

Abstract
Endo-retractors are convenient devices for exposure and traction during minimally invasive surgery and are widely used in laparoscopic cholecystectomy (LC). Complications associated with the use of this device are rare. We present a patient with symptomatic gallstones who underwent LC and developed a diaphragmatic laceration as a result of the inappropriate use of an endo retractor. Although the incidence of complications with endo retractors is low, this report indicates the potential risk of diaphragmatic injury while using the retractors for exposure and traction during minimally invasive surgery.
Keywords: Complication, diaphragmatic injury, endo-retractor, laparoscopic cholecystectomy
INTRODUCTION
Laparoscopic cholecystectomy (LC) has become the first-line procedure for most patients with gallstones. Endo-retractors are convenient devices for exposure and traction during minimally invasive surgery and are widely used in LC. However, complications associated with using endo-retractors had not been reported. Herein we present a patient with diaphragmatic injury caused by an endo-retractor during LC. Careful use of this type of retractor should be emphasised.
CASE REPORT
A 41-year-old woman without past medical history presented to surgery clinic for evaluation of symptomatic gallstone disease. An elective laparoscopic cholecystectomy (LC) was scheduled. The operation was performed under general anaesthesia, with the patient placed in the reverse Trendelenburg position. Mini-laparotomy was performed with an open technique through one intra-umbilical 10-mm-long skin incision that served as the camera port. After pneumoperitoneum had been established, two more 5-mm skin incisions were made in the upper abdomen to function as working ports.
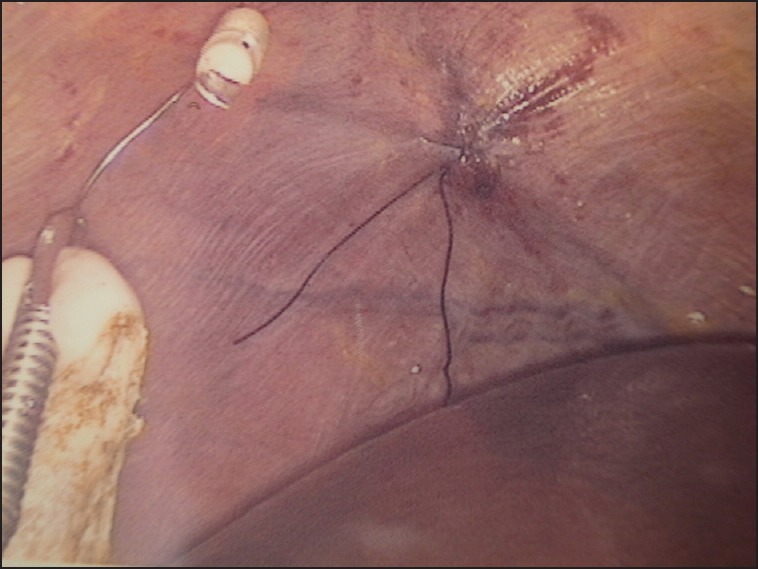
We applied an endo-retractor (EndoGrab™ Port-Free Endocavity. Virtual Ports, Ltd. 20 Alon Hatavor Street, Caesarea 3088900, Israel) for better exposure without making an additional working port during the dissection of Calot's triangle. The endo-retractor was used to retract the gallbladder cephalad by grasping the fundus and anchoring anterior to the right lobe of the liver. However, while using the anchoring clip to anchor to the peritoneum, a full-thickness laceration about 1 cm in length in the right hemi-diaphragm was noted. No pulmonary injury was observed. Intraoperative laparoscopic repair of the right hemi-diaphragm was performed with silk suture without difficulty [Figure 1a and b]. The cystic duct and artery were ligated and divided, followed by dissection of the gallbladder from the liver bed. Finally, the gallbladder was removed through the umbilical port site. After the operation, a chest X-ray showed no signs of pneumothorax or hemothorax. The total operation time was 83 min, and blood loss was minimal. The patient recovered uneventfully and was discharged home on the day after the operation. She reported no other complications at the outpatient clinic follow-up visit 1-week later.
Figure 1a.

Intraoperative laparoscopic repair of the right hemi-diaphragm was performed with silk suture
Figure 1b.
The right hemi-diaphragm, after laparoscopic repair
DISCUSSION
Laparoscopic cholecystectomy has the advantages of limited post-operative pain and shorter hospitalisation compared with open cholecystectomy and has become the first-line procedure for most patients with gallstones. In a large series, commonly reported complications during LC were bile duct injury (0.59%), vascular injury (0.25%), and bowel injury (0.14%).[1] Diaphragmatic injury seems an extremely rare complication in LC; in a literature review of the operation, only a few case reports described diaphragmatic injury as a complication of the operation.[2,3] In most of these reports, diaphragmatic injury occurred incidentally with the use of rigid instruments. To our knowledge, diaphragmatic injury with the EndoGrab™ Port-Free Endocavity Retractor device during LC has not been previously reported.
In the era of minimally invasive surgery, LC can be performed through a single port or several ports, as needed, or even through the natural orifice transluminal endoscopic surgery. Many factors, including the patient's condition, availability of surgical instruments, and the surgeon's technical skill and training influence the exact method of LC. The EndoGrab™ Port-Free Endocavity Retractor device is useful because it allows for better exposure and visualisation of the operative site in laparoscopic surgery, which helps minimize the number of working ports needed. An endo-retractor usually contains an “organ clip” and an “anchoring clip”. The organ to be retracted is attached with the organ clip and then to the internal operating cavity wall with the anchoring clip. In our case, the diaphragmatic laceration occurred immediately when the surgeon anchored the endo-retractor to the diaphragm. Two reasons may be responsible for this complication. First, we may have attached the anchoring clip to the too much diaphragmatic tissue. Second, the site we anchored may have been too centrally located on the diaphragm. Since the muscle near the central tendon of the diaphragm is relatively thin, the grasping of too much tissue by the anchoring clip may have resulted in a laceration of the diaphragm. Consequently, to minimize the risk of the diaphragmatic laceration, we recommend attaching the anchoring clip to a more peripheral area of the diaphragm and attaching the clip only to the peritoneum lining of the diaphragm.
This case illustrates that although rare, diaphragmatic injury caused by inappropriate use of an endo-retractor may be a complication in LC, and possibly in other minimally invasive abdominal operations. The incidence of this complication may be underestimated, and careful use of this type of retractor should be emphasised. Further improvements in technique and instruments may be required in order to make minimally invasive surgery safer.
Footnotes
Source of Support: Nil
Conflicts of Interest: None declared.
REFERENCES
- 1.Deziel DJ, Millikan KW, Economou SG, Doolas A, Ko ST, Airan MC. Complications of laparoscopic cholecystectomy: A national survey of 4,292 hospitals and an analysis of 77,604 cases. Am J Surg. 1993;165:9–14. doi: 10.1016/s0002-9610(05)80397-6. [DOI] [PubMed] [Google Scholar]
- 2.Seiler C, Glättli A, Metzger A, Czerniak A. Injury to the diaphragm and its repair during laparoscopic cholecystectomy. Surg Endosc. 1995;9:193–4. doi: 10.1007/BF00191964. [DOI] [PubMed] [Google Scholar]
- 3.Hosogi H, Lingohr P, Galetin T, Sakai Y, Saad S. Right diaphragm injury: An unusual complication in single-port laparoscopic cholecystectomy. Surg Laparosc Endosc Percutan Tech. 2011;21:e143–4. doi: 10.1097/SLE.0b013e31821a9dbf. [DOI] [PubMed] [Google Scholar]