

Abstract
Background:
The rising incidence of breast cancer is complicated by late presentation, which marks breast cancer diagnosis in Nigeria with about 70% of cases presenting at advanced stages of the disease. The aim of this study is to determine the general level of awareness of breast cancer, breast cancer risk factors, signs/symptoms as well as preventive measures nothern Nigerian women. It also aimed at determining their attitudes toward breast cancer cure, prevention and cause. Finally, it aims to determine their practices toward breast cancer and its associated factors.
Methods:
A cross-sectional community survey was used to study 230 women aged 15–60 years in Chikun Local Government Area. The subjects were selected based on nonprobability sampling. Data collected using self-administered questionnaire were analyzed using Statistical Package for Social Science students (version 16). Test of associations employed Chi-square statistical tool with the level of significance taken at 0.05.
Results:
About 75.2% knew about breast cancer with health facility (29.13%) being the greatest source of information. An average of 29.35% had knowledge of the risk factors tested. Mean knowledge of the signs and symptoms was 50.1% Average knowledge of breast cancer screening methods was 34.26% with breast self-examination (BSE) (46.1%) being the most recognized. In relation to perception, about 21.7% strongly agreed with the fact that breast cancer is treatable following early detection while 18.3% strongly agreed that screening is effective in detecting breast cancer. Concerning practice, an average of 10.2% practiced any of the screening methods, with BSE (17.4%) being the most practiced. Strongest reasons for nonpractice was ignorance (17.4%). An association was established between knowledge and practice of all the screening methods (P = 0.001 respectively).
Conclusions:
There is insufficient knowledge, as well as poor practices in relation to important factors associated with breast cancer prevalence.
Keywords: Attitudes, breast cancer, knowledge, Nigeria, practice, women
INTRODUCTION
Breast cancer is the most common cause of death from cancer in women worldwide. It is estimated to be responsible for almost 460,000 deaths in 2008 with more than 1 million being diagnosed annually.[1,2] The incidence seemed to be rising in the developing countries due to increasing life expectancy, urbanization and adoption of western lifestyles.[3] In these countries it tended to occur more commonly at a younger age.[4,5,6] In a place like Nigeria the rising incidence of breast cancer is complicated by late presentation, which marks breast cancer diagnosis in Nigeria, with about 70% of cases presenting at advanced stages of the disease.[7,8] This late presentation leaves them with the option of sophisticated treatment procedures, which in most cases may be unaffordable. Mammography which has been recommended as most effective diagnostic tool is not readily available and even when present is unaffordable.[9] However recognition of early warning signals, signs and symptoms as well as early screening by clinical breast examination (CBE) have been recommended as effective.[3] The positive role of breast self-examination (BSE) has also been strongly recommended as a commendable strategy in developing countries.[10,11,12]
These emphasize the need for appropriate awareness and attitude in breast cancer prevention. Unfortunately poor knowledge of risk factors and preventive measures such as early screening have been observed even among rural health workers.[6,13] The role of poor information and enlightenment as a barrier to early presentation has been highlighted in literature. Good knowledge attitude and practices would only be much helpful in Nigeria if it is acquired early, knowing that breast cancer presentation appear earlier among Nigerian women. The need for breast cancer research of this type is more critical in Northern Nigeria where little or nothing has been done compared to southern part of the country.
It was against this backdrop that this study was aimed at presenting the perspective of nothern Nigerian women in relation to breast cancer by determining their general level of awareness of breast cancer, breast cancer risk factors, signs/symptoms as well as preventive measures. It also aimed at determining their attitudes toward breast cancer cure, prevention and cause. Lastly it aimed at determining their practices toward breast cancer, its associated factors as well as strongest reasons for nonpractice of early detective measures in a rural community of Northern Nigeria.
METHODS
The study used a cross-sectional study technique to assess the level of knowledge, attitude, and practices of 230 women in Chukun local Government Area of Kaduna State North Central geopolitical zone of Nigeria. The sample size was statistically determined. The women included were only those residing within the study area during the period of the study and aged between 15 and 60 years. Informed consent from the director of primary health care of the local government was obtained in writing, while those of individual respondents were obtained orally. Purposive sampling was used to select 5 settlements (wards) in the area thought to be more representative of the population studied. Since the ward census figures were unavailable, the sample sizes were assumed to be equal, bearing in mind that all of them live in similar social setting. Hence, the subjects were equally divided among the five wards. The researcher took positions at the main entrance of each settlement and questionnaires were given to willing eligible participants until the required sample was completed. Initially planned systematic sampling procedure involving house to house survey could not be employed due to vicarious security situation in the state during the period. The questionnaires were filled by the respondents and collected on the spot by the researcher.
