or not.
Participants were 85% female, 57% single and 22% married with an average age of 35.5 years (SD = 11.63). Most participants were Black (68%) followed by White (23%), and Latino (5%). Thirteen percent graduated from college, 68% completed some college and 17% finished high school. Although more females (40%) met diagnostic criteria for PTSD than males (17%), this difference was not statistically significant, X2 (1, N = 40), 1.93, p = .16. Both groups had similar age, race/ethnicity, marital status, and educational attainment, X2 < 1.
Participants were excluded if they used reading glasses, consumed caffeine within four hours of participation, or wore eye makeup on the experimental day. Participants were informed of these exclusion criteria prior to signing up for the study; no one was excluded. Our Institutional Review Board granted permission to conduct this study. After complete description of the study, written informed consent was obtained. Participants received compensation ($150).
Apparatus
To monitor eye movements and pupil area, the Eyelink-1000 (SR research, Kanata, Ontario, Canada), a desktop mounted eye-tracking system with 0.01-dva-RMS resolution, 0.25–0.5 dva-accuracy, 1000 Hz temporal resolution and a wide field of view was used. The participants were seated on a height-adjustable kneeling chair, in a soundproof enclosure. To minimize head movements, a chin-rest and head-strap supported participants’ heads, and they were instructed not to move their head. Other than the computer screen used to present the visual stimuli, there was no source of light in the testing room.
Visual Stimuli
Respondents were monitored while viewing three different matched pairs of images (Fig. 1). Images from The International Affective Picture System (IAPS; Lang, Bradley, & Cuthbert, 2008) were selected to evoke emotions across a wide range of semantic categories, and have been rated for arousal and valence on a 9-point scale. To identify images of high threat content, images with valence and threat ratings greater than six were selected. For neutral images, we used images with neutral valence ratings at the scale midpoint and arousal ratings lower than the midpoint. Each threat-relevant image was matched to a neutral image in regard to the number, location and size of figural components, luminosity, and ethnicity of the protagonists.
Figure 1.
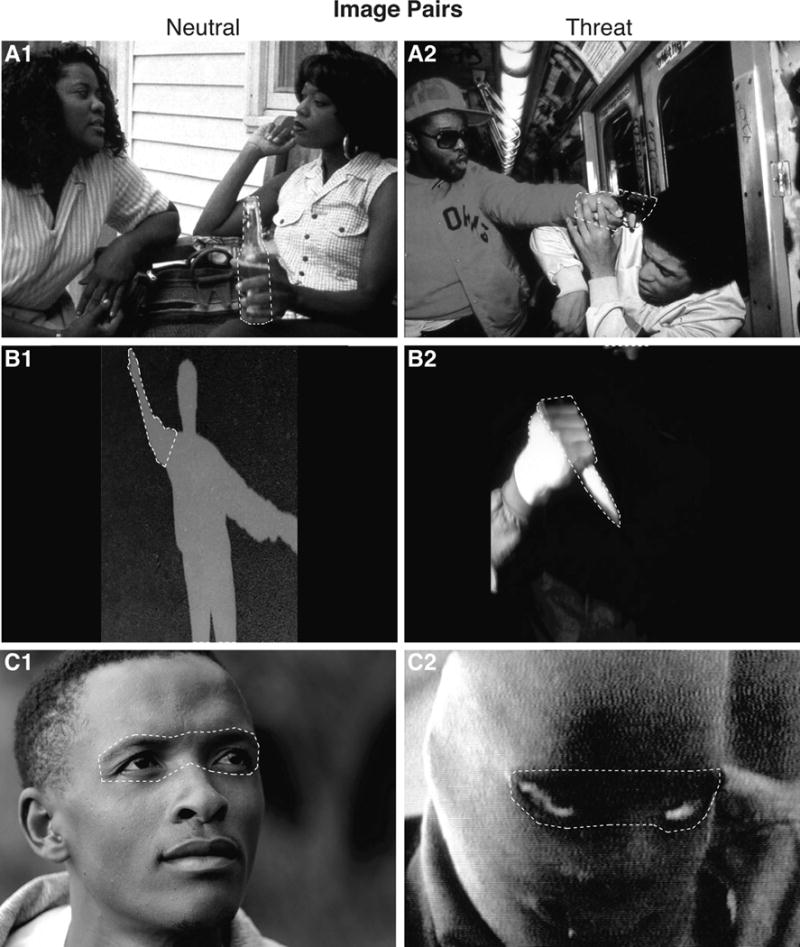
Visual stimuli used in the present study.
