

Abstract
Background. Given high rates of gun ownership among older adults, geriatric providers can assess firearm safety practices using a “5 Ls” approach: Locked; Loaded; Little children; feeling Low; and Learned owner. This study describes gun access and the “5 Ls” among US older adults. Methods. Data on the “5 Ls” from the Second Injury Control and Risk Survey (ICARIS-2), a national telephone survey conducted by the Centers for Disease Control and Prevention, were analyzed. Weighted variables were used to generate national estimates regarding prevalence of gun ownership and associated gun safety among older adults (≥55 years). Results. Of 2939 older adults, 39% (95% CI 37%–42%) reported ≥1 gun stored at home. Among those with guns at home, 21% (95% CI 18–24%) stored guns loaded and unlocked; 9.2% (95% CI 6.6–12%) had ≥1 child in household; 5.1% (95% CI 3.5–6.8%) reported past-year suicidal ideation and 3.6% (95% CI 2.1–5.2%) reported history of a suicide attempt; and 55% (95% CI 51–59%) stated that ≥1 adult had attended firearm safety workshop. Conclusion. Some older adults may be at elevated risk of firearm injury because of storage practices, suicidal thoughts, or limited safety training. Future work should assess effective approaches to reduce the risk of gun-related injuries among older adults.
1. Introduction
Gun safety among older adults is relevant to medical and public health professionals, given that older adults experience changes in memory, function, and mood that may increase risks of gun-related injuries and death, including suicide [1, 2]. Older adults have high rates of gun ownership [3], potentially placing individuals, families, and home healthcare providers at risk [4]; injury risk rises when guns are stored loaded and unlocked [5]. Older adults have high rates of suicide, and gun access is a risk factor for suicide [6–8]. Healthcare practitioners may play an important role in assessing gun safety and risk of injury in older adults [4, 9–11].
However, currently there are limited data on gun safety among older adults who own guns [12, 13]. Recent work proposed that clinicians ask older adults “Is there a firearm in the home?” and use a “5 Ls” framework to assess safety: (1) Is it Loaded? (2) Is it Locked? (3) Are Little children present? (4) Is the operator feeling Low? (5) Is the operator Learned? [10]. Using the “5 Ls” framework, this study employs the national Second Injury Control and Risk Survey (ICARIS-2) to examine the prevalence and characteristics of older adult gun owners, as well as gun safety related to firearm storage, suicidal thoughts, presence of children, and firearm safety training.
2. Methods
2.1. Survey Design and Participants
The Centers for Disease Control and Prevention conducted the ICARIS-2 survey between July 2001 and February 2003 [14]. The cross-sectional, random-digit-dial telephone survey included English- and Spanish-speaking adults aged ≥18 years in US households. The response rate was 48% [14]. This analysis includes adults aged ≥55 (n = 29390), who accounted for 29% of all respondents. Adults aged 55 years and older were chosen for this analysis because the survey was conducted approximately 10 years ago. Thus, inclusion of individuals 55 years and older reflects a US population cohort that are adults aged 65 and older at the time of this analysis. Analysis was at the level of the individual; survey weighting variables were used to generate national estimates. Weighting was conducted according to the recommended methods as described and recommended for interpretation of survey results [14]. This study was approved by the Colorado Multiple Institutional Review Board.
2.2. Variables
Demographic characteristics included age, gender, self-described race, and Hispanic ethnicity. Household characteristics included living alone, presence of children (<18 years), and annual household income. Presence of a firearm was based on the question “Any firearms kept in/around home in the past 12 months?” Participants who did not know (n = 5) or declined to answer (n = 64) were excluded.
Using the “5 Ls” framework, analysis addressed firearm storage (“Locked” and “Loaded”); presence of children in the home (“Little children”); suicidal thoughts and prior attempts (“feeling Low”); and prior firearm safety training (“Learned operator”). Survey wording (“Were any firearms ever kept loaded and unlocked while stored in or around your home”?) prevented separation of locked and loaded in terms of storage patterns.
