

Abstract
Background:
Some studies suggest that hormonal contraception, pregnancy, and/or breastfeeding may influence rates of HIV disease progression.
Methods:
From 1994 to 2012, HIV discordant couples recruited at couples' voluntary HIV counseling and testing centers in Lusaka were followed 3-monthly. Multivariate survival analyses explored associations between time-varying contraception, pregnancy, and breastfeeding and 2 outcomes among HIV-positive women: (1) time to death and (2) time to antiretroviral treatment (ART) initiation.
Results:
Among 1656 female seropositive, male seronegative couples followed for 3359 person-years (PY), 224 women died [6.7/100 PY; 95% confidence interval (CI): 5.8 to 7.6]. After 2003, 290 women initiated ART (14.5/100 PY; 95% CI: 12.9 to 16.2). In a multivariate model of time to death, hormonal implant [adjusted hazard ratio (aHR) = 0.30; 95% CI: 0.10 to 0.98] and injectable (aHR = 0.59; 95% CI: 0.36 to 0.97) were significantly protective relative to nonhormonal method use, whereas oral contraceptive pill (OCP) use was not (aHR = 1.08; 95% CI: 0.74 to 1.57) controlling for baseline HIV disease stage, time-varying pregnancy, time-varying breastfeeding, and year of enrollment. In a multivariate model of time-to-ART initiation, implant was significantly protective (aHR = 0.54; 95% CI: 0.31 to 0.95), whereas OCP (aHR = 0.70; 95% CI: 0.44 to 1.10) and injectable (aHR = 0.85; 95% CI: 0.55 to 1.32) were not relative to nonhormonal method use controlling for variables above, woman's age, and literacy. Pregnancy was not significantly associated with death (aHR = 1.07; 95% CI: 0.68 to 1.66) or ART initiation (aHR = 1.24; 95% CI: 0.83 to 1.86), whereas breastfeeding was protective for death (aHR = 0.34; 95% CI: 0.19 to 0.62) and ART initiation (aHR = 0.49; 95% CI: 0.29 to 0.85).
Conclusions:
Hormonal implants and injectables significantly predicted lower mortality; implants were protective for ART initiation. OCPs and pregnancy were not associated with death or ART initiation, whereas breastfeeding was protective for both. Findings from this 18-year cohort study suggest that (1) HIV-positive women desiring pregnancy can be counseled to do so and breastfeed and (2) all effective contraceptive methods, including injectables and implants, should be promoted to prevent unintended pregnancy.
Key Words: breastfeeding, HIV disease progression, hormonal contraception, longitudinal cohort, pregnancy, Zambia
INTRODUCTION
Hormonal contraceptive method use is associated with decreased maternal-child mortality, reduced unintended pregnancy, and improved reproductive autonomy for women.1 Hormonal methods are also a mainstay of Prong II (prevention of unintended pregnancy) of the WHO's 4-pronged prevention of mother-to-child transmission (PMTCT) strategy.2 However, conflicting evidence exists as to whether hormonal method use increases HIV disease progression in infected women.3 A systematic review by Phillips et al4 found that 10 of 11 observational studies showed no increased risk for HIV disease progression for hormonal versus nonhormonal method users. However, a randomized controlled trial (RCT) in which Zambian women were randomized to receive either the copper intrauterine device (IUD) or hormonal contraception [depot medroxyprogesterone acetate (DMPA) injectables or oral contraceptive pills (OCPs)] found in an intention-to-treat analysis that OCP use and DMPA use were associated with (1) CD4 <200 cells per cubic millimeter or antiretroviral treatment (ART) initiation and (2) death or CD4 <200 cells per cubic millimeter or ART initiation compared with women using the copper IUD.5 Although an RCT, this study suffered from high rates of method stopping and switching.3 Current WHO Medical Eligibility Criteria recommendations, developed after reviewing this literature, place no restriction on use of hormonal contraceptive methods by women based on HIV status.3
The alternative to contraception is often pregnancy, and the relationship between pregnancy and associated hormonal changes and HIV disease progression has been studied for over 2 decades6,7 also with mixed findings. A recent systematic review and meta-analysis7 synthesized findings from several observational studies. Of 4 studies meeting inclusion criteria,8–11 pregnancy was marginally though not significantly associated with low CD4 among ART-naive women; the only study from an Africa cohort (Uganda) also did not find an association between pregnancy and time to CD4 <200 cells per cubic millimeter.10 Conversely, in 5 studies meeting inclusion criteria,12–15 pregnancy was significantly associated with HIV-related death; the only study from an African cohort (Rwanda) did not find an association with time-to-HIV–related death.12 Three other recent observational studies (with the primary objective of assessing the relationship between hormonal contraception and HIV disease progression) also reported measures of effect for time-varying pregnancy with conflicting findings. A study of 2269 chronically HIV-infected women from 7 East and Southern African countries found that pregnancy was significantly associated with first occurrence of CD4 <200 cells per cubic millimeter, ART initiation, or nontraumatic death.16 Conversely, another study among 303 recently HIV-infected women from Uganda and Zimbabwe found no significant association between pregnancy and time-to-clinical AIDS, death, or ART initiation.17 Finally, a study among 625 Ugandan women also found no significant association between pregnancy and time to AIDS or death.18
Finally, as pregnancy is often followed by breastfeeding, which is also associated with hormonal changes, researchers have undertaken studies of the relationship between breastfeeding and HIV disease progression again with mixed findings. An RCT in Kenya showed that mortality among women randomized to breastfeeding increased 3-fold,19 whereas studies in Tanzania, Zambia, South Africa, Zimbabwe, and Malawi have not observed associations between breastfeeding and death or decreased CD4 count.20–24
With a growing population of HIV-infected women in sub-Saharan Africa, evaluating factors that may predict disease progression is imperative to improve health outcomes. In this study, we identify factors associated with HIV disease progression in HIV-positive women in Zambia and specifically evaluate the impact of contraceptive use, pregnancy, and breastfeeding on disease progression.