The participants were presented with three different matched pairs of images (A–C), each comprised of a neutral (1) and a threat-relevant (2) image. According to IAPS, the mean arousal ratings for males (M) and females (F) are as follows: threat image one (A2), M=6.8 (M) and M = 7.2 (F) and matched neutral image (A1), M = 3.8 (M) and M = 3.6 (F). The second threat image (B2), M = 6.4 (M) and M=6.8 (F), and matched neutral image (B1), M = 2.7 (M) and M = 3.2 (F). The third threat image (C2), M = 6.3 (M) and M = 6.6 (F) and matched neutral face (C1), M = 4.2 (M) and M = 3.5 (F). Regions, or interest areas, of each image with threatening elements were pre-identified and matched to similar regions in the neutral images for comparison. The interest areas are marked with dashed lines in this figure. However, these lines were not shown to the participants.
For each image, the most threatening element was pre-identified and matched to a similar region in the neutral images for comparison (see Fig. 1). The dashed lines superimposed on these images were not shown to the participants, but they defined the borders of interest areas used to quantify the participants’ pupil response to the most threatening aspects of each image.
Procedure
After obtaining self-report measures, and calibrating the eye-tracking system, the experiment began. Prior to each image, the computer screen displayed a dim gray background for 30 seconds. Images were presented sequentially for 30 seconds. Each threat image either preceded or followed its neutral image match; image presentation order was counterbalanced across participants. Participants were instructed to visually explore the images however they wished. Eye movements and pupil data were stored for off-line analyses. After the experiment, a licensed clinical psychologist evaluated respondents for PTSD diagnosis using the Clinician Administered PTSD Scale (CAPS). This interview was conducted after the experiment to avoid priming for heightened vigilance toward threat.
Arousal-related pupil response
Data elements were extracted using the Eyelink software. The pupil area for the entire viewing period of each image, and the pupil area while the individual gazed at the most threat-evoking element of the threatening image and matching figural element of the neutral image were measured.
Measures
The State Trait Anxiety Questionnaire
This scale differentiates between “state anxiety” and “trait anxiety.” Psychometric properties for this scale are well established (Spielberger, Reheiser, Ritterband, Sydeman, & Unger, 1995).
Trauma History Screen
Participants indicate how often 14 different traumatic events occurred: six items assess for violent victimization. Composite scores for violent victimization were computed based on the aggregate of events in each category. THS has demonstrated reliability and validity (Carlson et al., 2011).
CAPS
The CAPS is the gold standard in PTSD assessment (Blake et al., 1995). The CAPS’ psychometric properties are well established (Weathers, Keane, & Davidson, 2001). Individuals met diagnostic criteria if they attained at least one symptom of re-experiencing, three avoidance symptoms, and two arousal symptoms in the past month.
Results
Sixteen individuals met diagnostic criteria for PTSD and 24 were classified as trauma-exposed controls. Individuals with PTSD reported significantly more prior violent victimization experiences compared to trauma-exposed controls (M = 2.81, SD ± 1.33 and M = 1.37, SD ± 1.44, respectively), F(1, 39) = 6.86, p < .05. Time-elapsed since trauma was, M = 12.72 years, SD ± 12.39. Since response to threat could vary as a function of time since trauma, this variable was treated as a covariate in analyses.
Arousal-related pupil responses
Repeated MANCOVAs were conducted to evaluate differences in arousal-related pupil responses for PTSD, with elapsed time since trauma, cumulative violence exposure, and trait anxiety as covariates. Data were pooled across the three threat and three neutral images to create two composite scores. Threat and neutral images were treated as a within-subjects variable. To evaluate pupil responses to the threat-evoking elements of the threat images, pupil area for the threat-evoking elements was divided by pupil area during the entire viewing period of each threat image. We chose this stringent normalization method to control for any within-image pupil variation, as the individual must demonstrate increased pupil area while gazing at the most threat-evoking element relative to the entire image. The same procedure was used to normalize pupil responses while viewing the matching elements of the neutral images.
