

Abstract
Sudden cardiac death (SCD) is progressively threatening the lives of young people throughout the world. We conducted a retrospective study of SCD cases identified among sudden death cases based on comprehensive autopsies and pathological examinations in the Center for Medicolegal Expertise of Sun Yat-Sen University to investigate the exact etiological distribution and epidemiological features of SCD. One thousand six hundred fifty-six cases were identified, and SCD accounted for 43.0% of these sudden death cases. The mean age of the SCD cases—where the data of definite ages were accessible—was 38.2 years, and the highest incidence occurred among the 31- to 40-year-old cases (25.6%). The male-to-female ratio among SCD cases was 4.3:1, and this ratio peaked in the 41- to 50-year-old group (7.7:1). The places of death were confirmed in 1411 cases, and predominantly in hospitals (46.3%) and at home (33.8%). SCD occurred throughout the year with a marginally increase in April and May. The major causes of SCD were coronary atherosclerotic disease (CAD, 41.6%), unexplained sudden death (15.1%), and myocarditis (11.8%). Our data indicated that in the age group of younger affected persons (below 35 years old), sudden unexplained death and myocarditis were much more prevalent than CAD. According to anatomical examinations of the CAD-related SCD cases, the proportion of cases with coronary artery stenosis exceeding 75% (grade IV) was 67.2%. Moreover, the percentages of higher grades of coronary atherosclerosis increased with age. Among all branches of the coronary arteries, the left anterior descending branch was the most prone to atherosclerosis; atherosclerosis was present in this branch in 95.4% of the cases with atherosclerosis. Additionally, lesions of multiple branches of the coronary artery were associated with ageing. This is the first study to report the causes of death and basic epidemiological data related to SCD in Southern China.
INTRODUCTION
Sudden cardiac death (SCD) is an unexpected natural death from cardiac causes that occurs within a short time period, generally within 1 hour from the onset of symptoms, in a person without any prior condition that appears fatal.1 SCD is responsible for nearly half of all cardiovascular deaths. The annual incidence of SCD in China is 41.8/100,000 persons,2 which is similar to the reported value of 40/100,000 persons in Asia3 and below the 50 to 100/100,000 persons reported for North America and Europe.4–7 Nevertheless, the number of SCD cases in China2 is significantly higher than the United States’ number because of China's large population.8 Moreover, SCD can occasionally be the first manifestation of coronary atherosclerotic disease (CAD). Therefore, the identification of the causes of SCD is important for SCD prevention and control. We conducted a retrospective study of 1656 SCD cases that were identified after comprehensive autopsies and pathological examinations in the Center for Medicolegal Expertise of Sun Yat-Sen University to investigate the exact etiological distribution and epidemiological features of SCD.
METHODS
Case Sources
The 1656 SCD cases were selected from 3770 sudden death cases that were identified in the Center for Medicolegal Expertise of Sun Yat-Sen University between September 1998 and August 2013. Systematic and thorough autopsies and histopathological examinations that included inspections of the cardiac conduction system were performed in all selected cases. All studies and data collection were conducted in strict accordance with ethics guidelines of the Zhongshan School of Medicine of Sun Yat-Sen University.
Inclusion Criteria
SCD refers to deaths that occur within 1 hour of the sudden loss of consciousness due to various cardiovascular diseases.9 However, it is difficult to accurately define the time from the onset of symptoms to death. In our study, deaths that occurred within 1 hour from the onset of symptoms or during sleep were included. Unwitnessed cases, in which the affected persons were considered healthy 24 hours before the event, were also included.10 Deaths due to noncardiac conditions, such as injuries, poisonings, epilepsy, acute pulmonary embolisms, and allergies, were excluded.
Statistical Methods
The statistical analyses of the 1656 SCD cases were performed with SPSS 13.0 software (SPSS, Inc, Chicago, IL). Pearson Chi-square tests or Fishers exact tests were used to analyze the differences in the proportions of the main pathogenic causes and the differences in the distributions of pathological changes in the 3 branches of coronary artery according to age and gender. The correlations of the degree of coronary stenosis with gender and age were analyzed with logistic regressions. Test results with 2-tailed values of P < 0.05 were considered statistically significant.
RESULTS
The Demographics of SCD
A total of 1656 cases were identified as SCD cases based on the inclusion criteria. SCD was the main cause of death for 43.9% of the 3770 sudden death cases followed by death due to respiratory and neurological diseases (Table 1). The mean age of the 1611 SCD cases was 38.2 years old (median age 38 years old) after the exclusion of 45 cases with unconfirmed ages. The age and gender distributions are illustrated in Figure 1. When all of the 1611 enrolled SCD cases were divided into age groups of 10 years, the age groups of the 31- to 40-year-old (412 cases, 25.6%) and 41- to 50-year-old age groups (349 cases, 21.7%) were predominant in SCD. The male-to-female ratio of SCD was 4.3:1, and this ratio peaked (7.7:1) in the 41- to 50-year-old age group followed by the 51- to 60-year-old age group (6.4:1).
TABLE 1.
Proportion of Causes in 3770 Sudden Death Cases From 1998 to 2013 by Center for Medicolegal Expertise of Sun Yat-Sen University
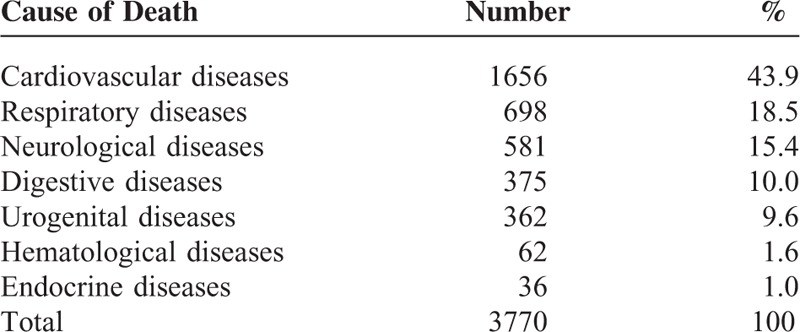
FIGURE 1.
