

Abstract
The Sjögren syndrome has been diagnosed in patients with HTLV-1 associated myelopathy and dry mouth and dry eyes are documented in HTLV-1 carriers. However the diagnosis of Sjögren syndrome in these subjects has been contested. In this cross-sectional study, we evaluated the role of immunological factors and proviral load, in sicca syndrome associated with HTLV-1 in patients without myelopathy. Subjects were recruited in the HTLV-1 Clinic, from 2009 to 2011. The proviral load and cytokine levels (IFN-γ, TNF-α, IL-5, and IL-10) were obtained from a database containing the values presented by the subjects at admission in the clinic. Of the 272 participants, 59 (21.7%) had sicca syndrome and in all of them anti-Sjögren syndrome related antigen A (SSA) and antigen B (SSB) were negatives. The production of TNF-α and IFN-γ was higher in the group with sicca syndrome (P < 0.05) than in HTLV-1 infected subjects without sicca syndrome. Our data indicates that patients with sicca syndrome associated with HTLV-1 do not have Sjögren syndrome. However the increased production of TNF-α and IFN-γ in this group of patients may contribute to the pathogenesis of sicca syndrome associated with HTLV-1.
1. Introduction
The human T lymphotropic virus type 1 (HTLV-1) infection is distributed worldwide with high prevalence in Central Africa, Central and South America, and South west of Japan [1]. Adult T cell leukemia/lymphoma (ATL), HTLV-1 associated myelopathy or tropical spastic paraparesis (HAM/TSP), and infective dermatitis are etiologically associated with HTLV-1 [2]. The HTLV-1 infects predominantly not only T cells but also B cells and myeloid cell lineage inducing cell activation and proliferation [3]. In such case it is possible that HTLV-1 infecting or activating autoreactive cells might induce the appearance of autoimmune diseases. Actually many reports in the last 20 years showed an association between rheumatoid arthritis, polymyositis, Sjögren syndrome, and systemic lupus erythematosus with HTLV-1 [4–6]. HTLV-1 infection was documented in up to 30% of patients with rheumatoid arthritis in endemic areas for this virus, and Sjögren syndrome was reported between 30 and 60% in patients who had HAM/TSP [7–9]. Sjögren syndrome is a chronic autoimmune disease of the exocrine glands that affects the salivary and lacrimal glands through a lymphocytic infiltrate, leading to xerostomia (dry mouth) and xeroftalmia (dry eye). However, more recently the association between autoimmune diseases and HTLV-1 has been contested [10, 11]. There is no doubt that a large number of HTLV-1 infected individuals have dry mouth, dry eyes, and arthropathy, but synovitis and polyarthritis are rare [12, 13]. Lymphocyte infiltration has been documented in salivary glands of HTLV-1 infected subjects indicating its participation in the pathogenesis of salivary glands destruction [14]. But occurrence of autoantibodies characteristic of Sjögren syndrome was not observed in patients with the sicca syndrome associated with HTLV-1 infection [10]. Moreover arthritis is not a common finding in patients with sicca syndrome associated with HTLV-1 [15]. Therefore the pathogenesis of sicca syndrome related to HTLV-1 is not clear and the possibility that an autoimmune disease may account for the occurrence of it has been argued.
The role of the inflammatory response and proviral load in the pathogenesis of clinical manifestations related to HTLV-1 has been well documented. Proinflammatory cytokines and chemokines are higher in supernatants of peripheral blood mononuclear cells (PBMCs) culture and in serum of HAM/TSP than HTLV-1 carriers [16, 17] and there is an association of high proviral load with HAM/TSP [18–20]. In patients with HTLV-1 associated periodontal disease, mRNA for tax was present in the periodontal tissue and there was an increased expression of IL-1β and IFN-γ and a decrease in the expression of IL-10 and regulatory T cells in this tissue [21, 22]. Furthermore, both proviral load and production of proinflammatory cytokines are higher in patients with neurogenic bladder associated with HTLV-1 but who do not fulfill the criteria for HAM/TSP, as well as in children with infective dermatitis, than in HTLV-1 carriers, which indicates that these variables are associated with diseases related to HTLV-1 [23, 24]. The aim of this study was to evaluate if there was an association between the levels of cytokines, proviral load, and anti-Sjögren syndrome related antigen A (SSA) and anti-Sjögren syndrome related antigen B (SSB) antibodies with sicca syndrome associated with HTLV-1.