METHODS
Ethics
Approvals by the Office for Human Research Protections–registered Institutional Review Boards at Emory University and in Zambia were obtained. All participating couples provided written informed consent.
Participants
Study recruitment, eligibility, follow-up, and data collection methods used by the Rwanda Zambia HIV Research Group (RZHRG) have been reported previously.25–28 Briefly, we recruited cohabiting couples in Lusaka, Zambia, through community promotions29–31 to receive couples' voluntary HIV counseling and testing services.32 HIV discordant couples were enrolled in 3-monthly longitudinal follow-up between 1994 and 2012. This analysis considers only couples in which the woman was HIV positive at enrollment; women were censored if the couple separated, their male partner seroconverted, or if either partner was lost to follow-up. HIV testing using rapid serologic tests was conducted at baseline (and 3-monthly visits for negative partners).33 The primary objective of this cohort study was to determine predictors of heterosexual HIV-1 transmission, and censoring criteria were selected based on that primary objective.
Exposures of Interest
Time-varying contraceptive method, pregnancy, and breastfeeding were the exposures of interest. Contraceptive methods were provided at the research site at each 3-monthly follow-up visit34,35 categorized as: condoms alone (OCPs were typically combination estrogen and progesterone; progesterone-only pills were prescribed to breastfeeding women until children were 6 months old), DMPA injectables (150 mg intramuscular dosage), copper IUD, contraceptive implant (Norplant or Jadelle levonorgestrel implant), or permanent methods (hysterectomy, tubal ligation, or vasectomy). Contraceptive methods were categorized as implant, injectable, or OCP versus nonhormonal contraception control (including condoms alone, copper IUD, or permanent methods). Time-varying pregnancy was determined by pregnancy test or visual confirmation by a nurse counselor. Time-varying breastfeeding included intervals in which women self-reported breastfeeding and all intervals that were up to 6 months postpartum without infant death.
Covariates
As previously reported, baseline and time-varying demographic, family planning, behavioral, sexual history, and clinical data are collected from each couple.28 In this analysis, we considered covariates known or hypothesized to be related to disease progression, including baseline measures of women's year of study enrollment, age (continuous and categorical measures considered), monthly household income (US Dollar equivalent, adjusted for exchange rate, continuous and categorical measures considered), literacy in Nyanja (the most common local language), and stage of HIV. We used the Modified Kigali combined HIV staging system, which incorporates clinical stage with erythrocyte sedimentation rate, hematocrit, and body mass index.32,36
Outcomes
Primary outcomes of interest are time to (1) all-cause death among female partners (>90% of which were HIV related) or (2) ART initiation (not including short course for PMTCT) among female partners. Since ART was not readily available in Zambia before 2003 and the first ART initiation occurred in November of 2003, analysis of ART initiation is restricted to November 2003 to 2012. Date of death among women was reported by male study partners or other family members. Time of ART initiation was obtained by self-report or plasma ART levels. Since we censor at ART initiation, no ART users are included in the time-to-death analysis.
Data Analyses
Analyses were conducted with SAS v9.4 (Cary, NC). Outcome rates were calculated as the number of outcomes per woman-year of follow-up, stratified by time-varying contraceptive method exposure, pregnancy, and breastfeeding. Event rates were compared with reference groups using univariate Cox models. Outcome rates were also calculated stratified by other demographic and clinical covariates. Associations between these covariates and the outcomes of interest were evaluated using univariate Cox models. Crude hazard ratios (HRs), 95% confidence intervals (CIs), and associated P values are presented.
Multivariate Cox models accounting for repeated observations estimated the effect of time-varying contraceptive methods and covariates on the outcomes of interest. Covariates included in the models were those that were significantly associated with the outcome of interest in univariate analyses using Bonferroni corrected P values (P = 0.006) and which changed point estimates for any exposures of interest by ±10%. Multicollinearity was assessed; if any 2 variables were collinear, the variable with the weakest association with the outcome was removed. The proportional hazard assumption was confirmed for time-independent covariates.
Sensitivity Analyses
Sensitivity analyses explored the effects of running models using censoring during pregnancy intervals and, for time to death, we additionally ran a model including women's baseline viral load (VL), which was a significant predictor of death but only available from 1999 onward. We also built multivariate models assessing the effect of progestin-only and combined OCPs separately, and removing IUDs from the reference group. Finally, we varied the assumed duration of breastfeeding from 4-month to 1-year postpartum.
RESULTS
Outcome Rates Overall and by Contraceptive Methods, Unadjusted
Among 1656 M-F+ couples followed for 3359 person-years (PY), 224 women died (6.7/100 PY; 95% CI: 5.8–7.6) (Table 1). Compared with women using nonhormonal methods, women using implants (HR = 0.32, P = 0.051) and injectables (HR = 0.60, P = 0.040) experienced lower rates of death, whereas women using OCPs did not (HR = 1.19, P = 0.340). Compared with women who were not pregnant, women who were currently pregnant did not experience significantly increased rates of death (HR = 1.32, P = 0.211), whereas women who were currently breastfeeding (HR = 0.32, P < 0.001) experienced lower rates of death.
TABLE 1.
