

Abstract
BACKGROUND
In 2010, the Louisiana Asthma Management and Prevention Program (LAMP) implemented the Asthma-Friendly Schools Initiative in high-risk Louisiana populations. The social ecological model (SEM) was used as a framework for an asthma program implemented in 70 state K-12 public schools over 2 years.
METHODS
Activities included a needs assessment, identification of students with asthma, individualized asthma action plans (AAP), staff trainings, environmental quality improvement, and school system policy changes to address the asthma burden.
RESULTS
There were 522 new or existing asthma cases recognized. Asthma knowledge/awareness was measurably improved among school personnel. School indoor air quality was improved across all locations. School-level polices were adopted that improved AAP collection, compliance to bus-idling restrictions, and asthma medication self-carry.
CONCLUSIONS
The SEM framework can be used for school-based programs to address successfully and improve asthma-related issues from the individual through policy levels.
Keywords: asthma, social ecological model, schools
Asthma is a chronic disease characterized by inflammation and narrowing of the airways that is triggered by allergens or irritants.1 Symptoms include coughing, wheezing, chest tightness, and difficulty breathing. Asthma accounts for nearly 2 million emergency department visits and over 3000 deaths in the United States annually.2,3
Asthma is the most common chronic disease among U.S. children, with approximately 8.4% of children currently diagnosed.4,5 School-aged children with asthma are at an academic disadvantage compared to their peers without asthma.6,7 The disparity may arise because asthma is the leading cause of school absences among children ages 5-17 and accounts for >10 million school days missed per year.5,8 Asthma particularly impacts quality of life and educational attainment of low-income, minority children who experience higher morbidity rates and lower access to health care.5,9 One way to address childhood asthma is through programs that address multiple components of asthma and can be sustainably incorporated into school operations. School-based asthma programs can impact the majority of children with asthma and address disparities in high-risk, hard-to-reach populations.
Asthma is a serious health issue for Louisiana’s students, with 8.3% of the state’s high school students reporting that they have current asthma.10 Louisiana children are at a particular risk of asthma exacerbations due to the state’s humid, subtropical climate that exposes students to harmful indoor and outdoor allergens, such as molds and cockroaches.11 The state also has the third highest percent (66%) of low-income students in public school, suggesting that the schools serve a population with a high burden of underdiagnosed and uncontrolled asthma.12 With over 700,000 students enrolled in 1500 public schools, Louisiana schools are an important setting for addressing asthma among students.13
The Louisiana Department of Health and Hospitals (DHH) has addressed the state asthma burden through school-based asthma activities since 2005. The Louisiana Asthma Management and Prevention Program (LAMP) was established by the DHH’s Bureau of Primary Care and Rural Health Chronic Disease Prevention and Control Unit in 2007 to improve the state’s capacity to address asthma. In 2009, LAMP and the Louisiana Asthma Surveillance Collaborative (LASC) successfully applied for Centers for Disease Control and Prevention (CDC) funding (#EH09-901) to develop or strengthen statewide asthma programs. To identify populations that would benefit most from state-run asthma initiatives, LAMP examined asthma surveillance data from the 2002-2008 Behavioral Risk Factor Surveillance System, the Louisiana Youth Risk Behavior Survey, Youth Tobacco Survey, Medicaid claims data, and Hospital Inpatient Discharge Database.14-16 Data indicated that asthma prevalence and hospitalizations were higher among children than adults.10 Based on the surveillance data, the success of the previous school asthma initiatives, and CDC guidance, LAMP decided to broaden their school-based asthma program. This article describes how LAMP established, implemented, and evaluated an asthma-friendly school program to address the asthma burden in school-aged children.
METHODS
Theoretical Basis
Louisiana Asthma Management and Prevention Program selected the social ecological model (SEM) as the theoretical framework to identify multiple layers of influence on asthmatic students at the individual, interpersonal, institutional, community, and policy levels (Figure 1).17-19 The resulting LAMP Asthma-Friendly Schools (AFS) Initiative had multiple components designed to impact factors that influence asthma on the different levels of the SEM (Table 1). This multicomponent program could be easily adopted by schools to better accommodate students with asthma.
Figure 1.
