

Abstract
With the advances in magnetic resonance imaging, previously unrecognized small brain lesions, which are mostly asymptomatic, have been increasingly detected. Diffusion-weighted imaging can identify small ischemic strokes, while gradient echo T2* imaging and susceptibility-weighted imaging can reveal tiny hemorrhagic strokes (microbleeds). In this article, we review silent brain lesions appearing soon after acute stroke events, including silent new ischemic lesions and microbleeds appearing 1) after acute ischemic stroke and 2) after acute intracerebral hemorrhage. Moreover, we briefly discuss the clinical implications of these silent new brain lesions.
Keywords: Silent brain lesions, New ischemic lesions, New microbleeds
Introduction
Although most strokes are considered a single event, subsequent strokes may follow shortly after an acute stressful event such as ischemic or hemorrhagic stroke. Remarkably, in many cases, such subsequent strokes after acute index events are asymptomatic. These silent new brain lesions can be demonstrated by diffusion-weighted imaging (DWI) and gradient echo T2* imaging (GRE) or susceptibility-weighted imaging. Although the name suggests clinically silent behaviors, their clinical importance remains controversial. While some researchers consider only clinically obvious stroke as clinically important [1], others have associated silent new brain lesions with future strokes or possible harmful effects on the brain function.
In this article, we aim to review silent new brain lesions in terms of their incidence, associated factors, mechanisms, and clinical implications. As both ischemic and hemorrhagic (microbleeds) strokes can appear as silent new brain lesions, this narrative review categorized silent new lesions into two groups: silent new ischemic lesions (SNILs) and silent new microbleeds (SNMs).
SNILs
SNILs after acute ischemic stroke
As mortality is increased in stroke patients with early recurrence [2,3], efforts have been made to identify patients at high risk of recurrence. To identify these patients in the early phase of the index stroke, DWI, which is the most sensitive imaging method for detecting hyperacute ischemic stroke [4,5], has been rigorously used to detect early recurrent ischemic lesions.
Definition and incidence
SNILs can be arbitrarily divided into early and late SNILs based on the time of magnetic resonance imaging (MRI). Early SNILs are usually defined as a new lesion on 5-day to 7-day DWI outside the region of the acutely symptomatic lesion (Table 1) [6-14]. Early SNILs are reportedly found in 24.2%-34.3% of patients with acute ischemic stroke [6-11], while higher rates have been reported in patients with large artery atherosclerosis [13,14] or in those receiving thrombolysis [12]. These rates of early SNILs largely exceed those of clinical evident recurrence, of which the cumulative rates have been reported to be 2% within 1 week [15] and 1.6%-8% in 90 days [16-18]. Accordingly, the majority of early SNILs are asymptomatic [6-10,13].
Table 1.
New ischemic lesions after acute ischemic stroke and minor stroke or TIA
| Author | Time of follow-up MRI | No. of patients | Incidence of SNILs | Asymptomatic | Factors associated with new ischemic lesions* | |
|---|---|---|---|---|---|---|
| Kang [6] | Within 1 week | 99 | 34 (34.3%) | 32 (94.1%) | Initial multiple DWI lesions | |
| Kang [7] | Early: 5 days | 80 | Early: 27 (33.8%) | Early: 25 (92.6%) | Early lesion recurrence (for late lesion recurrence) | |
| Late: 30/90 days | Late: 21 (26.3%) | Late: 18 (85.7%) | ||||
| Kang [8] | Early: 5 days | 104 | Early: 35 (33.7%) | Early: 35 (100%) | ||
| Late: 30/90 days | Late: 15 (22.1% of 68) | Late: 10 (66.7%) | ||||
| Nolte [9] | 2nd: <48 hours | 159 | 46 (28.9%) | 42 (91.3%) | Carotid stenosis >50% | |
| 3rd: 5/6 days | Recanalization | |||||
| Multiple lesion pattern | ||||||
| Kang [10] | 5 days | 153 | 37 (24.2%) | 35 (94.6%) | Initial multiple DWI lesions | |
| Large artery atherosclerosis | ||||||
| Log D-dimer | ||||||
| Jeon [11] | 7 days | 117 | 34 (29.1%) | Not specified | Biochemical aspirin resistance (for distant early lesion recurrence) | |
| Bang [12] | 7 days | 74 | 39 (52.7%) | Not specified | Large mild perfusion delay, endovascular therapy | |
| Kang [13] | Within 1 week | 133 | 63 (47.4%) | 55 (87.3%) | ||
| Jeong [14] | 5 days | 76 | 36 (47.4%) | Not specified | A certain CYP2C19 genotype, poor metabolizer | |
| Minor stroke or TIA | ||||||
| Coutts [29] | 30 days | 143 (65 TIA) | 14 (9.8%) | 8 (57.1%) | ||
| Asdaghi [30] | 7, 30 days | 50 (22 TIA) | 9 (18.0%) at 7 days | 6 (66.7%) | Baseline DWI lesion volume | |
| 11 (22.0%) at 30 days | ||||||
| Nah [31] | 3 days (in 45) | 90 TIA | 3 days: 21/45 (46.7%) | 3 days: 14 (66.7%) | ||
| 90 days (in 45) | 90 days: 3/45 (6.7%) | 90 days: 2 (66.7%) | ||||
Only variables determined as significant by multivariable analysis.
DWI, diffusion-weighted imaging; MRI, magnetic resonance imaging; SNILs, silent new ischemic lesions; TIA, transient ischemic attack.
Late SNILs occurring at a subacute stage have also been measured in several studies using DWI and fluid attenuated inversion recovery imaging at 30 or 90 days after the index stroke [7,8]. In these studies, the incidence of late SNILs was reported as 22.1%-26.3%, which is lower than that of early SNILs. However, the majority of late SNILs are also asymptomatic.
Characteristics
SNILs after acute ischemic stroke can be further categorized into two groups based on their locations, namely “local” or “distant” lesion recurrence according to whether a new lesion occurs within or outside the territory of initial perfusion deficit (Figures 1 and 2) [6,7]. In early SNILs, the proportion of local lesion recurrence is slightly higher than that of distant lesion recurrence (44.4%-51.9% vs. 44.1%-47.1%). On the contrary, in late SNILs, local lesion recurrence is less frequent than distant lesion recurrence (23.8% vs. 76.2%) [7].
Figure 1.
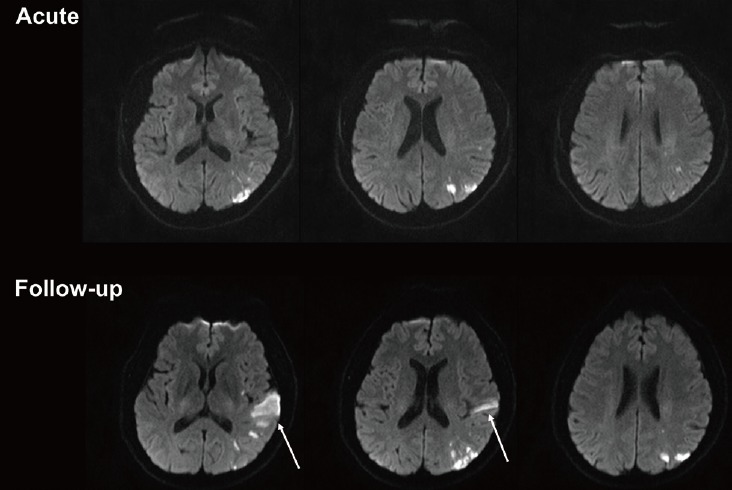
Early local silent new ischemic lesions (SNILs). Acute diffusion-weighted imaging (DWI) was performed within 24 hours after symptom onset and follow-up DWI was performed 2 days after the index ischemic stroke. Early local SNILs (arrows) are shown on the follow-up DWI.
Figure 2.
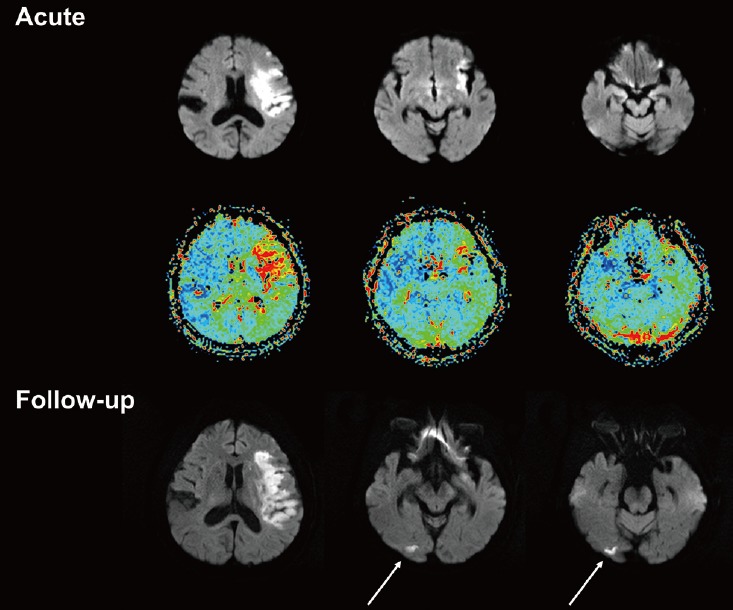
Early distant silent new ischemic lesions (SNILs). Acute diffusion-weighted imaging (DWI) and perfusion-weighted imaging were performed within 24 hours after symptom onset. Follow-up DWI was performed 8 days after the index ischemic stroke. Early distant SNILs (arrows) are indicated on the follow-up DWI.
