

Abstract
Background:
Janani Shishu Suraksha Karyakram (JSSK) was initiated in 2011 to reduce the out of pocket expenditure for pregnant women. We estimated the proportion of mothers who received JSSK benefits and out of pocket expenditure (OOP) if any in Sirmaur, Himachal Pradesh.
Materials and Methods:
We did cross sectional survey in public sector facilities among 156 consecutive mothers using structured questionnaire. We computed the proportion of mother who received the benefits and the median OOP expenditure.
Results:
Among 156 mothers surveyed, 93 (60%) received the full benefits during hospital stay and 29 (19%) received full transport benefits. Free diagnostics and drugs were given to 149 (96%) and 134 (86%) respectively. Overall, 63 (40%) had median OOP Rs 210 during hospitalization and 127 (81%) had median OOP of Rs 420 during transport.
Conclusion:
JSSK benefitted the mothers utilizing the public sector facilities however drugs, consumables and transport contributed to the OOP expenditure.
Keywords: Delivery, Himachal Pradesh, India, JSSK, out of pocket expenditure
Introduction
Globally there were 535, 900 maternal deaths in 2005 of which 45% were in the Asian countries. India is one of the five countries that accounted for half of the maternal deaths worldwide. India had MMR of 450 per 100,000 live births in 2005.(1) MMR in India declined from 523 in 1990 to 254 per 100,000 live births in 2008.(2) However the decline was not adequate to achieve the MDG goals. One of the key reasons for poor utilization of maternal health care services was the financial burden on the families.(3) A national survey analysis indicated that 80% of the households reported out of pocket expenditure for maternal health care services.(4) Out of pocket expenditure on institutional delivery in India was 39 USD in public sector facilities in 2004-08.(5)
Government of India initiated several programs to improve the institutional deliveries with the goal of reducing maternal mortality. Janani Suraksha Yojana (JSY) is a conditional cash transfer scheme under National Rural Health Mission. The JSY led to 8% (29.8% to 37.8%) increase in the institutional deliveries between 2004 to 2008.(6) A national level survey analysis indicated 42% JSY beneficiaries among the public sector deliveries.(7) Government of India launched Janani Shishu Suraksha Karyakram (JSSK) scheme in June 2011 to further enhance the institutional delivery and reduce the out of pocket expenses for families of all pregnant women in the public sector facilities. JSSK provides free and cashless delivery in the public sector institutions.(8)
Institutional deliveries in the Himachal Pradesh increased from 63.4% in 2010-11 to 75.5% in 2012-2013 after implementing JSSK.(9) Sirmaur district had third lowest proportion of institutional deliveries (57%) in 2011.(9) The utilisation for various components of services under JSSK scheme in Himachal Pradesh was variable ranging from 40-70% for various components.(10) However, there was lack of data regarding utilization for each benefit and the out of pocket expenditure among beneficiaries. Therefore we estimated the proportion of mothers who received various components of JSSK benefits and out of pocket expenditure among beneficiaries in the secondary level health facilities of Sirmaur district.
Materials and Methods
Study design and study population
We conducted cross sectional survey among women who delivered in the public sector facilities where JSSK was implemented in district Sirmaur, Himachal Pradesh. JSSK was implemented in three Community Health Centres, three civil hospitals, and one district hospital.
Sample size and sampling procedure
All consecutive deliveries in seven public sector facilities during January-March, 2013 were included till the sample size was reached. We obtained sample size of 156 mothers assuming 40% utilization of JSSK by mothers (based on the Himachal Pradesh state report), 8% absolute precision, 95% confidence and 10% non response.
Operational definitions
JSSK benefits to pregnant women
The services for the following components should be offered free to the pregnant mothers. The components included normal delivery, ceasarean section, drugs and consumables, diagnostics, diet, blood transfusion, exemption from user charges, transport from home to health institutions, transport between facilities in case of referral and free drop back from institutions to home after 48 hrs stay.
Full benefit of JSSK during hospitalization
We defined full benefit if mother received all the benefits mentioned above during hospitalization except transport.
Full transport benefit
If the mother availed government ambulance both ways or they were reimbursed at the prescribed per kilometre rate for both ways or government ambulance one way and reimbursement for the other trip.
Data collection and analysis
We used structured questionnaires to collect data from mothers regarding socio demographic status, antenatal history, details of the delivery, benefits received for different components, cost incurred if any and reasons for not receiving benefits. Data was collected from mothers after delivery before the discharge from health facility. Analysis was done using Epi-info 3.5.3 version. We estimated the proportion for various benefits received by mothers and median cost incurred for each component.