Disease Progression Outcome Rates and Univariate Associations With Time-Varying Contraceptive Methods, Pregnancy Status, and Breastfeeding (N = 1656 HIV-Positive Women in Discordant Relationships, Lusaka, Zambia)
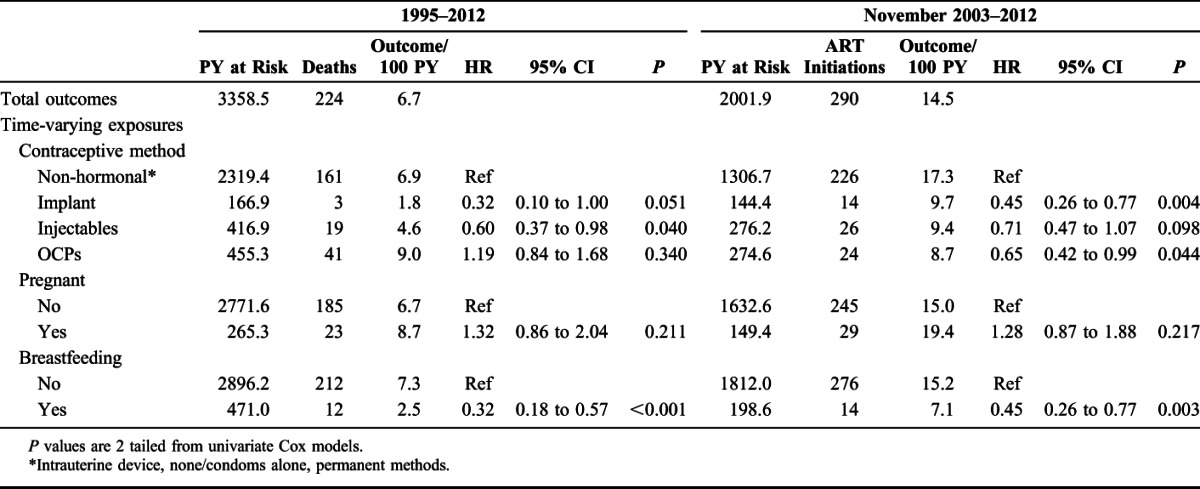
The first ART initiation occurred in November 2003. Between November 2003 and 2012, 290 women initiated ART (14.5/100 PY; 95% CI: 12.9 to 16.2). Compared with women using nonhormonal methods, women using implants (HR = 0.45, P = 0.004) and OCPs (HR = 0.65, P = 0.044) experienced significantly lower rates of ART initiation in univariate analyses, as did women using injectables though this was not significant (HR = 0.71, P = 0.098). Compared with women who were not pregnant, women who were currently pregnant experienced non–statistically significantly increased rates of ART initiation (HR = 1.28, P = 0.217), whereas women who were currently breastfeeding (HR = 0.45, P = 0.003) experienced significantly lower rates of ART initiation.
Outcome Rates by Covariates, Unadjusted
Covariates significantly (Bonferroni P < 0.006) associated with time to death included enrolling in the study at any time before 2007 (HR between 2.12 and 3.02) versus after 2007, and having stage III (HR = 2.15) or stage IV (HR = 2.91) HIV disease versus stage I at enrollment, and increasing VL (HR = 2.43) (Table 2).
TABLE 2.
Disease Progression Outcome Rates and Univariate Associations With Baseline Covariates (N = 1656 HIV-Positive Women in Discordant Relationships, Lusaka, Zambia)
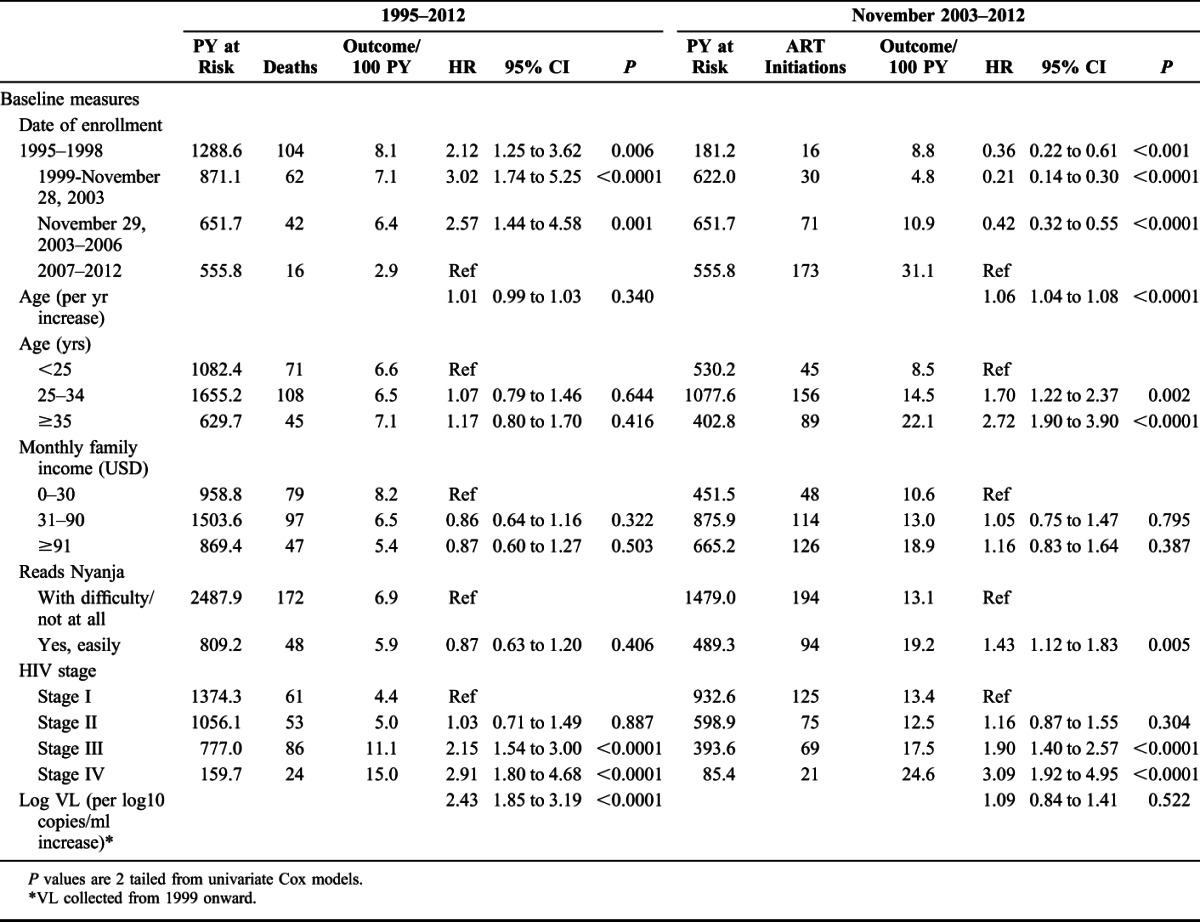
Covariates associated (Bonferroni P < 0.006) with time-to-ART initiation included enrolling in the study before 2007 (HR between 0.21 and 0.42) versus any time after 2007, increasing woman's age (HR = 1.06), being literate in Nyanja (HR = 1.43), and having stage III (HR = 1.90) or stage IV (HR = 3.09) HIV disease versus stage I at enrollment.