There were no group differences in average pupil area for neutral and threatening images (p’s > .20, Fig. 2B1). In contrast, the normalized pupil response to the threat-evoking element showed statistically significant effects for image, F(1,35) = 6.99, p < .01, image by PTSD interaction, F(1,35) = 7.94, p < .01, and group effect for PTSD, F(1,35) = 7.66, p < .01 (Fig. 2B2). Post hoc tests indicated that individuals with PTSD showed significantly higher arousal-related pupil dilation to the threat element compared to the neutral element, paired samples t(15) = 2.29, p < .05, and to trauma-exposed controls, F(1,39) = 6.41, p < .01. Individuals with PTSD showed a 35% increase in pupil dilation while viewing the threat element and an 8% increase while viewing the matching element of the neutral image. In contrast, trauma-exposed controls showed an 8% increase in pupil size while viewing the threat element and a 5% increase while viewing the neutral element.
Figure 2.
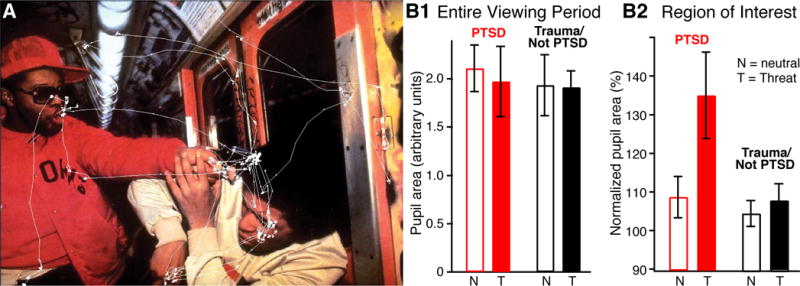
Pattern of visual exploration and differential pupil responses as a function of PTSD status.
(A) Visual exploration of an emotionally-arousing image. The eye movements are represented by a white line superimposed onto the image presented to a participant belonging to the PTSD group. (B1) Average pupil area (± SEM) during entire viewing period of neutral (N, empty bars) or threatening (T, filled bars) images in PTSD (gray) and trauma-exposed/no-PTSD (black) participants. (B2) Average (± SEM) normalized pupil area in interest areas of neutral and threatening images in PTSD and trauma/no-PTSD participants.
Prediction of PTSD
Hierarchical logistic regression was used to evaluate the hypothesis that arousal-related pupil response would independently predict PTSD after controlling for time elapsed since trauma, cumulative violence exposure, and trait anxiety. X2 tests were used to test the significance of the model at each step and Nagelkerke R2 provided an estimate of the percent of variance explained by variable(s) at each step. In the first step, elapsed time since trauma did not significantly contribute to PTSD, X2 (1, N = 40), 3.05, p = .08, R2 = .10. In steps two and three, cumulative violence exposure and trait anxiety each significantly predicted PTSD, X2 (step two) (1, N = 40), 9.88, p < .01, ΔR2 = .20 and X2 (step three) (1, N = 40), 21.08, p < .001, ΔR2 = .43. In the final step, change in pupil (threat element) also significantly predicted PTSD, X2 (1, N = 40), 8.38, p < .01. The final model was statistically significant, X2 (3, N = 40), 39.34, p < .001, R2 = .85, and correctly classified 95% of the sample, 93.8% of individuals with PTSD and 95.8% of trauma-exposed controls.
