

Abstract
The aim of the study was to investigate current situation of postoperative pain management in medical institutions in Shandong Province.A questionnaire was developed on the basis of guidelines of acute pain and pain quality assessment scale. The questionnaire was used to obtain information regarding the nature and scale of the medical institution, structure of pain management organization, implementation of pain assessment, and analgesic techniques and processes used in clinical practice. A multistage stratified and cluster sampling method was employed to investigate the current situation of postoperative pain management in 168 medical institutions in Shandong Province.
For acute pain service (APS), 32% of the hospitals established postoperative pain management organizations similar to APS. For pain evaluation, 57.1% of the hospitals evaluated pain as the fifth vital sign, and 47.0% of the hospitals evaluated pain at rest and during activity. Furthermore, 43.0% of the surveyed hospitals employed patient-controlled analgesia mode, of which hospitals employing brachial plexus block, lumbar plexus block, and femoral nerve block analgesia accounted for 5.0%, 1.0%, and 4.0%, respectively. The survey revealed that 51.0% of the hospitals educated patients about pain and pain management, of which patients were postoperatively educated by ward nurses in 5.0% and patients were educated by APS during ward rounds in 2.0%.
There is a lack of standardized postoperative pain management, the involvement of nurses in pain management is scarce, and the pain assessment and education and application of advanced analgesic management techniques were found to be inadequate in medical institutions in Shandong Province.
INTRODUCTION
With the increasing popularity of minimally invasive technology over the last few decades, there is an increasing number of studies investigating the mechanisms of analgesia. Research has delved deep into postoperative pain and pain relief, including the mechanism of acute pain, the implementation of multimodal analgesia, acute pain service (APS), as well as established guidelines for postoperative acute pain management, and achieved enormous progress in this field. Despite this, postoperative patients still suffer from moderate and severe pain.1–3 A retrospective survey of postoperative pain management of 2252 patients carried out across 25 hospitals in Germany in 2010 revealed that the incidence of moderate and severe pain in postoperative patients at rest and activity was 29.5% and >50.0%, respectively.4 There is evidence demonstrating that the establishment of APS can enable medical staff to employ evidence-based medicine for pain management, which can achieve broader and more flexible selection of analgesic measures as well as regulate the postoperative pain management and improve analgesia and satisfaction in patients.5,6
Although an increasing number of national and international researchers are focusing on postoperative pain and hospitals also provide postoperative analgesia, there is a significant difference in the structure and function of different APS organizations: although some organizations offer pain treatment follow-up and good pain education for patients and nurses, others only provide analgesic measures because of lack of manpower or financial resources.7 Thus far, no studies have investigated the development status of APS and postoperative pain management in medical institutions in Shandong Province. Therefore, this article conducted a survey and statistical analysis on the status of postoperative pain management in medical institutions in Shandong Province to identify problems and propose appropriate suggestions for improving analgesia services to postoperative patients.
MATERIALS AND METHODS
Subjects
This study was approved by the Anesthesia Quality Control Center in Shandong Province. Four prefecture-level cities were randomly selected each from the eastern, southern, western, northern, and central regions of the Shandong Province, resulting in a total of 20 cities for this analysis. From these cities, 168 hospitals with medical practice licenses were selected, from which the directors of the Anesthesiology Department or experienced anesthesiologist with a working experience of >5 years were contacted for participation in this study.
Methods
Questionnaire Setting
The Current Status of Postoperative Pain Management questionnaire was developed on the basis of the guidelines of acute pain and pain assessment scale.1–3 The questionnaire consisted of 2 parts. The first part contained questions pertaining to general information such as information of the person completing the form, and the nature and scale of the medical institution. The second part of the questionnaire contained 7 large entries and 50 small items, and contained questions about postoperative pain management, such as the preoperative preparation for pain management, structure of postoperative pain management organization, implementation of pain assessment and analgesic techniques, and acute pain management procedure.
Reliability and Validity Testing
Five pain management experts were invited to evaluate the validity of the questionnaire, and the content validity index was 0.923. Twenty hospitals were selected to conduct preliminary trials for the questionnaire, and the tested Cronbach α coefficient was 0.896.
Dispatching and Receiving the Questionnaire
The questionnaires were uniformly dispatched and received a week later by investigators. Upon receipt, if there were omissions or any of the items failed to meet the requirements in the form, the respondents were required to add and amend the items to ensure integrity and accuracy of the data.