2.3. Statistical Analysis
All responses were summarized using weighted proportions and 95% Confidence Intervals (CI). Characteristics of respondents with and without firearms at home were compared using Chi Square analyses. Analyses were performed using Stata, version 11.2, with appropriate operations for weighted survey data.
3. Results
The survey respondents were 56% female, and 22% were at least 75 years old at the time of the survey. In older adults aged ≥55 years, 39% (95% CI 37%–42%) reported ≥1 gun stored in or around the home. Figure 1 shows the percentages of individuals with at least 1 firearm in the home by age group. Of individuals with a gun at home, 65% (95% CI 62%–69%) said ≥1 was a handgun and 69% (95% CI 65%–72%) reported being the owner of the gun, with a higher proportion of men (92%, 95% CI 89–94%) than women (40%, 95% CI 33–46%) reporting being the owner (p < 0.001).
Figure 1.
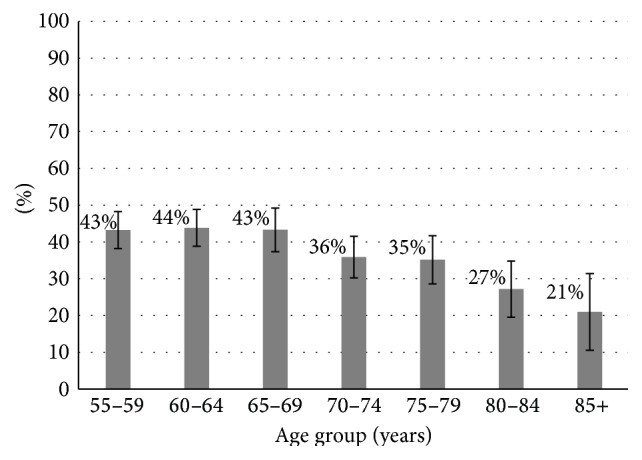
Older adults with ≥1 gun at home, by age group (N = 2939). Weighted proportion of older adults with ≥1 firearm in the home, by age group. Error bars represent 95% Confidence Intervals.
Proportions of respondents reporting a gun at home was higher in the younger cohorts (ages 55–64 and 65–74) and among respondents who were white, had less formal education, and had income above the poverty level (Table 1). Firearm presence at home was lower among individuals living alone. The prevalence of households with a gun varied by region, with the highest levels in the Mountain region (55%, 95% CI 46%–65%) and lowest in the Mid-Atlantic region (23%, 95% CI 18%–28%).
Table 1.
Characteristics of older adults by presence of ≥1 gun stored in or around the home.
| Gun in the home | No gun in the home | Total | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Weighted %a | 95% CI | Weighted %a | 95% CI | Weighted %a | 95% CI | ||||
| Age group∗∗ | |||||||||
| 55–64 | 47 | 43 | 51 | 39 | 36 | 42 | 42 | 40 | 45 |
| 65–74 | 36 | 33 | 40 | 36 | 33 | 39 | 36 | 34 | 38 |
| 75–84 | 15 | 13 | 18 | 21 | 19 | 23 | 19 | 17 | 21 |
| 85+ | 1.7 | 0.7 | 2.6 | 4.1 | 3.0 | 5.2 | 3.1 | 2.4 | 3.9 |
| Female | 44 | 40 | 48 | 63 | 61 | 66 | 56 | 54 | 58 |
| Raceb | |||||||||
| White∗∗ | 89 | 86 | 92 | 79 | 77 | 82 | 83 | 81 | 85 |
| Black∗∗ | 6.0 | 4.1 | 7.9 | 12 | 10 | 14 | 9.6 | 8.2 | 11 |
| Other | 2.7 | 1.5 | 3.9 | 4.5 | 3.1 | 5.9 | 3.8 | 2.8 | 4.8 |