Discussion
Participants were presented with threat and neutral images sequentially, constraining gaze behavior within each image. This enabled comparison of responses to different emotionally arousing aspects of the threat image. This is the first study to show that individuals with PTSD exhibit significantly more pupil dilation to threat-relevant stimuli than trauma-exposed controls, yet similar responses to neutral figural elements. This effect was observed independently of elapsed time since trauma, cumulative violence exposure, and trait anxiety, and was only detected in response to specific threat-relevant regions and only for those with PTSD. These findings are consistent with prior work showing heightened arousal and increased physiological responsiveness among those with PTSD (Fani et al., 2012; Kimble et al., 2010). However, they contrast with other studies, which reported that trauma-exposure alone was associated with increased pupil dilation to threat words (Felmingham et al., 2011). One interpretation for these contradictory results is that lexical stimuli have low salience and limited similarity to naturally occurring environmental stressors.
Although the mechanism underlying the heightened physiological arousal in the PTSD group was not examined here, existing research suggests that dysregulation of the brain networks that normally mediate fear is involved. Indeed, functional imaging studies in humans have revealed that brain structures regulating fear expression in animals show abnormal activity patterns in PTSD. In particular, trauma reminders were found to activate the amygdala more strongly in participants with PTSD than in controls (Shin, Rauch, & Pitman, 2006). Moreover, a prospective study reported that higher amygdala activation in response to emotional images before trauma predicted reports of higher PTSD symptom severity (Admon et al., 2009). Also, another brain region known to inhibit fear expression, the ventromedial prefrontal cortex, was found to be smaller in volume and less responsive in participants with PTSD relative to trauma-exposed controls (Bremner, Elzinga, Schmahl, & Vermetten, 2008).
The cross-sectional design limits conclusions about causal inferences regarding the role of pupil response to threat. It is unclear whether the observed pupil dilation precedes trauma-exposure or is a consequence. Prospective research will be necessary to untangle these effects. Participants were not asked how threatening or arousing they perceived each image, which would have been useful to evaluate the relationship between pupil responses and subjective report of threat or arousal. Despite these limitations, the present findings suggest that pupil responses to threat constitute a potential physiological marker of PTSD. Additionally, pupil responses could offer another method to evaluate treatment response. That is, one would expect threat-evoked pupil dilation to decrease as one recovers from PTSD. This technique has recently being applied to PTSD in clinical trials (e.g., Bar-Haim, 2011).
Acknowledgments
Portions of this paper were presented at the 29th Annual Meeting of the International Society for Traumatic Stress Studies, Philadelphia, PA. None of the authors reports competing interests. This material is based upon work supported by NIMH grants RO1 MH083710 and MH-098738 to Denis Paré.
Contributor Information
Michele Cascardi, Child Advocacy and Policy, Montclair State University, Montclair NJCenter for Molecular and Behavioral Neuroscience, Rutgers University, Newark, NJ.
Davine Armstrong, Center for Molecular and Behavioral Neuroscience, Rutgers University, Newark, NJ.
Leeyup Chung, Department of Neurobiology, Duke University, Durham, NC.
Denis Paré, Center for Molecular and Behavioral Neuroscience, Rutgers University, Newark, NJ.
References
- Admon R, Lubin G, Stern O, Rosenberg K, Sela L, Ben-Ami H, Hendler T. Human vulnerability to stress depends on amygdala’s predisposition and hippocampal plasticity. Proceedings of the National Academy of Sciences. 2009;106:14120–14125. doi: 10.1073/pnas.0903183106. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bar-Haim Y. Attention bias modification treatment for patients with post traumatic stress disorder (PTSD) 2011 http://clinicaltrials.gov/ct2/show/NCT01368302.