Human subject protection
We obtained written informed consent from the participants. Confidentiality of the participants was maintained. We obtained approval from the Institutional ethics committee and Himachal Pradesh Health officials.
Results
Characteristics of mothers
Among 156 mothers surveyed, mean age of the mothers was 24 years but 62% were below 25 years of age. Mean age at marriage was 21 years. Median family income was 5000 INR (80 USD) with 22.4% of families below poverty line. Majority of the mothers were literate (93%). Fifty percent of the mothers were primigravida mothers. Only 16% came to the facility due to obstetric emergency and the remaining came by self choice. Only 44 (28%) reached by government ambulance and 8% were referred from other health facilities. Mean duration of stay in the hospital for normal delivery and for caesarean sections was 34 hours and 100 hours respectively. Only 23% used government ambulance for transport from facility to home.
JSSK services
Overall 93 (60%) mothers received all JSSK benefits during hospitalization and 29 (19%) received full benefit for transport. Only 23 (15%) mothers were fully benefitted during stay and transport. The proportion of mothers who received diagnostics, drugs and consumables were 96%, 86% and 64% respectively [Figure 1].
Figure 1.
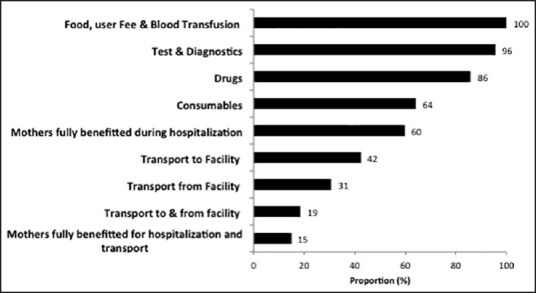
Proportion of mothers who received the benefits under JSSK program, Sirmaur, Himachal Pradesh, India, 2013. (N = 156)
Only nine mothers consulted hospital in the post partum period for minor ailments related to delivery however none were hospitalized. All nine mothers incurred expenditure in the range of Rs 50-100 for the outpatient visits in nearby government or private facility. These facilities were not providing free services under JSSK. Only six newborns aged 15-30 days were hospitalized and all received free services during the hospitalization and transport benefits.
Out-of-pocket (OOPs) expenditure
The proportion of mothers who had out of pocket (OOP) expenditure during the ANC checkups (not included in JSSK) was 68% and the median expenditure was 550 INR (8.8 USD).
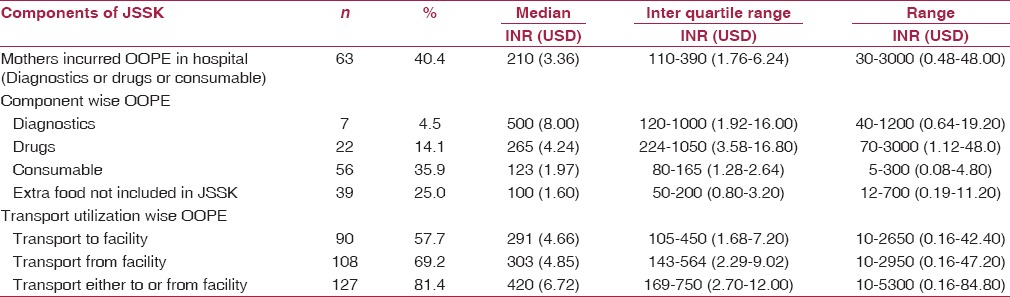
Overall 63 (40%) mothers had OOP expenditure for one or more components during hospitalization. The OOP expenditure for diagnostics, drugs and consumables was 500 INR (8 USD), 265 INR (4.24 USD) and 123 INR (1.97 USD) respectively during hospitalization. Apart from hospitalization, transport expenditure was very high [Table 1].
Table 1.
Median out of pocket expenditure for various components covered under JSSK and proportion of mothers who incurred the expenditure in Sirmaur, Himachal Pradesh, India, 2013 (N = 156)
Discussion
Our study described the level of utilization of various benefits under JSSK among mothers. Though mothers received many of the benefits, there was OOPE on many components. All mothers received user fee exemption; blood transfusion and diet however majority of the mothers did incur out of pocket expenditure on consumable, drugs, diagnostics and transport.