Multivariate Models and Sensitivity Analyses: Time-to-Death
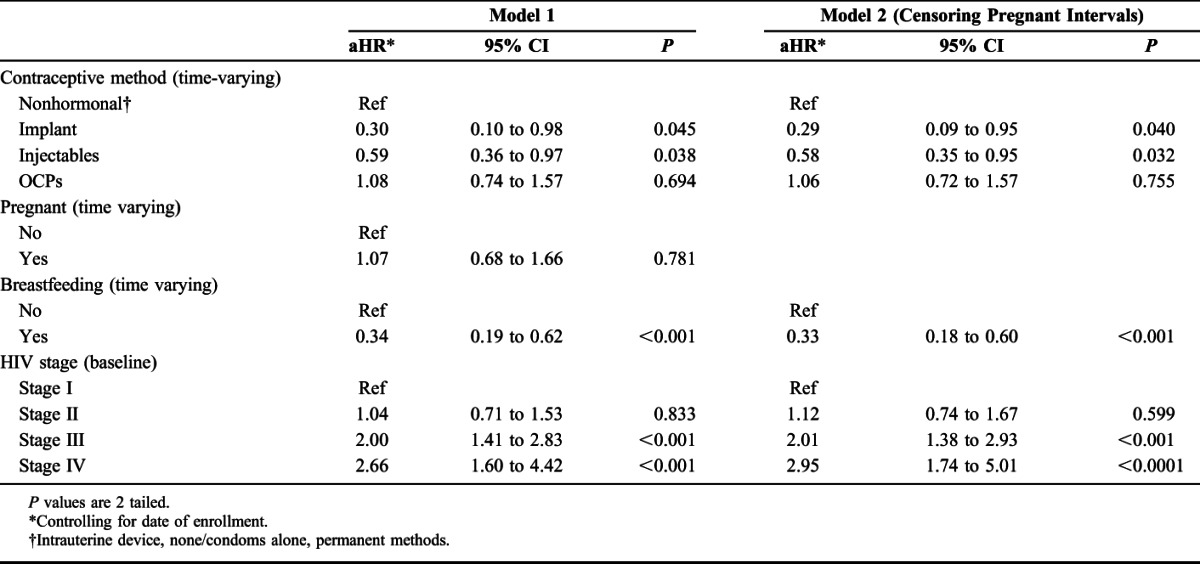
In a multivariate model of time to death (model 1), hormonal implant [adjusted hazard ratio (aHR) = 0.30] and injectable (aHR = 0.59) were significantly protective relative to nonhormonal method use, whereas OCP use was not [aHR = 1.08, not significant (NS)] controlling for baseline HIV disease stage, time-varying pregnancy, breastfeeding, and year of study enrollment (Table 3). Pregnancy was not significantly associated with death (aHR = 1.07, NS), whereas breastfeeding significantly delayed death (aHR = 0.34) in multivariate analyses. In the model censoring for pregnancy intervals (model 2), implant use (P = 0.040), injectable use (P = 0.032), and breastfeeding (P < 0.001) reached significance for their protective effects on time to death. In both models 1 and 2, having stage III (aHR = 2.00–2.01) or stage IV (aHR = 2.66–2.95) HIV disease versus stage I at enrollment was significantly associated with time to death.
TABLE 3.
Multivariate Cox Models of Time to Death (N = 1656 HIV-Positive Women in Discordant Relationships, Lusaka, Zambia, 1995–2012)
In a multivariate model additionally controlling for baseline log VL, though VL was significantly associated with time to death (aHR = 2.66; 95% CI: 1.99 to 3.53, P < 0.0001), the addition of VL did not change the point estimates for the exposures of interests by ±10% and was therefore not considered a confounder of the associations of interest. Running models among those with VL measures (collected after 1999) but without the VL covariate showed similar results (data not shown).
