

Abstract
Background:
Although a recognized and discussed injury, chondral rib fractures in professional American football have not been previously reported in the literature. There currently exists no consensus on how to identify and treat these injuries or the expected return to play for the athlete.
Purpose:
To present 2 cases of chondral rib injuries in the National Football League (NFL) and discuss the current practice patterns for management of these injuries among the NFL team physicians.
Study Design:
Case series; Level of evidence, 4.
Methods:
Two cases of NFL players with chondral rib injuries are presented. A survey regarding work-up and treatment of these injuries was completed by team physicians at the 2014 NFL Combine. Our experience in identifying and treating these injuries is presented in conjunction with a survey of NFL team physicians’ experiences.
Results:
Two cases of rib chondral injuries were diagnosed by computed tomography (CT) and treated with rest and protective splinting. Return to play was 2 to 4 weeks. NFL Combine survey results show that NFL team physicians see a mean of 4 costal cartilage injuries per 5-year period, or approximately 1 case per year per team. Seventy percent of team physicians use CT scanning and 43% use magnetic resonance imaging for diagnosis of these injuries. An anesthetic block is used acutely in 57% and only electively in subsequent games by 39%.
Conclusion:
A high index of suspicion is necessary to diagnose chondral rib injuries in American football. CT scan is most commonly used to confirm diagnosis. Return to play can take up to 2 to 4 weeks with a protective device, although anesthetic blocks can be used to potentially expedite return.
Clinical Relevance:
Chondral rib injuries are common among NFL football players, while there is no literature to support proper diagnosis and treatment of these injuries or expected duration of recovery. These injuries are likely common in other contact sports and levels of competition as well. Our series combined with NFL team physician survey results can aid team physicians in identifying these injuries, obtaining useful imaging, and counseling players and coaches and the expected time of recovery.
Keywords: chondral injury, rib, fracture, injury, football, return to play, treatment
Rib fractures are commonly seen in contact sports.1,3–5 Most of these injuries involve the osseous component of the rib, but chondral rib (also known as “costal cartilage”) fractures can also occur.4,6,14 Although chondral rib fractures are recognized and discussed in American football, to our knowledge, there are no previous reports in the literature of chondral rib fractures in professional American football players. We present 2 cases of chondral rib fractures and discuss the mechanism of injury, diagnosis, management, and return to play. In addition, we performed a written survey of National Football League (NFL) team physicians at the 2014 NFL Combine regarding their experience with these injuries. The purpose of this study was to enhance our understanding of the current practice patterns for chondral rib fractures in professional American football through 2 case reports and a survey of head team physicians across the NFL.
Case 1
A 25-year-old linebacker in the NFL sustained a blunt injury to his left flank during a tackle on a kickoff return. He was evaluated on the sideline and complained of pain in his left anterior ribs. Examination showed tenderness to palpation with swelling at the border of his rectus abdominus. The patient reported “clicking” with active twisting motions. He was removed from the game and a plain film rib series radiography at the stadium showed no obvious injury. Oxygen saturation was 99% on room air with stable vital signs. Examination by the team medical physician showed no abdominal or renal tenderness. There was no hematuria or hemoptysis. Chest radiography showed no evidence of pneumothorax, and the lungs were clear to auscultation. A noncontrast computed tomography (CT) scan was obtained and showed a minimally displaced fracture at the chondral portion of the left seventh rib (Figure 1). The patient was treated with rest for 3 days followed by physical therapy with various modalities and progressive mobility. Light jogging was started 5 days postinjury, with agility exercises on day 6 to tolerance. An anesthetic block of 3 mL 0.5% plain bupivacaine prior to the game did not provide sufficient pain relief for return to play on postinjury day 7. An additional 3 days of rest followed by physical therapy was begun, and the patient returned to play at postinjury day 14, with a pregame anesthetic block of 3 mL 0.5% plain bupivacaine and a protective pad. The patient had no further limitations from the chondral fracture and did not require any additional anesthetic blocks in subsequent games, although the athlete stated it took approximately 8 weeks before it felt “normal” without any soreness or clicking. No follow-up imaging was performed given the resolution of his symptoms.
Figure 1.

Case 1. (A) Transverse, noncontrast computed tomography (CT) image at the level of the left seventh rib showing fracture and overlap of the costal cartilage (arrows). (B) Sagittal reformation CT showing overlapping costal cartilage at the level of the fracture (arrows). (C) Three-dimensional volume rendering of CT data showing disruption of the seventh costal cartilage (arrow). Three-dimensional reconstructions can be helpful in visualizing costal cartilage fractures.
