

Epilepsy genetics is complex and involves a multitude of different candidate genes with diverse mechanisms, varying modes of inheritance, and often a broad range of phenotypes for single genes (1). Patients and families frequently request genetic testing to better understand the basis of their disease, obtain a better understanding of potential risks to future offspring, and often with the hope to personalize treatment based on the genetic finding (2). Although a genetic diagnosis has a direct treatment implication only in a small number of cases, identifying a genetic cause may help avoid unnecessary testing and offer an explanation to patients and families (3, 4). There are also risks of testing including incurring substantial patient cost, patient fear of discrimination, and obtaining variants of uncertain significance that may be confusing for physicians and families (2, 5, 6).
Given these complexities and the accelerating pace of discovery in epilepsy genetics, it has become increasing challenging to understand the proper application of genetic testing in epilepsy. Although there are reviews and proposed algorithms detailing genetic testing options in epilepsy, no formalized guidelines exist to date (5, 7–9). An understanding of the current perceptions and experiences with genetic testing in epilepsy among neurologists may be instrumental in identifying knowledge gaps and barriers to testing—ultimately improving epilepsy care.
This Quantitative Practical Use-Driven Learning Survey in epilepsy (Q-PULSE) of the medical directors of leading U.S. epilepsy centers was conducted to investigate the varying practices and beliefs among pediatric and adult neurologists in the utilization of epilepsy genetic testing.
Survey Results
A total of 109 panelists responded. Of the respondents, 21 (19.3%) treated mostly pediatric patients, 83 (76.1%) treated mostly adult patients, and 5 (4.6%) treated an equal mix of pediatrics and adults. The responses of those who treated an equal mix of adult and pediatric patients did not dramatically differ from the other groups. Statistical analysis used Fisher Exact Test when appropriate.
The following case scenario was presented: “An 18-year-old man has global developmental delay and a history of infantile spasms, which led to Lennox-Gastaut syndrome. An MRI shows some enlargement of the right ventricle but no other findings, and the exam is nonfocal. The seizures are drug resistant. Metabolic testing was negative. Would you order genetic testing?”
Physicians caring for mostly adult patients were significantly less likely to order genetic testing than were physicians caring for mostly pediatric patients (33% vs 80%, p = 0.003) (Figure 1).
FIGURE 1.
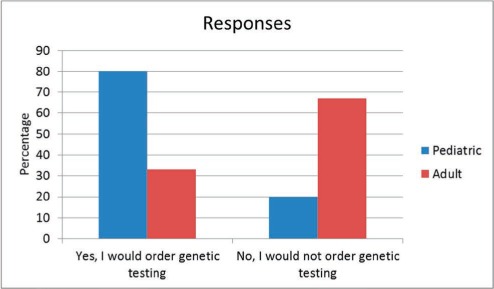
Case scenario: Would you order genetic testing?
Most adult neurologists and pediatric neurologists—78% and 95%, respectively—had ordered genetic testing within the last 2 years; 76% of pediatric neurologists and no adult neurologists had ordered more than 20 tests during this time frame (p = < 0.001). Pediatric neurologists were more likely than adult neurologists to have ever found genetic testing useful in patient care (95% vs 70%, p = 0.03).
Some other results were informative but did not reach statistical significance:
Among all respondents, the most common genetic testing modality ordered was a gene panel, which was ordered by 84% of respondents, followed by single gene testing (45%), genome-wide arrays (36%), karyotypes (28%), whole exome sequencing (27%), and whole genome sequencing (6%).
Seventy-five percent of pediatric and 51% of adult neurologists have had a patient request genetic testing. The majority of pediatric and adult neurologists (96.7% and 87.6%, respectively) had access to a genetics consultant service or genetic counselor, or were capable of providing the counseling themselves.
Respondents were also asked their opinion on this statement: “Every level 4 epilepsy center must have expertise using genetic testing in epilepsy and interpreting results.” The majority of pediatric epileptologists completely agreed (75%), while the view was shared only by a minority of the adult epileptologists (19.8%). Ninety percent of pediatric and 80% of adult neurologists agreed at least in principle, although a plurality believed that centers might not have the necessary resources to devote to this problem.
Among all respondents, the two most common perceived barriers to ordering genetic testing were related to cost: potentially too expensive for the patient (89%) and pre-approval is often denied by insurance (65%). The third most common identified barrier was that genetic testing is seldom useful in clinical care (40%).