Multivariate Models and Sensitivity Analyses: Time-to-ART Initiation
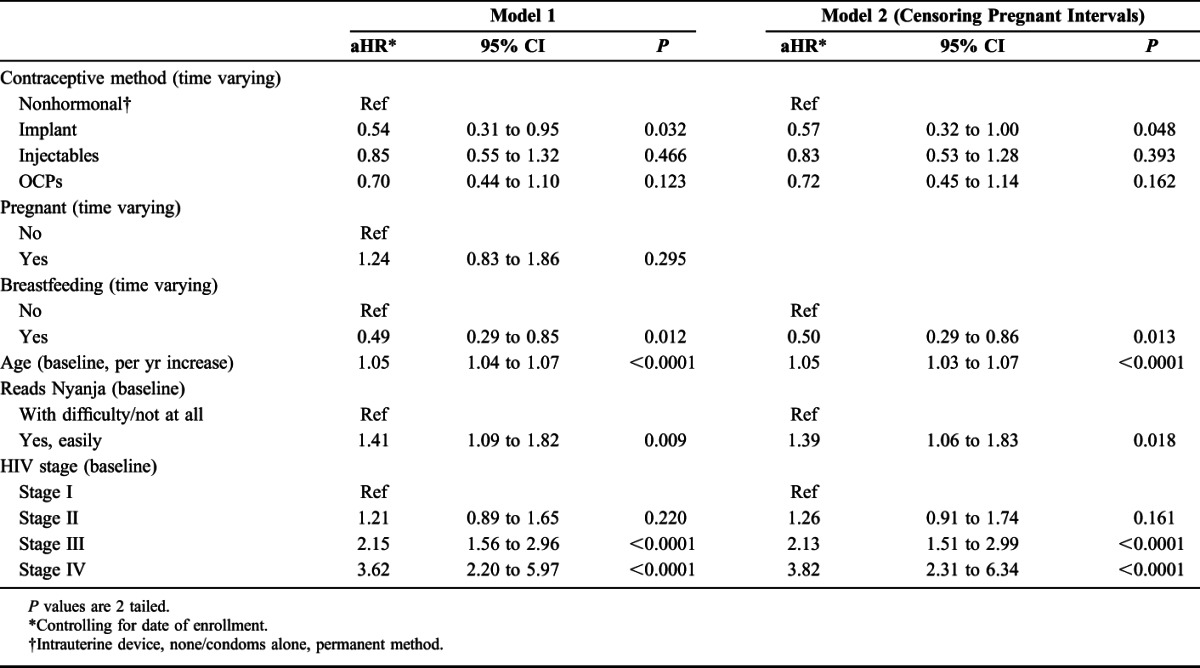
In a multivariate model of time-to-ART initiation post-November 2003 (model 1), implant was significantly protective (aHR = 0.54), whereas OCP (aHR = 0.70, NS) and injectable (aHR = 0.85, NS) use were not significantly protective relative to nonhormonal method use controlling for woman's baseline age, literacy, HIV disease stage, time-varying pregnancy, time-varying breastfeeding, and year of study enrollment. Pregnancy was not significantly associated with ART initiation (aHR = 1.24, NS), whereas breastfeeding was significantly protective for ART initiation (aHR = 0.49) in multivariate analyses (Table 4). In the model censoring for pregnancy intervals (model 2), implant use (P = 0.048) and breastfeeding (P = 0.013) reached significance for their protective effects on time to ART initiation, whereas injectable (P = 0.393) and OCP use (P = 0.162) were non–significantly protective. In both models 1 and 2, increasing age (aHR = 1.05), being literate in Nyanja (aHR = 1.39–1.41), and having stage III (aHR = 2.13–2.15) or stage IV (aHR = 3.62–3.82) HIV disease versus stage I at enrollment were significantly associated with time to ART initiation.
TABLE 4.
Multivariate Cox Models of Time to ART Initiation (N = 1656 HIV-Positive Women in Discordant Relationships, Lusaka, Zambia, November 2003–2012)
Sensitivity Analyses (Data Not Shown)
Multivariate models assessing the effect of progestin-only and combined OCPs separately did not change our findings related to OCPs (ie, the point estimates for OCPs in multivariate models did not change in magnitude by ±10%, direction, or statistical significance). For example, in multivariate model 1 of time-to-ART initiation, the HR for combined OCPs was 0.69; 95% CI: 0.42 to 1.12 and for progestin-only OCPs was 0.78; 95% CI: 0.19 to 3.20. Excluding IUDs from the referent group leads to similar findings (ie, the point estimates for contraceptive methods in multivariate models did not change in magnitude by ±10%, direction, or statistical significance). We do not have the power to look at IUD users individually (only 1.5% of all intervals were IUD using intervals). Assuming breastfeeding of 4 months up to 1 year did not change our findings (ie, the point estimates for breastfeeding in multivariate models did not change in magnitude by ±10%, direction, or statistical significance).
DISCUSSION
In this prospective cohort of HIV-positive Zambian women in discordant couples, we found injectable hormonal contraception and hormonal implant associated with significantly lower mortality rates when adjusted for pregnancy, breastfeeding, and demographic and clinical covariates. We did not observe this association with OCP. In an analogous analysis of time-to-ART initiation, only the protective effect of the hormonal implant was statistically significant. Time-dependent measures of pregnancy were not significantly associated with either death or ART initiation, whereas breastfeeding was significantly protective for both.
The majority of published observational studies have found no increased HIV disease progression among women using hormonal methods.4 Our study shows a protective effect of hormonal implant and injectable contraception. These findings are similar to Allen et al,35 which found a borderline protective effect for time varying injectable (P = 0.09) and OCP (P = 0.08) use and time-to-HIV–related death in Rwandan women in multivariate models. Similarly, Heffron et al16 found that rates of disease progression (using a composite outcome of CD4 decline to less than 200 cells per cubic millimeter, initiation of ART, or death) were significantly lower for women using hormonal contraceptives versus nonhormonal contraceptive methods in a prospective cohort of women from 7 East and southern African countries.