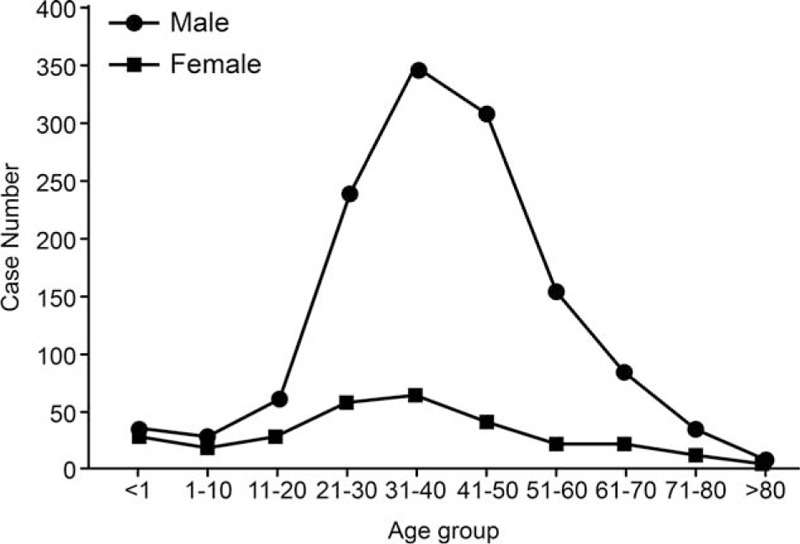
The distribution of age and gender in sudden cardiac death cases. Sudden cardiac death (SCD) cases occurred more frequently in males than females in all age groups. And both male and female SCD victims were most among the age groups of 21 to 30, 31 to 40, and 41 to 50 years old.
The Circumstances of SCD
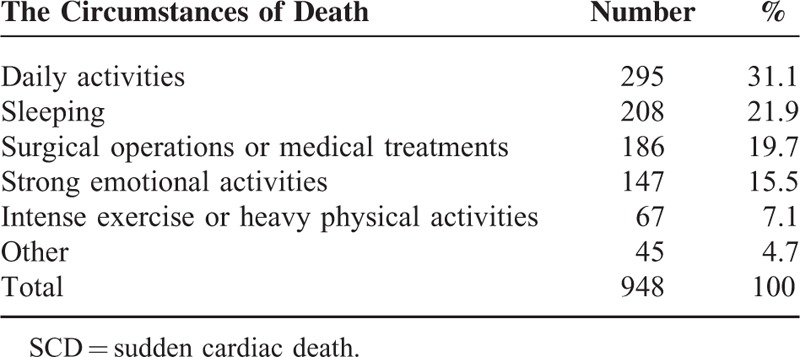
The locations of the SCD occurrences varied. After the exclusion of 245 cases due to unconfirmed occurrence locations, 46.3% of the SCD cases were found to occur in hospitals or emergency rooms, 33.8% occurred at home or in rental houses, 12.0% occurred in shopping malls, hotels, airports, and other public places, 4.2% occurred in prisons or detention houses, and the remaining 3.7% occurred on trains, in factories or in other locations. The circumstances of death in the selected SCD cases (excluding 708 cases with unidentified conditions) are presented in Table 2. Furthermore, 295 cases (31.1%) happened during daily activities, 208 cases (21.9%) occurred while sleeping, 186 cases (19.7%) took placed while undergoing surgical operations or medical treatments, 147 cases (15.5%) occurred during quarrels or other strongly emotional activities, 67 cases (7.1%) happened after intense exercise or heavy physical activities, and 45 cases (4.7%) took placed while drinking, tumbling, following slight injuries, etc.
TABLE 2.
The Circumstances of Death in SCD
The Monthly Distribution of SCD
SCD was most prevalent in the months through April to July, and least prevalent in January and February (Figure 2).
FIGURE 2.
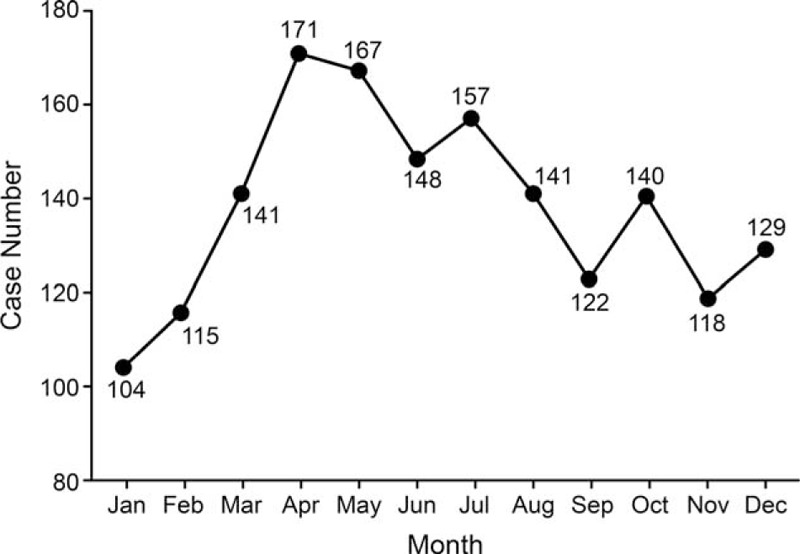
The monthly distribution of sudden cardiac death cases. Sudden cardiac death was the most prevalent in the months of April, May, June, and July, and the least prevalent in January and February.