Statistical Analysis
The collected questionnaire data were checked by 2 investigators and input into the EpiData database; at this time, timely correction was achieved by verifying with the raw data in case of deviations. The Excel sheets were exported for statistical analysis using SPSS version 17.0 (SPSS Inc, Chicago, IL).
RESULTS
A total of 168 questionnaires were dispatched and answered.
General Information of Surveyed Hospitals
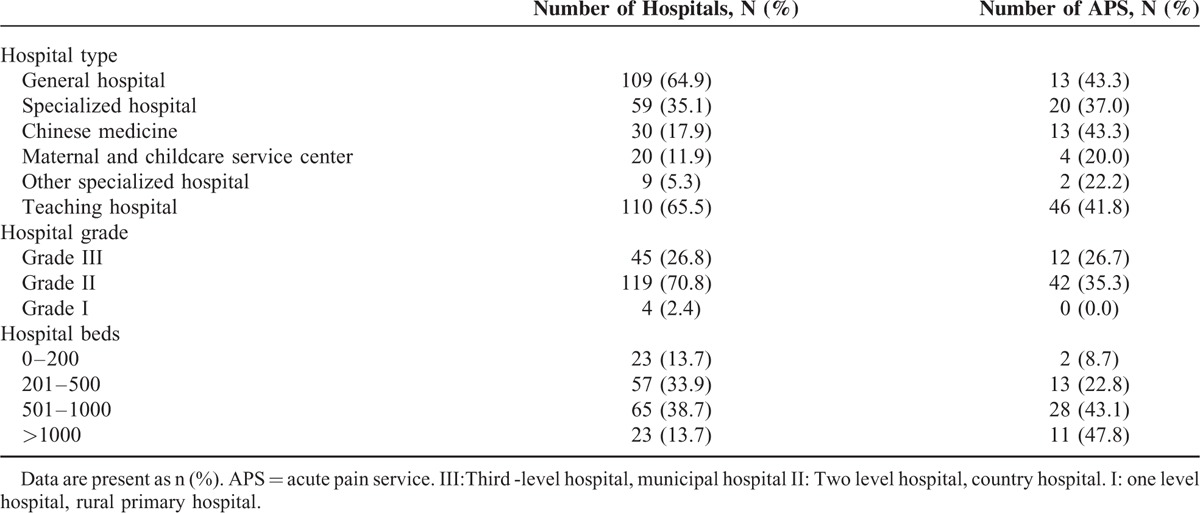
A total of 625 hospitals in Shandong Province were included. Of these, 81 were Grade III hospitals, 426 were Grade II hospitals, and 118 were Grade I hospitals. A total of 168 hospitals were included in this survey, accounting for 25.0% of the total number of hospitals in Shandong Province. Of these, 45 were Grade III hospitals, accounting for 55.6% of the total number of tertiary hospitals, 119 Grade II hospitals, accounting for 28.0% of the total number of second-class hospitals, and 4 Grade I hospitals, accounting for 3.4% of the total number of the Grade I hospitals (Table 1).
TABLE 1.
General Information of Hospitals
Construction of Postoperative Pain Management Organization
Management Mode of Postoperative Pain
A total of 54 hospitals (32%) had established pain management organizations similar to APS. Among these 54 hospitals, 43 (80.0%) employed an anesthesiologist-based management mode, 4 (7.4%) adopted a pain resource nurse-based mode, and 7 (13.0%) employed a nurse-based mode with supervision by anesthesiologists.
APS Demographics and Funding
The personnel comorising the typical APS included anesthesiologists in 54 hospitals (100%), advanced practice nurse in 6 hospitals (11.1%), the ward nurses in 10 hospitals (18.5%), surgeons in 16 hospitals(29.6%), and pharmacists in 10 hospitals (18.5%). However, no psychologists or physical therapists were involved in APS of any of these hospitals (Figure 1).
FIGURE 1.