2. Material and Methods
2.1. Subjects and Diagnosis Criteria
This is a cross-sectional study comparing proviral load and cytokine levels among HTLV-1 infected subjects with or without sicca syndrome. Participants of this study include 272 HTLV-1 infected subjects with age range from 18 to 60 years, of both genders, followed at the HTLV-1 Multidisciplinary Clinic of the Hospital Universitário Professor Edgard Santos in Salvador, Bahia, Brazil. Subjects admitted to the clinic are referred from blood banks or from other clinics due to a positive serology for HTLV-1 and HTLV-2, by enzyme-limited immunosorbent assay (Murex HTLV-I + II Abbot, Dartford, UK). The diagnosis of HTLV-1 is confirmed by Western blot (HTLV Blot 2.4, Genelab, Singapore). The inclusion criteria for participation in the study were the presence of a positive serology for HTLV-1 confirmed by Western blot. Exclusion criteria were presence of human immune deficiency virus (HIV) and diagnosis of HAM/TSP based on the Osame motor disability score (OMDS) ≥ 1. Moreover 27 patients were excluded due to coinfection with hepatitis B or hepatitis C virus. All subjects answered a questionnaire regarding dry mouth and dry eyes and had clinical examination. Dry mouth was determined by oral examination and the salivary flux by the Saxon test [25]. Sicca syndrome was defined by the documentation of dry mouth and abnormal Saxon test. The majority of the patients also complained of dry eyes.
2.2. Evaluation of Autoantibodies
Serum samples were screened for antinuclear antibodies by immunofluorescence and anti-SSA and anti-SSB by ELISA as previously described [26, 27].
2.3. Immunologic Studies
Cytokines were determined in supernatants of unstimulated PBMCs cultures as previously described [23]. Briefly, PBMCs were obtained from heparinized venous blood by density gradient centrifugation with Ficoll-hypaque (GE Healthcare Bio-Sciences Uppsala Sweden). The mononuclear cells were then washed in saline and after being adjusted to the concentration of 3 × 106 cells/mL were resuspended in RPMI 1640 (Life Technologies Gibco BRL, Gran Island, New York) supplemented with 10% of fetal bovine serum and antibiotics. Unstimulated cells were incubated for 72 hours at 37°C 5% CO2 and the supernatants were harvested. Determination of IFN-γ, TNF-α, IL-5, and IL-10 was performed by ELISA using reagents from BD Biosciences Pharmingen, San Jose, CA.
2.4. HTLV-1 Proviral Load
DNA was extracted from 106 PBMCs using proteinase K and salting-out method. The HTLV-1 proviral load was quantified using a real-time TaqMan PCR method as previously described using the ABI Prism 7700 Sequence detector system (Applied Biosystems) [28]. Albumin DNA was used as an endogenous reference. The normalized value of the HTLV-1 proviral load was calculated as the ratio of (HTLV-1 DNA average copy number/albumin DNA average copy number) × 2 × 106 and expressed as the number of HTLV-1 copies per 106 PBMCs.
2.5. Statistical Analysis
The comparison between the ages in the 2 groups was performed by Student's t-test. The comparison between proportions was performed by Fisher exact test. The data on cytokine levels and proviral load were expressed as median and interquartile (IQ) range and were analyzed by the Kruskal-Wallis test. The correlation between proviral load and cytokine levels was performed by the correlation of Spearmen. The GraphPad Prism 5 (San Diego, CA) was used to perform the statistical evaluation and P values < 0.05 were considered statistically significant.
