

Abstract
An otherwise fit and well 27-year-old man presented with acute onset unexplained bilateral shoulder pain, and was found to have bilateral shoulder fractures and dislocations on imaging. Although features were atypical, a nocturnal seizure causing the bilateral shoulder fractures was suspected and EEG showed features compatible with epilepsy.
Background
This case highlights the importance of considering imaging investigations in young patients with severe shoulder pain, particularly if it was of sudden onset with no obvious precipitating factors.
The second important point is that a first seizure can present as bilateral shoulder pain. This is atypical and clinicians should consider this differential in patients with sudden onset severe bilateral shoulder pain, especially if no triggering factors were identified.
Case presentation
A 27-year-old man who was previously fit and well presented to the rheumatology clinic, with severe bilateral shoulder pain that began on waking-up in the morning 7 months prior. Both shoulders had minimal global range of movement and the intense pain kept him up at night. There was no history of trauma. He had been treated for muscle spasm in accident and emergency and for frozen shoulder by his general practitioner. The bilateral shoulder pain had not resolved since onset and therefore he was referred to the rheumatology department.
Investigations
Rheumatology arranged bilateral MRI and X-ray, which showed chronic bilateral anteroinferior dislocations of both shoulders and fractures through the greater tuberosity (figures 1 and 2). The fractures were thought to have occurred at the same time.
Figure 1.
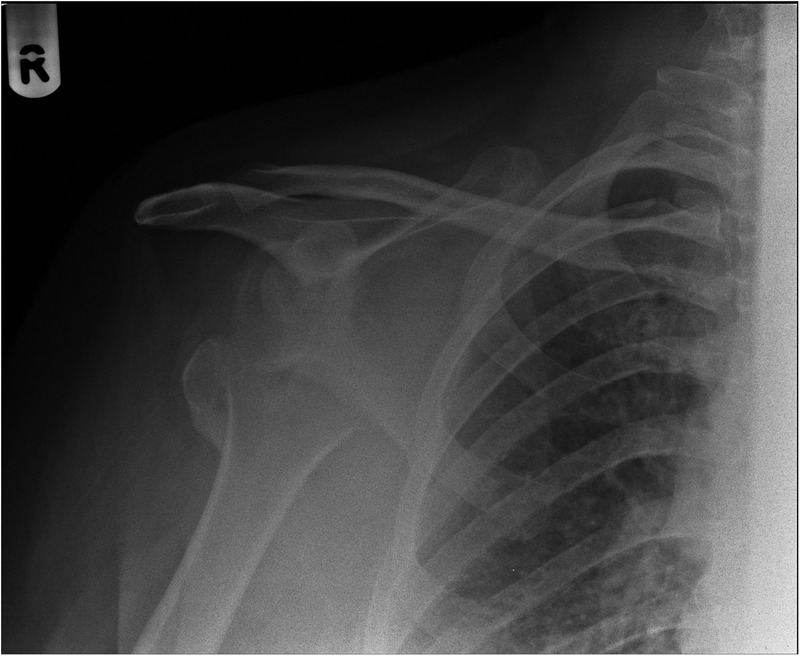
Right shoulder radiograph; chronic anteroinferior dislocation and fracture through the greater tuberosity.
Figure 2.
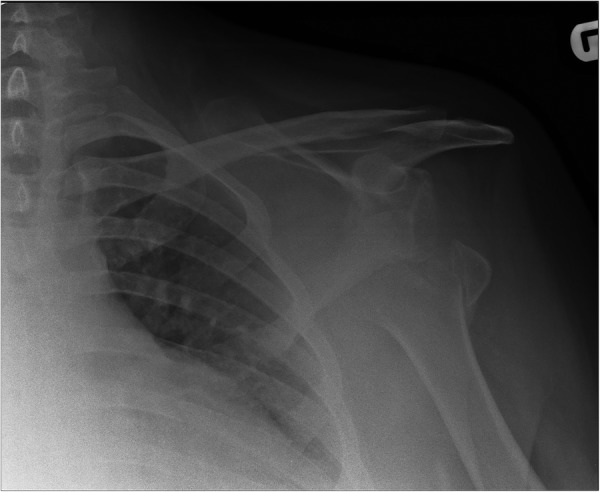
Left shoulder radiograph; chronic anteroinferior dislocation and fracture through the greater tuberosity.
A nocturnal seizure causing bilateral shoulder fractures was suspected and the patient was referred to neurology. Further questioning revealed that he had woken up that morning 7 months earlier with significant amnesia and in a confused state. He had not consumed alcohol the night before and there was no incontinence. He had slept alone. MRI of the brain was normal but EEG showed frontal sharp waves suggestive of a tendency to epilepsy.
Treatment
The neurologists started him on levetiracetam for his epilepsy, while the orthopaedic surgeons performed complex open shoulder reconstruction (bilateral reduction of anterior chronic dislocated shoulders plus greater tuberosity fixation and coracoid transfer), required due to the delay in diagnosis.
Outcome and follow-up
Follow-up shoulder radiographs 11 months and 6 months after the right and left shoulder reconstruction surgeries, respectively, showed satisfactory reuniting of bones (figures 3 and 4).
Figure 3.