| Live alone∗∗ | 16 | 14 | 18 | 30 | 28 | 32 | 25 | 23 | 26 |
| Income below poverty level∗ | 43 | 39 | 47 | 48 | 45 | 52 | 46 | 44 | 49 |
| Education∗ | |||||||||
| College or higher | 34 | 30 | 37 | 36 | 33 | 39 | 35 | 33 | 37 |
| High school | 26 | 23 | 30 | 24 | 21 | 27 | 25 | 23 | 27 |
| Below high school | 40 | 36 | 44 | 40 | 37 | 43 | 40 | 38 | 42 |
| Census division (with included states)∗∗ | |||||||||
| New England (CT, MA, ME, NH, RI, VT) | 4.7 | 2.9 | 6.4 | 6.7 | 5.1 | 8.3 | 5.9 | 4.7 | 7.1 |
| Mid-Atlantic (NJ, NY, PA) | 8.9 | 6.8 | 11 | 20 | 18 | 22 | 15 | 14 | 17 |
| East North Central (IL, IN, MI, OH, WI) | 15 | 12 | 17 | 16 | 13 | 18 | 15 | 14 | 17 |
| West North Central (IA, KS, MN, MO, ND, NE, SD) | 7.2 | 5.2 | 9.3 | 6.9 | 5.5 | 8.4 | 7.1 | 5.9 | 8.3 |
| South Atlantic (DC, DE, FL, GA, MD, NC, WV, SC, VA) | 20 | 17 | 23 | 18 | 16 | 21 | 19 | 17 | 21 |
| East South Central (AL, KY, MS, TN) | 8.6 | 6.5 | 11 | 4.6 | 3.4 | 5.8 | 6.2 | 5.1 | 7.3 |
| West South Central (AR, LA, OK, TX) | 13 | 10 | 15 | 8.1 | 6.4 | 9.7 | 9.8 | 8.5 | 11 |
| Mountain (AZ, CO, ID, MT, NM, NV, UT) | 9.6 | 7.1 | 12 | 5.0 | 3.8 | 6.3 | 6.8 | 5.6 | 8.1 |
| Pacific (AK, CA, HI, OR, WA) | 14 | 11 | 16 | 15 | 13 | 17 | 14 | 12.6 | 16.1 |
N = 2,939. CI: Confidence Interval. aSurvey data includes weighting variables for generation of national estimates. bMultiple responses allowed per participant; ∗ p ≤ 0.05; ∗∗ p ≤ 0.001 under Pearson chi-square tests; numbers may not add to 100% due to rounding.
Figure 2 shows the prevalence of potential gun safety risks associated with having a gun at home using the “5 Ls” framework [10]. While the prevalences of children in the household, suicidal ideation, and history of suicide attempt were low, one-fifth (21%, 95% CI 18–24%) of gun owners reported having kept the gun loaded and unlocked at some point over the past year. Those with a child in the household were more likely to report safe gun storage (i.e., unloaded and locked; 90%, 95% CI 82–98%; versus 77%, 95% CI 73–80%; p < 0.01). Only about half (55%; 95% CI 51–59%) of respondents with a gun at home reported that at least one adult household member had attended a firearm safety workshop or class. There was no association between storing a gun loaded and unlocked and having at least one adult who had attended gun safety training (p = 0.8).
Figure 2.