3. Results
Of the 272 participants of the study, 59 (21.7%) had sicca syndrome. The age, gender, and ethnic group of HTLV-1 infected subjects with sicca syndrome and without sicca syndrome are shown in Table 1. There was no difference regarding age in the two groups (P = 0.847) and the female gender predominates in both groups without statistical significance. There were more blacks in the group with sicca syndrome (P = 0.03).
Table 1.
Demographic characteristics of patients with and without sicca syndrome associated with HTLV-1 infection.
| Without sicca syndrome | With sicca syndrome | P value | |||
|---|---|---|---|---|---|
| (n = 213; 88.3%) | (n = 59; 21.7%) | ||||
| Gender | 0.100 | ||||
| Male, n (%) | 94 | 44.1% | 19 | 32.2% | |
| Female, n (%) | 119 | 55.9% | 40 | 67.8% | |
| Age | Mean | SD | Mean | SD | 0.847 |
| 46.90 | 12.13 | 46.54 | 14.22 | ||
| Race | 0.03 | ||||
| White, n (%) | 48 | 23.2% | 13 | 23.6% | |
| Mulate, n (%) | 94 | 45.4% | 15 | 27.3% | |
| Black, n (%) | 62 | 30.0% | 27 | 49.1% | |
| Other, n (%) | 3 | 1.4% | 0 | 0.0% | |
The diagnosis of sicca syndrome was based on oral examination and a reduction in the salivary fluid by Saxon test [25]. Regarding other diseases related to HTLV-1, overactive bladder a manifestation considered as an oligosymptomatic form of HAM/TSP was documented in 11 (18.6%) of the patients with sicca syndrome and in 26 (12.2%) in the patients without sicca syndrome (P > 0.5). There was also no difference regarding polyarthralgia in the 2 groups and synovitis was detected in only 2 patients. One patient had mixed connective tissue disease and sicca syndrome and the other had a seronegative rheumatic arthritis and did not have sicca syndrome.
The spontaneous cytokines (TNF-α, IFN-γ, IL-5, and IL-10) levels in supernatants of PBMCs are shown in Figure 1. The levels of TNF-α in patients with sicca syndrome (median 803 pg/mL, IQ range 116–1,498) were higher (P < 0.009, Figure 1(a)) than that observed in patients without sicca syndrome (median 281 pg/mL, IQ range 0–946). The production of IFN-γ in patients with sicca syndrome (median 1,352 pg/mL, IQ range 717–2,477) was higher (P = 0.006, Figure 1(b)) than in the group without sicca syndrome (median 682 pg/mL, IQ range 42–1,604). No difference was observed in the median of the IL-5 levels (P = 0.88, Figure 1(c)) in the group with sicca syndrome (1 pg/mL, IQ range 0–61) and that without sicca syndrome (median 0 pg/mL, IQ range 0–62). The production of IL-10 (Figure 1(d)) did not differ between groups (P = 0.39). Cytokine levels were undetectable or were very low in supernatants of PBMCs of patients with sicca syndrome.
Figure 1.

Levels of TNF-α (a), IFN-γ (b), IL-5 (c), and IL-10 (d) produced by PBMC from HTLV-1 infected individuals with and without sicca syndrome. Cytokines data represent the values in unstimulated cultures. The levels of cytokines were measured by ELISA.
The proviral load in HTLV-1 infected subjects with and without sicca syndrome is shown in Figure 2. There was no difference between proviral load (P = 0.58) in patients with sicca syndrome (median 45,554, IQ range 13,171–126,803 copies/106 cells) and in patients without sicca syndrome (median 49,861 copies/106 cells, IQ range 2,184–128,187). There was a direct correlation between proviral load and IFN-γ and proviral load and TNF-α when values obtained in the whole sample were analyzed (Figure 3). However no correlation was observed when data from patients with sicca syndrome or without sicca syndrome were analyzed isolatedly.