Case 2
A 26-year-old defensive back sustained a direct blow to his abdomen and right flank by a running back’s helmet on a goal line tackle. He was examined on the field and stated he “had the wind knocked out of him” but still had significant pain in his right anterior ribs. Swelling was seen at his rectus abdominus and costal margin and he reported a “clicking sensation” with Valsalva maneuver or twisting motions. Plain film rib series was negative. Abdominal examination was negative for renal or hepatic injury, with normal vital signs, oxygen saturation (98%), and chest radiography. The patient was unable to ambulate due to discomfort. However, given that the injury occurred at an “away” game and the patient’s significant symptoms, we were concerned about his tolerance of the 4.5-hour return flight and were compelled to exclude intra-abdominal injury. A noncontrast CT scan was performed at the local hospital and revealed no evidence of acute organ injury but demonstrated a chondral fracture of the right sixth rib with 100% displacement and a nondisplaced chondral fracture of the right seventh rib (Figure 2). He underwent 7 days of rest followed by physical therapy. The athlete was unable to return for the next 3 games due to pain that limited function. The risks and benefits of an anesthetic block were discussed and the patient declined. He was able to return at 4 weeks with a protective brace. No further treatment was necessary, and he reported no further discomfort or clicking after week 6 postinjury. No follow-up imaging was obtained given the resolution of his symptoms.
Figure 2.
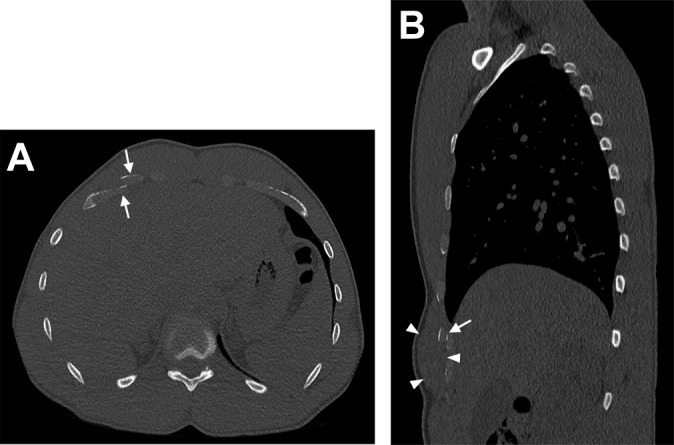
Case 2. (A) Transverse, noncontrast computed tomography (CT) image at the level of the right sixth rib showing fracture and overlap of the sixth costal cartilage (arrow). Other nondisplaced fractures not shown. (B) Sagittal reformation CT showing costal cartilage fracture (arrow) and adjacent soft tissue swelling involving adjacent musculature (arrowheads).
Team Physician Survey
After approval by the NFL research committee, a survey was issued to all 32 NFL team physicians at the 2014 NFL Combine in Indianapolis, Indiana (see the Appendix). Completed forms were received from 23 teams. The mean number of costal rib fractures seen by the group over the previous 5 years was 4, ranging from 0 to 15. All team physicians initially utilized plain films to rule out an osseous rib fracture. If negative and there was suspicion of a chondral rib injury, 70% of team physicians utilized a CT scan of the chest as the advanced imaging method of choice. Two physicians reported that they used CT only if there was continued pain beyond what would be expected for a rib contusion. Forty-three percent of physicians had utilized magnetic resonance imaging (MRI) to assist in making the diagnosis, with most citing that they would do so if the CT scan was negative and clinical symptoms suggested chondral injury. Fifty-seven percent of team physicians used anesthetic blocks in an effort to expedite return to play in both the acute and elective setting; 39% of physicians would use an anesthetic block only electively for subsequent games, but not in the acute setting. One team responded that they would never offer or utilize an anesthetic block in the setting of chondral rib fractures.
Discussion
Chondral rib fractures are a recognized injury in professional American football players, with estimates of 4 fractures per 5-year period (approximately 1 case per team per year) seen by the NFL team physicians in our survey. Most rib fracture studies in the sports literature focus on stress fractures, commonly seen in rowing athletes and baseball pitchers.9,10 Studies of acute chondral rib fractures in the athlete secondary to blunt injury are limited. To our knowledge, there are no previous reports of chondral rib fracture in professional American football in the literature. An epidemiologic study of NFL spine and axial skeleton injuries notes 4% (86/2208) of these injuries are “thoracic and ribs,” and only 10 of these were fractures,8 but this is in contrast to the experience of the NFL team physician based on our survey.