Moreover, the lesion size of most SNILs is small [12,13], with the reported lesion volumes ranging between 0.3 and 0.7 mL [13], and the majority of SNILs (70.6%) being 10 mm or less in diameter [12]. These findings are consistent with the fact that most recurrent ischemic lesions do not cause any evident symptoms in the patients.
Associated factors and mechanism
Multiple ischemic lesions on baseline DWI are significantly associated with early SNILs [6,9,10]. If multiple acute lesions are demonstrated on clinical presentation, especially with varying degree of apparent diffusion coefficient (e.g., reduced and normalized), those lesions may have occurred at varying time points before or after the clinical stroke onset [6,19]. Moreover, increased microembolic events have been reported to be related with these multiple lesion patterns [20].
Among the different stroke subtypes, large-artery atherosclerosis (LAA) has been most frequently associated with early SNILs [6,8-10,13], and has been shown as an independent predictor of SNILs after acute ischemic stroke [10]. In particular, early SNILs in intracranial LAA have different characteristics compared to other stroke subtypes [13]. Early SNILs in intracranial LAA occur mostly in the pial area of the same vascular territory as the index stroke and are more frequently observed in higher grades of stenosis. On the other hand, in extracranial LAA, the degree of stenosis is not related to early SNILs, and these are not associated with subsequent recanalization, whereas in cases of cardioembolism, early SNILs are associated with significant recanalization. In intracranial LAA, artery-to-artery embolism or hemodynamic insufficiency may play an important role in the pathogenesis of recurrent ischemic stroke [21]. Meanwhile, plaque heterogeneity and fragmentation of the initial embolus may be more crucial in the pathogenesis of SNILs in extracranial LAA and cardioembolism, respectively [22]. Lastly, early SNILs in intracranial LAA are more closely associated with clinical recurrence than in the other subtypes. In line with these findings, patients with stroke resulting from intracranial LAA have been demonstrated to show a high risk of recurrent stroke (>20% over 2 years) [23].
Thrombolytic therapy and vessel recanalization have also been shown to be associated with early SNILs [9,12]. Chronologically, recombinant tissue-type plasminogen activator treatment is associated with acute SNILs, which occur between 24 and 48 hours, while spontaneous vessel recanalization is associated with subacute SNILs, occurring between 2 and 6 days [9]. Recombinant tissue-type plasminogen activator treatment can contribute to the occurrence of SNILs by imperfect dissolution of either the embolus at the site of the main vessel occlusion or the thrombus at the site of origin; however, its short half-life may limit its role to only the acute phase.
Regarding the baseline hypoperfusion status, large mild perfusion delays have been shown to be independently associated with early SNILs. Meanwhile, more severe perfusion delays, together with large initial DWI lesion, have been demonstrated to be related with infarct lesion growth in the subsequent DWI within 7 days [12].
Among the various plasma or serum biomarkers measured within 24 hours after the onset of index stroke, an elevated level of D-dimer has been shown to be independently associated with early SNILs at 5-day [10]. Increased D-dimer levels may reflect ongoing thrombus formation within cerebral vessels or systemic hypercoagulability [24]. Moreover, D-dimer itself may induce the inflammatory process by stimulating monocyte synthesis and release of proinflammatory cytokines such as interleukin-6 [25].
Insufficient inhibition of platelet aggregation by the administered drugs may also contribute to the advent of SNILs [11,14]. Biochemical aspirin resistance, defined as an aspirin reaction unit ≥550 (VerifyNow Aspirin Assay), was associated with distant early SNILs occurring outside the vascular territories of index stroke in one previous study [11]. In addition, a certain genotype of cytochrome P450 2C19, which poorly metabolizes clopidogrel into its active form, has been reported to relate with a significantly higher rate of SNILs in patients with stroke due to LAA [14].
Taken together, the mechanisms of early or late SNILs are diverse (Figure 3), and they can be categorized according to the locational distribution of SNILs. For local lesion recurrence, several mechanisms are plausible, including 1) fragmentation of the initial embolus during the process of recanalization and reperfusion [6]; 2) recurrent ischemic events (recurrent emboli) within the same perfusion deficit caused by intrinsic atherosclerosis [6]; and 3) recurrent ischemic events due to prolonged hypoperfusion [11]. Meanwhile, for distant lesion recurrence, recurrent embolic events arising from a proximal source, such as the heart or activated atherosclerotic plaque located outside of the initial culprit vessels, may be important. Accordingly, atrial fibrillation and the presence of microembolic signals demonstrated by transcranial Doppler ultrasonography are reportedly associated with the advent of early SNILs [20]. Of note, there are also other players acting as common pathogenic denominators. For example, induced inflammatory response after stroke and/or hypercoagulability, which sustainably activate plaque, may contribute to the development of both local and distant SNILs [6].
Figure 3.
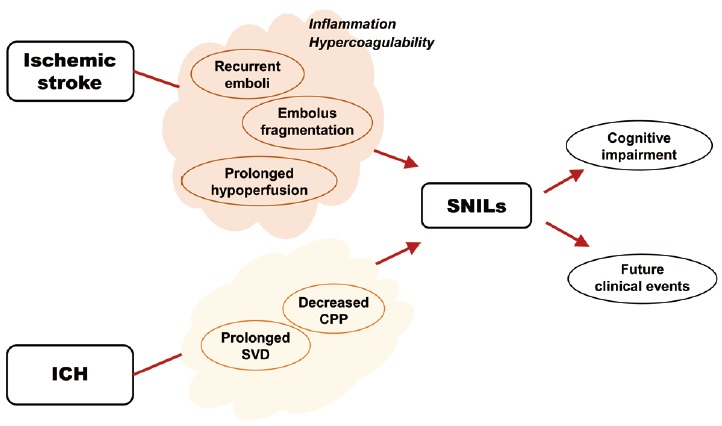
Pathophysiology and clinical implications of silent new ischemic lesions (SNILs) after stroke. CPP, cerebral perfusion pressure; ICH, intracerebral hemorrhage; SVD, small vessel disease.
Early and late SNILs and clinical vascular events
Early SNILs at 5 days have been shown to be independently associated with late SNILs at 30 or 90 days, suggesting a continued risk of recurrent ischemic lesions in the weeks following the index stroke [7]. Atheroma, which is an acute-on-chronic disease causing recurrent episodes of thromboembolism before the stabilization of an ulcerated plaque, has been suggested as the culprit mechanism for this prolonged stroke-prone state [26].
As for clinical vascular events, late SNILs independently predict recurrent ischemic strokes. Early SNILs, together with late SNILs, can predict the combined clinical endpoints of recurrent ischemic stroke, transient ischemic attack (TIA), and vascular death [8]. The superiority of late SNILs to early SNILs in predicting subsequent clinical vascular events may be explained by the different pathogeneses of the two types of SNILs. Early SNILs, which include local lesion recurrence, may result from progression of the initial ischemic event. On the contrary, late SNILs, of which the major form is distant lesion recurrence, may accurately reflect the risk of future recurrent ischemic events [8].
Minor stroke and TIA
It has been considered that a previous TIA or minor stroke confers a greater risk for recurrent stroke [27,28]. Accordingly, SNILs can also appear after TIA and minor stroke (National Institutes of Health Stroke Scale score <3-6) [29-31]. The incidences of SNILs in this population have been reported as 18% at 7 days, and 7%-22% at 30 or 90 days, both of which are lower than those of SNILs after acute ischemic stroke (Table 1). This difference may be attributable to the fact that TIA and minor strokes are less likely to recur compared to acute ischemic strokes [29].
Further, LAA and cardioembolism are most likely to be associated with SNILs in patients with TIA and minor strokes [19,29]. Among the MRI parameters, the baseline DWI lesion volume and perfusion deficits have been shown to significantly associate with the advent of SNILs [30,31].
SNILs after acute intracerebral hemorrhage (ICH)
Since ischemic and hemorrhagic strokes are distinctive diseases, stroke patients usually present with one of the two. However, although rare, symptomatic acute ischemic and hemorrhagic stroke can occur simultaneously or shortly after one another [32-34]. Moreover, both types of stroke share common risk factors such as old age, hypertension, and high alcohol intake [35,36]. In this regard, there have been efforts to investigate SNILs after acute ICH using DWI.