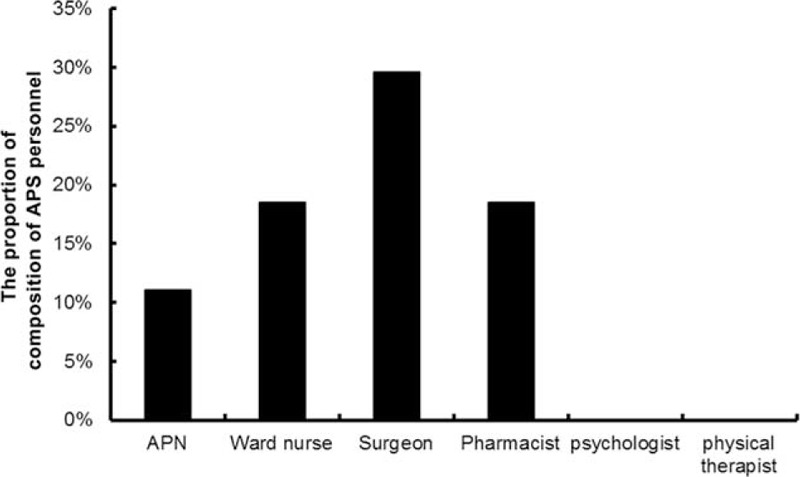
Composition of APS personnel. APN = advanced practice nurse, APS = acute pain service.
Protocols of Postoperative Pain Management
A total of 147 hospitals (87.5%) were found to have established pain protocols: 10 (6.8%) included sedation evaluation, 27 (18.4%) conducted pain evaluation, 26 (17.7%) set up an APS consulting group for acute pain-related problems, 23 hospitals (15.6%) mentioned strategies of non-drug therapy, and 10 hospitals (6.8%) mentioned conducting management for patients with postoperative acute pain at night and during holidays. Furthermore, 144 hospitals (85.7%) required patients to sign an analgesia protocol and agreement preoperatively, and pain service management during holidays were only provided in 16 (9.5%) of the hospitals with APS organization.
Implementation of Pain Assessment and Reassessment
Ninety-six hospitals (57.1%) carried out pain assessment as the fifth vital sign, and 70 hospitals (47.0%) evaluated pain at rest and movement, and 70 hospitals (47.0%) conducted pain assessment after pain intervention.
Analgesia Method
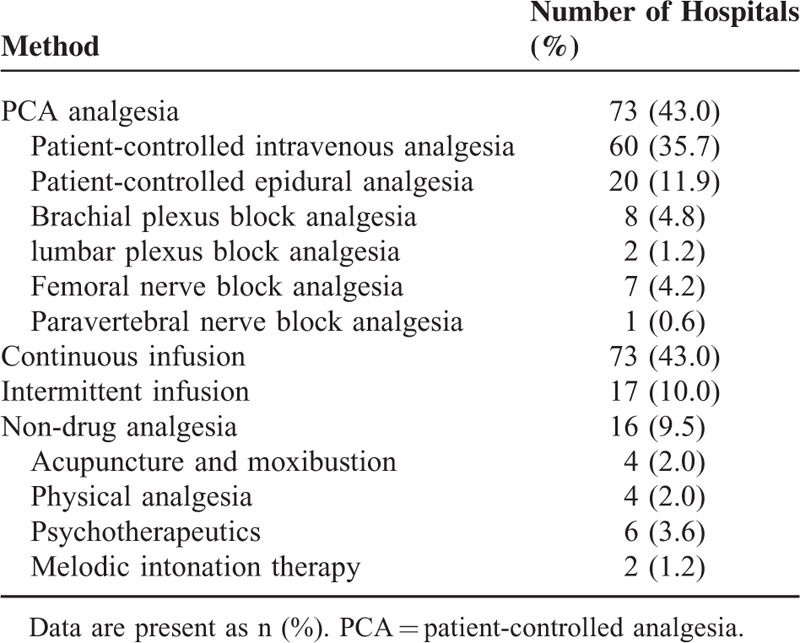
Seventy-three hospitals (43.0%) employed patient-controlled analgesia (PCA), 73 hospitals (43.0%) adopted continuous-infusion analgesia, 17 hospitals (10.0%) adopted intermittent intramuscular analgesia, 4 hospitals (2.0%) adopted physical analgesia, 4 hospitals (2.0%) adopted acupuncture and moxibustion, 6 hospitals (3.6%) employed psychotherapeutics (such as relaxation training, deep breathing, and meditation), and 2 hospitals (1.2%) adopted music therapy (Table 2).
TABLE 2.
Method of Postoperative Analgesia
PCA Approaches
Among the 73 hospitals that used PCA analgesia, 60 (35.7%) implemented patient-controlled intravenous analgesia, 20 hospitals (11.9%) adopted patient-controlled epidural analgesia, 18 hospitals (10.8%) adopted patient-controlled peripheral nerve block analgesia, 8 hospitals (4.8%) adopted brachial plexus block analgesia, 2 hospitals (1.2%) adopted lumbar plexus block analgesia, 7 hospitals (4.2%) adopted femoral nerve block analgesia, and only 1 hospital (0.6%) adopted paravertebral nerve block analgesia (Table 2).