Figure 2.
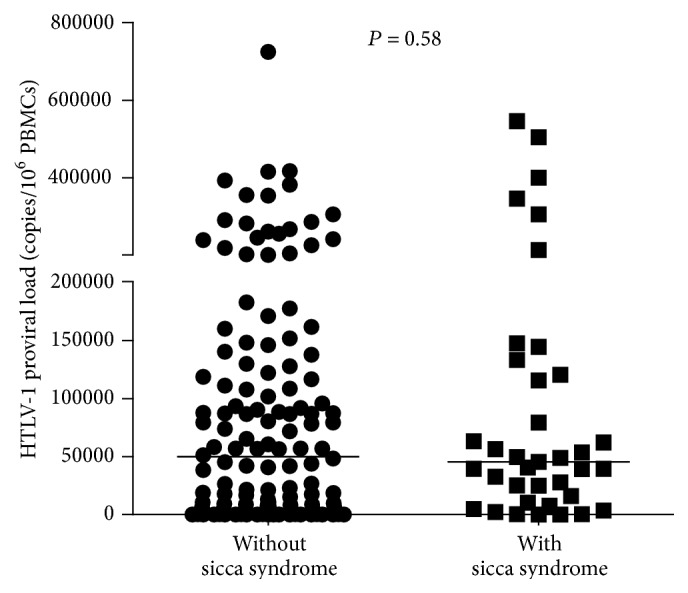
HTLV-1 proviral load of HTLV-1 infected individuals with and without sicca syndrome. Proviral load was quantified by real-time TaqMan PCR method and the normalized value of the proviral load was calculated as the ratio of (HTLV-1 DNA average copy number/albumin DNA average copy number) × 2 × 106 and expressed as the number of HTLV-1 copies per 106 PBMCs.
Figure 3.

Correlation between proviral load and cytokine levels in HTLV-1 infected subjects. There was a direct correlation between proviral load and TNF-α levels (a) and between proviral load and IFN-γ levels (b) when data from all participants of the study were analyzed.
Antinuclear antibodies and anti-SSA and anti-SSB antibodies were determined in the two groups. Anti-SSA and anti-SSB antibodies were absent in all subjects. Antinuclear antibodies were detected in 2 subjects, one in the group with and another in the group without sicca syndrome.
4. Discussion
In the present study we show that the proinflammatory cytokines IFN-γ and TNF-α were higher in HTLV-1 infected patients with sicca syndrome than in HTLV-1 infected subjects without sicca syndrome, indicating that the exacerbated proinflammatory response observed in HTLV-1 infection may play a role in the destruction of the salivary and lacrimal glands observed during this viral infection. Moreover our data indicate that autoimmune rheumatic diseases are rarely associated with HTLV-1 and that there is no evidence of Sjögren syndrome in HTLV-1 infected subjects without HAM/TSP.
The prevalence of Sjögren-like syndrome in HTLV-1 infected subjects ranges in accordance with the population studied. Initial studies showed that this association was mainly found in patients with HAM/TSP [7, 8]. However in a cross-sectional study evaluating the frequency of clinical manifestations in HTLV-1 carriers and in seronegative controls, the prevalence of dry mouth was 20.8% in carriers, while it was 11.3% in non-HTLV-1-infected subjects [13]. Poetker et al. also showed a prevalence of 22.5% of dry mouth in HTLV-1 carriers referred from blood banks recently diagnosed with HTLV-1 [12]. Herein, based on the complaint and documentation of dry mouth in the oral examination and a decrease in salivary output determined by Saxon test, the frequency of sicca syndrome in HTLV-1 infected subjects without HAM/TSP was similar to that previously found in a study performed in a HTLV-1 Clinic with small number of participants [29]. HAM/TSP and ATL are the more severe diseases related to HTLV-1, but other recognized manifestations associated with this viral infection include uveitis, chronic periodontitis, urinary manifestations of overactive bladder, sicca syndrome, and HTLV-1 associated arthropathy [2, 13, 30, 31]. It is worthwhile to emphasize that for many years HTLV-1 infection was considered a low morbidity infection as less than 5% of the infected subjects develop HAM/TSP or ATL. In this study we showed that sicca syndrome is frequent even in patients without HAM/TSP.