Definition, incidence, and baseline characteristics
SNILs after acute ICH are defined as any hyperintense lesions on the subsequent DWI that are distinct from hemorrhage and the area of perihematomal edema (Figure 4) [37-43]. SNILs may appear as early as within 5 days; follow-up MRI is usually performed within 14 days, but may be performed up to 3 months after the index hemorrhage (Table 2). The reported prevalence rates of SNILs after acute ICH are 11.1%-41.1% within 14-days, 22.9%-26.5% at 1 month, and 13.2% at 3 months. The lesion size of SNILs after ICH also tends to be small; more than 70% of lesions have a diameter less than 10 mm [37,38,42]. Further, patients with cerebral amyloid angiopathy are more likely to develop SNILs at 3 months after ICH, and have a more severe hemorrhagic burden (i.e., more frequent microbleeds, multiple ICHs, and intraventricular hemorrhage) compared to those with other primary ICHs [38]. The main locations of SNILs have been reported to vary. Notably, however, patients with hypertensive ICH develop SNILs mainly in the subcortical white matter or brainstem [41].
Figure 4.
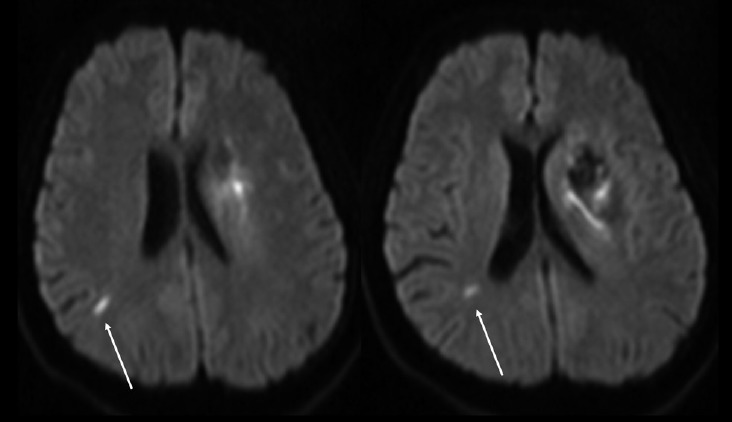
Early silent new ischemic lesions (arrows) coexisting with acute intracerebral hemorrhage in the left basal ganglion. Magnetic resonance imaging was performed 2 days after symptom onset.
Table 2.
New ischemic lesions after acute intracerebral hemorrhage
| Time of follow-up MRI | No. of patients | Incidence of SNILs | Location | Associated factors with new ischemic lesions* | |
|---|---|---|---|---|---|
| Prabhakaran [37] | Within 28 days | 118 | 27 (22.9%) | Subcortical (70.4%) | Prior ischemic stroke, craniotomy, delta MAP |
| lowering ≥40%, hypertensive etiology | |||||
| Gregoire [38] | Within 3 months | 114 | 15 (13.2%) | Mainly cortical | WM change score |
| CAA: 9/39 (23.1%) | Presence of lobar MBs | ||||
| Others: 6/75 (8.0%) | |||||
| Menon [39] | Baseline (median 2 days) and 1 month | 138 | Base: 42/119 (35.2%) | Base: 44% in lobar | Baseline: Hematoma volume, baseline IVH, baseline MBs, and delta MAP |
| 1 month: 30/113 (26.5%)† | 1 month: 13% in lobar | ||||
| 1 month: Any prior stroke, baseline microbleeds | |||||
| Garg [40] | Within 10 days | 95 | 39 (41.1%) | Not available | |
| Kang [41] | Within 5 days | 97‡ | 26 (26.8%) | Subcortical WM or brainstem (75.5%) | Baseline MBs >2, moderate-to-severe WM leukoaraiosis |
| Tsai [42] | 2 weeks (DWI) | 153 | 2 weeks: 17/153 (11.1%) § | Cortical (64.7%) | |
| 3 months (T2W/FLAIR) | |||||
| Gioia [43] | Within 14 days | 117 | 17 (14.5%) | Cortical (50.0%) | |
| Subcortical (47.6%) |
Only variables determined as significant by multivariable analysis;
Of the 40 DWI lesions at 1 month, 33 (82.5%) were new compared to in the baseline DWI;
Only patients with hypertensive intracranial hemorrhage;
Of the 20 DWI lesions, 13 (52.0%) were not found on the follow-up T2-weighted or FLAIR images.
CAA, cerebral amyloid angiopathy; DWI, diffusion-weighted imaging; FLAIR, fluid attenuated inversion recovery; IVH, intraventricular hemorrhage; MAP, mean arterial pressure; MBs, microbleeds; MRI, magnetic resonance imaging; SNILs, silent new ischemic lesions; T2W, T2 weighted; WM, white matter.
The natural course of SNILs after acute ICH is dynamic. When comparing baseline (median, 2 days) and 1-month DWIs after acute primary ICH, more than 80% of SNILs on the follow-up DWI were not present at baseline, demonstrating that SNILs develop through an ongoing process during the acute phase [39]. Meanwhile, half of all SNILs on the 2-week DWI reportedly do not remain on the subsequent 3-month MRI, suggesting that not all early SNILs after acute ICH indicate permanent tissue injury [42].
Associated factors and mechanisms
Several risk and clinical factors have been reported to be assoassociated with SNILs after acute ICH, although the results are inconsistent and even contradictory among studies.
Microbleeds and leukoaraiosis have been independently and consistently associated with the occurrence of SNILs after acute ICH [38,39,41]. Microbleeds are an imaging marker of bleeding-prone microangiopathies [44], while leukoaraiosis represents chronic hypoperfusion in the distal deep and arteriolar territories [45]. Remarkably, microbleeds and leukoaraiosis are strongly correlated [46], and, when combined, they represent small vessel pathology [47]. Chronic changes by longstanding hypertension in the form of microaneurysm, lipohyalinosis, and fibrinoid degeneration develop in the deep small vessels and are associated with both hypertensive ICH and ischemic lacunes. Thus, an active small-vessel angiopathic process induced by hemorrhagic insults may underlie the advent of SNILs [41].
History of ischemic stroke has been suggested as an independent predictor of SNILs after acute ICH [37,39]. Moreover, this has been regarded as a surrogate marker of perforator disease, where relative hypoperfusion can result in ischemia in a single or multiple perforators [37]. However, the association between prior ischemic stroke and SNILs after acute ICH was denied in other studies [40,41].
Another suggested risk factor of SNILs after acute ICH is decreased blood pressure during the acute phase [37,39,40]. In chronic hypertension, the curve of cerebral autoregulation is shifted to the right, and after acute brain injury, autoregulation may be abolished so that cerebral blood flow changes linearly according to cerebral perfusion pressure [48]. As elevations in intracranial pressure due to acute ICH would result in cerebral perfusion pressure decreases, aggressive blood pressure lowering therapy beyond the lower limits of cerebral autoregulation might induce cerebral ischemia in ICH patients with chronic hypertension [37]. However, of note, the perihematoma region is known to be unaccompanied by hypoperfusion or ischemia, and rather shows benign oligemia [49-53]. Moreover, the relationship between reduction of blood pressure and the advent of SNILs was not reproduced in some studies [41,43]. Thus, it remains controversial whether decreased blood pressure is the culprit behind the occurrence of SNILs.
Large ICH volume and subsequent craniotomy have been suggested to be associated with SNIL development [37,39]. Elevated intracranial pressure in patients with large volume of ICH may have a negative impact on the cerebral perfusion pressure and secondarily on the cerebral blood flow. In addition, brain shifts from large hematomas may directly compress neighboring vascular structures, contributing to tissue infarction. However, both large ICH volume and craniotomy did not show any significant association with SNILs in other studies [40,41].
Clinical implication of SNILs
Predictor of prognosis and future events
SNILs on DWI after acute ischemic or hemorrhagic stroke can be used to predict future clinical events and prognosis. DWI can be considered as a crystal ball, while SNILs are an omen.
Regarding SNILs after acute ischemic stroke, both early SNILs at 5 days and late SNILs in the subacute phase up to 90 days have been shown to be independent predictors of subsequent clinical vascular events such as recurrent ischemic stroke, TIA, and vascular death during a median follow-up of 1.6 years [7,8]. Thus, patients with SNILs over the early weeks after an index stroke should be considered optimal candidates for early aggressive stroke prevention therapy. In addition, SNILs may provide a useful surrogate endpoint in clinical trials evaluating stroke prevention therapies, with the reduction in the lesion recurrence rate upon pharmacologic intervention over the initial weeks used as a surrogate for reduction in clinical stroke recurrence over the following years. Clinical trials to test the efficacy of therapeutic interventions usually take many years to recruit for and complete. An MRI surrogate endpoint of recurrent stroke, which would allow substantially fewer patients and shorter follow-up period, would result in enormous savings of cost and time in evaluating the preventive therapies. However, currently, only data from single-center and retrospective studies are available. Thus, future prospective randomized controlled trials testing the effect of a stroke prevention therapy on SNILs and clinical stroke recurrence in the long-term are required.
SNILs after acute ICH also have prognostic value; in one study, they were independently associated with dependence or death of patients at 3 months [40], and in another, with the comcomposite of clinical cerebrovascular endpoints (i.e., ischemic stroke, ICH, and vascular death) during a median follow-up of 3.5 years [41]. These findings warrant special care in ICH patients with SNILs to reduce the risk of cerebrovascular events in the future. As SNILs after acute ICH predict not only hemorrhagic but also ischemic strokes during the follow-up, antiplatelets associated with lower risks of bleeding complications may be considered in this group of patients to prevent subsequent cerebrovascular events. The efficacy of antiplatelets in these patients should be proven, and the safe interval from ICH onset to initiation of antiplatelet administration is also to be determined. In addition, the optimal level of blood pressure should be delicately set to prevent SNILs as well as ICH progression.