Multimodal Analgesia and Percentage of use of Analgesic Drugs
A total of 60 hospitals (35.7%) adopted multimodal analgesia and the percentage of use of analgesic drugs used was as follows: for opioids, fentanyl (80.0%), sufentanil (70.0%), morphine (35.0%), pethidine hydrochloride (11.0%), and tramadol (7.0%). The proportions of nonsteroidal anti-inflammatory drugs are as follows: flurbiprofen (6.0%), parecoxib (1.0%), ketorolac (7.0%), and acetaminophen (2.0%). The proportions of other analgesics were dezocine (15.0%), nefopam (5.0%), and lappaconitine (13.0%), as shown in Figure 2.
FIGURE 2.
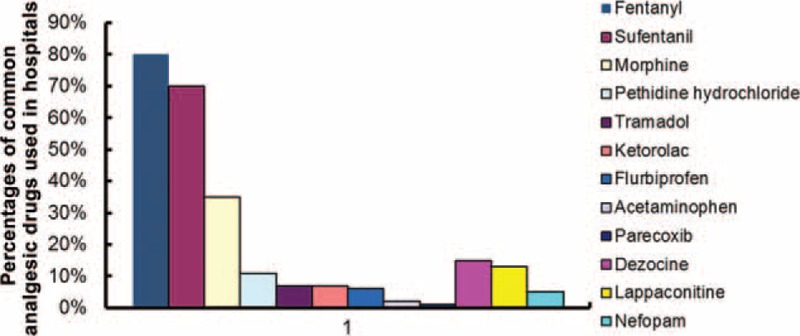
Percentages of common analgesic drugs used in hospitals.
Pain Management Education
Presence and Timing of Education
Only 86 (51.0%) respondents mentioned using pain education to patients, of which 58 hospitals (66.0%), Pain education terms such as:how to use the PCA; when should press the button? 13 hospitals (14.0%) educated the patients after entering the operating room; 13 (14.0%), in the postanesthesia care unit); and 5 (5.0%), when the patient returns to the ward. Only 2 hospitals mentioned that pain control education was disseminated during ward rounds (Figure 3).
FIGURE 3.
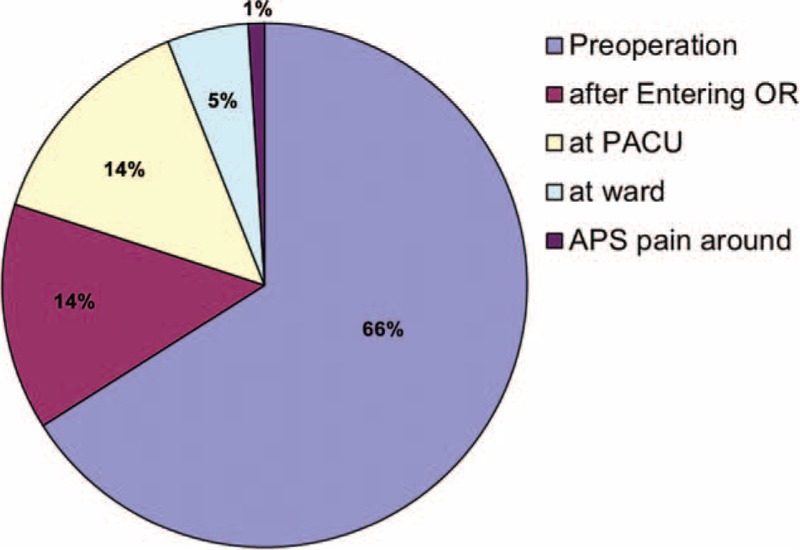
Pain management education time. APS = acute pain service, OR = operating room, PACU = postanesthesia care unit.
Educating Patients About Pain Management
Of the 86 hospitals that educated patients about pain and pain management, it was conducted by anesthesiologists in 58 hospitals (34.5%), it was conducted by surgeons in 4 hospitals (2.4%), it was conducted by ward nurses in 18 hospitals (11%), and it was carried out by APS in only 4 hospitals (3.1.%), as shown in Figure 4.
FIGURE 4.