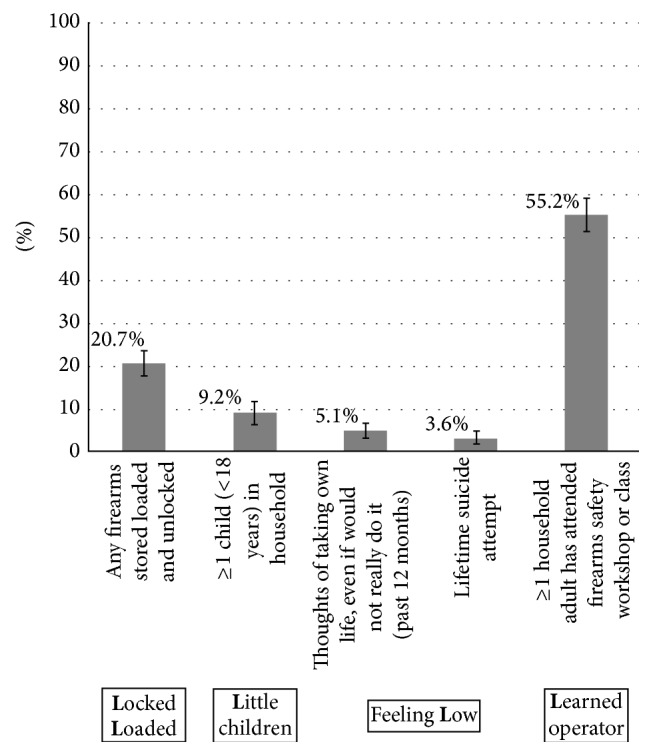
Gun safety practices among older adults with ≥1 gun at home. Weighted prevalence of the 5 Ls framework for gun safety among older adult gun owners (N = 987). Error bars represent 95% Confidence Intervals.
4. Discussion
In this national survey of US older adults, nearly 40% reported a gun in the home, and approximately 1 out of 5 respondents with a gun at home reported that the gun was stored loaded and unlocked. Given the risks for gun-related injuries among older adults, these findings support the importance of considering firearm safety in older adults. The relevance of healthcare providers asking about gun storage is emphasized by studies demonstrating a high prevalence of loaded firearms in households including individuals with dementia (45%) [15] or children (50%) [16]. In this study, less than 10% with a gun at home reported that a child under age 18 lived in the household and those with children in the home were more likely to report safe gun storage, consistent with other reports [17]. In this era of heightened awareness about firearm-related injuries, healthcare practitioners play an important role in assessing gun safety [4, 18, 19]. Although the ICARIS-2 survey did not ask respondents about cognitive or functional status, future studies, as well as clinical practice, should include detailed assessment of these domains that are also important to the overall safety of older adults and may interact with gun safety practices.
Although the report of suicidal ideation and history of suicide attempt were both low, the importance of assessing risk for self-harm must be emphasized. Rates of firearm suicide rise with age, peaking among those aged 80 to 84 years at an age-adjusted rate of 13.3 per 100,000 [20], and a newly acquired firearm warrants further evaluation due to increased mortality risk [6, 15, 21]. Men account for over 90% of all suicides among those aged 70 years and older [20]. Given the evidence of “lethal means restriction” (i.e., restricting access to guns and other lethal methods of suicide) as a suicide prevention approach [22, 23], healthcare providers should assess firearm access in anyone with suicidal thoughts or behaviors.
There are limitations in interpreting these results. While the overall response rate was only 48%, the weighting variable adjusts for over- or undersampling and nonparticipation and the survey's wide sampling frame further strengthens its generalizability to community-dwelling US adults. Second, the survey relies on self-report of potentially sensitive topics (firearms and suicidal thoughts) without external verification for accuracy. Social desirability may have biased responses to sensitive questions, although this would likely be in a direction that would overestimate gun safety. Temporal changes in gun ownership are also a potential limitation, as current gun safety practices may have changed since the survey was conducted. Still, these data are the most recent national estimates with information about the “5 Ls” framework at the individual level.
5. Conclusions
This study provides information about firearm safety practices among US older adults. It emphasizes the potentially elevated risk of firearm injury because of storage practices, suicidal thoughts, or limited firearm safety training. Geriatric practitioners and other health care providers can use the “5 Ls” framework to identify older adults potentially at risk for firearm injury, including those storing guns loaded and unlocked, those with suicidal ideation, and those with limited formal gun safety training. These findings support the need for research to identify effective approaches to assess gun safety and reduce the risk of gun-related injuries among older adults and their household members.