The Incidence of SCD
Based on comprehensive postmortem examinations, the forensic pathological diagnoses of the 1656 SCD cases are illustrated in Table 3 and Figure 3. CAD was the leading cause of SCD followed by sudden unexplained death (SUD) and myocarditis. Moreover, the SUD cases included 194 cases of sudden manhood death syndrome (SMDS), 24 cases of sudden infant death syndrome (SIDS), and 33 cases of SUD during physical activities. The cases of cardiac conduction system disease primarily involved fatty infiltration or fibrosis of the cardiac conduction system, whereas the cases of aortic root aneurysm ruptured involved only pericardial tamponades due to ruptured aneurysms. The cases of cardiomyopathy included 40 cases of hypertrophic cardiomyopathy, 10 cases of dilated cardiomyopathy, 6 cases of restrictive cardiomyopathy, 1 case of unclassified cardiomyopathy, and 20 cases of arrhythmogenic right ventricular cardiomyopathy. Additionally, the 4 cases with specific diagnoses presented in Table 3 and Figure 3 were classified as cases of other diseases that included 1 case each of Keshan disease, Marfan syndrome, hyperthyroid heart disease, and pulmonary heart disease.
TABLE 3.
Forensic Pathological Diagnoses of 1656 SCD Cases
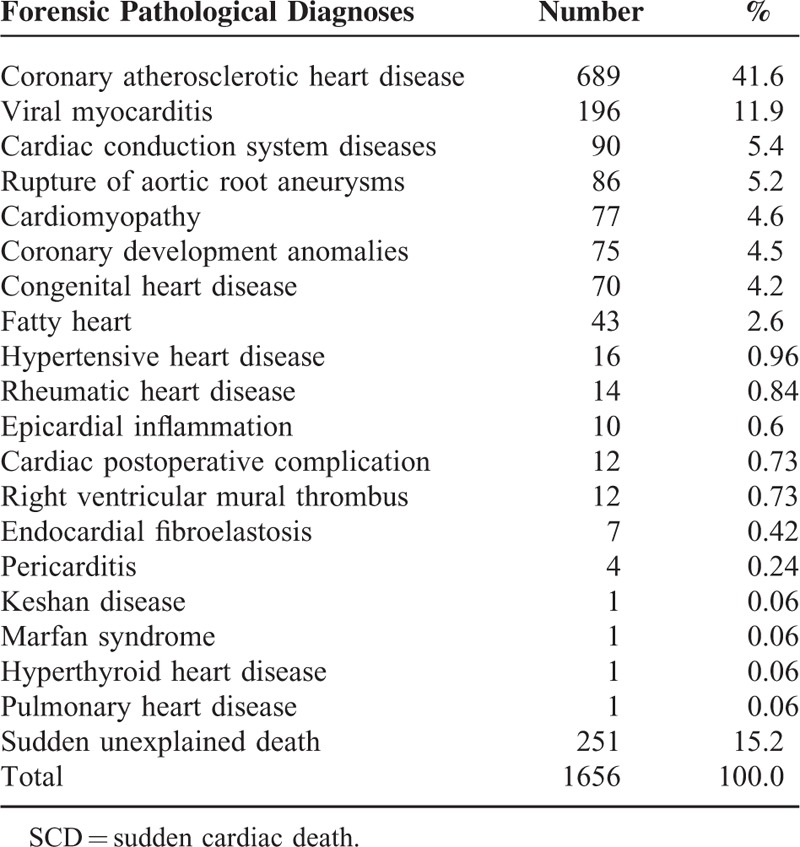
FIGURE 3.
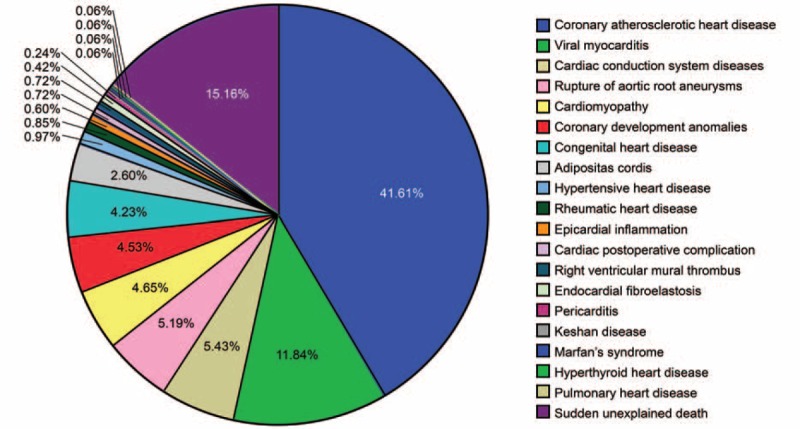
Forensic pathological diagnoses of 1656 SCD cases presented as percentages. Coronary atherosclerotic heart disease, sudden unexplained death, and viral myocarditis were the 3 leading causes of SCD accounting for 41.61%, 15.16%, and 11.84% of the cases, respectively.