Overall median OOP expenditure in our study was much lower than the OOP expenditure (Rs 2400) reported for Himachal Pradesh during 2004-08 in DLHS-3 survey.(7) The components contributing to OOP expenditure were consumables and drugs as there was only one cashless private provider in most of the facilities. The arrangement for cashless procurement should be made with multiple private providers in the vicinity of hospitals for beneficiaries. Himachal Pradesh has high public sector utilization for deliveries and similar scenario was also observed in other Indian states such as Tamil Nadu. However, Himachal Pradesh had higher OOP expenditure in the public sector facilities as compared to Tamil Nadu.(5) One of the reasons for low expenditure in Tamil Nadu might be central procurement agency for drugs and consumables and therefore better availability in the health facilities.(11) There is need for better procurement policies in the public sector to ensure access to free drugs and consumables at the facility level.
In our study, majority of the mothers got the transport benefits as defined by JSSK guidelines however OOP incurred among those who were fully benefited was mostly due to extra cost of transport over and above the eligibility for reimbursement. Median expenditure on transport to the facility in the study population was more than double (Rs 150) of the expenditure reported in the DLHS-3 for India.(7) This might be due to the hilly terrain and poor accessibility of the health facilities. Provision of accessible and reliable free transport especially in the hilly and difficult to reach villages might further help reduce the OOP.
Our study was cross-sectional in nature and there was lack of baseline data regarding out of pocket expenditure in the Sirmaur district in 2011 before JSSK program. Therefore we cannot comment regarding changes in the OOP after the introduction of JSSK specifically for the district.
JSSK benefitted the mothers utilizing the public sector facilities however consumables, drugs and transport continued to contribute to the OOP expenditure. There is need for cashless transport facility and better availabiliy of drugs and consumables to further reduce the OOP expenditure on deliveries.
Footnotes
Source of Support: National Institute of Epidemiology, Chennai
Conflicts of interest: None declared.
References
- 1.Hill K, Thomas K, AbouZahr C, Walker N, Say L, Inoue M, et al. Maternal Mortality Working Group. Estimates of maternal mortality worldwide between 1990 and 2005: An assessment of available data. Lancet. 2007;370:1311–9. doi: 10.1016/S0140-6736(07)61572-4. [DOI] [PubMed] [Google Scholar]
- 2.Hogan MC, Foreman KJ, Naghavi M, Ahn SY, Wang M, Makela SM, et al. Maternal mortality for 181 countries, 1980-2008: A systematic analysis of progress towards Millennium Development Goal 5. Lancet. 2010;375:1609–23. doi: 10.1016/S0140-6736(10)60518-1. [DOI] [PubMed] [Google Scholar]
- 3.Mumbai: International Institute for Population Sciences and Macro International; 2007. International Institute for Population Sciences and Macro International. National Family Health Survey (NFHS-3), 2005-06. India; p. 210. [Google Scholar]
- 4.Leone T, James K, Padmadas SS. The burden of maternal health care expenditure in India: Multilevel analysis of national data. Matern Child Health J. 2013;17:1622–30. doi: 10.1007/s10995-012-1174-9. [DOI] [PubMed] [Google Scholar]
- 5.Mohanty SK, Srivastava A. Out-of-pocket expenditure on institutional delivery in India. Health Policy Plan. 2013;28:247–62. doi: 10.1093/heapol/czs057. [DOI] [PubMed] [Google Scholar]
- 6.Paul VK, Sachdev HS, Mavalankar D, Ramachandran P, Sankar MJ, Bhandari N, et al. Reproductive health, and child health and nutrition in India: Meeting the challenge. Lancet. 2011;377:332–49. doi: 10.1016/S0140-6736(10)61492-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Modugu HR, Kumar M, Kumar A, Millett C. State and socio-demographic group variation in out-of-pocket expenditure, borrowings and Janani Suraksha Yojana (JSY) programme use for birth deliveries in India. BMC Public Health. 2012;12:1048. doi: 10.1186/1471-2458-12-1048. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Center for Health Informatics N. Janani Sishu Suraksha Karyakram (JSSK), National Health Portal New Delhi. 2013. [Last accessed on 2014 May 1]. Available from: http://www.nhp.gov.in/jssk .
- 9.Shimla: Health and Family Welfare Department; 2011. Office of Director Health Services HP. Reports from state Statistical Cell. [Google Scholar]
- 10.Bhushan H. Janani Shishu Suraksha Karyakram; Secretaries review meeting; September 11, 2012 2011. Available from: http://www.wbhealth.gov.in/nrhmwb/Revised JSSK PRESENTATION FOR 11092012.ppt .
- 11.Tamil Nadu Medical Services Corporation limited. Tamil Nadu Medical Services Corporation Limited Services Chennai. 2013. [Last accessed on 2013 Mar 25]. Available from: http://www.tnmsc.com/tnmsc/new/html/services.php .