We also did not find that time-varying measures of pregnancy were significantly associated with either HIV disease progression outcome, similar to findings from several meta-analyses and individual studies, which do not indicate a deleterious effect of pregnancy on HIV disease progression6,7,17,18,35,37 and in contrast to the relatively few studies that have seen this association.7,16 The finding that breastfeeding was strongly associated with a delay in both death and ART initiation was somewhat surprising given an RCT in Kenya, which showed that mortality among women randomized to breastfeeding was 3 times higher than the corresponding rate among bottle-feeding women.19 However, subsequent studies in Tanzania, Zambia, South Africa, Zimbabwe, and Malawi have not seen an association between breastfeeding and death or decreased CD4 count.20–24 We may be observing the result of the “healthy pregnant woman” bias, since women who are able to get pregnant (and then breastfeed a child who survives) are healthier.
The association between women who experience pregnancy or breastfeeding (not necessarily those who are currently pregnant or breastfeeding) is also of interest. In the time-to-ART initiation analysis, cumulative previous pregnancies and associated breastfeeding reported at enrollment were collinear with age. We retained age in the model (which was a significant risk factor); replacing age with cumulative previous pregnancy gave a nonsignificant protective effect for that variable (aHR = 0.99; 95% CI: 0.94 to 1.05, P = 0.75). Neither age nor cumulative previous pregnancies and associated breastfeeding were associated with death in univariate or multivariate analyses.
Although the findings of the START trial suggest that ART should now be offered at the time of diagnosis,38 we feel that use of ART initiation as a proxy outcome for disease progression remains relevant given that ART rationing is a current front-line reality in many locations.39,40 Despite the lowering of initiation criteria by WHO over the years, a review of 56 articles from 2002 to 2013 showed that “CD4 counts at ART presentation in sub-Saharan Africa have not increased over the past 10 years.41 However, it is possible that changes in national guidelines may lead to increased median CD4 counts at ART initiation, as it has in Rwanda42 and if economic conditions improve so that initiation on diagnosis becomes a reality, ART as a proxy outcome for disease progression may become less relevant.
It was not surprising that VL and HIV staging were predictive of mortality and that HIV staging was predictive of ART initiation. The staging system combining clinical and laboratory criteria used here has been shown to reflect a range of HIV-related outcomes including death and have prognostic significance among HIV-positive women in Rwanda32 and Zambia.36 This further supports the use of the modified Kigali combined staging system (using hematocrit and erythrocyte sedimentation rate in lieu of CD4, including pulmonary tuberculosis in stage 4, and substituting low body mass index for weight loss, among other less impactful adaptations) for predicting HIV-related disease outcomes among adults in circumstances that do not allow systematic CD4 screening.
Our findings also suggest that illiteracy may be a barrier to ART initiation. Similarly, recent systematic review using data from South Africa suggests that people with low education attainment have lower access to ART.43 In our study, although staff provided ART referrals and assisted patients in accessing ART services in government clinics to the extent possible if obstacles were reported, low literacy may have impeded patient willingness or their ability to follow through on referrals and prescriptions. This hypothesized role of socioeconomic disparities in health warrants further exploration among Zambian women.
Our study has limitations, including that we began following women after they were already HIV infected and therefore cannot measure time to event since HIV infection; however, we do not expect any bias introduced by not knowing the duration of infection to be differential. Similarly, we did not follow women from the time they initiated contraception before study start, but again we do not expect this bias to be differential—and in fact, most women (77.2%) were not using any method of contraception at baseline. Deaths were reported by family members, who provided verbal autopsies, and many ART initiations were self-reported, but again we do not expect any information bias to be differential by the exposure of interest. Women who chose certain contraceptive methods may be different from those who chose others by unmeasured confounders. In addition, as we censor couples at seroconversion of the HIV-negative male partner, we may be limiting our follow-up of more vulnerable woman PY. Loss to follow-up among M-F+ couples, which we have reported in our cohorts to be associated with residence far from the clinic, younger age, and younger women's age at first intercourse, no income, fewer lifetime sex partners, no history of genital abnormalities in women, and male partners having a recent concurrent partner26 may also limit the generalizability of our findings. Finally, 3-monthly study visits included assessments of HIV disease and referrals to government clinics where ART was available, so our clients were likely to initiate ART sooner than people in the general population also limiting generalizability.
Our study has several strengths. We are able to reliably assess contraceptive method use and rates of stopping/switching by providing the methods at the research site every 3 months; this overcomes limitations with self-reported method use commonly reported in other studies. As the outcomes of interest were also assessed often, at least 3-monthly, we are able to more accurately assess when outcomes occurred. We also have relatively more power than previous studies to disaggregate the effects of implant use (73% power for the time-to-death analysis and 55% power for the ART initiation analysis for implant use) on disease progression. Finally, we measure and control for several fixed and time-varying covariates associated with disease progression.
CONCLUSIONS
Hormonal contraceptive implants and injectable contraception were associated with significantly lower mortality rates among HIV-infected women. Hormonal implants were also protective for ART initiation. OCPs and pregnancy were not associated with death or ART initiation, whereas breastfeeding was protective for both. These findings add to a relatively small, inconclusive literature and suggest that HIV-positive women desiring pregnancy can be counseled to do so and to breastfeed without concerns about deleterious health related to pregnancy or breastfeeding.
For HIV-positive women who wish to delay fertility, our findings support the conclusion that hormonal implants and injectables can be used without concerns about deleterious health effects and with possible health benefits. Given high rates of unintended pregnancy and associated maternal-child mortality among HIV-positive women in sub-Saharan Africa, as well as the cost-effectiveness of prevention of unintended pregnancy for PMTCT strategy,44 we recommend increasing the contraceptive method mix for all women with and at risk of HIV with a focus on long-acting reversible contraceptive (LARC) methods, both hormonal and nonhormonal, which are highly effective and may be associated with better health outcomes among HIV-positive women but remain inaccessible in much of Africa. Further study is needed of the copper IUD, a nonhormonal LARC method that is highly cost-effective in preventing unplanned pregnancy and may have health benefits for HIV-positive women. Finally, as we have shown previously that contraception uptake increases, especially LARC methods, after couples' HIV and family planning counseling with fertility intention assessment,45 we recommend that HIV and family planning services in Africa be integrated with a focus on couples.