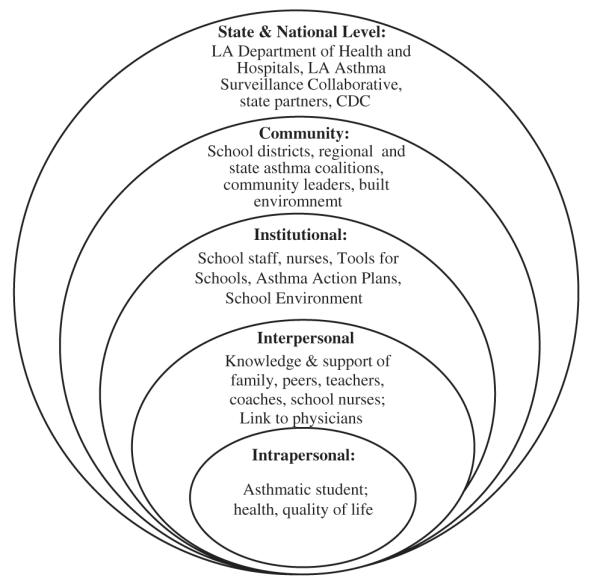
Social Ecological Model Displaying the Multilevel Factors That Influence the Asthma Outcomes for a Student With Asthma and the Components That Address These Influences
Table 1.
Major Components and Effects of the Louisiana Asthma Management and Prevention’s Asthma-Friendly School Initiative as Outlined by Constructs of the Social Ecological Model.
| Intrapersonal | Interpersonal | Institutional | Community | State/National | |
|---|---|---|---|---|---|
| Asthma Regional Coordinators |
Engage schools. Train school staff to increase asthma awareness. Promote school-wide implementation of Act 145. Conduct IAQ walkthroughs Provide materials from the state to the school. |
Engage school districts Act as state liaison to school districts and regional organizations. Promote district-wide implementation of Act 145. Assists with regional coalition activities and AFS designation. |
|||
| Asthma Action Plans (AAP) |
Provide individualized asthma management plan for each student leading to improved asthma self-management. |
Inform caregivers and pertinent school faculty about managing a student’s asthma. Link students with asthma to a primary care physician. |
Inform school nurses and faculty about an appropriate response during an asthma emergency. |
||
| School trainings | Train school staff to have more effective interactions with students with asthma. |
Increase awareness in schools about asthma risk factors and policies. Teaches staff how to improve and maintain a healthy school environment for students with asthma. |
|||
| Indoor Air Quality (IAQ) walkthroughs, “nO idLING” and State Tobacco-Free Policy |
School faculty learn how to reduce asthma triggers in classroom. “No bus idling” signs discourage parents and school bus drivers from idling their vehicles. |
Reduces school asthma triggers. Improves air quality outside of the school. |
Supports school district-wide implementation of “no bus idling zones.” |
Louisiana Tobacco-Free School District Policy prohibits tobacco use on campuses, sporting events, dances or other events on school property. |
|
| Regional, state coalitions |
Designate and promote asthma-friendly schools. Identify school-level needs for addressing asthma. Develop asthma-related materials for the ARC to distribute to schools. |
Identify high-need districts for intervention implementation. Engage and guide community asthma coalitions. |
Provide information on program success to state legislators. Share success stories and resources with other state asthma programs. |
ARC, Asthma Regional Coordinators.
Asthma-Friendly Schools Initiative Development
Using surveillance data, LAMP identified regions with the highest prevalence of childhood asthma. Asthma Regional Coordinators (ARCs) were contracted from nonprofit organizations and served as regional representatives for LAMP. Asthma Regional Coordinators established regional asthma coalitions and helped them select school districts that would benefit most from the program. The ARCs also worked directly with schools to improve indoor air quality and provided outreach to student caregivers.
Asthma Regional Coordinators and LAMP collaborated with the Louisiana School Nurses Organization to administer a needs assessment survey (Table 2) to 82 school nurses from 32 school districts. The 20-item survey asked nurses about the school’s current asthma policies, treatment frequency for students with asthma, school environmental triggers, proper medication use, asthma action plan (AAP) availability, and perceived needs for serving students with asthma. The needs assessment suggested that the program should use an adapted version of the National Heart, Lung, and Blood Institutes’ (NHLBI) National Asthma Education and Prevention Program “How Asthma Friendly Is Your School?” checklist as a guide (Figure 2).20 Louisiana Asthma Management and Prevention Program also incorporated the CDC’s “Initiating Change: Creating an Asthma Friendly School” toolkit to develop and implement the asthma-friendly school program and policies.21 This effort to improve asthma outcomes for school children in Louisiana school districts became known as the AFS Initiative.