The instrument for data collection was semi structured questionnaire developed from those used in previous published studies. Knowledge and practices toward breast cancer were measured based on respondents’ answers, depending on whether the subject chose “Yes” or “No” option to the relevant questions. “Yes” indicated presence of knowledge while “No” indicated absence of it. Attitudes were measured based on four scale options -“Strongly agreed”, “Agreed,” disagreed and strongly disagreed. Levels of attitudes were estimated based on number of people that ticked a particular option.
The semi-structured questionnaire was divided into three sections, the first section contained questions aimed at determining the subjects general knowledge of breast cancer as well as knowledge of breast cancer risk factors, signs and symptoms and methods of early detection. The second section contained questions aimed at determining their perception toward curability of breast cancer, effectiveness of early screen and cause of breast cancer. The third section contained questions aimed at determining their practices in relation to recommended methods of early detection. The data were analyzed using Statistical Package for Social Science Students (version 16, United States, 2007). Test of association was done using Chi-square statistics, with level of significance taken at 5%.
RESULTS
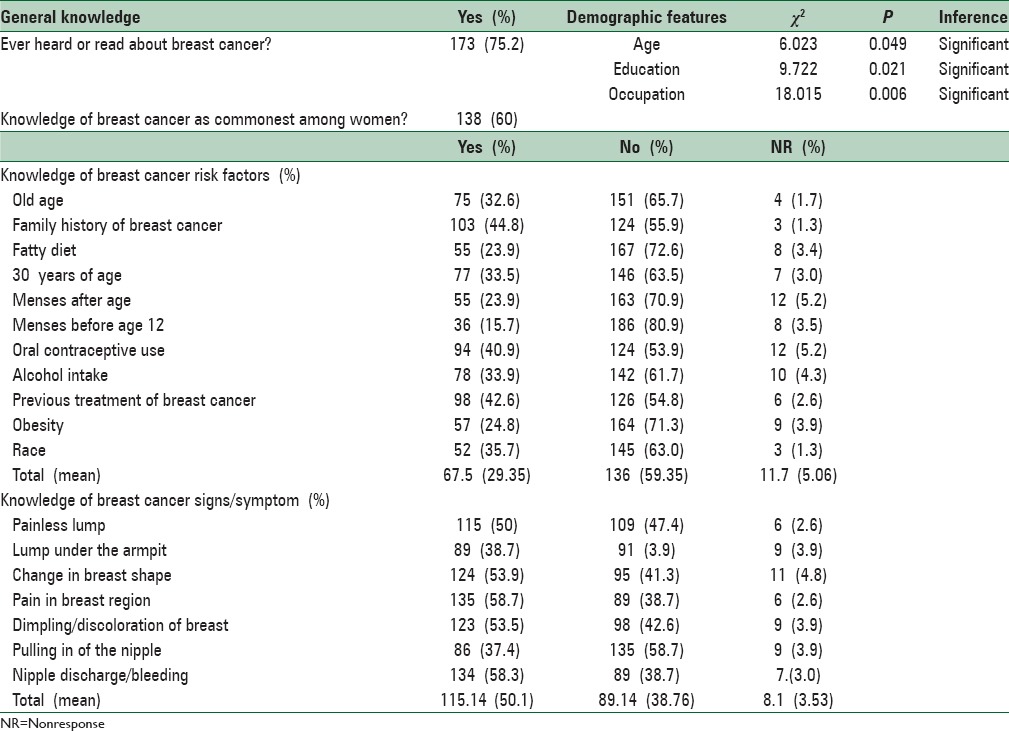
Table 1 indicated that greater number 194 (84.3%) were below the age of 40 years. Singles 97 (42.2), followed by married, 90 (39.1) were more represented. Christianity (67.8%) followed by Islam (23.9%) has the greatest population. A good number has tertiary education (45.7%). Secondary education was (32.6%), while primary was 9.6%. Students (28.7%) have higher population, followed by civil servant (23.9%), then traders (20.4%). Professionals constitute about 7.8%, Fulltime housewives, 7%, the rest were below 6 Table 2 shows that about 173 (75.2%) knew about breast cancer. This knowledge seemed to be significantly associated with age (P = 0.049), educational status (0.021), and occupation (0.006). Mean number of people with knowledge of each of the risk factors was 68 (29.35%) with highest number being recorded for family history of breast cancer, 103 (44.8%) and lowest for menses before the age of 12, 36 (15.7%). Previous treatment was 98 (42.6%), while old age was 75 (32.6%) obesity was 57 (24.8%). Mean number of people with knowledge of each of the breast cancer signs and symptoms was 115 (50.1%), with highest frequency being recorded for Pain in the breast region, 135 (56.7%) and lowest for pulling in of the nipple, 86 (37.4%). Painless lump was 115 (50%) while lump under the armpit was 89 (38.7%).