Footnotes
Supported by the National Institute of Child Health and Development (NICHD R01 HD40125) and National Institute of Mental Health (NIMH R01 66767); with support from the AIDS International Training and Research Program Fogarty International Center (D43 TW001042); the Emory Center for AIDS Research (P30 AI050409); National Institute of Allergy and Infectious Diseases (NIAID R01 AI51231; NIAID R01 AI040951; NIAID R01 AI023980; NIAID R01 AI64060; NIAID R37 AI51231); and the International AIDS Vaccine Initiative. This study was made possible by the generous support of the American people through the United States Agency for International Development (USAID).
The authors have no conflicts of interest to disclose.
The contents do not necessarily reflect the views of USAID or the United States Government. The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the article.
REFERENCES
- 1.World Health Organization. Family Planning. Fact Sheet No 351. 2013. Available at: http://www.who.int/mediacentre/factsheets/fs351/en/. Accessed February 27, 2015. [Google Scholar]
- 2.World Health Organization, UNICEF, UNFPA, UNAIDS. Towards the Elimination of Mother-to-child Transmission of HIV. Report of a WHO Technical Consultation 2010. Available at: http://whqlibdoc.who.int/publications/2011/9789241501910_eng.pdf?ua=1. Accessed February 27, 2015. [Google Scholar]
- 3.World Health Organization. Hormonal Contraceptive Methods for Women at High Risk of HIV and Living with HIV. Guidance Statement 2014. Available at: http://apps.who.int/iris/bitstream/10665/128537/1/WHO_RHR_14.24_eng.pdf. Accessed February 27, 2015. [PubMed] [Google Scholar]
- 4.Phillips SJ, Curtis KM, Polis CB. Effect of hormonal contraceptive methods on HIV disease progression: a systematic review. AIDS. 2013;27:787–794. [DOI] [PubMed] [Google Scholar]
- 5.Stringer EM, Levy J, Sinkala M, et al. HIV disease progression by hormonal contraceptive method: secondary analysis of a randomized trial. AIDS. 2009;23:1377–1382. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.French R, Brocklehurst P. The effect of pregnancy on survival in women infected with HIV: a systematic review of the literature and meta-analysis. Br J Obstet Gynaecol. 1998;105:827–835. [DOI] [PubMed] [Google Scholar]
- 7.Calvert C, Ronsmans C. Pregnancy and HIV disease progression: a systematic review and meta-analysis. Trop Med Int Health. 2015;20:122–145. [DOI] [PubMed] [Google Scholar]
- 8.Alliegro MB, Dorrucci M, Phillips AN, et al. Incidence and consequences of pregnancy in women with known duration of HIV infection. Italian Seroconversion Study Group. Arch Intern Med. 1997;157:2585–2590. [PubMed] [Google Scholar]
- 9.Hocke C, Morlat P, Chene G, et al. Prospective cohort study of the effect of pregnancy on the progression of human immunodeficiency virus infection. The Groupe d'Epidemiologie Clinique Du SIDA en Aquitaine. Obstet Gynecol. 1995;86:886–891. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Lieve V, Shafer LA, Mayanja BN, et al. Effect of pregnancy on HIV disease progression and survival among women in rural Uganda. Trop Med Int Health. 2007;12:920–928. [DOI] [PubMed] [Google Scholar]
- 11.Weisser M, Rudin C, Battegay M, et al. Does pregnancy influence the course of HIV infection? Evidence from two large Swiss cohort studies. J Acquir Immune Defic Syndr. 1998;17:404–410. [DOI] [PubMed] [Google Scholar]
- 12.Allen S, Stephenson R, Weiss H, et al. Pregnancy, hormonal contraceptive use, and HIV-related death in Rwanda. J Womens Health. 2007;16:1017–1027. [DOI] [PubMed] [Google Scholar]
- 13.Berrebi A, Kobuch WE, Puel J, et al. Influence of pregnancy on human immunodeficiency virus disease. Eur J Obstet Gynecol Reprod Biol. 1990;37:211–217. [DOI] [PubMed] [Google Scholar]
- 14.Deschamps MM, Pape JW, Desvarieux M, et al. A prospective study of HIV-seropositive asymptomatic women of childbearing age in a developing country. J Acquir Immune Defi Syndr. 1993;6:446–451. [PubMed] [Google Scholar]
- 15.Kumar RM, Uduman SA, Khurrana AK. Impact of pregnancy on maternal AIDS. J Reprod Med. 1997;42:429–434. [PubMed] [Google Scholar]
- 16.Heffron R, Mugo N, Ngure K, et al. Hormonal contraceptive use and risk of HIV-1 disease progression. AIDS. 2013;27:261–267. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Morrison CS, Chen PL, Nankya I, et al. Hormonal contraceptive use and HIV disease progression among women in Uganda and Zimbabwe. J Acquir Immune Defic Syndr. 2011;57:157–164. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Polis CB, Wawer MJ, Kiwanuka N, et al. Effect of hormonal contraceptive use on HIV progression in female HIV seroconverters in Rakai, Uganda. AIDS. 2010;24:1937–1944. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Nduati R, Richardson BA, John G, et al. Effect of breastfeeding on mortality among HIV-1 infected women: a randomised trial. Lancet. 2001;357:1651–1655. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Coutsoudis A, Coovadia H, Pillay K, et al. Are HIV-infected women who breastfeed at increased risk of mortality? AIDS. 2001;15:653–655. [DOI] [PubMed] [Google Scholar]
- 21.Kuhn L, Kasonde P, Sinkala M, et al. Prolonged breast-feeding and mortality up to two years post-partum among HIV-positive women in Zambia. AIDS. 2005;19:1677–1681. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Sedgh G, Spiegelman D, Larsen U, et al. Breastfeeding and maternal HIV-1 disease progression and mortality. AIDS. 2004;18:1043–1049. [DOI] [PubMed] [Google Scholar]