Discussion
When a case could reasonably present to either a pediatric or adult practice for care, adult neurologists were significantly less likely to order genetic testing than were those caring for mostly pediatric patients (p = 0.003). This difference might be explained by our finding that adult neurologists seldom found genetic testing useful in the care of patients in contrast to pediatric neurologists (p = 0.03). Consistent with this theory is our finding that pediatric neurologists were more likely to have ordered a large number of genetic tests (p < 0.001). One possible explanation for these results is that the most severely affected genetic epilepsy patients are identified at a younger age, so pediatric neurologists are more likely to have obtained genetic testing results that proved useful. While it had been our subjective impression that there is a difference in perception of the usefulness of genetic testing between pediatric and adult epileptologists, we did not expect the difference to be so profound.
Despite a more negative attitude toward genetic testing, more than 80% of adult respondents agreed, at least in principle, that every level 4 epilepsy center should have expertise using genetic testing in epilepsy and interpreting the results, even though a large fraction felt that centers may not have the necessary resources. Participants consistently identified the main barriers to genetic testing as cost to the patient, insurance barriers, and low clinical utility.
In a prior survey, only 20% of neurologists had a patient request genetic testing in the last 6 months (10). In our survey, 50% of adult neurologists and 75% of pediatric neurologists had at least one patient ask for genetic testing in the last 2 years. These low values might reflect a lack of awareness in the epilepsy population about the use of genetic testing.
Genetics is inexorably transforming epilepsy practice and becoming standard in epilepsy care. While knowledge gaps likely exist among providers, the main barriers to epilepsy genetic testing in the United States are the potential for incurring high bills to patients, a stifling insurance approval processes, and the relatively low yield of genetic testing in the adult care setting.
Footnotes
Editor's Note: Authors have a Conflict of Interest disclosure which is posted under the Supplemental Materials (204.1KB, docx) link.
References
- 1.Helbig I, Scheffer IE, Mulley JC, Berkovic SF. Navigating the channels and beyond: Unravelling the genetics of the epilepsies. Lancet Neurol. 2008;7:231–245. doi: 10.1016/S1474-4422(08)70039-5. [DOI] [PubMed] [Google Scholar]
- 2.Okeke JO, Tangel VE, Sorge ST, Hesdorffer DC, Winawer MR, Goldsmith J, Phelan JC, Chung WK, Shostak S, Ottman R. Genetic testing preferences in families containing multiple individuals with epilepsy. Epilepsia. 2014;55:1705–1713. doi: 10.1111/epi.12810. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Berkovic SF. Genetics of epilepsy in clinical practice. Epilepsy Curr. 2015;15:192–196. doi: 10.5698/1535-7511-15.4.192. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Olsen HE, Poduri A, Pearl PL. Genetic forms of epilepsies and other paroxysmal disorders. Seminars in Neur. 2014;34:266–279. doi: 10.1055/s-0034-1386765. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Poduri A, Sheidley BR, Shostak S et al. Genetic testing in the epilepsies—Developments and dilemmas. Nat Rev Neurol. 2014;10:293–299. doi: 10.1038/nrneurol.2014.60. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Achkar CM, Olsen HE, Poduri A, Pearl PL. The genetics of the epilepsies. Curr Neur Neurosci Rep. 2015;15:39. doi: 10.1007/s11910-015-0559-8. [DOI] [PubMed] [Google Scholar]
- 7.Ream MA, Patel AD. Obtaining genetic testing in pediatric epilepsy. Epilepsia. 2015;56:1505–1514. doi: 10.1111/epi.13122. [DOI] [PubMed] [Google Scholar]
- 8.Mefford HC. Clinical genetic testing in epilepsy. Epilepsy Curr. 2015;15:197–201. doi: 10.5698/1535-7511-15.4.197. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Scheffer IE. Genetic testing in epilepsy: What should you be doing. Epilepsy Curr. 2011;11:107–111. doi: 10.5698/1535-7511-11.4.107. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Salm M, Abbate K, Appelbaum P, Ottman R, Chung W, Marder K, Leu CS, Alcalay R, Goldman J, Curtis AM, Leech C, Taber KJ, Klitzman R. Use of genetic tests among neurologists and psychiatrists: Knowledge, attitudes, behaviors, and needs for training. J Genet Counsel. 2014;23:156–153. doi: 10.1007/s10897-013-9624-0. [DOI] [PMC free article] [PubMed] [Google Scholar]