The documentation of a lymphocytic infiltration and the tax gene expression in the salivary gland of patients with dry mouth infected by the virus are the main evidences that salivary gland destruction in HTLV-1 infection is mediated by T cells [21, 32, 33]. Additionally HTLV-1 was expressed in salivary gland of transgenic mice that express the tax gene and presents a picture similar to Sjögren syndrome [34]. However more recently as autoantibodies related to Sjögren syndrome have not been documented in such patients, the occurrence of Sjögren syndrome associated with HTLV-1 has been argued [10, 35]. Herein patients with dry mouth and dry eyes did not present either anti-SSA or anti-SSB antibodies. This gives support to the concept that, rather than Sjögren syndrome, HTLV-1 infected subjects have a sicca syndrome due to destruction of the salivary glands.
The pathogenesis of the clinical manifestations related to HTLV-1 has been mainly studied in patients with HAM/TSP and is likely multifactorial. The neurologic disease has been associated with high proviral load [18–20] and increased levels of proinflammatory cytokines including IL-1, IL-6, TNF-α, and IFN-γ [36, 37]. In such case there is a passage of T cells from blood to the central nervous system and the tissue damage is mediated by an exaggerated and nonmodulated immunologic response [38, 39]. Giving support to the role of an exaggerated inflammatory response in the pathogenesis of manifestations due to HTLV-1, high levels of proinflammatory cytokines have been documented in other diseases associated with HTLV-1, as in patients with neurogenic bladder who do not fulfill the criteria for HAM/TSP [23], in patients with chronic periodontal disease associated with HTLV-1 [22], and in children with infective dermatitis, a disease associated with development of HAM/TSP [24].
The previous documentation that salivary glands in HTLV-1 infected subjects are infiltrated by lymphocytes and the present study showing an increased production of TNF-α and IFN-γ in patients with HTLV-1 associated with sicca syndrome indicate that viral factors and an increased inflammatory response participate in the pathogenesis of sicca syndrome associated with HTLV-1.
Acknowledgments
The authors are grateful to the staff and patients of HTLV-1 Clinic of the Professor Edgard Santos University Hospital. They also thank Cristiano Franco for secretarial assistance.
Conflict of Interests
The authors declare that they have no conflict of interests.
References
- 1.Gessain A., Cassar O. Epidemiological aspects and world distribution of HTLV-1 infection. Frontiers in Microbiology. 2012;3, article 388 doi: 10.3389/fmicb.2012.00388. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Proietti F. A., Carneiro-Proietti A. B. F., Catalan-Soares B. C., Murphy E. L. Global epidemiology of HTLV-I infection and associated diseases. Oncogene. 2005;24(39):6058–6068. doi: 10.1038/sj.onc.1208968. [DOI] [PubMed] [Google Scholar]
- 3.Yoshida M. Multiple viral strategies of HTLV-1 for dysregulation of cell growth control. Annual Review of Immunology. 2001;19:475–496. doi: 10.1146/annurev.immunol.19.1.475. [DOI] [PubMed] [Google Scholar]