- 23.Mortality among HIV-1-infected women according to children's feeding modality: an individual patient data meta-analysis. J Acquir Immune Defic Syndr. 2005;39:430–438. [DOI] [PubMed] [Google Scholar]
- 24.Taha TE, Kumwenda NI, Hoover DR, et al. The impact of breastfeeding on the health of HIV-positive mothers and their children in sub-Saharan Africa. Bull World Health Organ. 2006;84:546–554. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Allen S, Meinzen-Derr J, Kautzman M, et al. Sexual behavior of HIV discordant couples after HIV counseling and testing. AIDS. 2003;17:733–740. [DOI] [PubMed] [Google Scholar]
- 26.Kempf MC, Allen S, Zulu I, et al. Enrollment and retention of HIV discordant couples in Lusaka, Zambia. J Acquir Immune Defic Syndr. 2008;47:116–125. [DOI] [PubMed] [Google Scholar]
- 27.Stephenson R, Barker J, Cramer R, et al. The demographic profile of sero-discordant couples enrolled in clinical research in Rwanda and Zambia. AIDS Care. 2008;20:395–405. [DOI] [PubMed] [Google Scholar]
- 28.Wall KM, Kilembe W, Vwalika B, et al. Hormonal contraception does not increase women's HIV acquisition risk in Zambian discordant couples, 1994-2012. Contraception. 2015;91:480–487. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Wall KM, Kilembe W, Nizam A, et al. Promotion of couples' voluntary HIV counselling and testing in Lusaka, Zambia by influence network leaders and agents. BMJ Open. 2012 Sep 6;2(5). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Wall K, Karita E, Nizam A, et al. Influence network effectiveness in promoting couples' HIV voluntary counseling and testing in Kigali, Rwanda. AIDS. 2012;26:217–227. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Allen S, Karita E, Chomba E, et al. Promotion of couples' voluntary counselling and testing for HIV through influential networks in two African capital cities. BMC Public Health. 2007;7:349. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Peters PJ, Zulu I, Kancheya NG, et al. Modified Kigali combined staging predicts risk of mortality in HIV-infected adults in Lusaka, Zambia. AIDS Res Hum Retroviruses. 2008;24:919–924. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Boeras DI, Luisi N, Karita E, et al. Indeterminate and discrepant rapid HIV test results in couples' HIV testing and counselling centres in Africa. J Int AIDS Soc. 2011;14:18. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Stephenson R, Vwalika B, Greenberg L, et al. A randomized controlled trial to promote long-term contraceptive use among HIV-serodiscordant and concordant positive couples in Zambia. J Womens Health. 2011;20:567–574. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Mark KE, Meinzen-Derr J, Stephenson R, et al. Contraception among HIV concordant and discordant couples in Zambia: a randomized controlled trial. J Womens Health. 2007;16:1200–1210. [DOI] [PubMed] [Google Scholar]
- 36.Lifson AR, Allen S, Wolf W, et al. Classification of HIV infection and disease in women from Rwanda. Evaluation of the World Health Organization HIV staging system and recommended modifications. Ann Intern Med. 1995;122:262–270. [DOI] [PubMed] [Google Scholar]
- 37.MacCarthy S, Laher F, Nduna M, et al. Responding to her question: a review of the influence of pregnancy on HIV disease progression in the context of expanded access to HAART in sub-Saharan Africa. AIDS Behav. 2009;13(suppl 1):66–71. [DOI] [PubMed] [Google Scholar]
- 38.INSIGHT START Study Group, Lundgren JD, Babiker AG, et al. Initiation of antiretroviral therapy in early asymptomatic HIV infection. N Engl J Med. 2015;373:795–807. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Friedman W. Corruption and Averting AIDS Deaths. Vol Working Paper 395. Washington, DC: Center for Global Development; 2015. [Google Scholar]
- 40.Kavanagh M, Cohn J, Mabote L, et al. Evolving human rights and the science of antiretroviral medicine. Health Hum Rights. 2015;17:E76–E90. [PubMed] [Google Scholar]
- 41.Siedner MJ, Ng CK, Bassett IV, et al. Trends in CD4 count at presentation to care and treatment initiation in sub-Saharan Africa, 2002-2013: a meta-analysis. Clin Infect Dis. 2015;60:1120–1127. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Mutimura E, Addison D, Anastos K, et al. Trends in and correlates of CD4+ cell count at antiretroviral therapy initiation after changes in national ART guidelines in Rwanda. AIDS. 2015;29:67–76. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Tromp N, Michels C, Mikkelsen E, et al. Equity in utilization of antiretroviral therapy for HIV-infected people in South Africa: a systematic review. Int J Equity Health. 2014;13:60. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Reynolds HW, Janowitz B, Wilcher R, et al. Contraception to prevent HIV-positive births: current contribution and potential cost savings in PEPFAR countries. Sex Transm Infect. 2008;84(suppl 2):ii49–ii53. [DOI] [PubMed] [Google Scholar]
- 45.Khu NH, Vwalika B, Karita E, et al. Fertility goal-based counseling increases contraceptive implant and IUD use in HIV-discordant couples in Rwanda and Zambia. Contraception. 2013;88:74–82. [DOI] [PMC free article] [PubMed] [Google Scholar]