Table 1.
Sociodemographic data
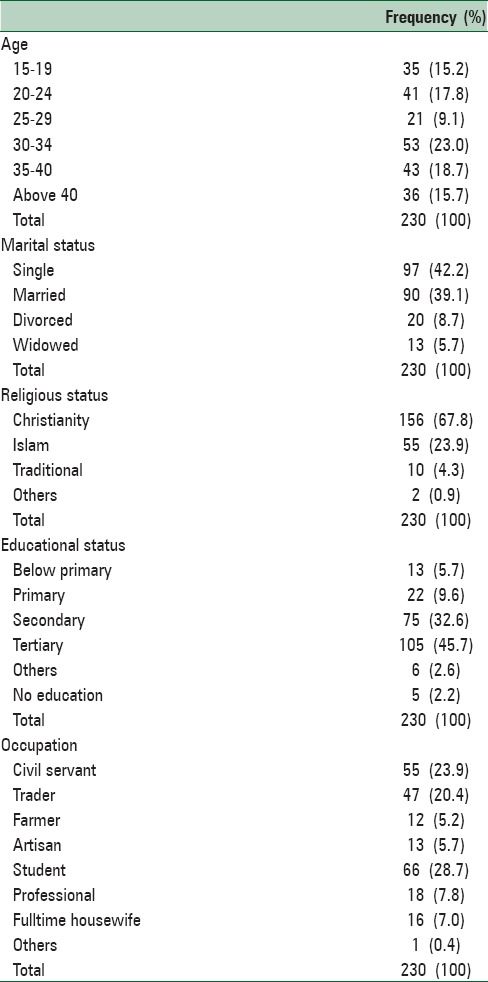
Table 2.
Knowledge of breast cancer: General information, risk factors, signs and symptoms
Strongly agree, agree, disagree, strongly disagree, nonresponse
Table 3 shows that it was only about 21.7% of the respondents that strongly agree (SA) with the opinion that breast cancer is curable when detected early. In relation to the effectiveness of early screening in detecting breast cancer, it was only 18.3%, while on the role of evil spirits in the causation of cancer it was 34.8% that strongly disagree (SD). These three perceptions seems to be significantly associated with education (P = 0.001, 0.031, and 0.005, respectively). Perception about curability of breast cancer in addition seems to be significantly associated with age (P = 0.049) and occupation (P = 0.037).
Table 3.
Perception toward cure, screening and cause of breast cancer

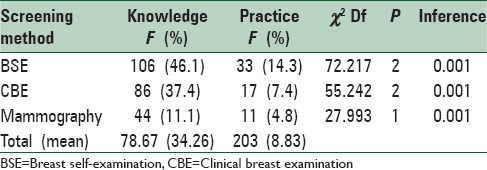
Table 4 indicates that the knowledge of BSE as screening method was 106 (46.1%) compared to practice 33 (14.3%), while that of CBE was 86 (37.4%) compared to 33 (14.3%). Knowledge of mammography was 44 (11.1%) compared to practice 11 (4.8%). Table 4 also shows that knowledge of these early detection procedures seem to be significantly associated with level practices toward them (P = 0.001 respectively).
Table 4.