Table 2.
Selected School Nurse Survey Items and Responses (N = 82).
| Survey Items and Responses | N (%) |
|---|---|
| “How many of your asthmatic students do not have an asthma action (AAP) available at the school they attend?” | |
| Yes | 6 (7.3) |
| No | 16 (19.5) |
| Don’t know | 58 (70.7) |
| “How often do you see students because of asthma attacks?” | |
| Daily | 15 (18.3) |
| Several times a week | 24 (29.3) |
| Rarely on a monthly basis | 14 (17.1) |
| “Do you view environmental factors in school as triggering an asthma response in students?” | |
| Yes | 68 (82.9) |
| No | 7 (8.5) |
| “Are more students at your schools absent due to asthma as compared to other diseases?” | |
| Yes | 57 (69.5) |
| No | 13 (15.9) |
| “What are the top five most needed items at your schools for caring for children with asthma?” | |
| Quick relief asthma inhalers | 38 (46.3) |
| Asthma action plans | 17 (20.7) |
| Education materials | 13 (15.9) |
| Spacers | 13 (15.9) |
| Peak flow meters | 10 (12.2) |
| “Does your school district have an asthma school toolkit?” | |
| Yes | 4 (4.9) |
| No/don’t know | 77 (93) |
Figure 2.

Louisiana Asthma Management and Prevention Program’s Adoption of the National Heart, Lung, and Blood Institute’s “How Asthma Friendly Is Your School?” Checklist.
Coalitions identified 32 high-burden public school districts for recruitment after a review of Medicaid claims and hospitalization data. Letters and emails were sent to selected district superintendents, administrators, and school nurses inviting them to participate in the AFS Initiative. Kindergarten through 12th grade public schools were targeted in alignment with the 2009 Louisiana Act 145, which mandates that students with asthma be allowed to self-carry/administer prescribed medications in public schools.22 Invitees met with ARCs and LAMP personnel to discuss their district’s asthma burden. Benefits of the AFS Initiative were promoted, including reduced absenteeism, increased instruction time, improved medication compliance, a healthier environment for students with asthma, and greater school recognition on the local and state level. Program feasibility was discussed, including a list of the ways the state asthma program would support AFS activities.
Implementation
School personnel training
Participating school personnel received a 30-minute, in-person asthma training session from ARCs and/or LAMP personnel, which educated them on asthma etiology, triggers, and symptoms. Proper use of quick relief inhalers, AAPs, and how to maintain an asthma-friendly environment were also discussed. Schools were provided with a Louisiana Asthma School Management Plan, which included protocols for treating students with asthma when school nurses were unavailable. School nurses received training on the Expert Panel Review 3 Asthma Clinical Guidelines created and provided by health care professionals who served on the LASC. Trainings provided school nurses with evidence-based knowledge necessary to provide effective care for asthmatic students.
Confirming diagnosis and treatment through AAPs
Information gathered from school files and personnel meetings indicated that there were students with undocumented and/or undiagnosed asthma. Among students with documented asthma, a large proportion did not have AAP on file. To adhere to AFS parameters, LAMP required participating schools to obtain AAPs for ≥50% of students with documented asthma and to identify students requiring a physician assessment for asthma. At the beginning of the academic year, nurses at participating schools conducted a baseline assessment of students with a physician-signed AAP and a Louisiana Medication Order Form that allowed for self-carry and administration of asthma drugs. Caregivers of undocumented asthmatic students were provided information on AAPs, the school district’s partnership with the state health department, and Louisiana Act 145. Caregivers were asked to schedule a physician visit to have the student’s asthma assessed, AAPs completed and placed on school files, and medications updated before the end of the first school quarter.