Cognitive impairment
Silent ischemic lesions on MRI have been associated with cognitive dysfunction or dementia in asymptomatic populations [54-67]. The size and location of ischemic lesions may be important for such associations. In order to remain silent, the ischemic lesions should be small and located in appropriate areas such as the frontal lobe, not causing focal neurologic deficits. However, as silent lesions accumulate in the affected area, the increased ischemic burden may contribute to impairment of cognitive function and to difficulties in mental flexibility, language, and memories [68-74]. Besides the location, the extent of silent ischemic lesions is also important for the development of cognitive dysfunction. The degree of the lesions on MRI has shown a positive correlation with the severity of cognitive impairment [65,75-77].
SNILs after acute ischemic or hemorrhagic strokes are small and asymptomatic initially; further, they can occur virtually anywhere according to the location of the index stroke. Thus, their accumulation may also contribute to cognitive decline during the follow-up. Moreover, considering that many patients with a history of ischemic or hemorrhagic strokes are also accompanied by many vascular risk factors, which are known to increase the risk of dementia [78], special attention should be paid to the risk of cognitive impairment in these patients.
SNMs
Microbleeds refer to small, round, dark-signal lesions detected by T2*-weighted GRE or susceptibility-weighted imaging [79-81]. They are known to be manifestations of focal extravascular leakage of blood components, representing old microhemorrhages, but rarely cause overt symptoms [82]. Although not studied as much as SNILs, SNMs are also known to appear after acute ischemic or hemorrhagic stroke.
SNMs after acute ischemic stroke
Microbleeds are frequently found in ischemic stroke patients, at varying rates (35%-71%) [82-84]. In addition, they are more common in patients with recurrent strokes than in those experiencing a first-ever stroke [85], whereas they are rarely found in TIA patients [86]. These findings suggest that ischemic stroke may trigger the occurrence of microbleeds.
Definition and incidence
Microbleeds are defined as unambiguous homogeneous, round, signal-loss lesions with diameters up to 5-10 mm and with blooming artifacts, as determined by GRE [87-89]. In one previous study, within 24 hours, approximately 30% of patients with acute ischemic stroke showed a number of concurrent microbleeds (median 2, range 1-33) in their brains [87]. During the acute phase, another 13% of patients developed SNMs (median 1, range 1-5) on the 7-day GRE, while 3% of patients lost their baseline microbleeds [87]. As for the locations, about half of all microbleeds were detected in the deep hemisphere; at baseline, 32% were located in the lobar location while 30% were in the deep location, whereas on follow-up GRE, 52% of SNMs were found in the lobar location [87].
The long-term fate of SNMs is also dynamic, as the appearance and disappearance of SNMs can occur years after the index acute ischemic stroke [88,89]. In one study, during a mean follow-up of 27 months, 38% of acute ischemic stroke patients had SNMs on their subsequent GRE, with the total number of microbleeds increasing by about 1.5-fold [88]. Among the patients with baseline microbleeds, 54% developed SNMs during their follow-up, showing a generally increasing trend in the number of microbleeds, although some of these lesions disappeared in 15% of those patients. In fact, de novo SNMs were detected even on the 5-year follow-up GRE in 30% of patients with index ischemic strokes [89].
Associated factors and mechanism
The presence and number of baseline microbleeds are consistently associated with the advent of SNMs on follow-up GREs, regardless of the time from baseline (5 days to 5 years) [87-89]. Moreover, they have been shown to be positively related with the annual rate at which SNMs develop [88]. The multiplicity of microbleeds at the initial clinical presentation may imply that they occurred through various time points around the onset of stroke, suggesting a prolonged risk of SNMs in particular stroke patients [87]. The number of baseline hemorrhages may be a marker of the severity and aggressiveness of the underlying vascular disease [87]. In addition, the above findings are in line with findings of other studies indicating that the total number of baseline microbleeds can predict the risk of future hemorrhages [90-92]. The burden of small vessel disease such as leukoaraiosis or lacunar infarctions is an independent predictor of the development of SNMs in ischemic stroke patients [87,88]. The small vessel disease severity is well known to correlate with the number of microbleeds [46]. As microbleeds arise from microangiopathic changes after chronic hypertension, the number of microbleeds may hence reflect bleeding-prone and small vessel disease-prone microangiopathy [93].
The level of low-density lipoprotein cholesterol is inversely associated with SNMs [88]. Low concentrations of serum cholesterol are related with the risk of microbleeds, suggesting an antagonizing role of cholesterol in the pathogenesis of microbleeds [94,95]. Given that microbleeds is characterized by hemosiderin pigment accumulations in macrophages adjacent to the ruptured atherosclerotic microvessels, the low-density lipoprotein cholesterol level may be related to either changes of microaneurysms [94,96] or the clearance of hemosiderin-containing microglia [88].
Increased body temperature has also been reported to be associated with the presence of SNMs within 7 days [87]. High temperature is known to induce blood-brain barrier disruption after ischemic stroke [97]. As endothelial activation and damage, with subsequent breakdown of the blood-brain barrier, are key features in cerebral small vessel diseases, high temperature may also contribute to the disease process [98].
However, a caution in interpretation is needed for the above-mentioned studies, since spatial registration of baseline and follow-up GRE images have not been performed in any published studies [82].
SNMs after acute ICH
The coexistence of SNMs in patients with ICH has consistently been reported as more frequent than that in ischemic stroke patients, reaching 50%-80% [91,93,99-101]. However, only limited studies have evaluated whether SNMs occur following acute ICH by performing serial GRE studies.
In one study, SNMs occurred in 9 of 24 patients (38%) with cerebral amyloid angiopathy and previous lobar hemorrhage during the 1.5-year follow-up period [102]. In another study, in hypertensive ICH patients, SNMs were found in 19 of 63 patients (30%) after a median follow-up of 23 months [90].
Clinical implication of SNMs
Since its discovery, the clinical significance of microbleeds has been actively investigated. The presence of microbleeds is associated with the future advent of hemorrhagic stroke after index ischemic or hemorrhagic stroke, especially in patients with severe white matter ischemic lesions [90,103,104]. In addition, microbleeds have been associated with larger volume of ICH [105,106] and hemorrhagic transformation after ischemic stroke [107-109], although the latter has been denied by other studies [110-114]. Recurrent ischemic stroke also has been linked to the presence of microbleeds [115], while the association turned out to be only modest when compared to that of hemorrhagic stroke in a systematic review [103]. Lastly, microbleeds are associated with cognitive dysfunction, especially frontal-executive impairment [116,117].
Based on the above-mentioned data, SNMs appearing after acute cerebrovascular events may be suggestive of future risk of hemorrhagic stroke and cognitive dysfunction, similar to SNILs. However, there is currently no direct evidence that SNMs can predict these events in the early phase after acute events. Thus, SNMs should be examined in more detail in terms of their clinical implications, and future studies are warranted.
This research was supported by the National Research Foundation of Korea Grant NRF-2014R1A2A1A11051280 funded by the Korea government, and the Korea Health Technology R&D Project, Ministry for Health & Welfare, Republic of Korea Grants HI12C1847 and HI14C1983.
The authors have no financial conflicts of interest.