Two case reports describe chondral rib fractures in the rugby athlete. Lopez et al6 reported on a 27-year-old rugby athlete with a right 5th and 6th costal cartilage fractures displaced 100%. The patient was treated conservatively and was pain free at 8 weeks. A CT scan at 10 weeks postinjury showed evidence of “healing,” but the patient reported occasional painless “clicking” 1 year postinjury.6 Willis-Owen et al14 reported on a 29-year-old rugby athlete who sustained a hepatic laceration and hematoma secondary to a displaced right 5th and 6th costochondral junction separation. No internal organ injury was seen in our 2 cases, and no organ injury secondary to chondral rib fracture was reported by the team physician survey.
The anatomy of the chondral ribs described in the literature is variable. Some images show a fusion of the chondral ribs extending to the xiphoid. We have found many cases without a fusion mass, and the length of the chondral projection is quite variable. It is classically seen that the sixth through eighth ribs are involved in chondral rib fractures as their anatomic position makes them the most exposed to blunt injury. Both of our cases had localized swelling at the rectus abdominus and costal margin that was seen on physical examination as well as CT imaging. This specific swelling pattern should raise the suspicion of the medical team for a possible chondral rib fracture in contact sport athletes. A click was also consistently palpated and recognized by the patient with Valsalva maneuver and twisting motions.
We used CT imaging as a reliable method to confirm the diagnosis, and this is the imaging modality most commonly utilized by NFL team physicians. CT is most useful for detecting displacement or discontinuities involving costal cartilage structures. Nondisplaced fractures involving costal cartilage may not be identified, but conservative treatment should focus on management of symptoms. Use of MRI has been described by Subhas et al13 and may be more sensitive than CT scanning in detecting nondisplaced fractures. However, MRI of ribs is challenging due to the small cross-sectional diameter of the ribs and long scan times. Regarding decisions for return to play in American football, CT imaging appears to be an efficient and very useful first-line modality, most commonly utilized by team physicians across the league. In any patient where solid organ injury is suspected, use of intravenous contrast should be considered, though this is not necessary for costal cartilage assessment itself. Ultrasound has also been reported as a useful diagnostic modality for assessment of chondral rib fractures but is highly operator dependent and much more commonly practiced overseas as compared with the United States.7
Treatment of chondral rib fractures should always start with rest until the acute pain and spasm declines, allowing for physical therapy to begin. Rib protectors have been previously described but are bulky and not well tolerated by many athletes.2 Newer versions of rib protection can be form-fitted and sewn into an undergarment (Figure 3). We have had no complaints from our athletes with use of these lower profile, lightweight devices in terms of return-to-play function.
Figure 3.

Custom-fitted rib protector sewn into undergarment.
Local anesthetic has been used to allow an injured contact athlete to return to play with reasonable safety but variable efficacy dependent on anatomic location.11,12 Anesthetic block to chondral rib injuries appears to be an accepted and commonly utilized treatment to assist in rapid return to play based on our survey of NFL team physicians. In 1 of our athletes, we were not successful in providing adequate pain relief after a block at week 1. Our experience has been a somewhat less predictable pain relief after a block for chondral versus osseous rib fractures; this may be due to the increased mobility of chondral rib fragments combined with the significant core muscular attachments of the abdomen. One of our athletes declined an anesthetic block after we discussed the theoretical risk of further injury, including abdominal injury, as well local or systemic reactions to the anesthetic.
The most common location of the sixth through eighth chondral rib fracture anesthetic block is anterior and superficial, and this procedure is relatively safe. We know of no reports of cardiothoracic or abdominal injury or significant reactions to blocks to this area, and no team physicians in our survey reported any complications. We are aware of rare anecdotal reports of pneumothorax after injection of osseous (not chondral) rib injuries, but this is outside the scope of this discussion. We performed our chondral rib injections on the superficial inferior aspect of the affected rib without image guidance. Ultrasound-guided injections have been used by some, but further experience is needed to see if this image guidance method is advantageous in this clinical setting.