- 4.Ijichi S., Matsuda T., Maruyama I., et al. Arthritis in a human T lymphotropic virus type I (HTLV-I) carrier. Annals of the Rheumatic Diseases. 1990;49(9):718–721. doi: 10.1136/ard.49.9.718. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Morgan O. S., Mora C., Rodgers-Johnson P., Char G. HTLV-1 and polymyositis in Jamaica. The Lancet. 1989;334(8673):1184–1187. doi: 10.1016/s0140-6736(89)91793-5. [DOI] [PubMed] [Google Scholar]
- 6.Pinheiro S. R., Lana-Peixoto M. A., Proietti A. B., Oréfice F., Lima-Martins M. V., Proietti F. A. HTLV-I associated uveitis, myelopathy, rheumatoid arthritis and Sjögren's syndrome. Arquivos de Neuro-Psiquiatria. 1995;53(4):777–781. doi: 10.1590/s0004-282x1995000500011. [DOI] [PubMed] [Google Scholar]
- 7.Nakamura H., Eguchi K., Nakamura T., et al. High prevalence of Sjögren's syndrome in patients with HTLV-I associated myelopathy. Annals of the Rheumatic Diseases. 1997;56(3):167–172. doi: 10.1136/ard.56.3.167. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Cartier L., Castilio J. L., Cea J. G., Villagra R. Chronic dacryosialadenitis in HTLV I associated myelopathy. Journal of Neurology Neurosurgery and Psychiatry. 1995;58(2):244–246. doi: 10.1136/jnnp.58.2.244. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Motokawa S., Hasunuma T., Tajima K., et al. High prevalence of arthropathy in HTLV-I carriers on a Japanese island. Annals of the Rheumatic Diseases. 1996;55(3):193–195. doi: 10.1136/ard.55.3.193. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Ferraz-Chaoui A. K., Atta A. M., Atta M. L. S., Galvão-Castro B., Santiago M. B. Study of autoantibodies in patients with keratoconjunctivitis sicca infected by the human T cell lymphotropic virus type 1. Rheumatology International. 2010;30(6):775–778. doi: 10.1007/s00296-009-1066-5. [DOI] [PubMed] [Google Scholar]
- 11.Bailer R. T., Lazo A., Harisdangkul V., et al. Lack of evidence for human T cell lymphotrophic virus type I or II infection in patients with systemic lupus erythematosus or rheumatoid arthritis. The Journal of Rheumatology. 1994;21(12):2217–2224. [PubMed] [Google Scholar]
- 12.Poetker S. K. W., Porto A. F., Giozza S. P., et al. Clinical manifestations in individuals with recent diagnosis of HTLV type I infection. Journal of Clinical Virology. 2011;51(1):54–58. doi: 10.1016/j.jcv.2011.02.004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Caskey M. F., Morgan D. J., Porto A. F., et al. Clinical manifestations associated with HTLV type I infection: a cross-sectional study. AIDS Research and Human Retroviruses. 2007;23(3):365–371. doi: 10.1089/aid.2006.0140. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Cartier L., Vergara C., Ramírez E. Viral Tax protein expression in salivary glands of patients infected with human t-cell lymphotropic virus type I and Sicca Syndrome. Revista Medica de Chile. 2005;133(10):1183–1190. doi: 10.4067/s0034-98872005001000007. [DOI] [PubMed] [Google Scholar]
- 15.de Carvalho M. M. N., Giozza S. P., dos Santos A. L. M. A., de Carvalho E. M., Araújo M. I. Frequency of rheumatic diseases in individuals infected with HTLV-1. Revista Brasileira de Reumatologia. 2006;46(5):315–322. doi: 10.1590/s0482-50042006000500003. [DOI] [Google Scholar]
- 16.Carvalho E. M., Bacellar O., Porto A. F., Braga S., Galvão-Castro B., Neva F. Cytokine profile and immunomodulation in asymptomatic human T-lymphotropic virus type 1-infected blood donors. Journal of Acquired Immune Deficiency Syndromes. 2001;27(1):1–6. doi: 10.1097/00126334-200105010-00001. [DOI] [PubMed] [Google Scholar]