The 1611 age-confirmed SCD cases were divided into 3 age groups: younger than 35 years, 35 to 55 years old, and older than 55 years. The pathological distributions differed between all 3 age groups are illustrated in Table 4 and Figure 4. The results of Pearson Chi-square test shows statistical significance of pathogenic distribution between 3 different age groups (the total χ2 = 529.704, P < 0.01). The χ2 values between the age group of 35 to 55 years old and that of younger than 35 years old, the age group of older than 55 years old and that of 35 to 55 years old, and the age group of older than 55 years old and that of younger than 35 years old are 310.548, 97.797, 355.701, respectively (all P < 0.01). CAD cases were primarily observed in the 35- to 55-year-old and over 55-year-old groups, whereas myocarditis and SUD occurred in much higher proportions than CAD in the group younger than 35 years old.
TABLE 4.
The Pathogenic Distribution of SCD in Different Age Groups

FIGURE 4.
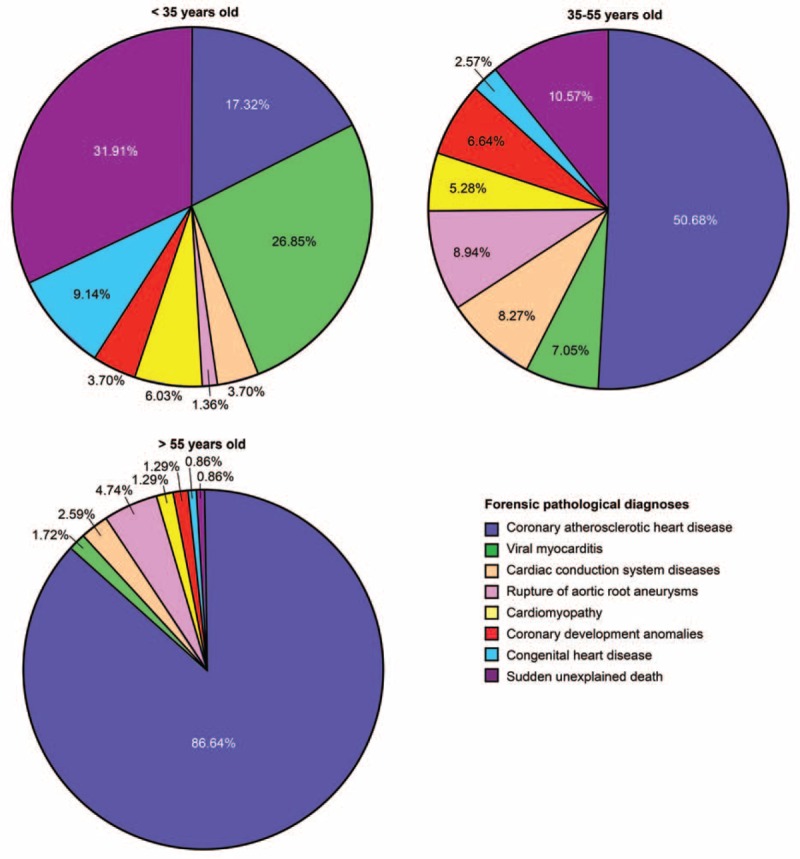
The etiological distributions of sudden cardiac death in the different age groups. Coronary atherosclerotic heart disease was the leading cause death in the 35- to 55 and >55-year-old age groups, whereas sudden unexplained death, viral myocarditis, and coronary atherosclerotic heart disease were the leading causes in the <35-year-old group.
The Pathology of Coronary Atherosclerotic Disease
Further analysis of the CAD cases was necessary because nearly half of the SCD cases were likely imputable to CAD. The mean age of the 664 CAD sudden death victims (excluding 25 cases with unconfirmed ages) was 49.2 years old, and the median age was 48 years old. There were only 2 cases of CAD in which the victims were under 20 years old (14 and 18 years old). The age group of the 35- to 55-year-old had the highest percentage (56.3%) of all CAD cases. The male-to-female ratio of CAD cases was 8.3:1. Following anatomical examinations of the 680 CAD sudden deaths (excluding 9 cases that lacked of details), the distribution of different degrees of coronary artery stenosis was calculated and is illustrated below. The extents of coronary artery stenosis in 17 cases (2.5%) were below 25% (grade I lesions), between 26% and 50% (grade II lesions) in 92 cases (13.5%), between 51% and 75% (grade III lesions) in 183 cases (26.9%), and greater than 76% (grade IV lesions) in 388 cases (57.1%). Regarding the 3 main branches of the coronary artery, 626 cases (95.4%) exhibited atherosclerosis in the left anterior descending artery (LAD), 312 cases (47.6%) exhibited atherosclerosis in the right coronary artery (RCA), and 177 cases (27.0%) exhibited atherosclerosis in the left circumflex artery (LCX). Furthermore, single-branch atherosclerosis occurred in 308 cases (47.0%), 2 branches were involved in 241 cases (36.7%), and all 3 branches were involved in 107 cases (16.3%) after the exclusion of 33 cases that lacked sufficient detail (Table 5).
TABLE 5.