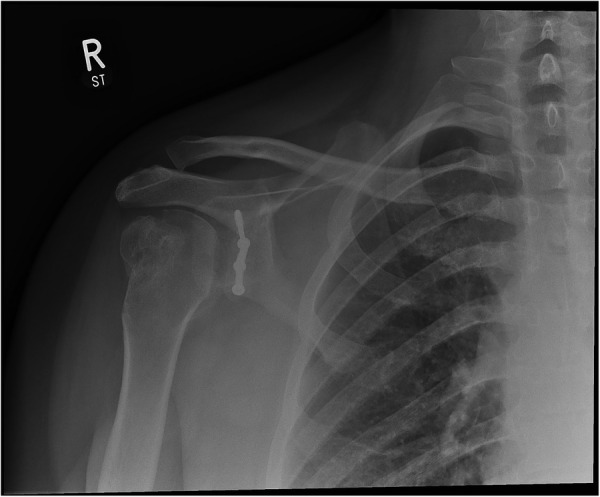
Right shoulder postreconstruction.
Figure 4.
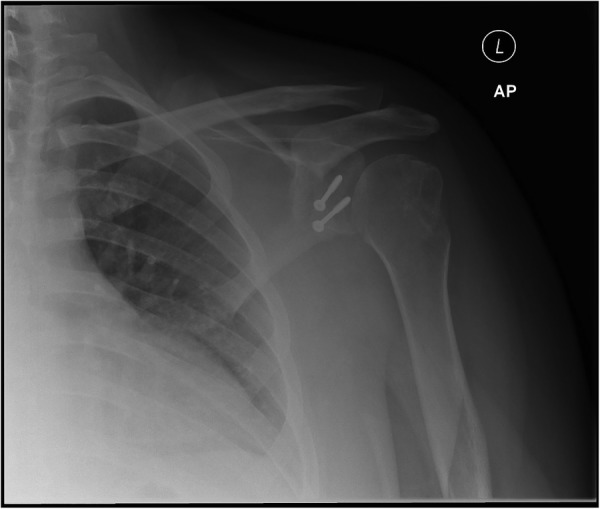
Left shoulder postreconstruction.
The patient was advised to maintain his levetiracetam use for the long term.
Discussion
Bilateral shoulder fractures-dislocations are rare. Most cases are either bilateral shoulder fractures or bilateral dislocations. Trauma may be due to tonic-clonic seizure, electrical shock1 or fall.2 The common aetiologies of bilateral anterior dislocation-fracture are sudden muscle contractions or violent bilateral traction, or deceleration forces.2
Fracture of the humeral greater tuberosity occurs in 15% of anterior dislocation cases.3 CT scan can identify bony fragment displacement and MRI can evaluate rotator cuff tears, which is helpful to identify surgical candidates.4
Surgical treatment should be tailored to the type of injury, the delay between the trauma and treatment, the patients’ age and desired functional ability.5 Some experts propose treatment within 2 years of injury while others suggest it to be ideal within 6-months in order to obtain excellent or good results. Delay in treatment leads to muscle atrophy, tissue scarring and capsulitis, leading to difficulty in restoring anatomy and function.5
In summary, four types of intervention are proposed, depending on the severity of injury.5
Reducible dislocation with non-displaced fracture and minimal articular surface involvement and viable humeral head; conservative treatment.
Non-reducible dislocation or displaced fracture with minimal articular surface involvement and a viable humeral head; open reduction, internal fixation.
Articular surface involvement or non-viable humeral head; hemiarthroplasty.
Humeral and glenoid articular surface involvement; total shoulder arthroplasty.
Our patient required an open reduction with internal fixation of the greater tuberosity and has regained almost full range of movement of his shoulders.
An important point highlighted in our case is that the seizure was neither witnessed nor accompanied by typical features of incontinence, but was confirmed on subsequent neurology investigations. Nocturnal seizure should be suspected in patients presenting with an unexplained confusional state.
Patients presenting with unexplained persistent bilateral shoulder pain should have shoulder imaging performed and be referred to a specialist for further investigations.
Learning points.
Shoulder imaging should be performed in patients with sudden onset severe shoulder pain, especially if no obvious precipitating factor is identified.
There should be no delay in the referral of persistent unexplained bilateral shoulder pain.
A first epileptic seizure may present as bilateral shoulder pain; a detailed history should be obtained.
Consider nocturnal seizure as a cause of unexplained confusional state and amnesia even if in the absence of other stigmata of seizures.
Footnotes
Contributors: IS drafted the manuscript. AF approved the final version.
Competing interests: None declared.
Patient consent: Obtained.
Provenance and peer review: Not commissioned; externally peer reviewed.
References
- 1.Salem MI. Bilateral anterior fracture-dislocation of the shoulder joints due to severe electric shock. Injury 1983;14:361–3. 10.1016/0020-1383(83)90258-9 [DOI] [PubMed] [Google Scholar]
- 2.Dinopoulos HT, Giannoudis PV, Smith RM et al. Bilateral anterior shoulder fracture-dislocation. A case report and a review of the literature. Int Orthop 1999;23:128–30. 10.1007/s002640050327 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Ferkel RD, Hedley AK, Eckardt JJ. Anterior fracture dislocations of the shoulder: pitfalls in treatment. J Trauma 1984;24:363–7. 10.1097/00005373-198404000-00016 [DOI] [PubMed] [Google Scholar]
- 4.Dlimi F, Mahfoud M, Lahlou A et al. Bilateral anterior shoulder dislocation with bilateral fractures of the greater tuberosity: a case report. J Clin Orthop Trauma 2012;3:122–5. 10.1016/j.jcot.2011.04.001 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Martens C, Hessels G. Bilateral posterior four-part fracture-dislocation of the shoulder. Acta Orthop Belg 1995;61:249–54. [PubMed] [Google Scholar]