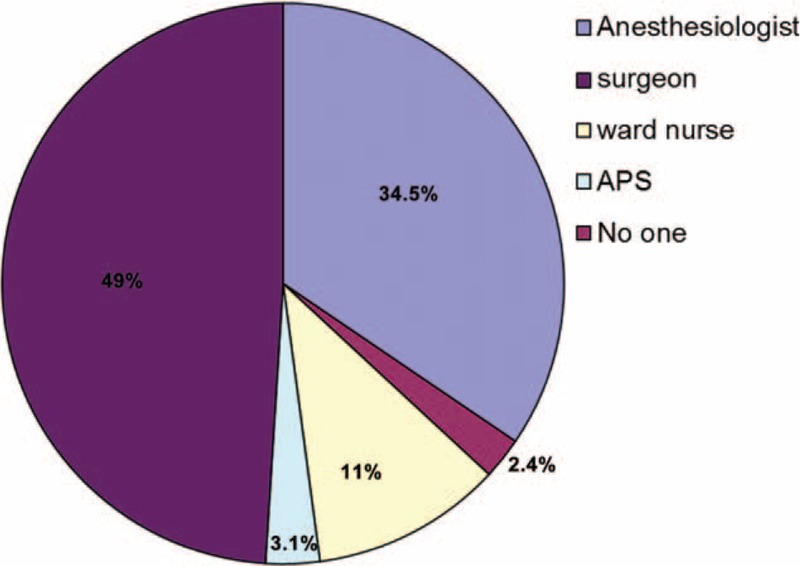
Personnel involved in pain management. APS = acute pain service.
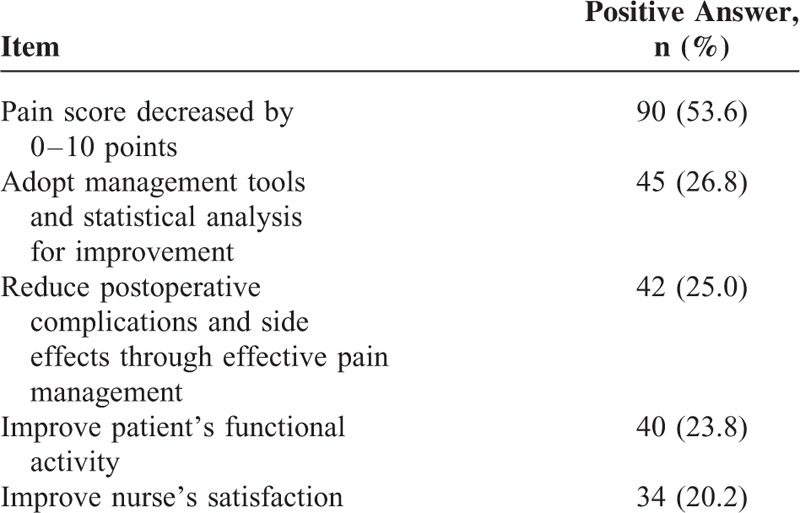
Criteria of Pain Improvement
Among the hospitals that responded positively to the question “how to criteria pain improvement ?,” 90 (53.6%) responded hospitals measured improvement in pain management by improved pain scores of patients, 45 (26.8%)responded hospitals measured improvement in pain management by higher patients’ satisfaction rating 42 (25%) hospitals by fewer postoperative complications and side effects from treatment, 40 (23.8%) hospitals by improved patient's functional activity, and 34 (20.2%) hospitals by improved nurse's satisfaction rating, as shown in Table 3.
TABLE 3.
How to Achieve Continuous Quality Improvement for Pain Management (n = 168)
DISCUSSION
These years, there are only a few studies evaluating the structure and function from the United States and Europe.7,8 However, the current status of APS in China remains limited. This study investigated the structure, existence, and responsibilities of APS teams and the reported implementation of the postoperative pain management. This article provides valuable advice that may provide guidance toward improved functioning of an APS and improved pain management in postoperative patients.
Insufficient Organizations for Postoperative Pain Management, Different APS Construction and Personnel Composition, Lack of Unity and Standard
Recent studies have reported that 90% of the hospitals in Netherlands, 75% of the hospitals in the United States, 77% of the hospitals in Ireland established APS pain management organizations in 2014, 2011, and 2007, respectively.7,9 However, among the 168 medical institutions in Shandong Province in this survey, only 32% have set up pain management organizations similar to APS, and these organizations were characterized by uneven and different functionalities and personnel composition. Furthermore, only 11.1% of these organizations accounted for pain management involving anesthetists and nurses specialized in pain management, and none of the hospitals involved psychologists and physical therapists in their pain management organizations.