Air quality walkthroughs
Asthma Regional Coordinators conducted campus walkthroughs accompanied by school maintenance and custodial staff to identify potential asthma triggers, such as pest control issues, blocked air ducts, scent dispensers, and exposure to bus exhaust fumes. Asthma Regional Coordinators checked off requirements in the “Louisiana’s Top Ten No- or Low-cost Tools for Schools Indoor Air Quality Interventions” (LA Top Ten) checklist adapted from the Environmental Protection Agency’s Top 10 Tips for Managing Asthma in Schools.23 Results were reviewed with school administration, school district officials, and LAMP personnel. Schools had to meet ≥70% of the LA Top Ten criteria to pass the assessment. If the mark was not met, the ARC helped the school resolve concerns and conducted follow-up walkthroughs. When major environmental issues were identified, the ARC requested a Louisiana’s Section of Environmental Epidemiology and Toxicology (SEET) indoor air quality expert to conduct a secondary walkthrough with advanced equipment and to provide advice to the school’s maintenance, custodial and administrative staff.
“No Bus Idling” and Tobacco-Free School District Policy support
The ARCs encouraged participating school districts to adopt a “no bus idling” policy developed by LAMP and SEET’s indoor air quality expert, which required buses to turn off engines on campus when possible. To meet a key component of the LA Top Ten checklist, schools were evaluated on their compliance to Louisiana’s Smoke-Free Air Act in Schools.24 The ARCs encouraged participating schools to adopt the Louisiana Tobacco Control Program’s Tobacco-Free School District Policy to reduce overall tobacco consumption among school personnel and students.25
Resources and collaboration at the state and national level
Louisiana Asthma Management and Prevention Program, LASC, and other state-level partnering institutions collaborated to create and distribute resources to participating AFS Initiative schools. Resources included the Louisiana AFS checklist, LA Top Ten checklist, and brochures to assist physicians with the development AAPs. Louisiana Asthma Management and Prevention Program also collaborated with LASC, school personnel, the Louisiana Department of Education, and the Louisiana School Nurses Organization to create the Louisiana Asthma Tools for Schools toolkit. This toolkit compiled asthma resources for school personnel, such as AAP templates and plain language translations of the 2009 Louisiana’s Act 145 and the Smoke-Free Air Act in Schools. Finally, LAMP, LASC, and the Secretary of Louisiana’s DHH supported state and national media recognition for schools designated as Asthma Friendly, which informed other schools in Louisiana and the United States about the Initiative.
Data collection and evaluation
Monitoring and evaluation were conducted for every AFS Initiative component. Using standardized forms provided by LAMP, school nurses tracked the number of students diagnosed with asthma and carrying signed AAPs on file at baseline, mid-, and end of year mark. School nurses also tracked the number of students with signed self-carry forms, indicating compliance with Louisiana Act 145. Asthma Regional Coordinators assessed asthma knowledge gained by school personnel participating in asthma trainings via a 10-item pre- and post-test with multiple choice and true/false items. Test questions assessed knowledge about their general understanding of asthma etiology, triggers, and symptoms, as well as other asthma-friendly school indicators. The paired samples t test measured changes in knowledge from pre- to post-test at a significance level of p < .05. The requirements in the LA Top 10 checklist from participating schools were summarized and the number of schools meeting ≥70% of achievements were quantified. Areas for improvement were qualitatively assessed. The LAMP program evaluator collected data from participating nurses on changes in the school asthma burden annually, including the frequency with which students were checking out of school with asthma-related symptoms and asthma-related absenteeism.
RESULTS
From 2010 to 2012, 64 schools in 8 school districts throughout the state participated in the Louisiana AFS Initiative in both urban and rural areas. The majority of schools were either elementary (48.9%) or high schools (31.3%), but included all schools with a grade range from K-12. Participating schools districts were located in the Claiborne, DeSoto, East Feliciana, Orleans, Red river, St. Bernard, West Baton Rouge, and West Carroll Parishes. The AFS Initiative helped schools identify an additional 522 students with undocumented asthma, a 36% increase from the average baseline number across all schools. The number of signed AAPs on file at participating schools increased 67% from baseline. The increase in AAPs did not match the number of students identified with undocumented asthma. The number of students authorized by physicians to carry and self-administer quick relief inhalers doubled from baseline to end of the year follow-up (133%).