References
- 1.Derdeyn CP. Diffusion-weighted imaging as a surrogate marker for stroke as a complication of cerebrovascular procedures and devices. AJNR Am J Neuroradiol. 2001;22:1234–1235. [PMC free article] [PubMed] [Google Scholar]
- 2.Sacco RL, Foulkes MA, Mohr JP, Wolf PA, Hier DB, Price TR. Determinants of early recurrence of cerebral infarction. The Stroke Data Bank. Stroke. 1989;20:983–989. doi: 10.1161/01.str.20.8.983. [DOI] [PubMed] [Google Scholar]
- 3.Sacco RL, Shi T, Zamanillo MC, Kargman DE. Predictors of mortality and recurrence after hospitalized cerebral infarction in an urban community: the Northern Manhattan Stroke Study. Neurology. 1994;44:626–634. doi: 10.1212/wnl.44.4.626. [DOI] [PubMed] [Google Scholar]
- 4.Warach S, Gaa J, Siewert B, Wielopolski P, Edelman RR. Acute human stroke studied by whole brain echo planar diffusion-weighted magnetic resonance imaging. Ann Neurol. 1995;37:231–241. doi: 10.1002/ana.410370214. [DOI] [PubMed] [Google Scholar]
- 5.Roh JK, Kang DW, Lee SH, Yoon BW, Chang KH. Significance of acute multiple brain infarction on diffusion-weighted imaging. Stroke. 2000;31:688–694. doi: 10.1161/01.str.31.3.688. [DOI] [PubMed] [Google Scholar]
- 6.Kang DW, Latour LL, Chalela JA, Dambrosia J, Warach S. Early ischemic lesion recurrence within a week after acute ischemic stroke. Ann Neurol. 2003;54:66–74. doi: 10.1002/ana.10592. [DOI] [PubMed] [Google Scholar]
- 7.Kang DW, Latour LL, Chalela JA, Dambrosia JA, Warach S. Early and late recurrence of ischemic lesion on MRI: evidence for a prolonged stroke-prone state? Neurology. 2004;63:2261–2265. doi: 10.1212/01.wnl.0000147295.50029.67. [DOI] [PubMed] [Google Scholar]
- 8.Kang DW, Lattimore SU, Latour LL, Warach S. Silent ischemic lesion recurrence on magnetic resonance imaging predicts subsequent clinical vascular events. Arch Neurol. 2006;63:1730–1733. doi: 10.1001/archneur.63.12.1730. [DOI] [PubMed] [Google Scholar]
- 9.Nolte CH, Albach FN, Heuschmann PU, Brunecker P, Villringer K, Endres M, et al. Silent new DWI lesions within the first week after stroke. Cerebrovasc Dis. 2012;33:248–254. doi: 10.1159/000334665. [DOI] [PubMed] [Google Scholar]
- 10.Kang DW, Yoo SH, Chun S, Kwon KY, Kwon SU, Koh JY, et al. Inflammatory and hemostatic biomarkers associated with early recurrent ischemic lesions in acute ischemic stroke. Stroke. 2009;40:1653–1658. doi: 10.1161/STROKEAHA.108.539429. [DOI] [PubMed] [Google Scholar]
- 11.Jeon SB, Song HS, Kim BJ, Kim HJ, Kang DW, Kim JS, et al. Biochemical aspirin resistance and recurrent lesions in patients with acute ischemic stroke. Eur Neurol. 2010;64:51–57. doi: 10.1159/000315147. [DOI] [PubMed] [Google Scholar]
- 12.Bang OY, Kim GM, Chung CS, Kim SJ, Kim KH, Jeon P, et al. Differential pathophysiological mechanisms of stroke evolution between new lesions and lesion growth: perfusion-weighted imaging study. Cerebrovasc Dis. 2010;29:328–335. doi: 10.1159/000278928. [DOI] [PubMed] [Google Scholar]
- 13.Kang DW, Kwon SU, Yoo SH, Kwon KY, Choi CG, Kim SJ, et al. Early recurrent ischemic lesions on diffusion-weighted imaging in symptomatic intracranial atherosclerosis. Arch Neurol. 2007;64:50–54. doi: 10.1001/archneur.64.1.50. [DOI] [PubMed] [Google Scholar]
- 14.Jeong TD, Kim SM, Kim HJ, Lee W, Kwon SU, Min WK, et al. CYP2C19 genotype and early ischemic lesion recurrence in stroke patients treated with clopidogrel. J Stroke Cerebrovasc Dis. 2015;24:440–446. doi: 10.1016/j.jstrokecerebrovasdis.2014.09.014. [DOI] [PubMed] [Google Scholar]
- 15.Petty GW, Brown RD, Jr, Whisnant JP, Sicks JD, O’Fallon WM, Wiebers DO. Survival and recurrence after first cerebral infarction: a population-based study in Rochester, Minnesota, 1975 through 1989. Neurology. 1998;50:208–216. doi: 10.1212/wnl.50.1.208. [DOI] [PubMed] [Google Scholar]
- 16.Berge E, Abdelnoor M, Nakstad PH, Sandset PM. Low molecular-weight heparin versus aspirin in patients with acute ischaemic stroke and atrial fibrillation: a double-blind randomised study. HAEST Study Group. Heparin in Acute Embolic Stroke Trial. Lancet. 2000;355:1205–1210. doi: 10.1016/s0140-6736(00)02085-7. [DOI] [PubMed] [Google Scholar]
- 17.The Publications Committee for the Trial of ORG 10172 in Acute Stroke Treatment (TOAST) Investigators Low molecular weight heparinoid, ORG 10172 (danaparoid), and outcome after acute ischemic stroke: a randomized controlled trial. JAMA. 1998;279:1265–1272. [PubMed] [Google Scholar]
- 18.International Stroke Trial Collaborative Group The International Stroke Trial (IST): a randomised trial of aspirin, subcutaneous heparin, both, or neither among 19435 patients with acute ischaemic stroke. Lancet. 1997;349:1569–1581. [PubMed] [Google Scholar]
- 19.Sylaja PN, Coutts SB, Subramaniam S, Hill MD, Eliasziw M, Demchuk AM. Acute ischemic lesions of varying ages predict risk of ischemic events in stroke/TIA patients. Neurology. 2007;68:415–419. doi: 10.1212/01.wnl.0000252938.76188.52. [DOI] [PubMed] [Google Scholar]
- 20.Iguchi Y, Kimura K, Kobayashi K, Ueno Y, Shibazaki K, Inoue T. Microembolic signals at 48 hours after stroke onset contribute to new ischaemia within a week. J Neurol Neurosurg Psychiatry. 2008;79:253–259. doi: 10.1136/jnnp.2007.123414. [DOI] [PubMed] [Google Scholar]
- 21.Arenillas JF, Molina CA, Montaner J, Abilleira S, Gonzalez-Sanchez MA, Alvarez-Sabin J. Progression and clinical recurrence of symptomatic middle cerebral artery stenosis: a long-term follow-up transcranial Doppler ultrasound study. Stroke. 2001;32:2898–2904. doi: 10.1161/hs1201.099652. [DOI] [PubMed] [Google Scholar]
- 22.AbuRahma AF, Wulu JT, Jr, Crotty B. Carotid plaque ultrasonic heterogeneity and severity of stenosis. Stroke. 2002;33:1772–1775. doi: 10.1161/01.str.0000019127.11189.b5. [DOI] [PubMed] [Google Scholar]
- 23.Chimowitz MI, Lynn MJ, Howlett-Smith H, Stern BJ, Hertzberg VS, Frankel MR, et al. Comparison of warfarin and aspirin for symptomatic intracranial arterial stenosis. N Engl J Med. 2005;352:1305–1316. doi: 10.1056/NEJMoa043033. [DOI] [PubMed] [Google Scholar]
- 24.Barber M, Langhorne P, Rumley A, Lowe GD, Stott DJ. Hemostatic function and progressing ischemic stroke: D-dimer predicts early clinical progression. Stroke. 2004;35:1421–1425. doi: 10.1161/01.STR.0000126890.63512.41. [DOI] [PubMed] [Google Scholar]
- 25.Robson SC, Shephard EG, Kirsch RE. Fibrin degradation product D-dimer induces the synthesis and release of biologically active IL-1 beta, IL-6 and plasminogen activator inhibitors from monocytes in vitro. Br J Haematol. 1994;86:322–326. doi: 10.1111/j.1365-2141.1994.tb04733.x. [DOI] [PubMed] [Google Scholar]
- 26.Hankey GJ, Jamrozik K, Broadhurst RJ, Forbes S, Burvill PW, Anderson CS, et al. Long-term risk of first recurrent stroke in the Perth Community Stroke Study. Stroke. 1998;29:2491–2500. doi: 10.1161/01.str.29.12.2491. [DOI] [PubMed] [Google Scholar]
- 27.Whisnant JP, Matsumoto N, Elveback LR. Transient cerebral ischemic attacks in a community. Rochester, Minnesota, 1955 through 1969. Mayo Clin Proc. 1973;48:194–198. [PubMed] [Google Scholar]
- 28.Friedman GD, Wilson WS, Mosier JM, Colandrea MA, Nichaman MZ. Transient ischemic attacks in a community. JAMA. 1969;210:1428–1434. [PubMed] [Google Scholar]
- 29.Coutts SB, Hill MD, Simon JE, Sohn CH, Scott JN, Demchuk AM. Silent ischemia in minor stroke and TIA patients identified on MR imaging. Neurology. 2005;65:513–517. doi: 10.1212/01.wnl.0000169031.39264.ff. [DOI] [PubMed] [Google Scholar]