APS is successful because it is an organization to provide effective pain management through multidisciplinary cooperation.10 However, a unified quality assessment system to evaluate the quality of postoperative control of APS is lacking. This survey found that 53.6% of the hospitals relied on the patients’ pain score to evaluate the postoperative analgesic efficacy, and only 25% of the surveyed hospitals considered the patient's effective functional activities, incidence of postoperative side effects, and application of quality management tools as indices of continuous quality improvement. Moreover, although 84.5% of the hospitals have pain management systems in place, the systems were not perfect, and sedation evaluation systems had been implemented in only 6.8% of the surveyed hospitals.
Lack of Effective Pain Assessment
A previous survey involving 105 hospitals in the United States found that 97.2% of the hospitals conducted evaluation of pain at rest in patients, and 63% of the hospitals evaluated the pain during activity.7 A domestic survey of nurses in 76 hospitals between 2011 and 2012 found that as many as 71.2% of the surveyed nurses did not focus on the effect of pain on the functional activity of patients.11 The same survey revealed that 57.1% of the hospitals assessed pain as the fifth vital sign, and 47% assessed the pain at rest and activity. In recent years, with the issuance of detailed rules for hospital accreditation, particularly the issuance of the guidelines regarding acute pain, has resulted in an increased focus by hospitals on pain management. Nearly half of the hospitals carry out pain assessment not only at rest but also during activity and after drug intervention. It is clear that pain scores alone should not be used to manage postoperative pain. Therefore, we should increase emphasis on use of patient outcomes to guide pain therapy rather than pain scores alone.
Shortcoming in the Analgesic Methods and Treatment Employed
Epidural block and peripheral nerve block are known to decrease the degree of postoperative pain. The pain guidelines of many countries have suggested that nerve block can be widely used in many surgeries, especially in patients who are already aware of severe postoperative pain.12 Compared with intravenous opioids, there is a significantly lower incidence of complications in epidural analgesia, indicating that the efficacy of postoperative epidural analgesia was better than that of intravenous analgesia, and the incidence of severe complications could be very small if proper regulations were implemented.13 However, this survey found that only 34% of the hospitals employed epidural block analgesia, and very few hospitals used brachial plexus block, femoral nerve block, and lumbar plexus nerve block analgesia.
The guidelines proposed by the American Society of Anesthesiologists (ASA) state that injection via the intramuscular route and pethidine hydrochloride injection are not recommended for analgesic treatment. However, the present survey found that 11.0% of the hospitals still considered pethidine hydrochloride as the common analgesic drugs, and only 35.7% of the hospitals implemented multimodal analgesia. A large number of studies have confirmed that multimodal analgesia has many advantages,3,14 and it is recommended by the guidelines of ASA and other institutions.4 Some studies have also shown that music and relaxation therapy can effectively alleviate pain.15,16 This survey found that only 3.6% of the hospitals implemented psychotherapy, and only 1.2% of the hospitals selected melodic intonation therapy as a part of the analgesic therapy.
Participation of Nurses in Pain Management
International studies have reported that nurses are the first to understand various pain symptoms in patients, as they spend more time with the patients during their stay at the hospital. Nurses play an important role in pain control and pain management, including communication and coordination, implementing analgesia, nursing measures, education, and training, correcting the patients’ misconception of pain, ensuring the effectiveness of pain management, observing the patients’ response to pain intervention, and ensuring patient safety.9,17,18 However, this survey found that only 11.0% of nurses participated in pain management.
Nurses specialized in pain management are important members of APS organizations. Not only can they implement advanced analgesic techniques and provide technique support and theoretical training to ward nurses, these specialized nurses can also be responsible for developing pain-related responsibilities, systems, and detailed rules to regulate pain assessment and recording. Such nurses can then act as links and bridges in multidisciplinary cooperation, thereby promoting communication between anesthetists, surgeons, and ward nurses.16 However, this survey found that only 6 of the surveyed hospitals had nurses specialized in pain management.
APS Management Mode
There are 3 management modes of APS locally and internationally. The first is an anesthetist-based management mode, which can provide patients with advanced analgesic techniques. However, as anesthetists are primarily responsible for daily anesthesia, they may not provide adequate attention to postoperative pain management, resulting in poor quality. The second mode is the nurse-based management mode, which can ensure more patients receiving adequate postoperative analgesia services. However, the guidance and participation of anesthetists is lacking in this mode, and poor pain management can occur in this mode as the nurses cannot fully employ advanced analgesic techniques without appropriate guidance. The last mode is the nurse-based anesthesiologist-supervised mode. This mode combines the advantages of the above 2 methods, ensuring that more patients receive adequate postoperative analgesia and advanced techniques can also be employed, avoiding many of the above-mentioned shortcomings.19 Domestic studies have shown that the patient satisfaction rate of postoperative analgesia can be as high as 96.4% after implementation of the nurse-oriented management mode with the anesthesiologist's guidance. In these studies, there was no incidence of severe complications of respiratory depression, whereas timely and effective treatment could be achieved in other complications such as insufficient analgesia, abdominal distension, nausea and vomiting, and cutaneous pruritus.20,21 This survey found that 80% of the APS systems employed the anesthetist-based management mode.