Atherosclerotic Pathological Changes of the 3 Branches of Coronary Artery

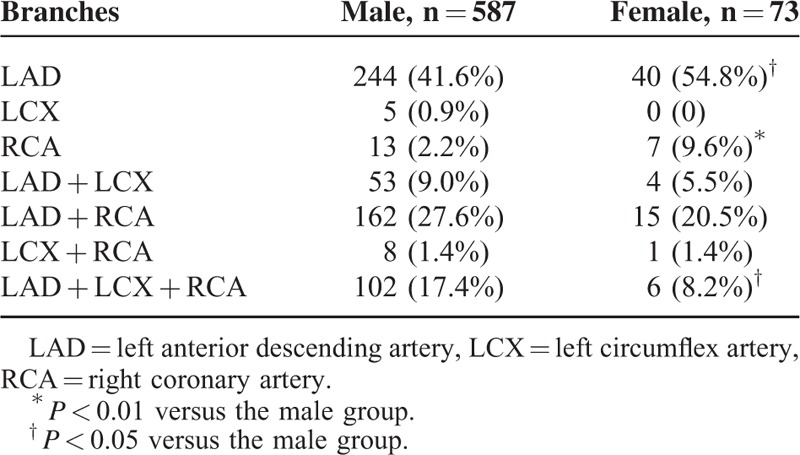
The general atherosclerosis situations of the 3 branches were calculated and are illustrated in Table 5. The cases were divided into the following 7 types: Type LAD/LCX/RCA (ie, disease involving a single artery); Types (LAD + LCX), (LAD + RCA), and (LCX + RCA) (ie, diseases involving 2 arteries); and Type (LAD + LCX + RCA) (ie, disease involving all 3 arteries). The differences in the atherosclerotic pathological distributions of the 3 branches between the different age and gender groups were analyzed, and the results are presented in Tables 6 and 7, respectively. The Pearson Chi-square test results show statistical significance of pathogenic distribution of the 3 branches between 3 different age groups (the total χ2 = 38.312, P < 0.01). The significant differences of this distribution were also observed between different gender groups (the total χ2 = 20.391, P < 0.05). The χ2 values between the age group of 35 to 55 years old and that of younger than 35 years old, the age group of older than 55 years old and that of younger than 35 years old are 23.098 (P < 0.05), 33.836 (P < 0.01), respectively. In all 3 age groups and both gender groups of the coronary atherosclerosis cases, the LAD was the most common site.
TABLE 6.
Atherosclerotic Pathological Distribution of the 3 Branches of Coronary Artery Between Different Age Groups
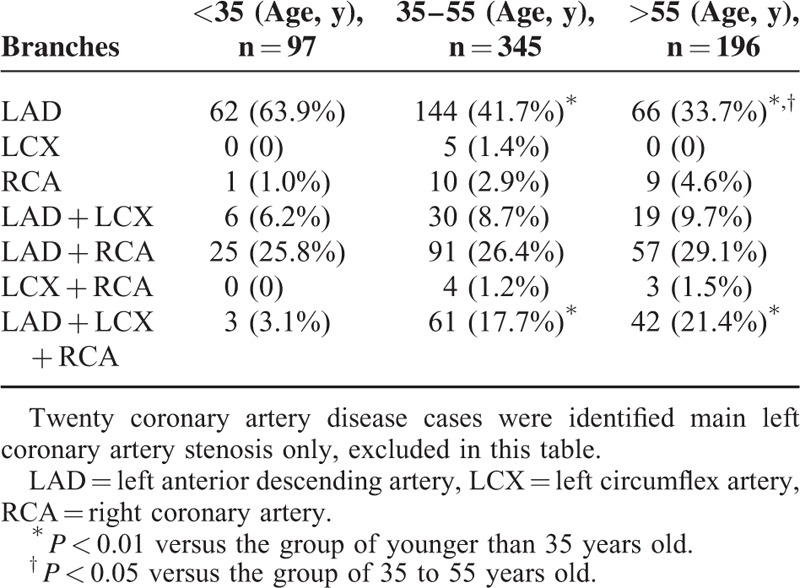
TABLE 7.
Atherosclerotic Pathological Distribution of the 3 Branches of Coronary Artery Between the Gender Groups
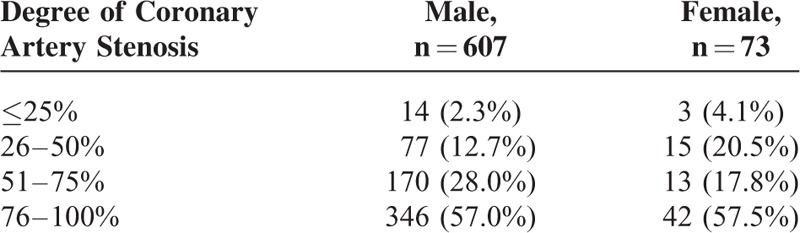
The degrees of coronary atherosclerosis in the different age and gender groups are quantified in Tables 8 and 9. In all 3 age groups and both gender groups, the fourth degree of coronary atherosclerosis (76–100%) was prevalent. Nevertheless, Chi-square tests revealed no significance differences in the distributions of the degree of atherosclerosis between the 3 age groups (total χ2 = 11.238, P > 0.05) or 2 gender groups (total χ2 = 6.341, P > 0.05).
TABLE 8.
Degree of Coronary Artery Stenosis Between Different Age Groups
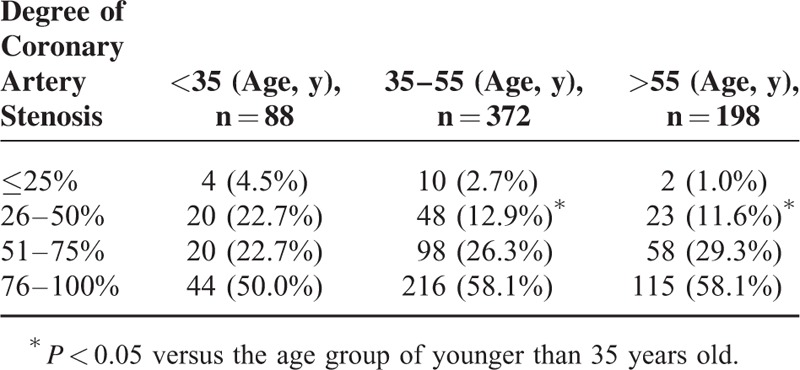
TABLE 9.