- Blake DD, Weathers FW, Nagy LM, Kaloupek DG, Gusman FD, Charney DS, Keane TM. The development of a clinician-administered PTSD scale. Journal of Traumatic Stress. 1995;8:75–90. doi: 10.1002/jts.2490080106. [DOI] [PubMed] [Google Scholar]
- Bremner JD, Elzinga B, Schmahl C, Vermetten E. Structural and functional plasticity of the human brain in posttraumatic stress disorder. Progressive Brain Research. 2008;167:171–186. doi: 10.1016/S0079-6123(07)67012-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Brewin CR, Rose S, Andrews B, Green J, Tata P, McEvedy C, Turner S, Foa EB. Brief screening instrument for post-traumatic stress disorder. The British Journal of Psychiatry. 2002;181:158–162. doi: 10.1017/s0007125000161896. [DOI] [PubMed] [Google Scholar]
- Carlson EB, Smith SR, Palmieri PA, Dalenberg C, Ruzek JI, Kimerling R, Spain DA. Development and validation of a brief self-report measure of trauma exposure: The Trauma History Screen. Psychological Assessment. 2011;23:463–477. doi: 10.1037/a0022294. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fani N, Tone EB, Phifer J, Norrholm SD, Bradley B, Ressler KJ, Kamkwalala A, Jovanovic T. Attention bias toward threat is associated with exaggerated fear expression and impaired extinction in PTSD. Psychological Medicine. 2012;42:533–543. doi: 10.1017/S0033291711001565. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Felmingham KL, Rennie C, Manorb B, Bryant RA. Eye tracking and physiological reactivity to threatening stimuli in posttraumatic stress disorder. Journal of Anxiety Disorders. 2011;25:668–673. doi: 10.1016/j.janxdis.2011.02.010. [DOI] [PubMed] [Google Scholar]
- Granholm E, Steinhauer SR. Pupillometric measures of cognitive and emotional processes. International Journal of Psychophysiology. 2004;52:1–6. doi: 10.1016/j.ijpsycho.2003.12.001. [DOI] [PubMed] [Google Scholar]
- Kessler RC, Berglund PA, Demler O, Jin R, Merikangas KR, Walters EE. Lifetime prevalence and age-of-onset distributions of DSM-IV disorders in the National Comorbidity Survey Replication (NCS-R) Archives of General Psychiatry. 2005;62:593–602. doi: 10.1001/archpsyc.62.6.593. 2. [DOI] [PubMed] [Google Scholar]
- Kimble MO, Fleming K, Bandy C, Kim J, Zambetti A. Eye tracking and visual attention to threatening stimuli in veterans of the Iraq war. Journal of Anxiety Disorders. 2010;24:293–299. doi: 10.1016/j.janxdis.2009.12.006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lang PJ, Bradley MM, Cuthbert BN. Technical Report A-8. University of Florida; Gainesville, FL: 2008. International affective picture system (IAPS): Affective ratings of pictures and instruction manual. [Google Scholar]
- Pineles SL, Shepherd JC, Mostoufi SM, Abramovitz SM, Yovel I. Attentional biases in PTSD: More evidence for interference. Behaviour Research and Therapy. 2009;47:1050–1057. doi: 10.1016/j.brat.2009.08.001. [DOI] [PubMed] [Google Scholar]
- Shalev AY, Freedmen S, Peri T, Brandes D, Sahar T, Orr SP, Pitman RK. Prospective study of posttraumatic stress disorder and depression following trauma. The American Journal of Psychiatry. 1998;155:630–637. doi: 10.1176/ajp.155.5.630. [DOI] [PubMed] [Google Scholar]
- Shin LM, Rauch SL, Pitman RK. Amygdala, medial prefrontal cortex, and hippocampal function in PTSD. Annals of New York Academy of Sciences. 2006;1071:67–79. doi: 10.1196/annals.1364.007. [DOI] [PubMed] [Google Scholar]
- Spielberger CD, Reheiser EC, Ritterband LM, Sydeman SJ, Unger KK. Assessment of emotional states and personality traits: Measuring psychological vital signs. In: Butcher JN, editor. Clinical Personality Assessment: Practical Approaches. NY: Oxford University Press; 1995. [Google Scholar]
- Weathers FW, Keane TM, Davidson JR. Clinician-Administered PTSD Scale: A review of the first ten years of research. (PDF) Depression and Anxiety. 2001;13:132–156. doi: 10.1002/da.1029. [DOI] [PubMed] [Google Scholar]
- Zoladz PR, Diamond DM. Current status on behavioral and biological markers of PTSD: A search for clarity in a conflicting literature. Neuroscience and Biobehavioral Reviews. 2013;37:860–895. doi: 10.1016/j.neubiorev.2013.03.024. doi.org/10.1016/j.neubiorev.2013.03.024. [DOI] [PubMed] [Google Scholar]