- 17.Guerreiro J. B., Santos S. B., Morgan D. J., et al. Levels of serum chemokines discriminate clinical myelopathy associated with human T lymphotropic virus type 1 (HTLV-1)/tropical spastic paraparesis (HAM/TSP) disease from HTLV-1 carrier state. Clinical and Experimental Immunology. 2006;145(2):296–301. doi: 10.1111/j.1365-2249.2006.03150.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Nagai M., Usuku K., Matsumoto W., et al. Analysis of HTLV-I proviral load in 202 HAM/TSP patients and 243 asymptomatic HTLV-I carriers: high proviral load strongly predisposes to HAM/TSP. Journal of NeuroVirology. 1998;4(6):586–593. doi: 10.3109/13550289809114225. [DOI] [PubMed] [Google Scholar]
- 19.Grassi M. F. R., Olavarria V. N., Kruschewsky R. D. A., et al. Human T cell lymphotropic virus type 1 (HTLV-1) proviral load of HTLV-associated myelopathy/tropical spastic paraparesis (HAM/TSP) patients according to new diagnostic criteria of HAM/TSP. Journal of Medical Virology. 2011;83(7):1269–1274. doi: 10.1002/jmv.22087. [DOI] [PubMed] [Google Scholar]
- 20.Olindo S., Lézin A., Cabre P., et al. HTLV-1 proviral load in peripheral blood mononuclear cells quantified in 100 HAM/TSP patients: a marker of disease progression. Journal of the Neurological Sciences. 2005;237(1-2):53–59. doi: 10.1016/j.jns.2005.05.010. [DOI] [PubMed] [Google Scholar]
- 21.Mariette X., Agbalika F., Zucker-Franklin D., et al. Detection of the tax gene of HTLV-I in labial salivary glands from patients with Sjögren's syndrome and other diseases of the oral cavity. Clinical and Experimental Rheumatology. 2000;18(3):341–347. [PubMed] [Google Scholar]
- 22.Garlet G. P., Giozza S. P., Silveira E. M., et al. Association of human T lymphotropic virus 1 amplification of periodontitis severity with altered cytokine expression in response to a standard periodontopathogen infection. Clinical Infectious Diseases. 2010;50(3):e11–e18. doi: 10.1086/649871. [DOI] [PubMed] [Google Scholar]
- 23.Santos S. B., Oliveira P., Luna T., et al. Immunological and viral features in patients with overactive bladder associated with human T-cell lymphotropic virus type 1 infection. Journal of Medical Virology. 2012;84(11):1809–1817. doi: 10.1002/jmv.23341. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Nascimento M. C. F., Primo J., Bittencourt A., et al. Infective dermatitis has similar immunological features to human T lymphotropic virus-type 1-associated myelopathy/tropical spastic paraparesis. Clinical and Experimental Immunology. 2009;156(3):455–462. doi: 10.1111/j.1365-2249.2008.03869.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Kohler P. F., Winter M. E. A quantitative test for xerostomia. The Saxon test, an oral equivalent of the Schirmer test. Arthritis and Rheumatism. 1985;28(10):1128–1132. doi: 10.1002/art.1780281008. [DOI] [PubMed] [Google Scholar]
- 26.Maddison P. J., Skinner R. P., Vlachoyiannopoulos P., Brennand D. M., Hough D. Antibodies to nRNP, Sm, Ro(SSA) and La(SSB) detected by ELISA: their specificity and inter-relations in connective tissue disease sera. Clinical and Experimental Immunology. 1985;62(2):337–345. [PMC free article] [PubMed] [Google Scholar]
- 27.Blomberg S., Ronnblom L., Wallgren A. C., Nilsson B., Karlsson-Parra A. Anti-SSA/Ro antibody determination by enzyme-linked immunosorbent assay as a supplement to standard immunofluorescence in antinuclear antibody screening. Scandinavian Journal of Immunology. 2000;51(6):612–617. doi: 10.1046/j.1365-3083.2000.00735.x. [DOI] [PubMed] [Google Scholar]