Over 2400 school personnel were trained on asthma basics, asthma-friendly environments, and asthma attack response. Most participants were teachers (70%) and the remainder self-classified as administration, coaches, counselors, maintenance, or “other staff.” Asthma knowledge scores increased significantly from pre- to post-test (7.1 ± 1.6 to 8.9 ± 1.1, respectively, p < .05). No differences were observed between job categories. Most participants correctly answered pre-test items related to whether asthma is fatal (91.8%) and properly identified lesser known asthma triggers, such as perfume (89.1%) and laughing (80.1%). Respondents were also aware that children with asthma can be as active as peers without asthma if they are given proper care (96.8%). However, most participants were unaware of asthma symptoms and certain types of triggers, such as animal dander (47.6%) and exercise (33.7%). Prior to the training, approximately 40% falsely believed that designated smoking areas on a school campus were asthma-friendly characteristics, but the trainings reduced this percentage to below 10% (p < .01).
Thirty-three percent of schools that did not meet the 70% mark on the LA Top Ten checklist at baseline improved their score to ≥70% after the indoor air quality walkthroughs. Air quality walkthroughs in poorer, older Louisiana schools identified and addressed common environmental triggers, including chipping paint, mold from water damage, heavy dust in cluttered rooms, and aging heating, ventilation, and air conditioning systems. One noteworthy success was St. Bernard School District, which improved from an air quality score of 63 to a near-perfect 99 (scale 0 to 100). Schools made changes such as removing scent producers and outdated rugs in classrooms and reducing the concentration of chemicals used in cleaning supplies. All eight participating school districts adopted a bus-idling policy.
In a follow-up survey of 14 head school nurses in each of the targeted school districts, 60% reported fewer students checking out of school with asthma-related symptoms and a perceived a reduction in asthma-related absenteeism. They also reported a noticeable increase (not quantified) in the number of AAPs on file and enforcement of the district’s school bus idling policy. Nurses also reported an increase in their own awareness, including an improved understanding among school personnel on asthma triggers, asthma symptoms, and caring for students with asthma.
Conclusions
The evaluation results suggest that the Louisiana AFS Initiative provides a feasible and sustainable program for improving outcomes among students with asthma. Many of the tools, such as CDC AFS toolkit, were available on-line at no cost and easily adapted for specific purposes in Louisiana. Schools in other states could use this same approach in developing resources for reducing the burden of asthma. State partners, such as the Louisiana Department of Education, the state’s nurse organization, and the Office of Public Health SEET Indoor Air Quality expert provided important perspectives on AFS documents and program priorities. Contributions from these partners were also free of cost. Louisiana Asthma Management and Prevention Program’s relationship with the school nurse organization helped gain the opinions and respect of school nurses across the state. Furthermore, low-cost state resources, such as the school toolkit, training materials, and AAP templates helped to reduce the burden on participating school nurses.
The AFS trainings were not time consuming and uniformly enhanced asthma-related knowledge for all school districts. This finding suggests that the trainings were both appropriate and helpful for all school personnel, regardless of job category. The change in the percentage of schools meeting asthma-friendly air quality standards indicates that the program can improve learning environments for asthma students. Evidence of sustainability was demonstrated by improvements maintained throughout the school year, such as indoor air quality, improvements in children’s health and school participation as observed by nurses, as well as school personnel’s knowledge and concepts of a healthy environment.
From a socioecological perspective, there were many factors that contributed to the AFS Initiative’s success. Surveillance data informed LAMP who and where to target delivery of AFS resources for optimal results. Asthma Regional Coordinators were instrumental in promoting the program on campuses, which allowed them to specify the schools’ concerns or identify environmental issues firsthand. Face-to-face trainings engaged school personnel more than a manual or online training and ensured that feedback was appropriately collected. The relationship between the regional coordinators and school personnel was instrumental in increasing awareness within the school and the number of AAPs on file. School nurses were integral to the AFS Initiative’s success because they helped collect data, guide the distribution and collection of AAPs and self-carry forms, and they supported school-wide adherence to AFS guidelines. In addition, school nurse observations provided vital information for improving the quality of the program and care for asthmatic students. Some nurses reported that their participation with the program empowered them to make their schools more asthma friendly. Finally, the AFS Initiative’s engagement of regional asthma coalitions in school recruitment and assessment was also an effective method for gaining school district and community support.