Knowledge and practices toward breast cancer screening methods
DISCUSSION
The sociodemographic data according to Table 1 indicated that greater number were below the age of 40 years. This showed that most of them were younger, active, mobile and within their prime age of reproduction. Singles followed by married, were more represented. This may probably be due to the security situation, which might have forced some married women to stay back at home because of their children. Christianity followed by Islam has the greatest population probably due to the Stronger influence of Christianity in southern Kaduna compared to northern Kaduna where Islam dominates. The level of education seemed to be very high compared to what might be expected in a typical rural community in northern Nigeria with greater number 105 (45.7%) having tertiary education. This suggested that most of them might have good opportunities for breast cancer information. The higher representation of students and civil servants may be in consistent with the fact that most of them were educated, single and younger. General knowledge was good compared to 58.2% reported in north eastern Nigeria,[14] and 43.67% recently reported among south Indian women, possibly due to differences in educational and work exposures. However, these findings fell below the report of another recent study among southern Nigerian women.[15] It was quite disturbing however that substantial number (24.8%) had no idea of breast cancer. General knowledge seemed to be significantly associated with age (P = 0.049), educational status (P = 0.021), occupation (P = 0.006). It seemed that as people grew older their tendency to be exposed to information increased. About 74.55% of those aged between 15 and 24 had information, compared to 86.59% among those aged 35–55 years of age. However, Grunfeld et al. in his study of British women did not associate higher knowledge of risk factors with increasing age.[16] The variable in this study however is “general knowledge”. Higher number of people with knowledge of breast cancer was also recorded among those with tertiary education and Professional occupations. There were also suggestions in keeping with this study that increasing level of education and occupational status tended to be associated with knowledge and practices.[6,17] Mean number of people with knowledge of the risk factors was low 68 (29.35%). This low knowledge was worse for “menses before the age of 12” (15.7%) compared to “family history of breast cancer” (44.8%). Poor knowledge of breast cancer risk factors among women have been reported in several studies.[6,9,18] However the record in this study seemed to be lower than most of them, but slightly higher than the average recorded in a recent study in southern Nigeria,[19] primary prevention of breast cancer would be difficult in an environment where the population are ignorant of the key risk factors implicated, since they may not see much reasons to reduce their exposures to them. “Family history of breast cancer” which was most recognized by the respondents had been so recognized in previous studies,[16,20,21,22] in contrast to another.[6,19] The poor recognition of factors such as “occurrence of menstruation before the age of 12,” “menstruation after the age of 55,” “ first birth after the age of 30 years” etc., had also been noted in previous studies,[23,24,25] old age which is an important risk factor in the development of breast cancer[26] was recognized by only 75 (32.6%) in contrast to other previous studies,[16,25] but higher than reports by another study in Benin city.[15] Lack of access by most women to vital information on risk factors that decrease breast cancer risk had been linked to observed late presentation in some places.[26]
Mean number of people with knowledge of the breast cancer signs and symptoms was 115 (50.1%). This was relatively good in comparison to mean knowledge of risk factors (29.35%) and indicated that preventive measures among them were more likely to commence at the level of secondary prevention after signs and symptoms had already appeared. Moreover, the leading signs and symptoms recognized seemed to be those associated with advancing conditions of the disease such as nipple discharge/bleeding, pains in the breast region, (which may either be associated with advancing or benign condition),[27] and change in the breast shape, Painless lump and lump under the armpit, which recognition hold the key to early detection were less recognized. This pattern of recognition had been echoed in previous study in southern Nigeria[19] and strongly suggested the tendency for late presentation which had been noted among Nigerian women by several authors.[6,20] In general, the knowledge of signs/symptoms in this study seemed to be higher than several past studies,[6,19,28,29,30,31] while lagging behind in another.[20] These might be attributed to differences in educational and work exposures as well as time gap.
In relation to attitudes, it was only 50 (21.7%) of the respondents that strongly agreed with the opinion that breast cancer is curable when detected early. Strong perception towards the effectiveness of screening was seen in only in 42 (18.3%). These might suggest tendency for poor health seeking attitude towards conventional screening and treatment. This could aggravate risk. These were in contrast with the findings of previous studies in southern Nigeria where fairly good attitude levels were recorded.[15,32,33] These perceptions were significantly associated with levels of education (P = 0.001 and 0.031 respectively). Perception toward cure was also significantly associated with age (P = 0.049), and occupation (P = 0.037). In relation to perception towards the role of evil spirits in the etiology of breast cancer it was only 34.8% that strongly disagreed with the opinion that evil powers have role in it. This might be one of the reasons why many could not perceive screening and treatment as effective. It might reflect the role of superstitious beliefs about cancer etiology reported in literature.[6] However in a more recent study from southern Nigeria, most of the respondents (82.4%) disagreed with the opinion that breast cancer is the work of evil spirits.[15] This discrepancy in perceptions might be attributed to differences in socio cultural beliefs. This perception was significantly associated with level of education (P = 0.005).