- 28.Dehée A., Césaire R., Désiré N., et al. Quantitation of HTLV-I proviral load by a TaqMan real-time PCR assay. Journal of Virological Methods. 2002;102(1-2):37–51. doi: 10.1016/s0166-0934(01)00445-1. [DOI] [PubMed] [Google Scholar]
- 29.Vernant J.-C., Buisson G., Magdeleine J., et al. T-lymphocyte alveolitis, tropical spastic paresis, and Sjögren syndrome. The Lancet. 1988;331(8578):p. 177. doi: 10.1016/s0140-6736(88)92744-4. [DOI] [PubMed] [Google Scholar]
- 30.Giozza S. P., Santos S. B., Martinelli M., Porto M. A., Muniz A. L., Carvalho E. M. Salivary and lacrymal gland disorders and HTLV-1 infection. Revue de Stomatologie et de Chirurgie Maxillo-Faciale. 2008;109(3):153–157. doi: 10.1016/j.stomax.2007.08.008. [DOI] [PubMed] [Google Scholar]
- 31.Murphy E. L., Wang B., Sacher R. A., et al. Respiratory and urinary tract infections, arthritis, and asthma associated with HTLV-I and HTLV-II infection. Emerging Infectious Diseases. 2004;10(1):109–116. doi: 10.3201/eid1001.020714. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Mariette X., Agbalika F., Daniel M.-T., et al. Detection of human T lymphotropic virus type I tax gene in salivary gland epithelium from two patients with Sjögren's syndrome. Arthritis and Rheumatism. 1993;36(10):1423–1428. doi: 10.1002/art.1780361015. [DOI] [PubMed] [Google Scholar]
- 33.Sumida T., Yonaha F., Maeda T., et al. Expression of sequences homologous to HTLV-I tax gene in the labial salivary glands of Japanese patients with Sjögren's syndrome. Arthritis and Rheumatism. 1994;37(4):545–550. doi: 10.1002/art.1780370415. [DOI] [PubMed] [Google Scholar]
- 34.Green J. E., Hinrichs S. H., Vogel J., Jay G. Exocrinopathy resembling Sjogren's syndrome in HTLV-1 tax transgenic mice. Nature. 1989;341(6237):72–74. doi: 10.1038/341072a0. [DOI] [PubMed] [Google Scholar]
- 35.Carvalho M. M., Novaes A. E., Carvalho E. M., Araújo M. I. Doenças reumáticas auto-imunes em indivíduos infectados pelo HTLV-1. Revista Brasileira de Reumatologia. 2006;46(5):334–339. doi: 10.1590/s0482-50042006000500006. [DOI] [Google Scholar]
- 36.Nishiura Y., Nakamura T., Ichinose K., et al. Increased production of inflammatory cytokines in cultured CD4+ cells from patients with HTLV-I-associated myelopathy. The Tohoku Journal of Experimental Medicine. 1996;179(4):227–233. doi: 10.1620/tjem.179.227. [DOI] [PubMed] [Google Scholar]
- 37.Santos S. B., Porto A. F., Muniz A. L., et al. Exacerbated inflammatory cellular immune response characteristics of HAM/TSP is observed in a large proportion of HTLV-I asymptomatic carriers. BMC Infectious Diseases. 2004;4, article 7 doi: 10.1186/1471-2334-4-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Kuroda Y., Matsui M., Takashima H., Kurohara K. Granulocyte-macrophage colony-stimulating factor and interleukin-1 increase in cerebrospinal fluid, but not in serum, of HTLV-I-associated myelopathy. Journal of Neuroimmunology. 1993;45(1-2):133–136. doi: 10.1016/0165-5728(93)90173-v. [DOI] [PubMed] [Google Scholar]
- 39.Nishimoto N., Yoshizaki K., Eiraku N., et al. Elevated levels of interleukin-6 in serum and cerebrospinal fluid of HTLV-I-associated myelopathy/tropical spastic paraparesis. Journal of the Neurological Sciences. 1990;97(2-3):183–193. doi: 10.1016/0022-510X(90)90217-B. [DOI] [PubMed] [Google Scholar]