- 30.Asdaghi N, Hameed B, Saini M, Jeerakathil T, Emery D, Butcher K. Acute perfusion and diffusion abnormalities predict early new MRI lesions 1 week after minor stroke and transient ischemic attack. Stroke. 2011;42:2191–2195. doi: 10.1161/STROKEAHA.110.611376. [DOI] [PubMed] [Google Scholar]
- 31.Nah HW, Kwon SU, Kang DW, Lee DH, Kim JS. Diagnostic and prognostic value of multimodal MRI in transient ischemic attack. Int J Stroke. 2014;9:895–901. doi: 10.1111/ijs.12212. [DOI] [PubMed] [Google Scholar]
- 32.Guzzini F, Conti A, Esposito F. Simultaneous ischemic and hemorrhagic lesions of the brain detected by CT scan in a patient with thrombotic thrombocytopenic purpura. Haematologica. 1998;83:280. [PubMed] [Google Scholar]
- 33.Kim CH, Kim JS. Development of cerebral infarction shortly after intracerebral hemorrhage. Eur Neurol. 2007;57:145–149. doi: 10.1159/000098465. [DOI] [PubMed] [Google Scholar]
- 34.Toyoda K, Kumai Y, Fujii K, Ando T, Ibayashi S. Simultaneous onset of haemorrhagic and ischaemic strokes in a haemodialysis patient. J Neurol Neurosurg Psychiatry. 2002;72:673–674. doi: 10.1136/jnnp.72.5.673. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Ariesen MJ, Claus SP, Rinkel GJ, Algra A. Risk factors for intracerebral hemorrhage in the general population: a systematic review. Stroke. 2003;34:2060–2065. doi: 10.1161/01.STR.0000080678.09344.8D. [DOI] [PubMed] [Google Scholar]
- 36.Allen CL, Bayraktutan U. Risk factors for ischaemic stroke. Int J Stroke. 2008;3:105–116. doi: 10.1111/j.1747-4949.2008.00187.x. [DOI] [PubMed] [Google Scholar]
- 37.Prabhakaran S, Gupta R, Ouyang B, John S, Temes RE, Mohammad Y, et al. Acute brain infarcts after spontaneous intracerebral hemorrhage: a diffusion-weighted imaging study. Stroke. 2010;41:89–94. doi: 10.1161/STROKEAHA.109.566257. [DOI] [PubMed] [Google Scholar]
- 38.Gregoire SM, Charidimou A, Gadapa N, Dolan E, Antoun N, Peeters A, et al. Acute ischaemic brain lesions in intracerebral haemorrhage: multicentre cross-sectional magnetic resonance imaging study. Brain. 2011;134:2376–2386. doi: 10.1093/brain/awr172. [DOI] [PubMed] [Google Scholar]
- 39.Menon RS, Burgess RE, Wing JJ, Gibbons MC, Shara NM, Fernandez S, et al. Predictors of highly prevalent brain ischemia in intracerebral hemorrhage. Ann Neurol. 2012;71:199–205. doi: 10.1002/ana.22668. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Garg RK, Liebling SM, Maas MB, Nemeth AJ, Russell EJ, Naidech AM. Blood pressure reduction, decreased diffusion on MRI, and outcomes after intracerebral hemorrhage. Stroke. 2012;43:67–71. doi: 10.1161/STROKEAHA.111.629493. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Kang DW, Han MK, Kim HJ, Yun SC, Jeon SB, Bae HJ, et al. New ischemic lesions coexisting with acute intracerebral hemorrhage. Neurology. 2012;79:848–855. doi: 10.1212/WNL.0b013e3182648a79. [DOI] [PubMed] [Google Scholar]
- 42.Tsai YH, Lee MH, Weng HH, Chang SW, Yang JT, Huang YC. Fate of diffusion restricted lesions in acute intracerebral hemorrhage. PLoS One. 2014;9: doi: 10.1371/journal.pone.0105970. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Gioia LC, Kate M, Choi V, Sivakumar L, Jeerakathil T, Kosior J, et al. Ischemia in intracerebral hemorrhage is associated with leukoaraiosis and hematoma volume, not blood pressure reduction. Stroke. 2015;46:1541–1547. doi: 10.1161/STROKEAHA.114.008304. [DOI] [PubMed] [Google Scholar]
- 44.Roob G, Fazekas F. Magnetic resonance imaging of cerebral microbleeds. Curr Opin Neurol. 2000;13:69–73. doi: 10.1097/00019052-200002000-00013. [DOI] [PubMed] [Google Scholar]
- 45.Inzitari D. Leukoaraiosis: an independent risk factor for stroke? Stroke. 2003;34:2067–2071. doi: 10.1161/01.STR.0000080934.68280.82. [DOI] [PubMed] [Google Scholar]
- 46.Lee SH, Bae HJ, Ko SB, Kim H, Yoon BW, Roh JK. Comparative analysis of the spatial distribution and severity of cerebral microbleeds and old lacunes. J Neurol Neurosurg Psychiatry. 2004;75:423–427. doi: 10.1136/jnnp.2003.015990. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Staals J, Makin SD, Doubal FN, Dennis MS, Wardlaw JM. Stroke subtype, vascular risk factors, and total MRI brain small-vessel disease burden. Neurology. 2014;83:1228–1234. doi: 10.1212/WNL.0000000000000837. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Paulson OB, Waldemar G, Schmidt JF, Strandgaard S. Cerebral circulation under normal and pathologic conditions. Am J Cardiol. 1989;63:2c–5c. doi: 10.1016/0002-9149(89)90396-2. [DOI] [PubMed] [Google Scholar]
- 49.Powers WJ, Zazulia AR, Videen TO, Adams RE, Yundt KD, Aiyagari V, et al. Autoregulation of cerebral blood flow surrounding acute (6 to 22 hours) intracerebral hemorrhage. Neurology. 2001;57:18–24. doi: 10.1212/wnl.57.1.18. [DOI] [PubMed] [Google Scholar]
- 50.Zazulia AR, Diringer MN, Videen TO, Adams RE, Yundt K, Aiyagari V, et al. Hypoperfusion without ischemia surrounding acute intracerebral hemorrhage. J Cereb Blood Flow Metab. 2001;21:804–810. doi: 10.1097/00004647-200107000-00005. [DOI] [PubMed] [Google Scholar]
- 51.Mayer SA, Lignelli A, Fink ME, Kessler DB, Thomas CE, Swarup R, et al. Perilesional blood flow and edema formation in acute intracerebral hemorrhage: a SPECT study. Stroke. 1998;29:1791–1798. doi: 10.1161/01.str.29.9.1791. [DOI] [PubMed] [Google Scholar]
- 52.Kidwell CS, Saver JL, Mattiello J, Warach S, Liebeskind DS, Starkman S, et al. Diffusion-perfusion MR evaluation of perihematomal injury in hyperacute intracerebral hemorrhage. Neurology. 2001;57:1611–1617. doi: 10.1212/wnl.57.9.1611. [DOI] [PubMed] [Google Scholar]
- 53.Herweh C, Juttler E, Schellinger PD, Klotz E, Jenetzky E, Orakcioglu B, et al. Evidence against a perihemorrhagic penumbra provided by perfusion computed tomography. Stroke. 2007;38:2941–2947. doi: 10.1161/STROKEAHA.107.486977. [DOI] [PubMed] [Google Scholar]
- 54.Hofman A, de Jong PT, van Duijn CM, Breteler MM. Epidemiology of neurological diseases in elderly people: what did we learn from the Rotterdam Study? Lancet Neurol. 2006;5:545–550. doi: 10.1016/S1474-4422(06)70473-2. [DOI] [PubMed] [Google Scholar]
- 55.Longstreth WT, Jr, Dulberg C, Manolio TA, Lewis MR, Beauchamp NJ, Jr, O’Leary D, et al. Incidence, manifestations, and predictors of brain infarcts defined by serial cranial magnetic resonance imaging in the elderly: the Cardiovascular Health Study. Stroke. 2002;33:2376–2382. doi: 10.1161/01.str.0000032241.58727.49. [DOI] [PubMed] [Google Scholar]
- 56.van der Flier WM, van Straaten EC, Barkhof F, Verdelho A, Madureira S, Pantoni L, et al. Small vessel disease and general cognitive function in nondisabled elderly: the LADIS study. Stroke. 2005;36:2116–2120. doi: 10.1161/01.STR.0000179092.59909.42. [DOI] [PubMed] [Google Scholar]
- 57.Mosley TH, Jr, Knopman DS, Catellier DJ, Bryan N, Hutchinson RG, Grothues CA, et al. Cerebral MRI findings and cognitive functioning: the Atherosclerosis Risk in Communities study. Neurology. 2005;64:2056–2062. doi: 10.1212/01.WNL.0000165985.97397.88. [DOI] [PubMed] [Google Scholar]
- 58.Soderlund H, Nilsson LG, Berger K, Breteler MM, Dufouil C, Fuhrer R, et al. Cerebral changes on MRI and cognitive function: the CASCADE study. Neurobiol Aging. 2006;27:16–23. doi: 10.1016/j.neurobiolaging.2004.12.008. [DOI] [PubMed] [Google Scholar]
- 59.Atwood LD, Wolf PA, Heard-Costa NL, Massaro JM, Beiser A, D’Agostino RB, et al. Genetic variation in white matter hyperintensity volume in the Framingham Study. Stroke. 2004;35:1609–1613. doi: 10.1161/01.STR.0000129643.77045.10. [DOI] [PubMed] [Google Scholar]