Table 4 indicated that the level of knowledge expressed for BSE, CBE and mammography respectively was substantially higher than their corresponding level of practice. The same pattern had been noted in previous local studies, strongly suggesting that knowledge might not always lead to practice despite presence of significant association.[15,19,34] The mean knowledge of early detection practices was 79 (34.26.%). Poor knowledge of preventive practices had been widely reported even among rural health workers.[6,13,35,36] Where knowledge had been relatively high it had always been among a very enlightened urban population.[23,35,37] This might be responsible for the abysmally poor level of practice observed not only in this study, but also in previous studies.[4,14,36,38] Significant associations were established between knowledge of these early detection procedures and levels of practices towards them (P = 0.001 respectively). Similar associations had also been reported in Nigeria and other place.[15,39] The commonest sources of breast cancer information according to Figure 1 were hospital/health center and electronic media. Electronic media and hospital as leading sources of breast cancer information had been documented in Nigeria and other places.[6,28,38,40] It suggested the important opportunity these channels present in the dissemination of breast cancer information. However in another study in north-eastern Nigeria, family and friends (52.38%), followed by health workers were the leading sources of information.[14]
Figure 1.
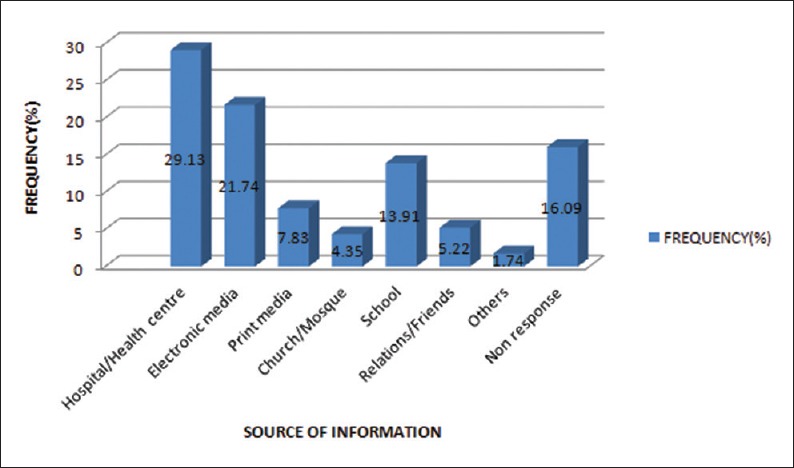
Source of breast cancer information. That the commonest source of breast cancer information was hospital/health centre 67 (29.13%), followed by electronic media 50 (21.74%) then school 32 (13.91%), before print media 18 (7.83%)
According to Figure 2 the strongest reason why most of the respondents did not practice screening procedures was “lack of knowledge,” followed by the “feeling that one cannot get cancer,” then the desire to avoid fear or anxiety.
Figure 2.
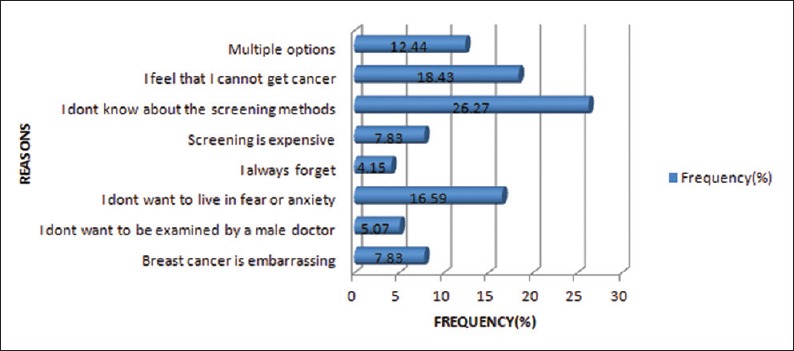
Strongest reasons for nonpractice of early detection measures. That the strongest reason hindering practice according to the respondents was “lack of knowledge” 60 (26.27%), followed by the “feeling that one cannot get cancer” 42 (18.43%), then the desire to avoid fear or anxiety 38 (16.59%)
These were the same three top reasons cited by respondents in Benin city, southern Nigeria.[15] Other previous studies had also cited the same reasons.[41,42] These reasons further confirmed the findings that practice is positively associated with level of knowledge. The “feeling that they cannot get cancer” reflected their poor awareness of breast cancer risk factors earlier cited, while the desire to avoid fear and anxiety reflected in their poor practices toward early detection. These might increase the risk of late presentation. It also further suggested that the respondents seemed to be ignorant of the seriousness of breast cancer.