Return to play was 2 and 4 weeks in our cases, but the latter case did not undergo any anesthetic blocks. Regardless, we believe these injuries can significantly limit function due to the mobility of the chondral ribs and core muscle attachments, and an anesthetic block may not be sufficient in the acute period to guarantee early return to play. In the American football athlete, one should be prepared to wait 3 to 4 weeks before return to play, and symptoms may persist longer. We did not obtain follow-up imaging as the players’ symptoms had completely resolved; therefore, we do not know whether the fractures healed radiographically. Although these injuries may not always form a chondral union, they appear to stabilize to allow full function without deficit. One study recommends fragment excision and even states “these patients do badly with conservative management and have persistent symptoms.”4 Based on our anecdotal experience and discussion with other team physicians, we are not aware of long-term consequences of these injuries, but no systematic or long-term follow-up is available. Neither of the 2 athletes we report on here experienced any residual symptoms after 8 weeks, and neither required further treatment. Further study is needed to determine which patients are at increased risk for persistent symptoms and the potential need for later surgery.
Conclusion
A high index of suspicion of chondral rib fracture is necessary for the American football athlete who has tenderness and swelling at the lateral rectus abdominus and costal margin border, especially if a “click” is present. Plain radiographs are typically normal, but CT imaging is highly effective in detection of displaced chondral rib fractures. Return to play may be up to 4 weeks and can be assisted by a protective device. An anesthetic block may also be a reasonable means to expedite return to play, but only after thorough discussion of the risks and benefits with the athlete.
Appendix
National Football League (NFL) Rib Injury Questionnaire

Footnotes
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution.
References
- 1. Barrett GR, Shelton WR, Miles JW. First rib fractures in football players. A case report and literature review. Am J Sports Med. 1988;16:674–676. [DOI] [PubMed] [Google Scholar]
- 2. Cain TE, Donzis B, Meins J. Use of the air-inflated jacket in football. Am J Sports Med. 1981;9:240–243. [DOI] [PubMed] [Google Scholar]
- 3. Colosimo AJ, Byrne E, Heidt RS, Jr, Carlonas RL, Wyatt H. Acute traumatic first-rib fracture in the contact athlete: a case report. Am J Sports Med. 2004;32:1310–1312. [DOI] [PubMed] [Google Scholar]
- 4. Gregory PL, Biswas AC, Batt ME. Musculoskeletal problems of the chest wall in athletes. Sports Med. 2002;32:235–250. [DOI] [PubMed] [Google Scholar]
- 5. Hame SL, LaFemina JM, McAllister DR, Schaadt GW, Dorey FJ. Fractures in the collegiate athlete. Am J Sports Med. 2004;32:446–451. [DOI] [PubMed] [Google Scholar]
- 6. Lopez V, Jr, Ma R, Li X, Steele J, Allen AA. Costal cartilage fractures and disruptions in a rugby football player. Clin J Sport Med. 2013;23:232–234. [DOI] [PubMed] [Google Scholar]
- 7. Malghem J, Vande Berg B, Lecouvet F, Maldague B. Costal cartilage fractures as revealed on CT and sonography. AJR Am J Roentgenol. 2001;176:429–432. [DOI] [PubMed] [Google Scholar]
- 8. Mall NA, Buchowski J, Zebala L, Brophy RH, Wright RW, Matava MJ. Spine and axial skeleton injuries in the National Football League. Am J Sports Med. 2012;40:1755–1761. [DOI] [PubMed] [Google Scholar]
- 9. Miller TL, Harris JD, Kaeding CC. Stress fractures of the ribs and upper extremities: causation, evaluation, and management. Sports Med. 2013;43:665–674. [DOI] [PubMed] [Google Scholar]
- 10. O’Neal M, Ganey TM, Ogden JA. First rib stress fracture and pseudarthrosis in the adolescent athlete: the role of costosternal anatomy. Clin J Sport Med. 2009;19:65–67. [DOI] [PubMed] [Google Scholar]
- 11. Orchard JW. Is it safe to use local anaesthetic painkilling injections in professional football? Sports Med. 2004;34:209–219. [DOI] [PubMed] [Google Scholar]
- 12. Orchard JW, Steet E, Massey A, Dan S, Gardiner B, Ibrahim A. Long-term safety of using local anesthetic injections in professional rugby league. Am J Sports Med. 2010;38:2259–2266. [DOI] [PubMed] [Google Scholar]
- 13. Subhas N, Kline MJ, Moskal MJ, White LM, Recht MP. MRI evaluation of costal cartilage injuries. AJR Am J Roentgenol. 2008;191:129–132. [DOI] [PubMed] [Google Scholar]
- 14. Willis-Owen C, Kemp SP, Thomas RD. Hepatic injury after costochondral separation in a rugby football player. Clin J Sport Med. 2009;19:70–71. [DOI] [PubMed] [Google Scholar]