The results also show areas where the AFS Initiative could improve. For example, the AAPs did not match the number of students identified with undocumented asthma, suggesting that linkages between students with asthma and their physician need to be strengthened. Pre- and post-test results indicate that trainings should focus on asthma symptoms, common triggers, and smoke-free environments. Louisiana Asthma Management and Prevention Program continues to identify program components that can be enhanced to improve the AFS Initiative. To improve understanding of the Initiative’s impact, LAMP seeks a new mechanism for tracking asthma-related school absences. In addition, LAMP is examining ways to provide continuing asthma education and reminders about state regulations regarding self-carry policies to students, parents, and school personnel. Other future considerations include developing an online AFS training module that can quickly and easily be administered to schools for which face-to-face trainings are not feasible.
IMPLICATIONS FOR SCHOOL HEALTH
This article demonstrates that the application of a social ecological framework to addressing asthma burden at the school level can be both effective and feasible. At the most exterior layer, the inclusion of state and national support and resources provides a low-cost and critical foundation for school districts to implement public health initiatives, such as the AFS Initiative. This support proved to be instrumental in Louisiana in successfully implementing AFS activities at the institutional and community levels. As a result, schools were better equipped and able to identify students with asthma, potentially improve linkages between children with asthma and physicians, improve knowledge among teachers, and improve indoor air quality. We recommend other school districts in other parts of the nation include state and national support to implement and maintain school-based asthma programs.
We also recommend that other schools wishing to improve conditions for their asthmatic students incorporate institutional policies and regulations, such as setting limits on bus idling and prohibiting tobacco use on campus. If not for the environmental impact, adopting such policies and regulations creates awareness and consideration of students with asthma. This awareness can extend from campuses to homes and on into the larger community. We also found that holding schools accountable for making improvements and recognizing their accomplishments had reinforcing effects on successful schools. By keeping track of a schools’ status via a comprehensive checklist, such as the tool employed by AFS, administrators can be made aware of conditions in their schools and prime them for change.
When designing and implementing school-based asthma programs, the incorporation of a theory-based framework, such as the SEM, is a viable and important strategy for program success. A framework provides a road map for program activities, areas of focus to maximize resources, and illuminates measureable processes and outcomes that can be evaluated. We found the SEM to be particularly useful in our work as it provided us with a comprehensive view of school-based asthma management and prevention.
With a low cost to schools and high potential for impact on childhood asthma, the Louisiana AFS Initiative provides a programmatic framework that other states can feasibly replicate. By using the SEM as the framework for AFS, school-based asthma programs can comprehensively and sustainably address childhood asthma. Perhaps the main public health implication is that programs or interventions run locally in schools with state- and community-level assistance can lead to better identification of students with asthma, potentially improved linkages between children with asthma and physicians, improved knowledge among teachers, and more sustainable school-level air quality.
Human Subjects Approval Statement
This program and related activities were exempt to regulatory requirements as described in the Code of Federal Regulations 45 CFR 46, section 46.101(b).
Acknowledgments
Funding for the Louisiana Asthma Management and Prevention Programis provided by the Centers for Disease Control and Prevention (CDC) grant # CDC-RFA-EH09-90105CONT13. The findings and conclusions in this article are those of the authors and do not necessarily represent the views of the CDC.
REFERENCES
- 1.US Centers for Disease Control and Prevention [Accessed August 22, 2013];Asthma. Basic information. What is asthma? Available at: http://www.cdc.gov/asthma/faqs.htm.
- 2.US Centers for Disease Control and Prevention [Accessed August 19, 2013];National Hospital Ambulatory Medical Care Survey: 2010 emergency department summary tables. Available at: www.cdc.gov/nchs/data/series/sr_03/sr03_035.pdf.
- 3.Murphy SL, Xu JQ, Kochanek KD. National Vital Statistics Reports. National Center for Health Statistics; Hyattsville, MD: May, 2013. Deaths: Final Data for 2010. DHHS Publication No. 2013-1120. [PubMed] [Google Scholar]
- 4.World Health Organization [Accessed August 19, 2013];Asthma fact sheet number 307. Available at: http://www.who.int/mediacentre/factsheets/fs307/en/index.html.