CONCLUSIONS
The study suggested that the respondents seemed not to be sufficiently informed to the extent of reducing their exposure and vulnerability to breast cancer. Much of what they knew would do little to encourage behavioral change and health seeking behavior relevant for primary prevention and early detection. Good attitudes and practices towards prevention were also poor. However while there was evidence that when knowledge improved, practice level also seemed to improve, there was also strong suggestion that not everyone who had knowledge was willing to practice it. Generally, knowledge and attitude seemed to be affected by age, education and occupation. Their ignorance and negative beliefs also seemed to be interfering with good practices.
Limitation of the study
One limitation of this study lies in the sampling of subjects. The initially planned sampling of subjects based on systematic house to house survey could not be applied owing to prevailing security situation in the northern Nigerian communities during the period of the study.
Recommendations
Health education on breast cancer prevention should focus on creating awareness about common risk factors in the population that increases vulnerability. Emphasis on the need and procedure for early detection of painless lumps should be made
Breast cancer awareness programs in the rural communities should be designed to tackle sociocultural and superstitious beliefs about the nature and cause of breast cancer, as well as presented in a manner that would evoke behavioral change. This can be achieved by the use of audiovisuals, as well as a supervised demonstration sections for common procedures such as BSE on the spot. This would increase their confidence on practice
Exploring health facility avenues and electronic media in the creating awareness about breast cancer should also be encouraged
The study could be repeated in the same or similar setting with individual subjects sampled based on systematic house to house survey.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- 1.Sabouhi F, Babaee S, Naji H, Zade AH. knowledge, awareness, attitudes and practice about hypertension in hypertensive patients referring to public health care centers in Khoor and Biabanak 2009. Iran J Nurs Midwifery Res. 2011;16:35–41. [PMC free article] [PubMed] [Google Scholar]
- 2.Coughlin SS, Ekwueme DU. Breast cancer as a global health concern. Cancer Epidemiol. 2009;33:315–8. doi: 10.1016/j.canep.2009.10.003. [DOI] [PubMed] [Google Scholar]
- 3.World Health Organization. Prevention and Control of Breast Cancer. [Last accessed on 2015 Dec 14]. Available from: http://www.who.int/cancer/detection/breastcancer/en/
- 4.Rosmawati NH. Knowledge, attitudes and practice of breast self-examination among women in a suburban area in Terengganu, Malaysia. Asian Pac J Cancer Prev. 2010;11:1503–8. [PubMed] [Google Scholar]
- 5.Adesunkanmi AR, Lawal OO, Adelusola KA, Durosimi MA. The severity, outcome and challenges of breast cancer in Nigeria. Breast. 2006;15:399–409. doi: 10.1016/j.breast.2005.06.008. [DOI] [PubMed] [Google Scholar]
- 6.Okobia MN, Bunker CH, Okonofua FE, Osime U. Knowledge, attitude and practice of Nigerian women towards breast cancer: A cross-sectional study. World J Surg Oncol. 2006;4:11. doi: 10.1186/1477-7819-4-11. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Okobia MN, Osime U. Clinicopathological study of carcinoma of the breast in Benin City. Afr J Reprod Health. 2001;5:56–62. [PubMed] [Google Scholar]
- 8.Anyanwu SN. Breast cancer in eastern Nigeria: A ten year review. West Afr J Med. 2000;19:120–5. [PubMed] [Google Scholar]
- 9.Salaudeen AG, Akande TM, Musa OI. Knowledge and attitude to Breast cancer and breast self-examination among females. Eur J Soc Sci. 2009;7:157–65. [Google Scholar]