Degree of Coronary Artery Stenosis Between the Gender Groups
Furthermore, among all 1656 SCD cases, there were 67 cases that occurred after sporting or heavy physical activities, which resulted in an incidence of 4.05%. Sixty-two (92.54%) victims of physical activity-related SCD suffered from coronary atherosclerosis, and the degrees of coronary stenosis in 58 (86.57%) of the victims exceeded 50%. The victims were all elderly people in the age between 70 and 89 years. Forty-three of these subjects were male and 19 were female.
DISCUSSION
This is the first study to report the etiological distribution and basic epidemiology data of SCD cases in Southern China from the perspective of forensic identification. In the present study, the mean age of the SCD victims in Southern China was 38.2 years old, which is slightly younger than the 43.8 years old that was reported in a similar study performed by Wang group of 553 SCD cases in China from 1978 to 2008.11 This difference is probably related to differences in case selection (the youngest victim in our cases was 1 year old, whereas the victims in Wang study were all older than 18 years). In terms of gender, the number of male SCD cases was 4.3-fold greater than the number of female cases, and the greatest difference in the male-to-female ratio of 7.7 was observed in the 41- to 50-year-old age group. The gender differences were probably related to the intensive pressures of life and work experienced by males, particularly middle-aged males with multiple roles in life who suffer from work-related pressure due to fierce social competition and the family pressures of supporting parents and raising children. Moreover, the greater autopsy rate of males in China, particularly young males, also contributed to the decreased mean age and high male-to-female ratio.
Further statistical analyses of the times of SCD revealed that fewer cases suffered SCD during the winter, particularly in January and February. In contrast, other studies have reported a higher frequency of SCD in the winter compared with other seasons that potentially result from the common actions of the external environment and the endogenous biological rhythms of the human body.12,13 Additionally, many migrant workers come to Guangdong Province, and the main part goes home during the Spring Festival, which probably contributed to the lower proportions of SCD cases observed in January and February in the present study.
The present study indicated that CAD was the primary cause of SCD and accounted for 41.6% of the SCD cases. This value is lower than the 80% that has been reported in the United States1 and the 93.5% that has been reported in Great Britain.14 Studies by American researchers have indicated that the incidences of SCD differ according to race and that the Asian-American and Afro-American population exhibit the lowest and highest incidences, respectively.15 The proportion of CAD cases among the SCD cases reported here is also lower than the data from Wang study (50.3%).11 This difference is probably related to the inclusion of SCD cases younger than 18 years because this proportion increased to 45.6% when these young cases were excluded. The present study also revealed CAD proportions in the different age groups that were similar to those previously reported.1,11,14,15 Specifically observed were rates of 13.5%, 53.1%, and 81.0% in those younger than 35 years, 35- to 55-year-olds, and those older than 55 years, respectively, whereas Wang observed rates of 10.4%, 59.0%, and 83.0% in 18- to 34-, 35- to 54-, and 55- to 80-year-old groups, respectively.11 The incidence of CAD-related SCD increased with age.
We also found that rather than CAD, SUD, and myocarditis were more prevalent among the younger SCD victims. SUD accounted for 15.2% of the SCDs across all age groups and 24.9% of the SCDs among those younger than 35 years old; this latter finding is consistent with a Danish study that reported a rate of 29.0% among a 1- to 35-year-old group.16 However, the pathogeneses remain undetermined, and pathogenic diagnoses are urgently needed for the development and exploration of molecular pathological diagnostics. Our group was screened for mutations in genes related to cardiac ion channel diseases (ie, SCN5A, RYR2, KCNQ1, and KCNH2) to detect the relevance of mutations in these genes to SUD. Moreover, the proportion of cases of myocarditis was 11.8% among all SCD cases, and this proportion was 20.9% among the younger than 35-year-old group. This latter value is lower than the 34.7% among the 18- to 35-year-old group reported in Wang study in China and much higher than the 10% that has been reported in Italy.17 The reason for the higher incidence of sudden death due to myocarditis in China might involve subclinical infections of the myocardium and the higher proportion of focal myocarditis among Chinese youths.11,18
Further statistical analyses of the CAD cases revealed that the proportions of CAD-related SCD cases increased with increasing coronary artery stenosis severity in all 3 age groups (Figure 5). Moreover, the percentages of higher grades of coronary atherosclerosis increased with age. Regarding the three main branches of the coronary artery, the LAD was much more prone to atherosclerosis (626 cases, 95.4%) than the LCX and RCA, which is consistent with research conducted in foreign countries.19–21 Regarding the numbers of involved coronary arteries in the CAD cases, a single-branch involvement (308 cases, 47.0%) was more common than 2-(241 cases, 36.7%) and 3-branch involvement (107 cases, 16.3%). Moreover, multiple-branch coronary artery involvement increased with age (Figure 6). Together, these findings are consistent with the concept that age is a significant risk factor for coronary atherosclerosis, which has been revealed in many studies.22,23
FIGURE 5.