- 60.Price TR, Manolio TA, Kronmal RA, Kittner SJ, Yue NC, Robbins J, et al. Silent brain infarction on magnetic resonance imaging and neurological abnormalities in community-dwelling older adults. The Cardiovascular Health Study. CHS Collaborative Research Group. Stroke. 1997;28:1158–1164. doi: 10.1161/01.str.28.6.1158. [DOI] [PubMed] [Google Scholar]
- 61.Schmidt R, Ropele S, Enzinger C, Petrovic K, Smith S, Schmidt H, et al. White matter lesion progression, brain atrophy, and cognitive decline: the Austrian stroke prevention study. Ann Neurol. 2005;58:610–616. doi: 10.1002/ana.20630. [DOI] [PubMed] [Google Scholar]
- 62.Vermeer SE, Longstreth WT, Jr, Koudstaal PJ. Silent brain infarcts: a systematic review. Lancet Neurol. 2007;6:611–619. doi: 10.1016/S1474-4422(07)70170-9. [DOI] [PubMed] [Google Scholar]
- 63.Pathological correlates of late-onset dementia in a multicentre, community-based population in England and Wales Neuropathology Group of the Medical Research Council Cognitive Function and Ageing Study (MRC CFAS) Lancet. 2001;357:169–175. doi: 10.1016/s0140-6736(00)03589-3. [DOI] [PubMed] [Google Scholar]
- 64.Manschot SM, Brands AM, van der Grond J, Kessels RP, Algra A, Kappelle LJ, et al. Brain magnetic resonance imaging correlates of impaired cognition in patients with type 2 diabetes. Diabetes. 2006;55:1106–1113. doi: 10.2337/diabetes.55.04.06.db05-1323. [DOI] [PubMed] [Google Scholar]
- 65.Vermeer SE, Prins ND, den Heijer T, Hofman A, Koudstaal PJ, Breteler MM. Silent brain infarcts and the risk of dementia and cognitive decline. N Engl J Med. 2003;348:1215–1222. doi: 10.1056/NEJMoa022066. [DOI] [PubMed] [Google Scholar]
- 66.Gouw AA, van der Flier WM, Fazekas F, van Straaten EC, Pantoni L, Poggesi A, et al. Progression of white matter hyperintensities and incidence of new lacunes over a 3-year period: the Leukoaraiosis and Disability study. Stroke. 2008;39:1414–1420. doi: 10.1161/STROKEAHA.107.498535. [DOI] [PubMed] [Google Scholar]
- 67.Norrving B. Long-term prognosis after lacunar infarction. Lancet Neurol. 2003;2:238–245. doi: 10.1016/s1474-4422(03)00352-1. [DOI] [PubMed] [Google Scholar]
- 68.Sun X, Lindsay J, Monsein LH, Hill PC, Corso PJ. Silent brain injury after cardiac surgery: a review: cognitive dysfunction and magnetic resonance imaging diffusion-weighted imaging findings. J Am Coll Cardiol. 2012;60:791–797. doi: 10.1016/j.jacc.2012.02.079. [DOI] [PubMed] [Google Scholar]
- 69.Bendszus M, Stoll G. Silent cerebral ischaemia: hidden fingerprints of invasive medical procedures. Lancet Neurol. 2006;5:364–372. doi: 10.1016/S1474-4422(06)70412-4. [DOI] [PubMed] [Google Scholar]
- 70.Ishii N, Nishihara Y, Imamura T. Why do frontal lobe symptoms predominate in vascular dementia with lacunes? Neurology. 1986;36:340–345. doi: 10.1212/wnl.36.3.340. [DOI] [PubMed] [Google Scholar]
- 71.Wolfe N, Linn R, Babikian VL, Knoefel JE, Albert ML. Frontal systems impairment following multiple lacunar infarcts. Arch Neurol. 1990;47:129–132. doi: 10.1001/archneur.1990.00530020025010. [DOI] [PubMed] [Google Scholar]
- 72.Reed BR, Eberling JL, Mungas D, Weiner M, Kramer JH, Jagust WJ. Effects of white matter lesions and lacunes on cortical function. Arch Neurol. 2004;61:1545–1550. doi: 10.1001/archneur.61.10.1545. [DOI] [PubMed] [Google Scholar]
- 73.Vermeer SE, Den Heijer T, Koudstaal PJ, Oudkerk M, Hofman A, Breteler MM. Incidence and risk factors of silent brain infarcts in the population-based Rotterdam Scan Study. Stroke. 2003;34:392–396. doi: 10.1161/01.str.0000052631.98405.15. [DOI] [PubMed] [Google Scholar]
- 74.Mungas D, Harvey D, Reed BR, Jagust WJ, DeCarli C, Beckett L, et al. Longitudinal volumetric MRI change and rate of cognitive decline. Neurology. 2005;65:565–571. doi: 10.1212/01.wnl.0000172913.88973.0d. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 75.Vermeer SE, Koudstaal PJ, Oudkerk M, Hofman A, Breteler MM. Prevalence and risk factors of silent brain infarcts in the population-based Rotterdam Scan Study. Stroke. 2002;33:21–25. doi: 10.1161/hs0102.101629. [DOI] [PubMed] [Google Scholar]
- 76.De Groot JC, De Leeuw FE, Oudkerk M, Van Gijn J, Hofman A, Jolles J, et al. Periventricular cerebral white matter lesions predict rate of cognitive decline. Ann Neurol. 2002;52:335–341. doi: 10.1002/ana.10294. [DOI] [PubMed] [Google Scholar]
- 77.Wentzel C, Rockwood K, MacKnight C, Hachinski V, Hogan DB, Feldman H, et al. Progression of impairment in patients with vascular cognitive impairment without dementia. Neurology. 2001;57:714–716. doi: 10.1212/wnl.57.4.714. [DOI] [PubMed] [Google Scholar]
- 78.Norton S, Matthews FE, Barnes DE, Yaffe K, Brayne C. Potential for primary prevention of Alzheimer’s disease: an analysis of population-based data. Lancet Neurol. 2014;13:788–794. doi: 10.1016/S1474-4422(14)70136-X. [DOI] [PubMed] [Google Scholar]
- 79.Chan S, Kartha K, Yoon SS, Desmond DW, Hilal SK. Multifocal hypointense cerebral lesions on gradient-echo MR are associated with chronic hypertension. AJNR Am J Neuroradiol. 1996;17:1821–1827. [PMC free article] [PubMed] [Google Scholar]
- 80.Offenbacher H, Fazekas F, Schmidt R, Koch M, Fazekas G, Kapeller P. MR of cerebral abnormalities concomitant with primary intracerebral hematomas. AJNR Am J Neuroradiol. 1996;17:573–578. [PMC free article] [PubMed] [Google Scholar]
- 81.Greenberg SM, Finklestein SP, Schaefer PW. Petechial hemorrhages accompanying lobar hemorrhage: detection by gradient-echo MRI. Neurology. 1996;46:1751–1754. doi: 10.1212/wnl.46.6.1751. [DOI] [PubMed] [Google Scholar]
- 82.Kim BJ, Lee SH. Cerebral microbleeds: their associated factors, radiologic findings, and clinical implications. J Stroke. 2013;15:153–163. doi: 10.5853/jos.2013.15.3.153. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 83.Kinoshita T, Okudera T, Tamura H, Ogawa T, Hatazawa J. Assessment of lacunar hemorrhage associated with hypertensive stroke by echo-planar gradient-echo T2*-weighted MRI. Stroke. 2000;31:1646–1650. doi: 10.1161/01.str.31.7.1646. [DOI] [PubMed] [Google Scholar]
- 84.Tsushima Y, Aoki J, Endo K. Brain microhemorrhages detected on T2*-weighted gradient-echo MR images. AJNR Am J Neuroradiol. 2003;24:88–96. [PMC free article] [PubMed] [Google Scholar]
- 85.Cordonnier C, Al-Shahi Salman R, Wardlaw J. Spontaneous brain microbleeds: systematic review, subgroup analyses and standards for study design and reporting. Brain. 2007;130:1988–2003. doi: 10.1093/brain/awl387. [DOI] [PubMed] [Google Scholar]
- 86.Werring DJ, Coward LJ, Losseff NA, Jager HR, Brown MM. Cerebral microbleeds are common in ischemic stroke but rare in TIA. Neurology. 2005;65:1914–1918. doi: 10.1212/01.wnl.0000188874.48592.f7. [DOI] [PubMed] [Google Scholar]
- 87.Jeon SB, Kwon SU, Cho AH, Yun SC, Kim JS, Kang DW. Rapid appearance of new cerebral microbleeds after acute ischemic stroke. Neurology. 2009;73:1638–1644. doi: 10.1212/WNL.0b013e3181bd110f. [DOI] [PubMed] [Google Scholar]
- 88.Lee SH, Lee ST, Kim BJ, Park HK, Kim CK, Jung KH, et al. Dynamic temporal change of cerebral microbleeds: long-term follow-up MRI study. PLoS One. 2011;6: doi: 10.1371/journal.pone.0025930. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 89.Gregoire SM, Brown MM, Kallis C, Jager HR, Yousry TA, Werring DJ. MRI detection of new microbleeds in patients with ischemic stroke: five-year cohort follow-up study. Stroke. 2010;41:184–186. doi: 10.1161/STROKEAHA.109.568469. [DOI] [PubMed] [Google Scholar]