- 10.Obaji NC, Elom HA, Agwu UM, Nwigwe CH, Ezeonu PO, Umeora OUJ. Awareness and Practice of Breast Examination among Market women in Abakiliki, South East Nigeria. Ann Med Health Sci Res. 2013;3:12. doi: 10.4103/2141-9248.109457. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Siahpush M, Singh GK. Sociodemographic predictors of pap test receipt, currency and knowledge among Australian women. Prev Med. 2002;35:362–8. doi: 10.1006/pmed.2002.1086. [DOI] [PubMed] [Google Scholar]
- 12.Ferro S, Caroli A, Nanni O, Biggeri A, Gambi A. A cross sectional survey on breast self-examination practice, utilization of breast professional examination, mammography and associated factors in Romagna, Italy. Tumori. 1992;78:98–105. doi: 10.1177/030089169207800207. [DOI] [PubMed] [Google Scholar]
- 13.Akhigbe AO, Omuemu VO. Knowledge, attitudes and practice of breast cancer screening among female health workers in a Nigerian urban city. BMC Cancer. 2009;9:203. doi: 10.1186/1471-2407-9-203. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Omatara B, Yahya S, Amodu M, Bimba J. Awareness, attitude and practice of rural Women regarding breast cancer in Northeastern Nigeria. J Community Med Health Educ. 2012;2:5. [Google Scholar]
- 15.Azubuike S, Okwuokei S. Knowledge, attitude and practices of women towards breast cancer in Benin City, Nigeria. Ann Med Health Sci Res. 2013;3:155–60. doi: 10.4103/2141-9248.113653. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Grunfeld EA, Ramirez AJ, Hunter MS, Richards MA. Women's knowledge and beliefs regarding breast cancer. Br J Cancer. 2002;86:1373–8. doi: 10.1038/sj.bjc.6600260. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Adebamowo CA, Ajayi OO. Breast cancer in Nigeria. West Afr J Med. 2000;19:179–91. [PubMed] [Google Scholar]
- 18.Gakwaya A, Galukande M, Luwaga A, Jombwe J, Fualal J, Kiguli-Malwadde E, et al. Breast cancer guidelines for Uganda (2 nd Edition 2008) Afr Health Sci. 2008;8:126–32. [PMC free article] [PubMed] [Google Scholar]
- 19.Azubuike SO. Awareness and Practices Towards Breast Cancer Risk Factors in Benin City, Nigeria: Paper Presented at the First International Public Health Conference in Nigeria Held at Babcock University, Ogun State Nigeria; May 12–15. 2013 Yet to be published. [Google Scholar]
- 20.Osime OC, Okojie O, Aigbekaen ET, Aigbekaen IJ. Knowledge attitude and practice about breast cancer among civil servants in Benin City, Nigeria. Ann Afr Med. 2008;7:192–7. doi: 10.4103/1596-3519.55654. [DOI] [PubMed] [Google Scholar]
- 21.Paul C, Barratt A, Redman S, Cockburn J, Lowe J. Knowledge and perceptions about breast cancer incidence, fatality and risk among Australian women. Aust N Z J Public Health. 1999;23:396–400. doi: 10.1111/j.1467-842x.1999.tb01281.x. [DOI] [PubMed] [Google Scholar]
- 22.Elsie KM, Gonzaga MA, Francis B, Michael KG, Rebecca N, Rosemary BK, et al. Current knowledge, attitudes and practices of women on breast cancer and mammography at Mulago Hospital. Pan Afr Med J. 2010;5:9. doi: 10.4314/pamj.v5i1.56186. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Alwan NA, Al-Attar WM, Eliessa RA, Madfaie ZA, Tawfeeq FN. Knowledge, attitude and practice regarding breast cancer and breast self-examination among a sample of the educated population in Iraq. East Mediterr Health J. 2012;18:337–45. doi: 10.26719/2012.18.4.337. [DOI] [PubMed] [Google Scholar]
- 24.Pöhls UG, Renner SP, Fasching PA, Lux MP, Kreis H, Ackermann S, et al. Awareness of breast cancer incidence and risk factors among healthy women. Eur J Cancer Prev. 2004;13:249–56. doi: 10.1097/01.cej.0000136718.03089.a5. [DOI] [PubMed] [Google Scholar]
- 25.Hadi MA, Hassali MA, Shafie AA, Awaisu A. Evaluation of breast cancer awareness among female university students in Malaysia. Pharm Pract (Granada) 2010;8:29–34. doi: 10.4321/s1886-36552010000100003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Cancer Research UK. Breast Cancer Risk Factors. [Last accessed on 2015 Dec 14]. Available from: http://www.cancer.org/cancer/breastcancer/detailedguide/breast-cancer-risk-factors .