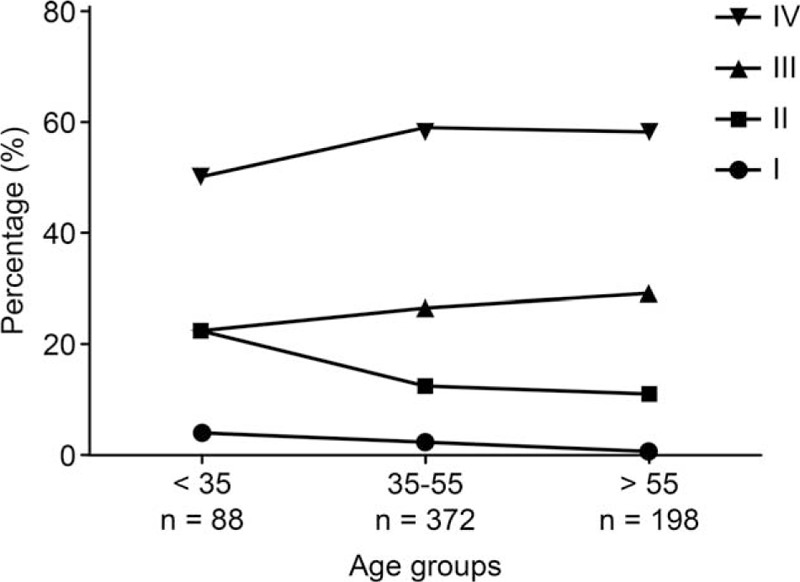
Frequencies (%) of coronary artery stenosis grades I–IV in the 3 age groups. The percentages of higher grades of coronary atherosclerosis increased with age.
FIGURE 6.
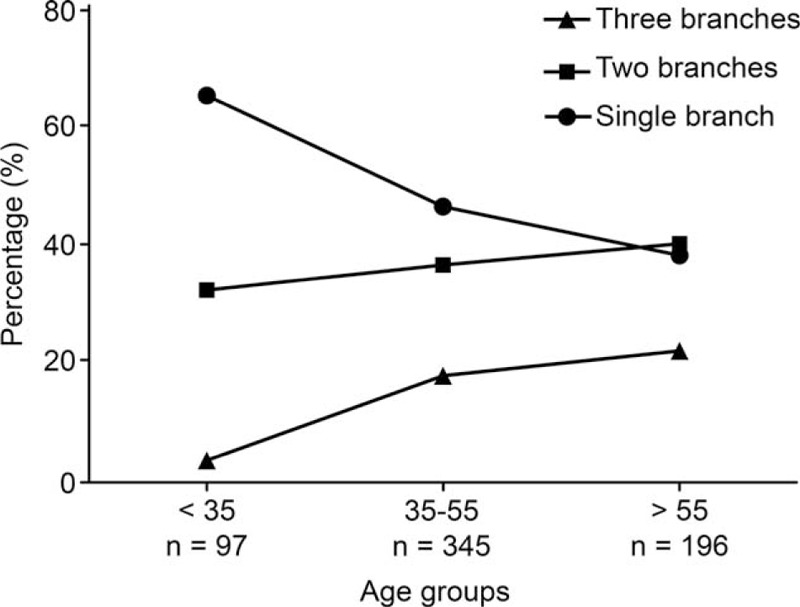
Frequencies (%) of the numbers of coronary artery branches involved in CAD in the 3 age groups. Multiple-branches coronary artery lesions increased with age.
Additionally, the incidence of SCD following exercise or heavy physical activities was relatively high; these victims were all elderly people, and most of them suffered from coronary heart disease. This situation was more common among males than females. During exercise or heavy physical activities, the oxygen and blood demands of the myocardium acutely increase while the blood flow in the coronary arteries is relatively deficient. When there is a pathological basis of coronary atherosclerosis, coronary blood flow deficiency becomes more obvious and may result in myocardial ischemia or ischemic arrhythmia and eventually lead to SCD. As Leischik et al24 noted, there are a variety of potential causes of exercise-related SCD, and these causes vary widely with a person's age. Further recommendations for preparticipation screening for sport are under discussion.25
CONCLUSION
Our retrospective study of 1656 SCD cases in Southern China indicated that the leading cause of SCD was CAD, whereas in the younger victims (below 35 years old), SUD and myocarditis were much more prevalent than CAD. Our study also demonstrated that the LAD was the artery branch that was primarily involved in CAD-related SCD and that age is a significant risk factor for CAD.
This epidemiological investigation of SCD based on the identification of the causes of death enabled us to obtained basic epidemiological data regarding SCD in Southern China. With this database of SCD cases, we will explore the risk factors, histopathological features, and molecular genetic information related to sudden death in greater depth to provide a scientific basis for the clinical prevention and treatment of SCD and a risk stratification for SCD.
Footnotes
Abbreviations: CAD = coronary atherosclerotic disease, LAD = left anterior descending artery, LCX = left circumflex artery, RCA = right coronary artery, SCD = sudden cardiac death, SIDS = sudden infant death syndrome, SMDS = sudden manhood death syndrome, SUD = sudden unexplained death.
This study was supported by grants 81430046 (the State Key Program), 81172901, and 81373238 from the National Natural Science Foundation of China, grant 11ykpy04 from the Fundamental Research Funds for the Central Universities, and grant S2012010009045 from the Guangdong Natural Science Foundation.
QW, LZ, JZ, and QZ contributed equally to this work.
The authors have no funding and conflicts of interest to disclose.