- 90.Jeon SB, Kang DW, Cho AH, Lee EM, Choi CG, Kwon SU, et al. Initial microbleeds at MR imaging can predict recurrent intracerebral hemorrhage. J Neurol. 2007;254:508–512. doi: 10.1007/s00415-006-0406-6. [DOI] [PubMed] [Google Scholar]
- 91.Greenberg SM, Eng JA, Ning M, Smith EE, Rosand J. Hemorrhage burden predicts recurrent intracerebral hemorrhage after lobar hemorrhage. Stroke. 2004;35:1415–1420. doi: 10.1161/01.STR.0000126807.69758.0e. [DOI] [PubMed] [Google Scholar]
- 92.Soo YO, Yang SR, Lam WW, Wong A, Fan YH, Leung HH, et al. Risk vs benefit of anti-thrombotic therapy in ischaemic stroke patients with cerebral microbleeds. J Neurol. 2008;255:1679–1686. doi: 10.1007/s00415-008-0967-7. [DOI] [PubMed] [Google Scholar]
- 93.Tanaka A, Ueno Y, Nakayama Y, Takano K, Takebayashi S. Small chronic hemorrhages and ischemic lesions in association with spontaneous intracerebral hematomas. Stroke. 1999;30:1637–1642. doi: 10.1161/01.str.30.8.1637. [DOI] [PubMed] [Google Scholar]
- 94.Lee SH, Bae HJ, Yoon BW, Kim H, Kim DE, Roh JK. Low concentration of serum total cholesterol is associated with multifocal signal loss lesions on gradient-echo magnetic resonance imaging: analysis of risk factors for multifocal signal loss lesions. Stroke. 2002;33:2845–2849. doi: 10.1161/01.str.0000036092.23649.2e. [DOI] [PubMed] [Google Scholar]
- 95.Vernooij MW, van der Lugt A, Ikram MA, Wielopolski PA, Niessen WJ, Hofman A, et al. Prevalence and risk factors of cerebral microbleeds: the Rotterdam Scan Study. Neurology. 2008;70:1208–1214. doi: 10.1212/01.wnl.0000307750.41970.d9. [DOI] [PubMed] [Google Scholar]
- 96.Reed DM. The paradox of high risk of stroke in populations with low risk of coronary heart disease. Am J Epidemiol. 1990;131:579–588. doi: 10.1093/oxfordjournals.aje.a115542. [DOI] [PubMed] [Google Scholar]
- 97.Dietrich WD, Busto R, Halley M, Valdes I. The importance of brain temperature in alterations of the blood-brain barrier following cerebral ischemia. J Neuropathol Exp Neurol. 1990;49:486–497. doi: 10.1097/00005072-199009000-00004. [DOI] [PubMed] [Google Scholar]
- 98.Hjort N, Butcher K, Davis SM, Kidwell CS, Koroshetz WJ, Rother J, et al. Magnetic resonance imaging criteria for thrombolysis in acute cerebral infarct. Stroke. 2005;36:388–397. doi: 10.1161/01.STR.0000152268.47919.be. [DOI] [PubMed] [Google Scholar]
- 99.Lee SH, Bae HJ, Kwon SJ, Kim H, Kim YH, Yoon BW, et al. Cerebral microbleeds are regionally associated with intracerebral hemorrhage. Neurology. 2004;62:72–76. doi: 10.1212/01.wnl.0000101463.50798.0d. [DOI] [PubMed] [Google Scholar]
- 100.Jeong SW, Jung KH, Chu K, Bae HJ, Lee SH, Roh JK. Clinical and radiologic differences between primary intracerebral hemorrhage with and without microbleeds on gradient-echo magnetic resonance images. Arch Neurol. 2004;61:905–909. doi: 10.1001/archneur.61.6.905. [DOI] [PubMed] [Google Scholar]
- 101.Imaizumi T, Honma T, Horita Y, Kawamura M, Kohama I, Miyata K, et al. The number of microbleeds on gradient T2*-weighted magnetic resonance image at the onset of intracerebral hemorrhage. J Stroke Cerebrovasc Dis. 2008;17:30–34. doi: 10.1016/j.jstrokecerebrovasdis.2007.11.001. [DOI] [PubMed] [Google Scholar]
- 102.Greenberg SM, O’Donnell HC, Schaefer PW, Kraft E. MRI detection of new hemorrhages: potential marker of progression in cerebral amyloid angiopathy. Neurology. 1999;53:1135–1138. doi: 10.1212/wnl.53.5.1135. [DOI] [PubMed] [Google Scholar]
- 103.Charidimou A, Kakar P, Fox Z, Werring DJ. Cerebral microbleeds and recurrent stroke risk: systematic review and meta-analysis of prospective ischemic stroke and transient ischemic attack cohorts. Stroke. 2013;44:995–1001. doi: 10.1161/STROKEAHA.111.000038. [DOI] [PubMed] [Google Scholar]
- 104.Lee SH, Heo JH, Yoon BW. Effects of microbleeds on hemorrhage development in leukoaraiosis patients. Hypertens Res. 2005;28:895–899. doi: 10.1291/hypres.28.895. [DOI] [PubMed] [Google Scholar]
- 105.Lee SH, Kim BJ, Roh JK. Silent microbleeds are associated with volume of primary intracerebral hemorrhage. Neurology. 2006;66:430–432. doi: 10.1212/01.wnl.0000196471.04165.2b. [DOI] [PubMed] [Google Scholar]
- 106.Imaizumi T, Honma T, Horita Y, Kohama I, Miyata K, Kawamura M, et al. Hematoma size in deep intracerebral hemorrhage and its correlation with dot-like hemosiderin spots on gradient echo T2*-weighted MRI. J Neuroimaging. 2006;16:236–242. doi: 10.1111/j.1552-6569.2006.00042.x. [DOI] [PubMed] [Google Scholar]
- 107.Kim BJ, Lee SH. Silent microbleeds and hemorrhagic conversion of an embolic infarction. J Clin Neurol. 2007;3:147–149. doi: 10.3988/jcn.2007.3.3.147. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 108.Kidwell CS, Saver JL, Villablanca JP, Duckwiler G, Fredieu A, Gough K, et al. Magnetic resonance imaging detection of microbleeds before thrombolysis: an emerging application. Stroke. 2002;33:95–98. doi: 10.1161/hs0102.101792. [DOI] [PubMed] [Google Scholar]
- 109.Nighoghossian N, Hermier M, Adeleine P, Blanc-Lasserre K, Derex L, Honnorat J, et al. Old microbleeds are a potential risk factor for cerebral bleeding after ischemic stroke: a gradient-echo T2*-weighted brain MRI study. Stroke. 2002;33:735–742. doi: 10.1161/hs0302.104615. [DOI] [PubMed] [Google Scholar]
- 110.Kim HS, Lee DH, Ryu CW, Lee JH, Choi CG, Kim SJ, et al. Multiple cerebral microbleeds in hyperacute ischemic stroke: impact on prevalence and severity of early hemorrhagic transformation after thrombolytic treatment. AJR Am J Roentgenol. 2006;186:1443–1449. doi: 10.2214/AJR.04.1933. [DOI] [PubMed] [Google Scholar]
- 111.Kakuda W, Thijs VN, Lansberg MG, Bammer R, Wechsler L, Kemp S, et al. Clinical importance of microbleeds in patients receiving IV thrombolysis. Neurology. 2005;65:1175–1178. doi: 10.1212/01.wnl.0000180519.27680.0f. [DOI] [PubMed] [Google Scholar]
- 112.Lee SH, Kang BS, Kim N, Roh JK. Does microbleed predict haemorrhagic transformation after acute atherothrombotic or cardioembolic stroke? J Neurol Neurosurg Psychiatry. 2008;79:913–916. doi: 10.1136/jnnp.2007.133876. [DOI] [PubMed] [Google Scholar]
- 113.Fiehler J, Albers GW, Boulanger JM, Derex L, Gass A, Hjort N, et al. Bleeding risk analysis in stroke imaging before thromboLysis (BRASIL): pooled analysis of T2*-weighted magnetic resonance imaging data from 570 patients. Stroke. 2007;38:2738–2744. doi: 10.1161/STROKEAHA.106.480848. [DOI] [PubMed] [Google Scholar]
- 114.Shoamanesh A, Kwok CS, Lim PA, Benavente OR. Postthrombolysis intracranial hemorrhage risk of cerebral microbleeds in acute stroke patients: a systematic review and meta-analysis. Int J Stroke. 2013;8:348–356. doi: 10.1111/j.1747-4949.2012.00869.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 115.Boulanger JM, Coutts SB, Eliasziw M, Gagnon AJ, Simon JE, Subramaniam S, et al. Cerebral microhemorrhages predict new disabling or fatal strokes in patients with acute ischemic stroke or transient ischemic attack. Stroke. 2006;37:911–914. doi: 10.1161/01.STR.0000204237.66466.5f. [DOI] [PubMed] [Google Scholar]
- 116.Werring DJ, Frazer DW, Coward LJ, Losseff NA, Watt H, Cipolotti L, et al. Cognitive dysfunction in patients with cerebral microbleeds on T2*-weighted gradient-echo MRI. Brain. 2004;127:2265–2275. doi: 10.1093/brain/awh253. [DOI] [PubMed] [Google Scholar]
- 117.Gregoire SM, Smith K, Jager HR, Benjamin M, Kallis C, Brown MM, et al. Cerebral microbleeds and long-term cognitive outcome: longitudinal cohort study of stroke clinic patients. Cerebrovasc Dis. 2012;33:430–435. doi: 10.1159/000336237. [DOI] [PubMed] [Google Scholar]