- 27.Lee EO, Ahn SH, You C, Lee DS, Han W, Choe KJ, et al. Determining the main risk factors and high-risk groups of breast cancer using a predictive model for breast cancer risk assessment in South Korea. Cancer Nurs. 2004;27:400–6. doi: 10.1097/00002820-200409000-00010. [DOI] [PubMed] [Google Scholar]
- 28.Pham CT, McPhee SJ. Knowledge, attitudes, and practices of breast and cervical cancer screening among Vietnamese women. J Cancer Educ. 1992;7:305–10. doi: 10.1080/08858199209528187. [DOI] [PubMed] [Google Scholar]
- 29.Oluwatosin OA, Oladepo O. Knowledge of breast cancer and its early detection measures among rural women in Akinyele Local Government Area, Ibadan, Nigeria. BMC Cancer. 2006;6:271. doi: 10.1186/1471-2407-6-271. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Montazeri A, Vahdaninia M, Harirchi I, Harirchi AM, Sajadian A, Khaleghi F, et al. Breast cancer in Iran: Need for greater women awareness of warning signs and effective screening methods. Asia Pac Fam Med. 2008;7:6. doi: 10.1186/1447-056X-7-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Uche EE. Cancer awareness among a Nigerian population. Trop Doct. 1999;29:39–40. doi: 10.1177/004947559902900114. [DOI] [PubMed] [Google Scholar]
- 32.Odusanya OO. Breast cancer: Knowledge, attitudes, and practices of female schoolteachers in Lagos, Nigeria. Breast J. 2001;7:171–5. doi: 10.1046/j.1524-4741.1998.410062.x-i1. [DOI] [PubMed] [Google Scholar]
- 33.Oluwatosin OA, Oladepo O. Knowledge of breast cancer and its early detection measures among rural women in Akinyele Local Government Area, Ibadan, Nigeria. BMC Cancer. 2006;6:271. doi: 10.1186/1471-2407-6-271. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Ahmad S, Qureshi AN, Atta S, Gul M, Rizwan M, Ahmad S, et al. Knowledge, attitude and practice for breast cancer risk factors and screening modalities in staff nurses of Ayub Teaching Hospital Abbottabad. J Ayub Med Coll Abbottabad. 2011;23:127–9. [PubMed] [Google Scholar]
- 35.Akpor E, Akpor M, Akhator A. Breast Cancer knowledge and screening practices among Nigerian Medical Students. Internet J Health. 2009;11:2. [Google Scholar]
- 36.El Mhamdi S, Bouanene I, Mhirsi A, Sriha A, Ben Salem K, Soltani MS. Women's knowledge, attitudes and practice about breast cancer screening in the region of Monastir (Tunisia) Aust J Prim Health. 2013;19:68–73. doi: 10.1071/PY11123. [DOI] [PubMed] [Google Scholar]
- 37.Oche MO, Ayodele SO, Umar AS. Breast cancer and mammography: Current knowledge attitudes and practices of female health workers in tertiary institutions in Northern Nigeria. Public Health Res. 2012;2:114–9. [Google Scholar]
- 38.Sharma PK, Ganguly E, Nagda D, Kamaraji T. Knowledge, attitude and practices of South Indian Women Towards breast Cancer. Health Agenda. 2013;1:16–22. [Google Scholar]
- 39.Haji-Mahmoodi M, Montazeri A, Jarvandi S, Ebrahimi M, Haghighat S, Harirchi I. Breast self-examination: Knowledge, attitudes, and practices among female health care workers in Tehran, Iran. Breast J. 2002;8:222–5. doi: 10.1046/j.1524-4741.2002.08406.x. [DOI] [PubMed] [Google Scholar]
- 40.Irurhe NK, Raji SB, Olowoyeji OA, Adeyomoye AO, Ibitoye AZ, et al. Knowledge and awareness of Breast Cancer among Female secondary School Students in Nigeria. Acad J Cancer Res. 2012;5:01–5. [Google Scholar]
- 41.Secginli S, Nahcivan N. Antalya/Turkey: Proceeding of the 2nd International and 9th National Nursing Congress; 2003. Sep 07-11, Breast Cancer Screening Behavior among Women. [Google Scholar]
- 42.Muhammed SM. Knowledge, Attitude and Practice Regarding Breast Cancer among Medical Students. Bangladesh (A Master's Thesis Protocol Studies) University Umea: Department of Public Health and Clinical Studies. 2007. [Last accessed on 2015 Dec 14]. Available from: http://www.cancer.gov/cancertopics/pdq/treatment/breast/patient/page2 .