REFERENCES
- 1.Zipes DP, Wellens HJ. Sudden cardiac death. Circulation 1998; 98:2334–2351. [DOI] [PubMed] [Google Scholar]
- 2.Hua W, Zhang LF, Wu YF, et al. Incidence of sudden cardiac death in China: analysis of 4 regional populations. J Am Coll Cardiol 2009; 54:1110–1118. [DOI] [PubMed] [Google Scholar]
- 3.Murakoshi N, Aonuma K. Epidemiology of arrhythmias and sudden cardiac death in Asia. Circ J 2013; 77:2419–2431. [DOI] [PubMed] [Google Scholar]
- 4.Byrne R, Constant O, Smyth Y, et al. Multiple source surveillance incidence and aetiology of out-of-hospital sudden cardiac death in a rural population in the West of Ireland. Eur Heart J 2008; 29:1418–1423. [DOI] [PubMed] [Google Scholar]
- 5.Chugh SS, Jui J, Gunson K, et al. Current burden of sudden cardiac death: multiple source surveillance versus retrospective death certificate-based review in a large U.S. community. J Am Coll Cardiol 2004; 44:1268–1275. [DOI] [PubMed] [Google Scholar]
- 6.de Vreede-Swagemakers JJ, Gorgels AP, Dubois-Arbouw WI, et al. Out-of-hospital cardiac arrest in the 1990's: a population-based study in the Maastricht area on incidence, characteristics and survival. J Am Coll Cardiol 1997; 30:1500–1505. [DOI] [PubMed] [Google Scholar]
- 7.Vaillancourt C, Stiell IG. Canadian Cardiovascular Outcomes Research Team. Cardiac arrest care and emergency medical services in Canada. Can J Cardiol 2004; 20:1081–1090. [PubMed] [Google Scholar]
- 8.Zipes DP, Camm AJ, Borggrefe M, et al. ACC/AHA/ESC 2006 Guidelines for Management of Patients With Ventricular Arrhythmias and the Prevention of Sudden Cardiac Death: a report of the American College of Cardiology/American Heart Association Task Force and the European Society of Cardiology Committee for Practice Guidelines (writing committee to develop Guidelines for Management of Patients With Ventricular Arrhythmias and the Prevention of Sudden Cardiac Death): developed in collaboration with the European Heart Rhythm Association and the Heart Rhythm Society. Circulation 2006; 114:e385–e484. [DOI] [PubMed] [Google Scholar]
- 9.Abhilash SP, Namboodiri N. Sudden cardiac death—historical perspectives. Indian Heart J 2014; 66 Suppl. 1:S4–S9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Pilmer CM, Kirsh JA, Hildebrandt D, et al. Sudden cardiac death in children and adolescents between 1 and 19 years of age. Heart Rhythm 2014; 11:239–245. [DOI] [PubMed] [Google Scholar]
- 11.Wang H, Yao Q, Zhu S, et al. The autopsy study of 553 cases of sudden cardiac death in Chinese adults. Heart Vessels 2014; 29:486–495. [DOI] [PubMed] [Google Scholar]
- 12.Pasqualetti P, Colantonio D, Casale R, et al. [The chronobiology of sudden cardiac death. The evidence for a circadian, circaseptimanal and circannual periodicity in its incidence] (In Italian). Minerva Med 1990; 81:391–398. [PubMed] [Google Scholar]
- 13.Messner T, Lundberg V. Trends in sudden cardiac death in the northern Sweden MONICA area 1985–99. J Intern Med 2003; 253:320–328. [DOI] [PubMed] [Google Scholar]
- 14.Moore MJ, Glover BM, McCann CJ, et al. Demographic and temporal trends in out of hospital sudden cardiac death in Belfast. Heart 2006; 92:311–315. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Zheng ZJ, Croft JB, Giles WH, et al. Sudden cardiac death in the United States, 1989 to 1998. Circulation 2001; 104:2158–2163. [DOI] [PubMed] [Google Scholar]
- 16.Winkel BG, Holst AG, Theilade J, et al. Nationwide study of sudden cardiac death in persons aged 1–35 years. Eur Heart J 2011; 32:983–990. [DOI] [PubMed] [Google Scholar]
- 17.Basso C, Calabrese F, Corrado D, et al. Postmortem diagnosis in sudden cardiac death victims: macroscopic, microscopic and molecular findings. Cardiovasc Res 2001; 50:290–300. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Basso C, Burke M, Fornes P, et al. Guidelines for autopsy investigation of sudden cardiac death. Virchows Arch 2008; 452:11–18. [DOI] [PubMed] [Google Scholar]
- 19.Bhanvadia VM, Desai NJ, Agarwal NM. Study of coronary atherosclerosis by modified American Heart Association Classification of Atherosclerosis—an autopsy study. J Clin Diagn Res 2013; 7:2494–2497. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Thej MJ, Kalyani R, Kiran J. Atherosclerosis in coronary artery and aorta in a semi-urban population by applying modified American Heart Association classification of atherosclerosis: an autopsy study. J Cardiovasc Dis Res 2012; 3:265–271. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Sudha ML, Sundaram S, Purushothaman KR, et al. Coronary atherosclerosis in sudden cardiac death: an autopsy study. Indian J Pathol Microbiol 2009; 52:486–489. [DOI] [PubMed] [Google Scholar]
- 22.McGill HC, Jr, McMahan CA, Zieske AW, et al. Association of Coronary Heart Disease Risk Factors with microscopic qualities of coronary atherosclerosis in youth. Circulation 2000; 102:374–379. [DOI] [PubMed] [Google Scholar]
- 23.Nakashima Y, Kiyohara Y, Doi Y, et al. Risk factors for coronary atherosclerosis in a general Japanese population: the Hisayama study. Pathol Res Pract 2009; 205:700–708. [DOI] [PubMed] [Google Scholar]
- 24.Leischik R. Endurance sport and cardiac injury. Kardiol Pol 2014; 72:587–597. [DOI] [PubMed] [Google Scholar]
- 25.Leischik R, Dworrak B, Foshag P, et al. Pre-participation and follow-up screening of athletes for endurance sport. J Clin Med Res 2015; 7:385–392. [DOI] [PMC free article] [PubMed] [Google Scholar]