Lack of Pain Management Education
Timely and effective pain control education provided to patients has been shown to alleviate anxiety, improve the level of comfort, mental attitude, and reduce the duration of hospital stay.22,23 The present survey found that only 51% of the hospitals carried out pain education, and this education occurred only during the preoperative stage. In general, the pain is the most intense on the day and night after the operation. Therefore, knowledge about pain and pain management should be provided to patients to patients’ individual difference, and customized education should be provided in the appropriate language and at the appropriate times.24
Suggestions for Effective Postoperative Pain Management in China
To improve the quality of postoperative pain management in China, it is necessary to develop the corresponding management disciplines in Chinese hospitals, and improve postoperative pain management practices through in-service education and quality improvement. First, a standard postoperative pain management organization and management service system should be established. The role of nurses should be given more importance and they should be provided with the appropriate training regarding pain and pain management. Misconceptions of the clinical nurses regarding pain should be corrected so that they can provide better services to postoperative patients. Second, the standardized training of pain and pain management techniques of clinical physicians and anesthetists should be improved. Advanced analgesic techniques should be applied in clinical practice, and multimodal analgesia should be implemented to improve patient satisfaction and comfort. Finally, research results showed that the assessment system for acute pain quality management recommended by the APS is suitable to evaluate the quality of pain management in China. Therefore, Chinese health administrative institutions and academic organizations can develop a quality evaluation standard for pain management and help hospitals to improve their systems to achieve high-quality pain management.25
Limitations
This survey was completed by personnel in the anesthesiology department; therefore, there may be some cognitive deviations about pain management in the ward. In addition, detailed investigation has not been conducted on the expenses incurred by postoperative pain management organizations. Finally, this survey included only medical staff, and no survey design has been developed for patients with postoperative pain; therefore, further research surveying patients on postoperative pain management is necessary.
CONCLUSIONS
This survey objectively revealed the status of postoperative pain management in medical institutions in Shandong Province, including personnel composition, management status, pain assessment, analgesic techniques, and workflow management. The study revealed that there is a lack of standardized postoperative pain management, medical staff did not have sufficient focus on managing postoperative pain, and nurses were rarely involved in pain management, and there is a need for applying advanced analgesic techniques and educating patients regarding pain management. It is recommended to set up standardized postoperative pain management organizations and a management evaluation system, give more importance to the role of nurses in pain management, conduct timely and effective propaganda and education to patients, implement multimodal analgesia, and standardize postoperative pain management, consequently improving the satisfaction and comfort of postoperative patients.
Acknowledgments
We are grateful to the Anesthesia Quality Control Center of Shandong Province, Yichang Renfu Pharmaceutical Company, and the participating hospitals for their support and assistance.
Footnotes
Abbreviations: APN = advanced practice nurse, APS = acute pain service, ASA = American Society of Anesthesiologists, PACU = post anesthesia care unit, PCA = patient-controlled analgesia.
The authors declare that they have no conflict of interest.