Acknowledgments
The authors thank Drs. Matthew Miller and Carol Runyan for their thoughtful comments on this study and paper. Special thanks are due to Joanna Dukes for assistance with paper preparation. This work was supported by the Paul B. Beeson Career Development Award Program (The National Institute on Aging, AFAR, The John A. Hartford Foundation, and The Atlantic Philanthropies; K23AG043123-Betz).
Disclosure
No sponsor had any direct involvement in study design, methods, subject recruitment, data collection, analysis, or paper preparation. This work was presented as a poster, and abstract was published in annual meeting issue: “Hillary D. Lum, Hanna K. Flaten, Marian E. Betz. Firearm Access and Safety Practices Among Older Adults in the US. (2015), Society for Academic Emergency Medicine Annual Meeting Abstracts. Academic Emergency Medicine, 22: S41. doi: 10.1111/acem.12644.”
Disclaimer
The views in this paper are those of the authors and do not represent the views of the Department of Veterans Affairs or of the funding agencies.
Conflict of Interests
The authors have no conflict of interests.
References
- 1.Mertens B., Sorenson S. B. Current considerations about the elderly and firearms. American Journal of Public Health. 2012;102(3):396–400. doi: 10.2105/ajph.2011.300404. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Kellermann A. L., Rivara F. P., Somes G., et al. Suicide in the home in relation to gun ownership. The New England Journal of Medicine. 1992;327(7):467–472. doi: 10.1056/nejm199208133270705. [DOI] [PubMed] [Google Scholar]
- 3.Hepburn L., Miller M., Azrael D., Hemenway D. The US gun stock: results from the 2004 national firearms survey. Injury Prevention. 2007;13(1):15–19. doi: 10.1136/ip.2006.013607. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Butkus R., Doherty R., Daniel H. Reducing firearm-related injuries and deaths in the United States: executive summary of a policy position paper from the American College of Physicians. Annals of Internal Medicine. 2014;160(12):858–860. doi: 10.7326/m14-0216. [DOI] [PubMed] [Google Scholar]
- 5.Miller M., Azrael D., Hemenway D., Vriniotis M. Firearm storage practices and rates of unintentional firearm deaths in the United States. Accident Analysis and Prevention. 2005;37(4):661–667. doi: 10.1016/j.aap.2005.02.003. [DOI] [PubMed] [Google Scholar]
- 6.Barber C. W., Miller M. J. Reducing a suicidal person's access to lethal means of suicide: a research agenda. American Journal of Preventive Medicine. 2014;47(3, supplement 2):S264–S274. doi: 10.1016/j.amepre.2014.05.028. [DOI] [PubMed] [Google Scholar]
- 7.Miller M., Barber C., White R. A., Azrael D. Firearms and suicide in the United States: is risk independent of underlying suicidal behavior? American Journal of Epidemiology. 2013;178(6):946–955. doi: 10.1093/aje/kwt197. [DOI] [PubMed] [Google Scholar]
- 8.Miller M., Lippmann S. J., Azrael D., Hemenway D. Household firearm ownership and rates of suicide across the 50 United States. Journal of Trauma—Injury, Infection and Critical Care. 2007;62(4):1029–1034. doi: 10.1097/01.ta.0000198214.24056.40. [DOI] [PubMed] [Google Scholar]
- 9.Narayan M. Guns and nurses. American Journal of Nursing. 2014;114(1):p. 11. doi: 10.1097/01.naj.0000441777.34969.2c. [DOI] [PubMed] [Google Scholar]
- 10.Pinholt E. M., Mitchell J. D., Butler J. H., Kumar H. ‘Is there a gun in the home?’ assessing the risks of gun ownership in older adults. Journal of the American Geriatrics Society. 2014;62(6):1142–1146. doi: 10.1111/jgs.12836. [DOI] [PubMed] [Google Scholar]