- 5.Akinbami LJ, Moorman JE, Bailey C, et al. Trends in asthma prevalence, health care use, and mortality in the United States, 2001-2010. NCHS Data Brief. 2012;94:1–8. [PubMed] [Google Scholar]
- 6.Crump C, Rivera D, London R, Landau M, Erlendson B, Rodriguez E. Chronic health conditions and school performance among children and youth. Ann Epidemiol. 2013;23(4):179–184. doi: 10.1016/j.annepidem.2013.01.001. [DOI] [PubMed] [Google Scholar]
- 7.Fowler MG, Davenport MG, Garg R. School functioning of US children with asthma. Pediatrics. 1992;90(6):939–944. [PubMed] [Google Scholar]
- 8.Akinbami L. The state of childhood asthma, United States, 1980-2005. Adv Data. 2003;6(381):1–24. [PubMed] [Google Scholar]
- 9.Lewis TC, Robins TG, Joseph CL, et al. Identification of gaps in the diagnosis and treatment of childhood asthma using a community-based participatory research approach. J Urban Health. 2004;81(3):472–488. doi: 10.1093/jurban/jth131. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Youth Risk Behavior Surveillance System [Accessed August 19, 2013];Data from 2011. Available at: http://apps.nccd.cdc.gov/youthonline/App/Results.aspx?LID=LA.
- 11.Yang C-Y, Lin M-C, Hwang K-C. Childhood asthma and the indoor environment in a subtropical area. Chest. 1998;114(2):393–397. doi: 10.1378/chest.114.2.393. [DOI] [PubMed] [Google Scholar]
- 12.Southern Education Foundation [Accessed December 26, 2013];A new majority: low income students in the south and nation. Available at: http://www.southerneducation.org/Programs/P-12-Program/Early-Ed/NewMajority.aspx.
- 13.Kids Count Data Center [Accessed January 6, 2014];Student enrollment in public schools: Louisiana. Available at: http://datacenter.kidscount.org/data/tables/1470-student-enrollment-in-public-schools?loc=20&loct=2#detailed/2/any/false/1026,921,800,88,87/any/9895.
- 14.US Centers for Disease Control and Prevention [Accessed August 19, 2013];Adolescent and school health. Available at: http://www.cdc.gov/healthyYouth/yrbs/factsheets/index.htm.
- 15.US Centers for Disease Control and Prevention [Accessed October 19, 2013];Smoking and tobacco use. Available at: http://www.cdc.gov/TOBACCO/data_statistics/surveys/yts/index.htm.
- 16.Louisiana Department of Health and Hospitals [Accessed January 6, 2014];State Center for Health Statistics. Available at: http://www.dhh.louisiana.gov/index.cfm/page/647/n/238.
- 17.McLeroy KR, Bibeau D, Steckler A, Glanz K. An ecological perspective on health promotion programs. Health Educ Q. 1988;15(4):351–377. doi: 10.1177/109019818801500401. [DOI] [PubMed] [Google Scholar]
- 18.Stokols D. Translating social ecological theory into guidelines for community health promotion. Am J Health Promot. 1996;10(4):282–298. doi: 10.4278/0890-1171-10.4.282. [DOI] [PubMed] [Google Scholar]
- 19.Richard L, Gauvin L, Gosselin C, Ducharme F, Sapinski JP, Trudel M. Integrating the ecological approach in health promotion for older adults: a survey of programs aimed at elder abuse prevention, falls prevention, and appropriate medication use. Int J Public Health. 2008;53(1):46–56. doi: 10.1007/s00038-007-6099-5. [DOI] [PubMed] [Google Scholar]
- 20.National Heart, Lung, and Blood Institute [Accessed August 28, 2013];How asthma-friendly is your school? Available at: http://www.nhlbi.nih.gov/health/public/lung/asthma/friendhi.htm.
- 21.US Centers for Disease Control and Prevention [Accessed August 23, 2013];Initiating change: creating an asthma-friendly school. Available at: http://www.cdc.gov/healthyyouth/asthma/creatingafs/index.htm.
- 22.Asthma Medication Law Louisiana Act 145, RS 17:436.1, June 25, 2009.
- 23.Environmental Protection Agency [Accessed August 19, 2014];Connector E-Newsletter #45: Top 10 tips for managing asthma in schools. Available at http://www.epa.gov/iaq/schools/managingasthma.html.
- 24.Louisiana Smoke-Free Air Act 815, RS 40:1300.251-263 (January 1, 2007).
- 25.The Louisiana Department of Health and Hospitals’ [Accessed January 6, 2014];Tobacco Control Program. Available at: http://www.latobaccocontrol.com.