REFERENCES
- 1.Fletcher D, Fermanian C, Mardaye A, et al. A patient-based national survey on postoperative pain management in France reveals significant achievements and persistent challenges. Pain 2008; 137:441–451. [DOI] [PubMed] [Google Scholar]
- 2.Sommer M, de Rijke JM, van Kleef M, et al. The prevalence of postoperative pain in a sample of 1490 surgical inpatients. Eur J Anaesthesiol 2008; 25:267–274. [DOI] [PubMed] [Google Scholar]
- 3.American Society of Anesthesiologists Task Force on Acute Pain M. Practice guidelines for acute pain management in the perioperative setting: an updated report by the American Society of Anesthesiologists Task Force on Acute Pain Management. Anesthesiology 2012; 116:248–273. [DOI] [PubMed] [Google Scholar]
- 4.Maier C, Nestler N, Richter H, et al. The quality of pain management in German hospitals. Dtsch Arztebl Int 2010; 107:607–614. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Kishore K, Agarwal A, Gaur A. Acute pain service. Saudi J Anaesth 2011; 5:123–124. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Hu P, Owens T, Harmon D. A survey of acute pain services in teaching hospitals in the Republic of Ireland. Ir J Med Sci 2007; 176:225–228. [DOI] [PubMed] [Google Scholar]
- 7.Nasir D, Howard JE, Joshi GP, et al. A survey of acute pain service structure and function in United States hospitals. Pain Res Treat 2011; 934932. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Rawal N. Organization, function, and implementation of acute pain service. Anesthesiol Clin North Am 2005; 23:211–225. [DOI] [PubMed] [Google Scholar]
- 9.van Boekel RL, Steegers MA, Verbeek-van Noord I, et al. Acute pain services and postsurgical pain management in the Netherlands: a survey. Pain Pract 2015; 15:447–454. [DOI] [PubMed] [Google Scholar]
- 10.Goldstein DH, VanDenKerkhof EG, Blaine WC. Acute pain management services have progressed, albeit insufficiently in Canadian academic hospitals. Can J Anaesth 2004; 51:231–235. [DOI] [PubMed] [Google Scholar]
- 11.Ying Ge T, Konstantatos AH, Cai Fang Z, et al. A cross-sectional exploratory survey of knowledge, attitudes and daily self-reported pain assessment practice among nurses in Mainland China. Pain Med 2013; 14:1468–1476. [DOI] [PubMed] [Google Scholar]
- 12.Gerbershagen HJ, Aduckathil S, van Wijck AJ, et al. Pain intensity on the first day after surgery: a prospective cohort study comparing 179 surgical procedures. Anesthesiology 2013; 118:934–944. [DOI] [PubMed] [Google Scholar]
- 13.Popping DM, Zahn PK, Van Aken HK, et al. Effectiveness and safety of postoperative pain management: a survey of 18 925 consecutive patients between 1998 and 2006 (2nd revision): a database analysis of prospectively raised data. Br J Anaesth 2008; 101:832–840. [DOI] [PubMed] [Google Scholar]
- 14.Gaskell H, Derry S, Moore RA, et al. Single dose oral oxycodone and oxycodone plus paracetamol (acetaminophen) for acute postoperative pain in adults. Cochrane Database Syst Rev 2009; 8:CD002763. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Smith CA, Levett KM, Collins CT, et al. Relaxation techniques for pain management in labour. Cochrane Database Syst Rev 2011; 7:CD009514. [DOI] [PubMed] [Google Scholar]
- 16.Huang ST, Good M, Zauszniewski JA. The effectiveness of music in relieving pain in cancer patients: a randomized controlled trial. Int J Nurs Stud 2010; 47:1354–1362. [DOI] [PubMed] [Google Scholar]
- 17.Zhao J, Jing C. The role of nurse in pain management. Chinese J Nurs 2009; 44:383–384. [Google Scholar]
- 18.Yang J, Liu W, Zhang Y, et al. Research progress on training for pain specialist nurses in China and in foreign countries. Chinese Nurs Educ 2010; 7:510–512. [Google Scholar]
- 19.Shapiro A, Zohar E, Kantor M, et al. Establishing a nurse-based, anesthesiologist-supervised inpatient acute pain service: experience of 4,617 patients. J Clin Anesth 2004; 16:415–420. [DOI] [PubMed] [Google Scholar]
- 20.Liu D, Zhang J, Chen X. Effects of APS management in patients after surgery. Nurs Res 2012; 26:2751–2753. [Google Scholar]
- 21.Liu D, Yan H, Ren X. Construction and practice of acute pain service organization. J Nurs 2012; 27:68–70. [Google Scholar]
- 22.Gleeson E, Carryer J. Nursing staff satisfaction with the acute pain service in a surgical ward setting. Nurs Prax N Z 2010; 26:14–26. [PubMed] [Google Scholar]
- 23.Shiqing L, Kangqing X, Peng Y, et al. Improving the quality of acute pain services: experiences of treatment of 5212 patients. Anestezjol Intens Ter 2009; 41:219–223. [PubMed] [Google Scholar]
- 24.Pan J, Fan L. Efficacy of postoperative pain intervention. Chinese J Pract Nurs 2011; 27:16–17. [Google Scholar]
- 25.Tong Y, Liu M, Liu D. Quality evaluation and analysis of postoperative pain management in 5 tertiary hospitals. Chinese J Hosp Admin 2013; 29:24–28. [Google Scholar]