- 11.Frattaroli S., Webster D. W., Wintemute G. J. Implementing a public health approach to gun violence prevention: the importance of physician engagement. Annals of Internal Medicine. 2013;158(9):697–698. doi: 10.7326/0003-4819-158-9-201305070-00597. [DOI] [PubMed] [Google Scholar]
- 12.Kapp M. B. Geriatric patients, firearms, and physicians. Annals of Internal Medicine. 2013;159(6):421–422. doi: 10.7326/0003-4819-159-5-201309030-00682. [DOI] [PubMed] [Google Scholar]
- 13.Johnson R. M., Coyne-Beasley T., Runyan C. W. Firearm ownership and storage practices, U.S. households, 1992–2002. A systematic review. American Journal of Preventive Medicine. 2004;27(2):173–182. doi: 10.1016/j.amepre.2004.04.015. [DOI] [PubMed] [Google Scholar]
- 14.United States Department of Health and Human Services. Centers for Disease Control and Prevention. OMB Number. 200-1996-00599. Atlanta, Ga, USA: United States Department of Health and Human Services, CDC; 2001. Second injury control and risk survey (ICARIS-2) http://www.cdc.gov/Injury/wisqars/pdf/ICARIS2-PublicUse-DataSet-Documentation.pdf. [Google Scholar]
- 15.Spangenberg K. B., Wagner M. T., Hendrix S., Bachman D. L. Firearm presence in households of patients with Alzheimer's disease and related dementias. Journal of the American Geriatrics Society. 1999;47(10):1183–1186. doi: 10.1111/j.1532-5415.1999.tb05197.x. [DOI] [PubMed] [Google Scholar]
- 16.DuRant R. H., Barkin S., Craig J. A., Weiley V. A., Ip E. H., Wasserman R. C. Firearm ownership and storage patterns among families with children who receive well-child care in pediatric offices. Pediatrics. 2007;119(6):e1271–e1279. doi: 10.1542/peds.2006-1485. Erratum in: Pediatrics, vol. 120, no. 2, p. 460, 2007. [DOI] [PubMed] [Google Scholar]
- 17.Coyne-Beasley T., Runyan C. W., Baccaglini L., Perkis D., Johnson R. M. Storage of poisonous substances and firearms in homes with young children visitors and older adults. American Journal of Preventive Medicine. 2005;28(1):109–115. doi: 10.1016/j.amepre.2004.09.013. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Albright T. L., Burge S. K. Improving firearm storage habits: impact of brief office counseling by family physicians. Journal of the American Board of Family Practice. 2003;16(1):40–46. doi: 10.3122/jabfm.16.1.40. [DOI] [PubMed] [Google Scholar]
- 19.Rathore M. H. Physician ‘gag laws’ and gun safety. Virtual Mentor. 2014;16(4):284–288. doi: 10.1001/virtualmentor.2014.16.04.pfor2-1404. [DOI] [PubMed] [Google Scholar]
- 20.Center for Disease Control. Web-based Injury Statistics Query and Reporting System (WISQARS) October 2014, http://www.cdc.gov/injury/wisqars/index.html.
- 21.Wintemute G. J., Parham C. A., Beaumont J. J., Wright M., Drake C. Mortality among recent purchasers of handguns. The New England Journal of Medicine. 1999;341(21):1583–1589. doi: 10.1056/nejm199911183412106. [DOI] [PubMed] [Google Scholar]
- 22.Mann J. J., Apter A., Bertolote J., et al. Suicide prevention strategies: a systematic review. The Journal of the American Medical Association. 2005;294(16):2064–2074. doi: 10.1001/jama.294.16.2064. [DOI] [PubMed] [Google Scholar]
- 23. National Strategy for Suicide Prevention: Goals and Objectives for Action, 2012, http://www.surgeongeneral.gov/library/reports/national-strategy-suicide-prevention/full-report.pdf. [PubMed]